
Abstract
Background:
Bipolar disorder often begins in adolescence or early adulthood, characterized by recurrent manic episodes that can lead to neurodegenerative brain changes and functional decline. While several oral second-generation antipsychotics are Food and Drug Administration (FDA)-approved for mania, adherence to maintenance treatment is frequently poor due to factors such as anosognosia, cognitive dysfunction, impulsivity, side effects aversion, and substance use. Long-acting injectable (LAI) antipsychotics, approved for adults with bipolar mania or schizoaffective disorder (bipolar type), offer a potential solution for adolescents with similar conditions. This study reports on the efficacy of LAI antipsychotics in managing bipolar mania in adolescents, tracking outcomes over up to a year with baseline and follow-up Young Mania Rating Scale (YMRS) assessments.
Methods:
The study included 116 adolescents with a mean age of 16.17 years (66% male, 48% white, 23% black). Of these, 73% were diagnosed with bipolar mania and 22% with schizoaffective disorder, bipolar type. The mean illness duration was 1.9 years, with a baseline YMRS score of 33.8 and a body mass index (BMI) of 23.4 kg/m2. LAI antipsychotics administered included aripiprazole, paliperidone, and risperidone, given at intervals of 1, 2, or 3 months.
Results:
YMRS scores showed substantial improvement, declining to 21.7 at 1 month, 12.3 at 2 months, 4.9 at 6 months, and 3.0 at 1 year. Common side effects were increased appetite and weight gain (mean BMI rose to 26.3 kg/m2). There were no dropouts, although 12% of participants switched formulations due to side effects. Notably, 86.2% of adolescents improved sufficiently to return to school or work. While 28.4% experienced depressive episodes, there were no suicide attempts or deaths during the 4- to 14-month follow-up.
Discussion:
This study demonstrates that LAI antipsychotics can effectively stabilize adolescents with bipolar mania or schizoaffective disorder, bipolar type, showing a marked decline in YMRS scores and high rates of remission and functional recovery. Despite the lack of FDA approval for LAI antipsychotics in those younger than 18, our results from off-label use suggest significant efficacy and tolerability. Further FDA clinical trials are needed to explore LAI antipsychotic formulations in adolescents to address the needs of this high-risk, nonadherent population.
Introduction
Bipolar disorder (BD) affects ∼2% of the global population with onset frequently during adolescence (Jain and Mitra, 2023). Adolescents with BD face unique challenges in treatment, particularly in managing symptoms and adhering to prescribed oral medications. This can lead to a significant increase in the risk of relapse, hospitalization, financial burden, and suicide attempts. Despite the plethora of treatment options, some adolescents remain noncompliant, often forgetting to take oral medications or stopping them abruptly when they feel better or worse. This nonadherence, driven by denial of illness, impulsivity, and stigma, highlights the need for specialized and novel treatment approaches.
Adolescents with BD experience nonadherence rates ranging between 44% and 66% (Coletti et al., 2005; Patel et al., 2005). When BD in adolescents remains untreated, it can profoundly affect their emotional and social development. Without appropriate medical care, the highs of mania and the lows of depression can become more severe and more difficult to control, potentially leading to treatment resistance. Untreated BD can also contribute to cognitive decline, including memory, attention, and executive functioning impairments. Prolonged periods of instability may also increase the risk of substance abuse, self-harm, and suicide. Social relationships, academic performance, and overall quality of life may deteriorate, causing long-term emotional sequelae. The neurobiology of BD is complex, encompassing genetic and environmental (psychosocial) factors, requiring a multifaceted treatment strategy (Freund and Juckel, 2019). Antipsychotic pharmacotherapy is an important component of managing BD due to elevated dopamine activity in mania.
