
Abstract
Objectives:
Bipolar disorder (BD) in adolescence often associates with risky conducts, nonsuicidal self-injury (NSSI), and suicidal ideation. Lithium salts represent the first-line choice for BD in youth to manage manic symptoms and prevent both manic and depressive relapses. Our study aimed to assess efficacy and tolerability of extended-release lithium sulfate (ERLS) in youths with BD.
Methods:
A longitudinal perspective intervention study was thus conducted on a single cohort of 36 patients with BD aged 12–17 years treated with ERLS and followed up for 1 year. ERLS was titrated up to reach optimal plasma concentrations during the 3 months before baseline visit (T0). Then, patients underwent five follow-up visits after 1, 2, 3, 5, and 11 months and were administered with a battery of self- and parent-rated questionnaires and interviews to evaluate, at each timepoint, ERLS-related side effects, manic and depressive symptoms, emotional dysregulation (ED), NSSI and suicidality, and aggressiveness. Regular clinical assessments were also conducted, as well as blood tests, urinalysis, and EKG. Regression models were applied to examine the time course of outcome variables.
Results:
Twenty-four patients completed the follow-up. Regressions showed a significant reduction of most dependent variables included in the models, including depressive symptoms (β = –0.0006; adj-p = 0.0007), aggressiveness (β = –0.0031; adj-p < 0.0001), ED (β = –0.0002; adj-p = 0.0497), and unstructured suicidal ideation (β = –0.0058; adj-p = 0.0340). Fine distal tremor, increased thirst, and diuresis were among the most frequently reported side effects.
Conclusions:
Findings from the present study support the use of ERLS as an effective and well-tolerated agent for the management of BD in youth, with a beneficial effect on associated severe symptoms, including NSSI and suicidality.
Introduction
Lithium was the first medication shown to be effective in treating mood disorders and remains commonly used for various psychiatric conditions in both adults and young people (Pisano et al., 2019). Extensive research has demonstrated its success in managing mood disorders in adults, providing significant clinical effectiveness against both depression and mania within bipolar disorder (BD) (Miura et al., 2014), and reducing the risk of suicide (Cipriani et al., 2013). For children and adolescents, lithium has been approved by the major regulatory agencies, including the Food and Drug Administration and the European Medicines Agency, for treating BD (Tueth et al., 1998). Albeit a high worldwide prevalence of BD in youth, up to 3.4% (Van Meter et al., 2019), less evidence supports efficacy of lithium in youth (Findling et al., 2015; Findling et al., 2013; Findling et al., 2005), particularly for what concerns its renowned effects in reducing suicidality and self-harming (Hauser et al., 2013).
A previous meta-analysis (Liu et al., 2011) on treating pediatric mania found lithium effectiveness unclear, largely due to the lack of double-blind studies at the time, with more promising outcomes reported for second-generation antipsychotics (SGAs). A more recent comprehensive review (Pisano et al., 2017) found a level 1b of evidence of effectiveness for lithium treatment on mania in pediatric BD [e.g., (Findling et al., 2015; Geller et al., 2012)], in line with the conclusions of a more recent systematic review (Duffy et al., 2018), suggesting that lithium may be an effective and tolerable treatment at least for some forms of pediatric mania. Indeed, lithium is clearly inferior in efficacy to risperidone in prepubertal patients diagnosed with protracted manic/mixed episodes and comorbid attention-deficit/hyperactivity disorder (ADHD) (Duffy et al., 2018), whereas a recent network meta-analysis confirmed that SGAs outperform lithium for manic symptom reduction and mania response in the acute treatment in children and adolescents (Vita et al., 2024).
Instead, less conclusive evidence is available for treating depression with highly suggestive studies providing an overall level 2b of evidence (Patel et al., 2006; Salpekar et al., 2015). Moreover, some long-term studies support its use in relapse prevention (Findling et al., 2013; Findling et al., 2005). Interestingly, recently published data from large longitudinal studies suggest potential clinical benefits of lithium in reducing or preventing suicide risk in youth with BD, but these findings are not yet comprehensive. For instance, in 2019, the Course and Outcome of Bipolar Youth (COBY) study (Hafeman et al., 2020) examined 340 youths with BD over 10 years and found that those on lithium had fewer suicide attempts than those on other mood stabilizers. Similarly, a study conducted on the Swedish national registries in 2023 (Desai Boström et al., 2023) found that higher use of lithium was associated with lower suicide rates compared with other treatments. Parasuicidal behaviors, including nonsuicidal self-injury (NSSI), might also benefit from lithium treatment, although evidence is still scarce and based on cross-sectional studies (Jerrell, 2008; Ko et al., 2014).
