
Abstract
Background:
Antidepressant medication adherence patterns are inconsistent in adolescents with anxiety and related disorders, and the clinical and demographic features predicting adherence are poorly understood.
Methods:
In an ongoing single-site prospective trial involving adolescents (aged 12–17) with the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition anxiety disorders treated with escitalopram, adherence was measured for 12 weeks using electronic monitoring caps. Adherence patterns were examined using qualitative and unsupervised clustering approaches, and predictors of adherence were evaluated using logistic regression, with demographic (age, sex, and race) and clinical variables (e.g., anxiety severity [Pediatric Anxiety Rating Scale], irritability [Affective Reactivity Index], depressive symptoms [Children’s Depression Rating Scale]).
Results:
Among adolescents (N = 33) aged 14.5 ± 1.8 years (64% female), four adherence patterns were identified: persistent adherence, intermittent adherence, early adherence-late nonadherence, and nonadherence. In a logistic model of a 5-day moving average measure of adherence, social anxiety disorder (β = −0.68 ± 0.19, p = 0.002) and separation anxiety disorder (β = −0.61 ± 0.18, p < 0.001) were associated with lower adherence. In contrast, panic disorder, attention-deficit/hyperactivity disorder, generalized anxiety disorder, and depressive symptoms were not associated with adherence. Baseline anxiety severity was linked to lower adherence (β = −0.199 ± 0.05, p < 0.001). Older age also reduced adherence (β = −0.342 ± 0.05, p < 0.001), with each additional year of age increasing time spent nonadherent by 5% (p < 0.001). Being female (β = 0.451 ± 0.17, p = 0.011) and expecting treatment to be efficacious (β = 0.092 ± 0.04, p = 0.011) increased adherence, while greater irritability was associated with nonadherence (β = −0.075 ± 0.03, p = 0.006).
Conclusions:
Antidepressant adherence is variable, with distinct patterns, and those with social and separation anxiety disorders were less likely to be adherent. Factors such as older age, severe anxiety, and greater irritability predicted lower adherence, while being female and expecting treatment efficacy were associated with better adherence. Interventions that address specific symptoms or enhance treatment expectations may improve adherence.
Introduction
Antidepressants reduce symptoms in youth with anxiety disorders (Dobson et al., 2019; Gosmann et al., 2021; Strawn et al., 2015), major depressive disorder (Zhou et al., 2019), and obsessive-compulsive disorder (Geller et al., 2001; Pediatric OCD Treatment Study (POTS) Team, 2004). However, many children and adolescents do not consistently take these medications as prescribed (Stimpfl et al., 2024), which are generally administered daily (Fontanella et al., 2011; Semahegn et al., 2020; Zehgeer et al., 2018). Antidepressant pharmacotherapy for these conditions in youth often involves selective serotonin reuptake inhibitors (SSRIs), which, even with perfect adherence, have variable blood concentrations over time (i.e., exposure) (Baumel et al., 2024; Strawn et al., 2021b).
Adherence to pharmacotherapy in children and adolescents with mood disorders and attention-deficit/hyperactivity disorder (ADHD) has been explored, although prospective data related to adherence in pediatric anxiety disorders are rare (Zehgeer et al., 2018). In a meta-analysis of 28 studies (N = 180,870), approximately 35% of children and adolescents with a primary psychotic disorder, bipolar disorder, depression, recent suicide attempt, or psychiatric hospitalization were medication nonadherent (Edgcomb and Zima, 2018). In this sample, involvement in psychotherapy and insight boosted adherence. In contrast, more severe illness, substance use, and ADHD worsened adherence (Edgcomb and Zima, 2018). However, adherence was also moderated by age, sex, primary disorder, and methodologic approaches across studies.
In addition to clinical variables, parental factors also affect adherence in children and adolescents with psychiatric disorders. A meta-analysis (K = 23, N = 77,188) of these factors suggests that socioeconomic status, family makeup and functioning, and parental perception of medication acceptability significantly influence medication adherence in youth (Kalaman et al., 2023). Specifically, children from higher socioeconomic backgrounds or those whose families perceive pharmacotherapy to be efficacious are more likely to adhere to their medication (Zehgeer et al., 2018).