Even though various treatment options for BD are available, it is hard to customize them to the individual needs of each nonadherent patient. If an individual has no family history of BD, it may take them longer to be diagnosed and treated (Vieta et al., 2018). A delayed diagnosis of BD can also result in turbulent life events as well as suicidal behavior due to depressive episodes (Tondo et al., 2014). Given that children and adolescents are still undergoing cognitive and physical development, it is imperative to use long-acting injectable (LAI) formulations as a first-line treatment option to improve long-term outcomes, especially if they are nonadherent to oral medications.
In recent years, LAI antipsychotics have shown promising results in treating severe cases of BD by improving medication adherence and reducing relapse rates in adults. However, there is still limited research on how well they work for adolescents with poor adherence. Due to the challenges of maintaining consistent medication adherence in adolescents, there is a preference for monthly or bimonthly LAI administration over oral medications because they can achieve therapeutic effects without the need for daily intake of oral medications, which can be highly inconsistent (Aggarwal et al., 2018). LAI formulations release the antimanic drug slowly and consistently into the bloodstream, leading to more stable plasma concentrations (low peak-to-trough) than oral formulations. Oral medications require daily adherence, which can be challenging for many young patients, particularly those with limited insight into their illness. Studies have suggested that missed doses of oral medications can lead to subtherapeutic plasma levels and increased relapse rates, making LAI a more reliable option for long-term maintenance therapy. Adolescents with BD are a vulnerable clinical population with ongoing challenges; incorporating LAIs into their care plan offers the potential for achieving sustained clinical stability.
The study includes data from 116 adolescent patients who were tried on LAIs for the treatment of mania in patients with BD. With this, we aim to address the clinical outcomes of LAIs in adolescents, mainly focusing on their potential benefits and limitations in this population. The patients in this study were administered LAIs, including aripiprazole, paliperidone, and risperidone, all of which are FDA-approved to treat acute mania in adults.
Methods
Study population and data sources
This case series involved 116 adolescent patients aged 12–17 years (mean age = 16.17 years) who were diagnosed with BD and whom we treated with LAI antipsychotics at our outpatient clinic from January 2016 to June 2024. The cohort included 55.9% males and 44.1% females, with a racial composition of 48% Caucasians, 25% Hispanics, 23% African Americans, and 3% belonging to other racial and ethnic affiliations. Diagnostic breakdown within the cohort included 73% with bipolar I disorder, manic episode, 22% with schizoaffective disorder, bipolar type, and the other 5% with BD (unspecified). The mean duration of illness before initiating LAI treatment was 1.9 years. 16.3% of patients had a first-degree relative with a history of BD. Data were collected from the electronic medical records of these patients, including demographic information, psychometric evaluations, clinical diagnoses, treatment details, and outcomes.
Inclusion criteria
Participants included in the study met the following criteria: (1) adolescents aged 12–17 years diagnosed with BD according to Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria; (2) initiation of LAI antipsychotic treatment within the study period from January 2016 to June 2024; (3) documented regular clinical follow-up and adherence to treatment for a minimum of 48 weeks postinitiation of LAI antipsychotics; (4) availability of complete baseline and follow-up data, including clinical history, and psychometric assessments at every follow-up; and (5) previously treated only with oral antipsychotics.
Baseline assessments and pre-LAI treatment
Baseline characteristics, before initiating LAI antipsychotic treatment, were assessed, including demographic data, clinical history, and psychometric evaluations. Mania severity was quantified using the Young Mania Rating Scale (YMRS) scores recorded in the patient’s charts. The YMRS interviews were conducted by qualified health care professionals, including psychiatrists and psychiatric nurse practitioners, who were experienced in the clinical assessment of manic symptoms. These professionals regularly performed the interviews and documented the YMRS score as part of their routine evaluation of patients. The mean YMRS score of the study sample at the baseline before administering LAI was 33.8 (standard deviation [SD] = 6.3). The mean baseline body mass index (BMI) was 23.4 kg/m2. All patients had previously been prescribed oral antipsychotic medications for an average duration ranging from 4 to 14 months but demonstrated nonadherence and inadequate symptom control, which prompted the transition to LAI antipsychotic treatment.