Theoretically, lithium may exert its antisuicidal effects by reducing relapses of mood disorder, but additional mechanisms should also be considered, especially in youth, since there is some evidence that lithium decreases aggression and possibly impulsivity, which might be another mechanism mediating its antisuicidal effect (Cipriani et al., 2013). Since adult patients taking lithium showed reduced self-harm and unintentional injury rates compared with those prescribed with other drugs, including valproate, quetiapine, and olanzapine (Hayes et al., 2016), lithium use might prevent suicidality by reducing impulsive aggression in addition to stabilizing mood. It has been hypothesized that the effectiveness of lithium treatment in preventing suicide is likely associated with reduced impulsivity and aggression often associated with dysphoric, agitated, and mixed states, which are particularly vulnerable to suicidal outcomes (Tondo and Baldessarini, 2016). In other words, lithium may promote its antisuicidal properties via reinforcing top-down brakes of impulsive actions, whereas, since even natural lithium intake in drinking water can influence impulsivity and suicidality (Kugimiya et al., 2021), speculatively, a lithium “deficiency state” may precipitate these situations (Giotakos, 2018). In line with this association between reduced impulsivity and aggressiveness and suicide prevention, lithium is also useful in patients with a variety of disorders featured by impulsivity and aggression (Sampogna et al., 2022). Indeed, several studies found that lithium is effective in reducing impulsive aggression and temper outbursts in severely violent and hostile conduct disorder youth, being significantly superior to placebo (Malone et al., 2000) either in monotherapy or in add-on with atypical antipsychotics (Masi et al., 2009).
Notably, emotional dysregulation (ED), including affective impulsivity and emotional reactivity, may represent another key factor underlying suicidality in developmental BD spectrum (Kulacaoglu and Izci, 2022). Indeed, temperamental features, and specifically cyclothymic-hypersensitive temperament, and ED may represent independent factors for increased vulnerability to persistent suicidal ideation not only in adults (Janiri et al., 2021) but also in youth (Masi et al., 2023) with BD. Unfortunately, direct evidence of efficacy of lithium treatment on clinical measures of ED based on randomized controlled trials or naturalistic studies is still missing. Nonetheless, scholars are now claiming the need for further research on the topic, as well as for evidence-based guidelines, to prevent potential missed opportunities for use of lithium among high-risk BD adolescents with ED symptoms and suicidality (Ko et al., 2014).
This is especially true when considering that, compared with other psychotropic medications, lithium has been found to be safe and tolerated both in adults and youths. Importantly, recent guidelines (Duffy and Grof, 2018; Yatham et al., 2018) confirm that lithium is reasonably well-tolerated for BD children and adolescents both as acute and maintenance treatment, although some safety concerns require monitoring. Thyroid and renal function need, as well as plasma calcium and cardiac rhythm (i.e., QT prolongation), should be assessed at least annually, especially for those on maintenance therapy, and lithium plasma levels should be carefully monitored to prevent toxicity (Yatham et al., 2018). Common side effects may include gastrointestinal symptoms (i.e., nausea, vomiting, and diarrhea), skin conditions (e.g., acne), and mild tremor. Nonetheless, these effects are generally accepted by the young patients, especially when long-term efficacy is observed, and the overall tolerability profile is much more convenient and cost-effective than that reported by other medications (e.g., antipsychotics) in terms of metabolic, neurological, and cognitive sequelae.
Thus, aim of the present study was to evaluate the efficacy of extended-release lithium sulfate (ERLS), a formulation not yet explored in youth, for the treatment of manic and depressive symptoms, as well as to assess its effectiveness on suicidality and self-harming, as well in hostility, aggression, and ED in a longitudinal sample of referred youths with BD.
Materials and Methods
Study design and aims
We conducted a longitudinal, prospective, single-cohort intervention study. The primary aim of this study was to corroborate previous evidence on effectiveness of the treatment with ERLS on clinical measures of depression, mania, aggression, and suicidality in adolescents with bipolar spectrum disorder over 1-year follow-up. We hypothesized that lithium therapy was effective in improving depressive/manic symptoms, decreasing suicidality, and reducing aggressiveness. Secondary aims included (a) exploring the efficacy of lithium salts on clinical measures of substance use, ED, and other psychopathological domains and (b) assessing its tolerability over time. This study was conducted in accordance with the Declaration of Helsinki and approved by the Regional Ethics Committee for Clinical Trials of Tuscany (Pediatric Ethics Committee at Meyer Children’ Hospital of Florence—date of approval: November 4, 2021—protocol code: Lit2020).
Recruitment
Participants were enrolled in this single-center study at our third-level hospital from October 2021 to May 2023. Patients were consecutively assessed at the Department of Child and Adolescent Psychiatry and Psychopharmacology of our hospital for eligibility. Those who met the eligibility criteria listed below were included following a thorough clinical screening. All participants and their caregivers were informed about the assessment procedure, and participation in the study was voluntary. Recruited patients and their parents were asked to provide their signed informed consent. In addition, patients were allowed to retrieve their consent any time during the study.