Beyond these meta-analytically observed effects, studies of youth with milder symptoms at the beginning of treatment and those without cooccurring externalizing disorders may have better adherence (Hamrin et al., 2010), as do those with better parent–child communication and greater parental involvement (Brinkman et al., 2012). In the Child/Adolescent Anxiety Multimodal Study (CAMS) (Walkup et al., 2008), youth living with two parents had improved adherence, although no demographic variables or clinical variables (e.g., anxiety severity) predicted adherence in this sample (Zehgeer et al., 2018). Furthermore, in prospectively followed anxious youth aged 7–17, the principal diagnosis and the number of other internalizing (other than separation, social or generalized anxiety disorders [GAD]) and externalizing (ADHD, oppositional defiant disorder, or conduct disorder) factors were not associated with adherence. However, the age-dependent comorbidity among anxiety disorders and syndromic overlap may have obscured this effect. Specifically, in younger children in this sample (age 7–11), comorbidity was higher, with nearly a third of the sample meeting the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-4) criteria for generalized, separation, and social anxiety disorders. In addition, alliance-related factors are also critically important (e.g., disliking the clinician, poor understanding of the rationale for treatment) (Charach et al., 2008; Hamrin et al., 2010) predictors of adherence in general in pediatric patients.
In adolescents with SSRI-resistant depression, variation in the dose-adjusted concentration of drug plus metabolites (concentration/dose ratio) was used as a proxy for nonadherence compared with clinician pill counts (e.g., 30% of the prescribed pills remaining). In this study, medication adherence, which was defined based on clinician-rated pill counts, was related to a higher response rate, and adherent patients were older and had lower rates of ADHD (8% vs. 17%); however, other clinical or demographic variables did not predict adherence (Woldu et al., 2011).
Most studies in children and adolescents have reported adherence based on pill counts or, in rare circumstances, therapeutic drug monitoring-based (Woldu et al., 2011) (i.e., using variation in concentrations over time across dosing). In addition, adherence in youth with anxiety disorders has neither been systematically evaluated nor have patterns of adherence been quantitatively described. Consequently, we cannot predict when patients become nonadherent, given that adherence patterns are generally thought to vary over time. We therefore evaluated patterns of electronically monitored adherence in adolescents with anxiety disorders who were participating in a double-blind, prospective trial of the SSRI escitalopram. We hypothesized, based on other adherence studies in youth, that (1) milder symptoms (e.g., less severe anxiety and less irritability), (2) greater expectations that treatment would be effective, and (3) being female would be associated with greater adherence. However, for the exploratory evaluation of temporal adherence patterns, which aimed to determine the number and type of specific adherence patterns, no specific type or number of categories was hypothesized.
Methods
Using data from an ongoing single-site outpatient study of adolescents (aged 12–17 years, inclusive, N = 33) with generalized, separation, and/or social anxiety disorder (pediatric anxiety triad) who were randomized to standard dosing of escitalopram or pharmacogenetically guided escitalopram dosing (Strawn et al., 2021a), we examined adherence patterns based on data from eCap™ electronic monitoring caps (eCAPS, Information Mediary Corporation). All patients provided written informed assent, and their parents provided written informed consent, and the institutional review board of the University of Cincinnati approved the study. Inclusion and exclusion criteria have been described elsewhere (Strawn et al., 2021a).
Briefly, patients were required to meet the DSM-5 criteria for generalized, separation, and/or social anxiety disorders and have a baseline Pediatric Anxiety Rating Scale (PARS) score ≥ 15 and a Clinical Global Impression-Severity score of > 4. The Mini-International Neuropsychiatric Interview for Children and Adolescents (MINI-KID), a structured diagnostic interview used to screen for DSM-5 psychiatric disorders and suicidality in children and adolescents (Sheehan et al., 2010), was administered by board-certified child and adolescent psychiatrists (J.R.S., J.F.) and uses a branching tree logic with two–four screening questions per disorder, followed by additional symptom questions if the screening questions are positively endorsed. The interview was completed with the parents and patient. Anxiety symptom severity was assessed using the PARS, a clinician-administered instrument that quantifies the severity of anxiety symptoms and probes symptoms of social, separation, and GAD in addition to physical symptoms and associated symptoms. The PARS evaluates the frequency, severity, and impairment of anxiety symptoms (RUPP, 2002) and is sensitive to change in treatment studies involving pediatric patients (Caporino et al., 2013; Johnco et al., 2015). To assess depressive symptoms, a board-certified child and adolescent psychiatrist administered the Children’s Depression Rating Scale (CDRS) (Mayes et al., 2010; Poznanski et al., 1984; Poznanski and Mokros, 1996), a semi-structured interview-based tool validated to quantify depressive symptoms in youth. Finally, the Affective Reactivity Index (ARI) was used to assess irritability in participants and quantify the frequency and impact of irritability symptoms (e.g., being easily annoyed, frequently losing temper, and staying angry) (Evans et al., 2021; Stringaris et al., 2012).