Intervention
The LAI antipsychotics administered Intramuscular (IM) included Abilify Maintena (aripiprazole) in 4.31% of patients, Abilify Asimtufii (aripiprazole) in 33.68%, Aristada (aripiprazole lauroxil) in 43.96%, Invega Sustenna (paliperidone palmitate) in 16.37%, and Uzedy (risperidone) in 1.68%. The specific LAI formulation was selected based on clinical judgment, patient treatment history, and individual preferences. Dosing intervals varied, with injections administered every 1 or 2 months, depending on the pharmacokinetic properties of the selected LAI and the patient’s clinical response.
Clinical outcomes
We measured the YMRS severity scores of patients treated with LAI antipsychotics during follow-up appointments at 4, 8, 16, 24, 32, 40, and 48 weeks. Functional status was evaluated based on the percentage of patients who could return to school, college, or work. The presence of suicidal ideation was measured both before and 48 weeks postintervention. The incidence of depressive episodes during the 48-week follow-up period was also recorded as part of the clinical outcomes in the study population.
Data analysis
Descriptive statistics were used to summarize the demographic and clinical characteristics. Continuous variables, such as age, duration of illness, BMI, and YMRS scores, were reported as means. Categorical variables, such as gender, race, diagnosis, and treatment details, were presented as percentages. The analysis aimed to provide a comprehensive overview of the patient population and the impact of LAI antipsychotic treatment on clinical outcomes.
Results
Trends in YMRS score over time
In this cohort of 116 adolescent patients with BD, treated with LAI antipsychotics, the mean YMRS score decreased from 33.8 at baseline to 21.7 at 4 weeks, 12.33 at 8 weeks, 6.53 at 16 weeks, 4.93 at 24 weeks, 4.09 at 32 weeks, 3.33 at 40 weeks, and 3.01 at 48 weeks (Table 1). The continuous