Inclusion criteria were as follows: adolescents aged 12–18 years; diagnosis of bipolar or related disorders [bipolar disorder type I (BD-I), bipolar disorder type II (BD-II), cyclothymic disorder, Other specified or unspecified bipolar disorder]; either no other psychotropic drug or under stable treatment with other psychotropic drugs for at least the last 6 weeks before baseline visit (T0); no current treatment-related side effects; informed consent obtained from the patient and both caregivers; and if sexually active fertile female, under contraceptives or with negative urinary pregnancy testing. Exclusion criteria were as follows: borderline cognitive functioning or intellectual disability, diagnosis of schizophrenia spectrum and other psychotic disorders, novel or unstable treatment with any psychotropic drugs in the last 6 weeks, any acute or unstable medical condition that may prevent study participation, and pregnant or breastfeeding.
Procedures
Participants were first thoroughly assessed for eligibility. Diagnoses were made according to the Diagnostic and Statistical Manual of Mental Disorders—Fifth Edition (DSM-5), based on medical history, clinical observations, and psychiatric interviews administered by trained child psychiatrists to both patients and parents. Cognitive functioning was determined based on medical history or by administering the Wechsler Intelligence Scales according to the patients’ age (Full-Scale Intelligence Quotient ≥ 85). Urinary pregnancy testing was performed whenever required. Those who were considered eligible were provided with details concerning the assessment procedures expected during the study and subsequently asked to sign the informed consent. Then, ERLS was prescribed and titrated over a 3-month period until dosage stabilization.
After 3 months of lithium titration and dosage stabilization, study visits were scheduled as follows. The baseline visit (T0) was followed by four follow-up visits approximately after 4 (T1), 8 (T2), 12 (T3), and 20 (T4) weeks, respectively, and a final visit (T5) after 24 weeks from T4. Criteria for study withdrawal were as follows: informed consent withdrawal from the patients or their caregivers; early discontinuation of lithium treatment; lithium dosage modification during the first 12 weeks after T0; unstable treatment with any other psychotropic drugs during the first 12 weeks; and occurrence of moderate-to-severe side effects due to lithium treatment.
At all visits (T0–T5), patients underwent a full clinical assessment, including history update, physical and neurological examination, acquisition of physical and vital parameters (i.e., weight, height, blood pressure, heart frequency), as well as blood sampling and EKG. At all visits (T0–T5), a battery of clinical questionnaires and interviews was completed, including the Child Behavior Checklist for ages 6–18 (CBCL—6/18), the Modified Overt Aggression Scale (MOAS), the Young Mania Rating Scale (YMRS), the Children Depression Rating Scale (CDRS), the Columbia-Suicide Severity Rating Scale (C-SSRS), the Deliberate Self-Harm Inventory (DSHI), the Lithium Side Effects Rating Scale (LiSERS), and the Abnormal Involuntary Movement Scale (AIMS). At T0, T4, and T5, patients were also administered a semi-structured clinical interview based on DSM-5 criteria, the Kiddie Schedule for Affective Disorders and Schizophrenia-Present and Lifetime version (K-SADS-PL).
Blood sampling and EKG
Blood sampling was performed on the day of each visit in the morning through venipuncture. Blood tests included lithium plasma levels, complete blood count, glucose, triglycerides, cholesterol, blood urea nitrogen, creatinine, serum electrolytes, liver enzymes, creatine phosphokinase (CPK), amylase, free thyroid hormone 3, free thyroid hormone 4, and thyroid-stimulating hormone (TSH). Routine urinalysis was also performed. Resting EKG was performed before the visit and examined by expert cardiologists to provide the following parameters: heart frequency, P wave duration, PR interval duration, QRS interval duration, and QT and corrected QT interval duration.
Clinical measures
At each visit, parents or caregivers filled in the CBCL—6/18 questionnaire, a 118-item scale with eight syndrome scales, six symptom scales, and three broadband scores designated as Internalizing, Externalizing, and Total Problems, as well as a Dysregulation Profile Index (CBCL-DPI) computed as the sum of T-scores of three syndrome scales, namely, Anxiety/Depression, Attention Problems, and Aggressive Behaviors. The following clinical questionnaires and interviews were administered at each visit to the patients by trained child psychiatrists: C-SSRS: a suicide risk screening tool that supports clinical assessment through a series of simple, plain-language questions and helps clinicians to identify whether patients are at risk for suicide by estimating the severity and immediacy of the risk; the scale provides a nominal index representing the presence or absence of Unspecified (Uns-SI) and Active (Act-SI) Suicidal Ideation, as well as of Suicidal Behavior (SB). DSHI: a 17-item self-report questionnaire developed to assess deliberate self-harm, which is behaviorally based and evaluates several different types of deliberate self-harming behaviors; it provides a nominal index of the presence or absence of NSSI behaviors.