trend of YMRS score reduction showed a consistent decline over the 48 weeks. Trends were similar across age groups, with consistent reductions observed in each age category from 13 to 17 years (Fig. 1). The most notable decrease occurred within the first 16 weeks of treatment, with a continued but more gradual decline after that. These trends remained consistent when stratified by age.
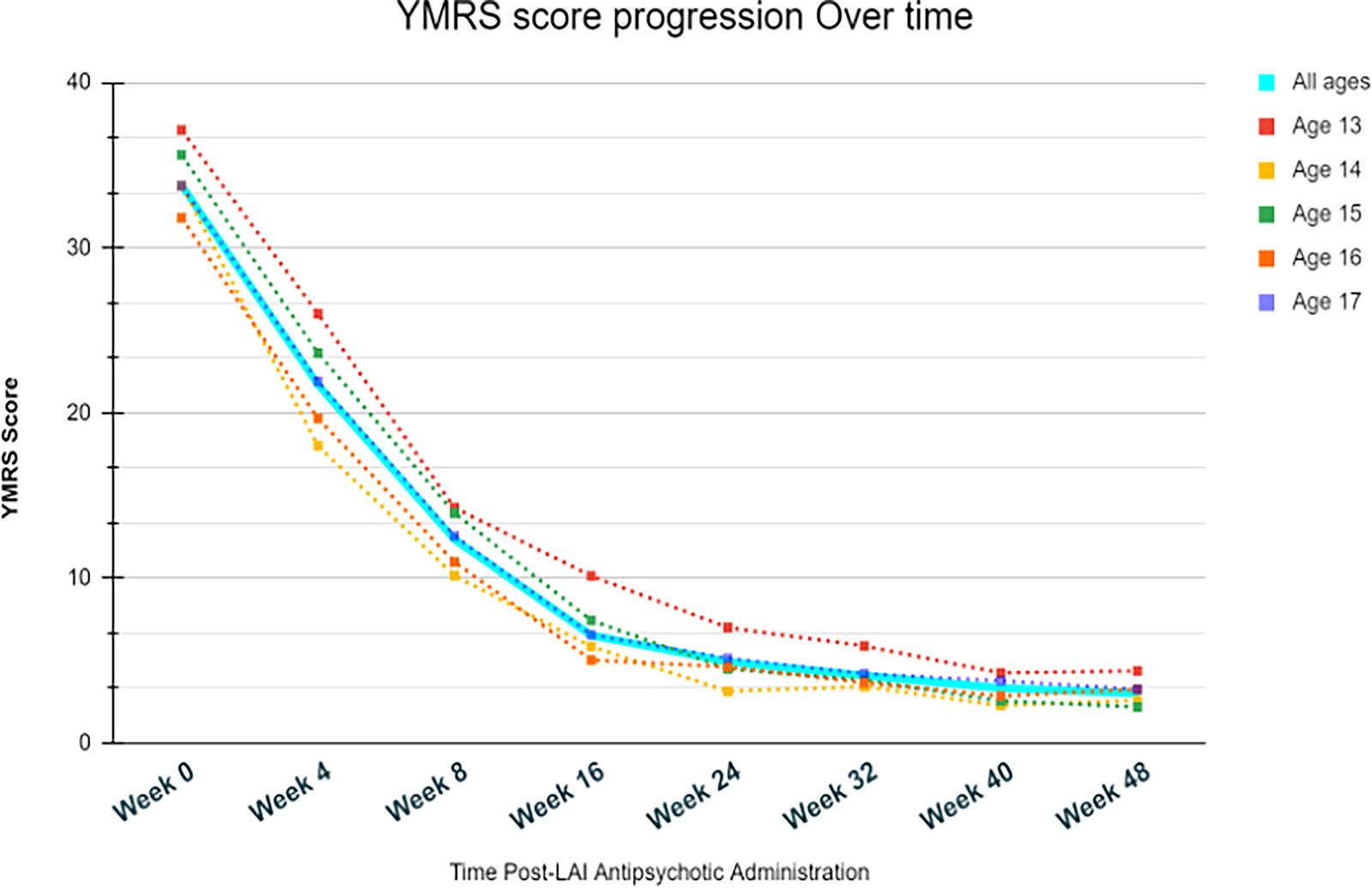
Trajectory of YMRS scores over 12 months following initiation of LAI antipsychotics. LAI, long-acting injectable; YMRS, Young Mania Rating Scale.
Young Mania Rating Scale Score Progression Stratified by Age
Scores represent mean values stratified by age group. Week 0 denotes the baseline. The data reflect YMRS scores at subsequent follow-up weeks (weeks 4, 8, 16, 24, 32, 40, and 48). The values represent the mean YMRS score for each age group at each time point. The “All ages” row represents all participants’ aggregated mean YMRS scores across the specified follow-up weeks.
YMRS, Young Mania Rating Scale.
Comorbid psychiatric condition
In our cohort of 116 adolescents diagnosed with BD, a significant proportion of patients also suffered from other psychiatric conditions. Substance-use disorders were the most prevalent, affecting 47.4% (n = 55) of the patients. Attention-deficit/hyperactivity disorder (ADHD) was present in 36.2% (n = 42) of the cohort, while social anxiety was identified in 18.1% (n = 21) of the patients. Generalized anxiety disorder (GAD) was diagnosed in 17.2% (n = 20) of the adolescents. The prevalence of panic disorder, obsessive-compulsive disorder (OCD), and Post-Traumatic Stress Disorder (PTSD) were 12.06% (n = 14), 5.1% (n = 6), and 4.3% (n = 5), respectively. Substance-use disorders were more prevalent among males, whereas OCD was more frequently observed in females. The prevalence rates for ADHD and GAD were similar across both genders.
Adverse effects
The most common side effects included increased appetite (n = 43, 37.1%), weight gain (n = 34, 29.3%), and restlessness (n = 13, 11.2%). Muscle stiffness was reported in 19 patients (16.4%) and drooling (n = 6, 5.1%). Hypersexuality as a side effect was observed in two patients (1.7%).
Due to uncontrollable side effects, 14 patients (12.1%) required a switch from one LAI antipsychotic to another. Specifically, the transition from paliperidone to aripiprazole was prompted by drooling, while the switch from aripiprazole to paliperidone was due to restlessness. These side effects could not be managed even with appropriate treatment adjustments, necessitating the change in LAI antipsychotics.
The mean BMI increased from 23.4 kg/m2 at baseline to 26.3 kg/m2 at the 48-week follow-up, reflecting the weight gain associated with all LAI treatment.
Other clinical outcomes
Among the 116 patients, 86.2% (n = 100) showed sufficient improvement to return to their previous educational or occupational settings. Before the initiation of LAI antipsychotic treatment, 33% (n = 38) of patients had a history of suicide ideation. During the 48-week follow-up, 4.3% (n = 5) reported new or continued suicide ideation, with no completed suicides recorded over the follow-up period. Furthermore, 28.4% (n = 33) of patients experienced depressive episodes after starting treatment. These episodes were documented through clinical assessments and patient self-reports.
Discussion
Our cohort of adolescents with BD treated with LAIs demonstrated very good clinical and functional outcomes. This is important because BD is often associated with deleterious impacts on the lives of patients, their families, and their communities. Early-onset BD, which occurs in individuals younger than 18 years, is associated with a more guarded prognosis compared with adult-onset BD (Young et al., 1978). This condition is often underdiagnosed, and even when diagnosed, adolescents may be reluctant to adhere to treatment or seek help due to stigma and peer pressure (Saxena et al., 2020). Early-onset BD frequently presents with more severe features, including increased psychotic symptoms, higher rates of substance abuse, comorbid conditions such as panic disorder and OCD, rapid mood cycling, diminished response to lithium, and a higher risk of suicide attempts (Taddeo et al., 2008). However, with timely and appropriate medication management, the need for hospitalization can often be mitigated, improving overall outcomes for these patients.
Genetics play a key role in early-onset BD, which makes inquiring about family history quite relevant (Youn et al., 2022). It is important to gather this information during the initial visit to make an adequate diagnosis. Our study had 16.3% adolescent patients who had first-degree and 31.5% had second-degree family history of BD. Although there are no major differences in the genetics between early- and late-onset BD, various environmental and developmental factors also play a significant factor in the development of symptoms.
Early-onset BD has been linked to severe cognitive deficits (Escamilla and Zavala, 2008). Adolescents with BD often exhibit smaller amygdalas, reduced hippocampal volumes, decreased gray matter, and thinner cortices in the prefrontal cortex compared with healthy controls (Biuckians et al., 2007). A recent study that compared healthy controls with BD patients found that attention was significantly affected in adolescents and adults regardless of the stage of their disease (euthymic phase, manic phase, or depressive phase) (Ching et al., 2022). Interestingly, a study found that adolescents with BD (14–17 years old) had persistent impairments in attention during remission and had poor cognitive function compared with healthy peers (Huang et al., 2023). In addition, the attention impairment of BD patients during manic episodes was worse. This also can lead to social impairment, poor academic performance, and an increase in risk-taking and grandiose behavior in the adolescent population.
This study cohort includes 42 patients (36.2%) who had comorbid diagnoses of ADHD and 20 patients (17.2%) with GAD. These additional diagnoses present complexities in managing BD, as ADHD symptoms can exacerbate mood instability and GAD can complicate anxiety management. Patients with comorbid ADHD displayed high levels of irritability, increased motor activity, rapid speech, grandiosity, and disruptive behavior during the initial visit. YMRS was administered at multiple points following the initial visit to evaluate the effectiveness of the treatment.