The following scales were rated by clinicians based on parents’ and patients’ reports: MOAS: a 4-item rating scale aimed to assess four types of aggressive behavior over the past week on 5-point scores, including verbal aggression, aggression against property, auto-aggression, and physical aggression, that provides a global score ranging from 0 to 40 computed according to the severity of the aggression type. YMRS: a 11-item clinical scale developed to rapidly and easily assess the severity of manic symptoms over the past 48 hours on 5-point scores (7 items are rated 0 – 1 – 2 – 3 – 4, 4 items are rated 0 – 2 – 4 – 6 – 8) for either screening or staging manic states to help guide clinicians on treatment planning and progress based on the total score. CDRS: a reliable, clinician-rated scale to assess depression in youth by providing an estimate of depressive symptomatology based on 17 items ranging up to 5 or 7, which are rated by clinicians via interviews with the child and are ultimately summed up to compute a global score. LiSERS: a rating scale that provides an exhaustive list of possible symptoms related to lithium toxicity and side effects. AIMS: a 12-item clinician-rated scale to assess the occurrence and severity of involuntary movements and dyskinesias in different areas of the patient’s body.
Statistics
Statistical analyses were performed using RStudio® (version 1.3.1093, RStudio, PBC). The effect of treatment duration over the trend of primary and secondary outcomes was assessed by means of a series of generalized linear mixed-effects models (GLMMs) performed using lme4 package (glmer function). For each model, the visit time from T0 as continuous predictor of interest, whereas the follow-up visit (hereafter, timepoint), was used both as ordinal and categorical predictor of interest to corroborate former results, as well as to detect the specific timepoints in which significant effects were confirmed. Lithium dosage (in milligrams) and age (in years) were used as continuous covariates; gender (M > F), ongoing psychotherapy (yes > no), and ongoing treatment with other psychotropic drugs (yes > no) were used as categorical covariates; and patients’ identities, as well as rating clinicians, were used as random intercepts of the models. Poisson GLMMs were computed for outcome variables with discrete distribution and logistic GLMMs for binomial outcomes. Statistical significance was corrected for multiple comparisons based on the False Discovery Rate method (FDR-corrected p value <0.05). Linear mixed-effects models (LMMs) and logistic GLMMs were finally conducted to assess the effect of follow-up visit (i.e., timepoint) as categorical predictor over the trend of clinical outcomes of safety and tolerability, including reported side effects and clinical parameters and examinations.
Results
Participants
Fifty-seven patients [38 females (66.66%), 15.77 ± 1.44 years (12.33–17.75)] were initially screened to be included in the study. Of these, 21 patients [17 females (80.95%), 15.35 ± 1.74 years (12.67–17.58)] were not considered eligible due to the following exclusion criteria: no diagnosis of bipolar or related disorders (n = 2); other add-on psychotropic drugs during the last 6 weeks before T0 (n = 3); unstable treatment with other psychotropic drugs during the last 6 weeks before T0 (n = 4); acute medical condition (n = 1); no informed consent obtained from caregivers (n = 4); no informed consent obtained from the patient (i.e., poor compliance) (n = 5); and borderline cognitive functioning (n = 2).
Thus, 36 patients [21 females (58.33%), 16.01 ± 1.19 years (12.33–17.75)] were recruited at T0. Twelve patients were lost during the study due to the following reasons: informed consent withdrawal (n = 2); early discontinuation of lithium treatment (n = 5); unstable treatment with other psychotropic drugs during the first 12 weeks (n = 3); and occurrence of moderate-to-severe side effects (n = 2). Patients were lost at the following visits: two patients at T1 (n = 34); two patients at T2 (n = 32); one patient at T3 (n = 31); two patients at T4 (n = 29); and five patients at T5 (n = 24). Twenty-four patients [14 females (58.33%), 16.80 ± 1.25 years (13.17–18.17)] fully completed the study. The whole duration of the study was 48.71 ± 4.04 weeks (40.86–56.00), and the follow-up visit intervals were as follows: T0–T1 4.48 ± 0.54 weeks; T1–T2 4.49 ± 0.55 weeks; T2–T3 4.96 ± 0.99 weeks; T3–T4 10.62 ± 3.42 weeks; and T4–T5 24.18 ± 2.73 weeks. The flowchart in Figure 1 shows the process of screening, recruitment, and follow-up of patients. Baseline and follow-up visits were performed by two authors (F.P. and G.S.) in different proportions, 64.52% and 35.48%, respectively.