The presence of comorbid conditions complicates treatment strategies as stimulants used to manage ADHD can potentially exacerbate manic episodes in BD (Mendez et al., 2020), necessitating a priority on mood stabilization with mood stabilizers or controlling an acute episode with second-generation antipsychotics before addressing ADHD symptoms. A multidisciplinary approach involving medication management, psychosocial interventions, and ongoing monitoring is essential for improving outcomes and managing the complexities associated with these co-occurring conditions.
Adolescents’ ongoing maturation in decision-making and impulse control poses challenges to consistent adherence to medication regimens. BD disrupts cognitive development, potentially leading to lasting implications for reduced functional capacity (Hossain et al., 2019) This may stem from a direct impact of the illness on brain function or from indirect consequences of medications or substances. The intricate interplay of cognitive and emotional development during adolescence complicates the diagnosis and treatment of BD. Resistance to treatment may arise from an adolescent’s relentless pursuit of independence and identity formation.
While managing BD in adolescents with LAI or oral antipsychotics, understanding the relationship between obesity and the severity of the condition is crucial. Although recent data from the U.S. general population (Patel et al., 2018) suggest that the prevalence of obesity among adolescents with BD is not significantly higher than their peers, it is linked to more severe manifestations of the disorder, such as increased suicide attempts and higher rates of psychiatric admissions (Goldstein et al., 2011). In our study, the mean baseline BMI of the adolescent participants on LAI treatment increased from 23.4 to 26.6 kg/m2, but it is a reasonable cost to restore long-term stability in BD, which can be highly disrupting, even fatal.
Early diagnosis and treatment with an antipsychotic approved for BD by the FDA can reduce cognitive decline to some extent. However, lack of insight about their condition and future consequences is often associated with low medication adherence and poorer results.
While LAIs ensure adherence and improve symptom control, certain antipsychotic medications used in LAI formulations are associated with weight gain (Verdoux and Bourgeois, 1993). This can be due to metabolic side effects such as increased appetite and changes in fat metabolism. Elevated BMI is a concern because it can lead to additional health issues, such as diabetes and cardiovascular disease, which are already prevalent in individuals with BD (Singh et al., 2012). Balancing the benefits of improved mood stability and the potential for weight gain requires careful management. Regular monitoring of BMI and metabolic health, along with lifestyle interventions, can help mitigate the risk of significant weight gain while maximizing the therapeutic benefits of LAIs.
Lithium remains the gold standard medication for long-term prophylaxis of BD (Priya and Moorthy, 2021). However, abrupt discontinuation of lithium is associated with an increased risk of relapse (Tuplin and Holahan, 2017). Oral or injectable antipsychotic medication is the mainstay of treatment for effective management of acute BD. These drugs reduce symptoms in the acute phase and, when used as a maintenance treatment, prevent relapse. It is also important to consider their potential side effects as antipsychotics. Despite being relatively rare, hypersexuality has emerged as a significant concern, with 1.7% of patients in our study reporting this side effect while on aripiprazole LAI treatment. Patients required a multicenter approach, insight, and an add-on 5-alpha reductase inhibitor to manage hypersexuality. None of the patients was required to switch from one LAI to another due to this adverse effect.
An overview of trends in research (Spoorthy et al., 2019) reported a 24-year-old male who was treated with oral and injectable aripiprazole for management of psychoses in schizophrenia. Aripiprazole, a commonly prescribed second-generation antipsychotic for schizophrenia and BD, has a unique pharmacological profile as it functions as a partial agonist at the dopamine D2 receptor, a partial agonist at the 5-HT1A receptor, and an antagonist at the 5-HT2A receptor (Grover et al., 2020). Research indicates that medications with partial dopaminergic agonistic activity, such as aripiprazole, may be associated with compulsive behaviors, including pathological gambling, compulsive eating, compulsive shopping, and hypersexuality (Grover et al., 2023).