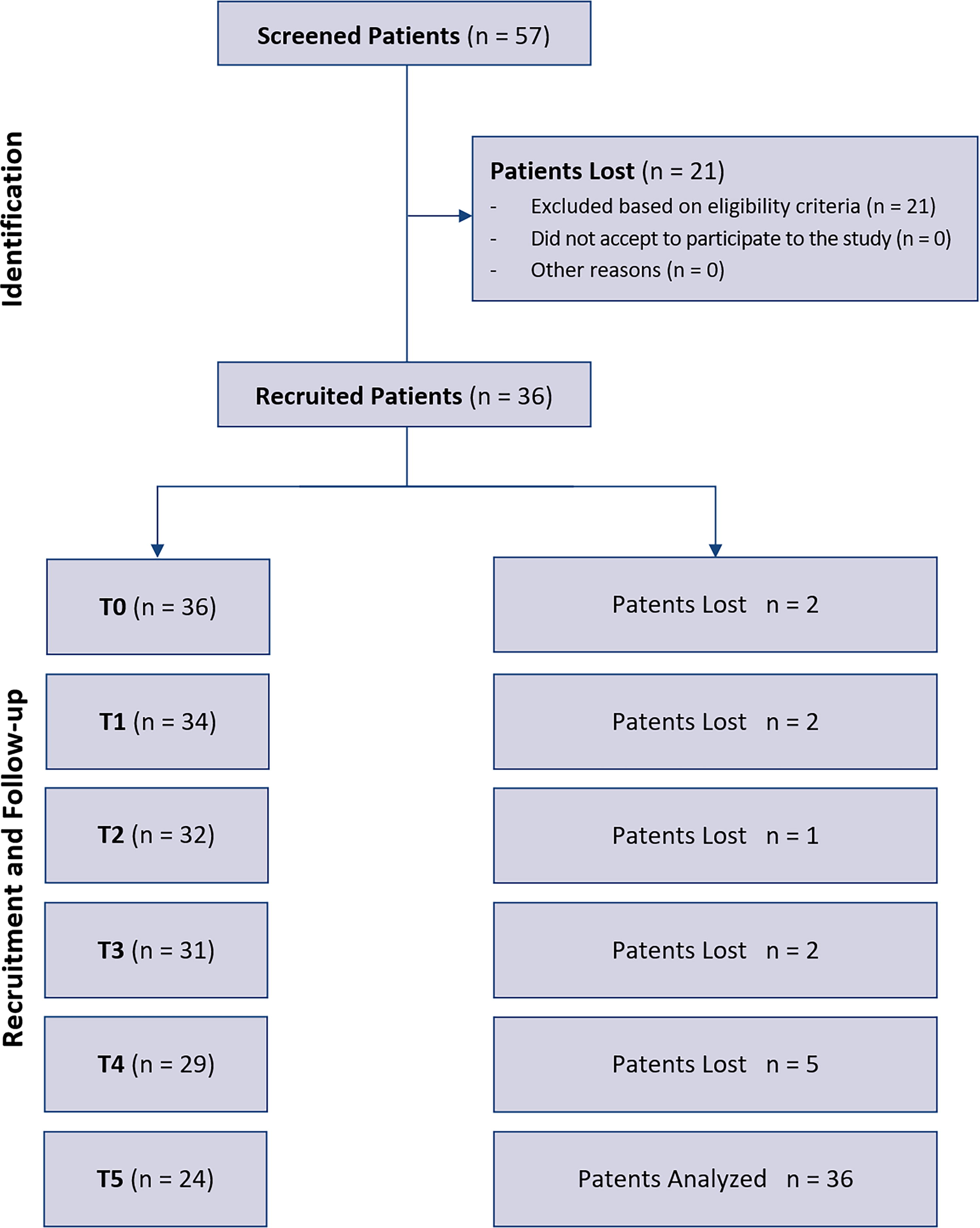
Flowchart of the study. The process of screening, recruitment, and follow-up of patients is here depicted.
Before recruitment, enrolled patients had received a diagnosis of a bipolar or related disorder based on the DSM-5 criteria as follows: n = 3 patients (8.33%) with BD-I; n = 10 patients (27.78%) with BD-II; n = 12 patients (33.33%) with cyclothymic disorder; and n = 11 patients (30.56%) with other specified-BD or unspecified-BD. At T0, 3 patients (8.33%) currently presented with a manic episode, 2 patients (5.55%) with a hypomanic episode, 13 patients (36.11%) with a major depression episode, and 4 patients (11.11%) with a depressive episode with mixed features based on the K-SADS-PL clinical interview. Recruited patients also exhibited the following comorbidities based on the K-SADS-PL clinical interview: n = 8 (22.22%) panic disorder; n = 10 (27.78%) separation anxiety disorder; n = 18 (50.00%) generalized anxiety disorder; n = 13 (36.11%) social anxiety disorder; n = 3 (8.33%) specific phobias; n = 3 (8.33%) obsessive–compulsive disorder; n = 2 (5.55%) Tics; n = 23 (63.89%); ADHD of whom n = 12 (33.33%) combined, n = 10 (27.78%) predominantly inattentive, and n = 1 (2.78%) predominantly hyperactive/impulsive; n = 5 (13.89%) oppositional defiant or conduct disorder; and n = 3 (8.33%) unspecified feeding and eating disorder. Clinical features of the sample are summarized in Table 1.
Clinical Features of the Sample
Raw numbers and percentages of patients displaying specific clinical features are here reported.
ADHD, attention-deficit/hyperactivity order.
ERLS dosages across timepoints were as follows: 142.11 ± 35.99 mg at T1; 142.29 ± 42.90 mg at T2; 141.10 ± 40.19 mg at T3; 147.56 ± 40.42 mg at T4; and 152.17 ± 38.05 mg at T5. Lithium plasma levels across timepoints were as follows: 0.58 ± 0.23 mmol/L at T1; 0.63 ± 0.23 mmol/L at T2; 0.60 ± 0.24 mmol/L at T3; 0.68 ± 0.20 mmol/L at T4; and 0.69 ± 0.23 mmol/L at T5. No lithium dosage was found to be over the toxic threshold of 1.20 mmol/L. Treatment with other ongoing psychotropic drugs included the following: antiepileptic mood stabilizers (i.e., valproic acid, lamotrigine); antidepressants (i.e., sertraline, fluoxetine, fluvoxamine, trazodone, mirtazapine); SGAs (i.e., lurasidone, quetiapine, aripiprazole, risperidone); psychostimulants (i.e., extended-release methylphenidate); and GABAergic agents (i.e., delorazepam, gabapentin).
Regression models
Regression analyses (see Table 2. A–V; see Supplementary Table S1 for confirmatory models with timepoint ordinal predictor, see Fig. 2A–I for specific timepoint effects with categorical predictor) showed a statistically significant negative effect of the regressor of interest “visit time from T0” on the MOAS (β = –0.0031, FDR-corrected p < 0.0001) and CDRS (β = –0.0006, FDR-corrected p = 0.0007) scales scores, as well as on the Anxious/Depressed (β = –0.0003, FDR-corrected p = 0.0175) and Anxiety Problems (β = –0.0003, FDR-corrected p = 0.0182) subscales scores and the DPI (β = –0.0002, FDR-corrected p = 0.0497) of the CBCL, indicating a significant reduction of scores on these clinical measures over time of treatment. A statistically significant negative effect was also found for the Uns-SI index of the C-SSRS (β = –0.0058, FDR-corrected p = 0.0034), whereas a non-FDR-corrected significant negative effect was detected for the NSSI index of the DSHI (β = –0.0063, p = 0.0292, FDR-corrected p = 0.1022), indicating a reduction in the amount of observations reporting presence of Uns-SI and NSSI over time of treatment. Similarly, a non-FDR-corrected significant negative effect was detected for the Affective Problems subscale score of the CBCL (β = –0.0003, p = 0.0200, FDR-corrected p = 0.0700). A non-FDR-corrected quasi-significant negative trend was found for the Act-SI and SB indexes of the C-SSRS, whereas no significant effect was reported for the YMRS and all the other CBCL subscales scores.

A–V. Regression Models
p < 0.05.
p < 0.01.
p < 0.001.
p < 0.0001.
Act-SI, Active Suicidal Ideation; ADHD, attention-deficit/hyperactivity disorder; CBCL, Child Behavior Checklist; CBCL—AB, Child Behavior Checklist-Aggressive Behaviors; CBCL—AD, Child Behavior Checklist-anxious/depressed; CBCL—Aff, Child Behavior Checklist-Affective problems; CBCL—Anx, Child Behavior Checklist-Anxious problems; CBCL—AP, Child Behavior Checklist-Attention Problems; CBCL—ODD, Child Behavior Checklist-Oppositional Defiant Disorder; CBCL—RBB, Child Behavior Checklist-Rule-breaking behaviors; CBCL—SC, Child Behavior Checklist-Somatic Complaints; CBCL—Som, Child Behavior Checklist-somatic problems; CBCL—SP, Child Behavior Checklist-Social Problems; CBCL—TP, Child Behavior Checklist-Thought Problems; CBCL—WD, Child Behavior Checklist-Withdrawn/Depressed; CDRS, Children Depression Rating Scale; C-SSRS, Columbia-Suicide Severity Rating Scale; DPI, Dysregulation Profile Index; DSHI, Deliberate Self-Harm Inventory; MOAS, Modified Overt Aggression Scale; NSSI, nonsuicidal self-injury; SB, Suicidal Behavior; Uns-SI, Unspecified Suicidal Ideation; YMRS, Young Mania Rating Scale.