While predicting who will develop such behaviors is challenging, individuals with a personal or family history of OCD, impulse control disorders, impulsive personality traits, alcoholism, drug abuse, or other addictive behaviors are considered at higher risk for these impulsive side effects (Perlis et al., 2006). By maintaining a comprehensive approach that includes patient education and family involvement, health care providers can effectively manage hypersexuality and enhance overall treatment outcomes.
Following effective management of acute bipolar phase with an oral or injectable antipsychotic and initiating mood stabilization, patients may experience residual depressive or manic symptoms. The persistence of these symptoms can affect overall functioning and quality of life, indicating that while LAIs are beneficial, they may not fully address all aspects of mood regulation (Deas, 2006). Our study reported that 28.4% of patients developed depressive episodes while being treated with an LAI. The treatment for residual depression post-LAI in adolescents focuses on the adjustment of treatment plan and a personalized approach.
In a multicentric cross-sectional study in India involving patients in clinical remission across 14 centers, residual symptoms were assessed using the Hamilton Depression Rating Scale (HDRS) and YMRS (Regier et al., 1990). Residual symptoms were defined as scores of more than 7 on both scales. The findings revealed that 79.8% of participants had residual symptoms, with 16.8% experiencing only depressive symptoms, 9.6% only manic symptoms, and 53.4% showing both residual depressive and manic symptoms. The occurrence of these symptoms was linked to the polarity of the most recent episode and lifetime predominant polarity, with a higher number of lifetime depressive episodes correlating with increased residual depressive symptoms, and more lifetime manic episodes associated with a greater likelihood of residual manic symptoms (Sonne and Brady, 2024). The study highlights that a significant proportion of BD patients continue to experience residual symptoms even during remission, underscoring the need for clinicians to actively identify and manage these residual symptoms to enhance treatment outcomes.
The co-occurrence of alcoholism and BD in adolescents presents a complex clinical challenge with significant implications for diagnosis, treatment, and long-term outcomes. Adolescents with BD are at an elevated risk of developing substance-use disorders, including alcoholism, which can complicate the management of both conditions (Grunze et al., 2021). The ECA study (Cerullo and Strakowski, 2007) revealed that 60.7% of people with bipolar I disorder had a lifetime diagnosis of a substance-use disorder (i.e., an alcohol or other drug use disorder), 48% with bipolar II disorder had a substance-use disorder, 39.2% had an alcohol-use disorder, and 21% had a drug abuse or dependence diagnosis (these figures reflect that overlap patients were concurrently on substance/alcohol/other drugs).
Individuals with alcoholism are more likely to experience mood disorders, including BD and conversely, adolescents with BD are at a higher risk of developing alcohol-use disorders. This bidirectional relationship exacerbates both conditions and complicates treatment. Alcohol is often used as a form of self-medication by individuals with BD to manage mood symptoms, particularly during depressive phases. However, alcohol use can worsen mood instability and interfere with the effectiveness of bipolar treatment.
Modern treatment concepts acknowledge the interplay between these disorders using an integrated therapy approach where they are both tackled in the same setting by a multiprofessional team. Motivational interviewing and cognitive behavioral and sociotherapies incorporating the family and social environment are cornerstones in psychotherapy, whereas the accompanying pharmacological treatment aims to reduce craving and optimize mood stability.