AB, aggressive behaviors; Aff, affective problems; Anx, anxious problems; AP, attention Problems; ODD, oppositional defiant disorder; RBB, rule breaking behaviors; Som, somatic problems; SC, somatic complaints; SP, social problems; TP, thought problems; WD, withdrawn/depressed.
Safety and tolerability
Lithium treatment was generally safe and well tolerated. As previously reported, only two patients were lost during the study due to the occurrence of moderate-to-severe side effects, including one case of transitory severe hyperthyroidism with suppressed TSH plasma levels and subsequent hypothyroidism treated with hormone replacement therapy, plus one case of sudden massive increase of CPK plasma levels in a patient with add-on aripiprazole. Both cases remitted after lithium treatment interruption.
As for auxologic parameters, while weight and particularly height increased likely due to the expected developmental growth of adolescent patients, body mass index (BMI) was substantially stable across the timepoints, indicating no significant effect of lithium on body weight. Systolic and diastolic pressure, as well as heart frequency, were also stable over time (see Supplemental Supplementary Table S2).
Side effects of lithium treatment, as reported by the patients through the LiSERS, are also shown in Supplemental Supplementary Table S2. The most frequently reported across the timepoints were the following one: increased appetite; increased thirst; increased diuresis; dry mouth; fine tremors; headaches; thyroid symptoms (e.g., fatigue); feeling restless; nausea; and sickness. Nonetheless, reported side effects were generally mild, and only occasionally moderate, including the same most frequently reported ones as above (e.g., increased thirst and diuresis, thyroid symptoms, fine tremors) plus rare cases of moderate sweating, vomiting, sleep problems, psoriasis, and palpitations; only one patient at T1 reported severe thyroid symptoms with fatigue and palpitations. Importantly, increased appetite showed a significant decreasing trend over time (p = 0.0244 at T4; p = 0.0222 at T5), as well as increased thirst at T1 (p = 0.0257), whereas fine tremors significantly increased at T5 (p = 0.0498). All the other reported side effects displayed no significant effect of timepoints.
Findings from blood examinations, urinalysis, and EKG are finally reported in Supplemental Supplementary Table S2. Mean and SDs are presented across the timepoint, along with the percentage of patients displaying levels over or below the clinical thresholds. Clinical examinations exhibiting the highest percentages of patients with levels over or below the clinical thresholds across the timepoints were the following ones: high density lipoprotein cholesterol, low density lipoprotein cholesterol, alkaline phosphatase (ALP), TSH, uric acid, urine-specific weight, creatinine, and CPK. Effect of timepoints on the clinical examinations is reported as well. Notably, a trend in reduction of sodium and iron plasma levels was observed over time, as well as for ALP levels, whereas a significant increase was found for TSH levels at T3, for the corrected QT trait length at the EKG at T5, and the urine specific weight at T5.
Discussion
The present study aimed to evaluate the efficacy of ERLS in treating manic and depressive symptoms, suicidality and self-harming behaviors, and hostility/aggression in adolescents with BD. The findings provide valuable insights into the role of lithium in this younger population, which has been underexplored compared with adult cohorts. Our results indicate a statistically significant reduction in depressive symptoms and aggressive behaviors. These findings corroborate previous studies suggesting that lithium is effective in managing depressive symptoms (Patel et al., 2006) and reducing aggression in youths with BD (Malone et al., 2000; Masi et al., 2009). The improvement in these aspects is crucial, given that depressive symptoms and aggression are strongly associated with functional impairment and poor quality of life in patients with BD (Gitlin and Miklowitz, 2017).
Interestingly, no significant improvement was detected in manic symptoms, which does not align with previous studies in the same age range (Duffy et al., 2018; Findling et al., 2015; Geller et al., 2012; Pisano et al., 2019), showing that lithium may be an effective option for treating pediatric mania. This raises questions about the differential efficacy of lithium across various symptom domains in pediatric BD. The lack of significant change in manic symptoms in our study could be attributed to several factors, including the relatively low baseline severity of mania in our sample or the concurrent use of other psychotropic medications, which might confound the assessment of lithium-specific effects. Moreover, relatively low lithium plasma levels could also contribute to this null finding.
Significant reductions were also observed in the anxiety-related CBCL subscales, including the Anxious/Depressed and Anxiety Problems subscales, as well as in the broader CBCL-DPI and MOAS aggression scores. This suggests that lithium not only acutely stabilizes mood but also has a positive impact on long-term ED-related symptoms, as well as on hostility and reactive aggression, which are prevalent in pediatric BD and often complicate the clinical picture. These findings suggesting lithium’s efficacy in managing ED, impulsivity, and aggression are paramount, since these are critical factors in BD-related suicidality and self-harm (Masi et al., 2023; Tondo and Baldessarini, 2016).