Parents and caregivers’ observations:
Caregivers and parents of adolescents with BD, who transitioned from oral medications to LAI medications to address issues of noncompliance, provided detailed feedback through interviews conducted at 4-week intervals. They observed several notable benefits from the switch to LAIs. Parents reported that the less frequent administration schedule of LAIs substantially improved their children’s medication adherence, reducing the daily challenge of managing oral medications. This improved adherence was associated with greater stability in their children’s mood and behavior. Caregivers noted that their children demonstrated enhanced functionality, with improvements in daily activities, academic performance, and social interactions. The switch also alleviated some of the stress and burden previously associated with ensuring daily medication adherence, leading to a more manageable and less stressful home environment. This off-label use of LAIs facilitated more effective communication with health care providers, as regular follow-ups with LAI treatments allowed for more comprehensive discussions about treatment progress and emerging concerns. Some parents expressed concerns regarding potential side effects and the need for ongoing support and education about the LAI regimen. Despite these concerns, the overall feedback was positive, indicating that LAI medications were effective in improving adherence, symptom management, and overall treatment outcomes for adolescents with BD.
To our knowledge, this is the largest reported sample of adolescents with BD treated with LAIs. Our clinical data reveal that treatment with LAI antipsychotics led to substantial stabilization in 116 adolescents with bipolar mania or Social Anxiety Disorder (SAD) -bipolar type, evidenced by a sharp decline in YMRS scores and a high rate of remission and functional recovery. Although LAI antipsychotics are not yet FDA-approved for patients younger than 18 years, our compassionate off-label use of LAI therapy in these high-risk adolescents showed excellent efficacy, tolerability, and long-term clinical stability, along with a significant return to functional improvement.
FDA clinical trials are warranted for LAI antipsychotic formulations in adolescents with bipolar mania to effectively address the clinical needs of this highly nonadherent and relapse-prone patient group.
Our study reveals that LAIs significantly reduced symptoms, high remission rates, and successful returns to school or work. The results also highlight the potential efficacy and tolerability of LAI antipsychotics in adolescent patients, offering a promising approach for achieving long-term clinical stability. In addition, the findings of this study suggest that LAI antipsychotics will offer solutions for adolescents who struggle to adhere to oral medications. Our article illuminates how successful LAIs are for the treatment of adolescents with bipolar. While these results are encouraging, further research is needed to understand better the long-term efficacy of LAIs in managing BD in younger populations.
Conclusion
LAI medications for BD offer promising potential to mitigate cognitive decline, primarily through enhanced medication adherence and mood stabilization. By providing consistent, less frequent dosing, LAIs help ensure that patients maintain steady therapeutic levels, which can lead to more stable mood control and reduced frequency of mood episodes. This stability is crucial for cognitive health, as frequent mood episodes often exacerbate cognitive impairments. Furthermore, stable mood management with LAIs may offer indirect cognitive benefits by reducing the cognitive disruptions associated with acute mood states. Although some antipsychotics in LAI formulations may have neuroprotective effects [36], more research is needed to confirm the direct impact of LAIs on cognitive functioning. Overall, while LAIs present a valuable tool for improving adherence and mood stability, their effect on cognitive decline in BD remains an area of active investigation.
Footnotes
Author Disclosure Statement
The authors declare that there are no conflicts of interest related to the content of this article. The views expressed are those of the authors and do not reflect the opinions of any affiliated institutions or organizations.No competing financial interests exist.
Authors’ Contributions
Parinda Parikh, MD, contributed to the study conceptualization, design, data collection, and analysis. Kanuja Sood assisted with data collection and contributed to the writing of the manuscript. Lajpat Rai Bansal played a role in the study design, did the data collection process, conducted data analysis, and contributed to the interpretation of results. Jeby Abraham contributed to literature review and manuscript drafting. Anjali Eichbaum helped with data collection and manuscript revisions. Enfu Keith Shoda provided statistical analysis and assisted with data interpretation. Mahiya Buddhavarapu supported the study design and contributed to manuscript revisions. Mina Oza was involved in data analysis and manuscript drafting. Arushi Parikh Chandra contributed to manuscript revisions and analysis of the study results. Channa Simanowitz assisted with data collection and provided critical revisions to the manuscript. Martin Witriol helped with statistical analysis and interpretation of results. Henry Nasrallah supervised the study, provided recommendations, and reviewed the final manuscript.
Funding Information
No funding was received for this article.