Another particularly notable finding of this study is the observed decrease in suicidal ideation and self-harming behaviors. The clinical measures of suicidality and para-suicidality we used in the present study showed a significant reduction in the prevalence of unspecified suicidal ideation, as well as a decrease in NSSI. These findings align with emerging evidence from longitudinal studies, which suggest that lithium may confer protective effects against suicide and self-harm in young patients with BD (Desai Boström et al., 2023; Hafeman et al., 2020; Jerrell, 2008; Ko et al., 2014). Particularly, the COBY study (Hafeman et al., 2020) previously showed that patients under 18 years of age on lithium treatment had half as many suicide attempts, fewer depressive symptoms, less psychosocial impairment, and less aggression than those on other mood stabilizers. Findings from this longitudinal study are consistent with adult trials, showing that lithium is associated with decreased suicidality, less depression, and better psychosocial functioning.
In addition, lithium was generally well-tolerated, with only a few cases of moderate-to-severe side effects leading to study withdrawal. Side effects were mostly mild to moderate, with increased thirst, appetite, and fine tremors being the most frequently reported. Two cases of severe side effects, including one instance of transitory hyperthyroidism and another of elevated CPK levels, underscore the importance of close monitoring of lithium therapy in adolescents. Overall, the stability of auxologic parameters, including BMI, blood pressure, and heart rate, over the treatment period suggests a favorable safety profile for ERLS in this population. Nonetheless, long-term studies are needed to fully understand lithium safety profile in this age group.
Findings from our study support the use of lithium as a viable option for treating depressive symptoms, aggression, impulsivity, and ED in adolescents with BD. The potential antisuicidal and self-harming effects of lithium highlight its importance in managing high-risk youth. However, the variable efficacy on manic symptoms suggests that a combination of treatments may be necessary for comprehensive management of BD in adolescents. Furthermore, the findings emphasize the need for individualized treatment plans and continuous monitoring to mitigate potential side effects and ensure safety.
Even though the present study did not compare different formulations of lithium and no conclusions can be drawn on this topic, the relevant issue related to the advantages of the extended- over the immediate-release lithium salts remains to be addressed. Theoretically, in terms of efficacy, no difference between the two formulations should be detected. Instead, clear benefits can be observed in terms of tolerability and intake effort for the ERLS, which could be critical factors for improving adherence in BD youth. Interestingly, two previous prospective naturalistic studies showed that mean plasma lithium levels and therapeutic adherence were higher for ERLS than the immediate-release formulation, as well as patients’ preference for ERLS for its better tolerability in terms of fine tremor and gastrointestinal symptoms (Barbuti et al., 2021; Durbano et al., 2002). Thus, future research comparing efficacy and tolerability of these two different formulations in youths will be paramount to provide further insights for clinicians on the adherence of BD children and adolescents to treatment. Nonetheless, the study findings should be interpreted in the context of its limitations, including the single-cohort design, the relatively small sample size, and the lack of a control group (e.g., patients receiving immediate-release lithium formulation). These factors limit the generalizability of the results and underscore the need for further randomized controlled trials to confirm these preliminary findings. Most importantly, the single-cohort design with no control arm prevented us to fully attribute the observed effects on BD symptoms to lithium treatment while excluding the normal course of symptoms over time. In addition, studies investigating the mechanisms underlying lithium antisuicidal effects could provide deeper insights into optimizing treatment strategies for adolescents with BD.
Conclusions
In conclusion, this study adds to the growing body of evidence supporting the efficacy of lithium in reducing depressive symptoms, aggression, ED, and suicidality in adolescents with BD. These findings highlight lithium’s potential role in comprehensive treatment strategies for pediatric BD, particularly in addressing the complex and multifaceted clinical presentation and challenging symptoms of the disorder, including among the others aggressiveness and suicidality. Future research should continue to explore the long-term effects and optimal management strategies for lithium treatment in this vulnerable population.
Footnotes
Clinical Significance
This study provides valuable insights into the effectiveness and tolerability of Lithium treatment for reducing emotional dysregulation and suicidality-related symptoms in adolescents with Bipolar Disorder. Our findings suggest that Extended-Release Lithium Salts may hold promise as a treatment option for managing challenging symptoms of the disorder, although further studies including larger samples, controlled designs, and longer follow-ups are needed to corroborate its effectiveness definitively. Furthermore, our study highlight the importance of implementing Lithium in the treatment of patients with severe clinical pictures due to its favorable side effects profile.
Authors’ Contributions
F.P. study design and methodology; F.B., D.D.C., D.R., S.B.a., G.T., G.S.c. methodology; S.B.e., V.V., P.F. conceptualization; A.M., G.M. supervision; G.S.e. supervison and data analysis.
Disclosures
G.M. has received research grants from Lundbeck and Humana, was in an advisory board for Angelini, and has been speaker for Angelini, FB Health, Janssen, Lundbeck, and Otsuka. All the other authors declare no conflicts of interest. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.