Treatment expectation was determined by eliciting the patient’s agreement with a series of three statements: (1) “I expect to get control over my anxiety through this treatment,” (2) “I expect to get better or become less anxious through this treatment,” and (3) “I expect my life to get better in some ways through this treatment” as previously described (Strawn et al., 2017). Responses to each statement were measured on a 5-point Likert scale, with the anchors being strongly disagree and strongly agree and a score of 3 being somewhat agree. The average of these three scores was taken to create a single variable corresponding to treatment expectations.
In youth randomized to standard dosing, escitalopram was prescribed consistent with the dosing strategy used in the adolescent registration trial that gave rise to the pediatric FDA approval for escitalopram (Strawn et al., 2023). In youth randomized to pharmacogenetically-guided escitalopram dosing, titration was based on their CYP2C19 phenotype and predicted escitalopram exposure (Strawn et al., 2019; Strawn et al., 2020).
Adherence, including the timing of the dose, was measured using eCAPS containing a computer chip embedded in a cap on the medication dram (McGrady et al., 2018). The chip records each date and time the dram is opened and provides an objective measure of medication adherence. Data were downloaded from the eCAP at each study visit. The data from each eCAP were visually inspected by a senior clinical research professional (Z.A.N.), a statistician (J.A.M.), and a child and adolescent psychiatrist (J.R.S.) to identify unusual or unexpected patterns that may have been related to movement artifacts. In these rare cases, collateral history was obtained from the family and patient, and pill counts were also conducted for each returned dram.
A quantitative dynamic measure of adherence was used, which involved computing a 5-day moving average of hourly time between doses of escitalopram (data from cap openings),
A categorical adherence variable was then developed from the hourly and 5-day moving average adherence patterns for each patient. A threshold of 5-day moving average >30 hours was judged as providing a reliable dynamic indicator of nonadherence. Alternate thresholds in the 5-day moving average (or in the hourly measure) were considered but failed to capture meaningful nonadherence periods for many patients. Specifically, we performed a sensitivity analysis to compare the performance of the 30-hour threshold with alternative thresholds (e.g., 28, 36, 40, 48 hours) to assess the proportion of nonadherence periods detected and agreement with an alternative adherence indicator (i.e., clinician impression).
Two approaches to classify patterns of adherence were implemented in parallel. First, adherence patterns for each patient were plotted for the entire treatment period, with the 5-day moving average superimposed on each plot. A board-certified child and adolescent psychiatrist and a senior statistician experienced in panel data analysis independently categorized these adherence patterns. Second, an unsupervised clustering approach was applied (Ziegel, 2003) to the 5-day moving averages. Two distance measures for time-series data of heterogeneous lengths, dynamic time warping (DTW), and Fréchet distance were used to calculate dissimilarity between each patient’s 5-day moving average (Giorgino, 2009) using the LongitudinalData package in R (version 2.4.5.1). Clustering was performed using hierarchical clustering and partitioning around medoids algorithms. The clusters resulting from each combination of distance measure and clustering algorithm were reviewed using visual representations, within-cluster sum of squares, and silhouette width metrics. The unsupervised clustering analysis was performed using R (version 4.4.1). Four doctoral-level investigators then reviewed the adherence classifications of the visual categorizations and unsupervised clustering to determine the final assignments used for further analysis.
To determine the influence of demographic and disorder characteristics (which are constant across the sample for each individual) on patterns of adherence, we first categorized patients by adherence pattern, then estimated a logistic regression with an indicator variable for adherence as the dependent variable (logistic models for other patterns of adherence were also considered where feasible-two of the four groups had three or fewer patients). Panel regressions were used to estimate the significance and magnitude of the effect of adherence predictors. The logistic regression used a categorical definition of adherence (5-day moving average >30 hours) to provide a dynamic indicator of nonadherence. Alternate thresholds (36-hour threshold in the 5-day moving average) were evaluated similarly to the selection of the 5-day moving average but failed to capture meaningful nonadherence periods for many patients.
The time to the first period of nonadherence (defined as ≥30 hours between doses in a 5-day moving average) was evaluated using Kaplan–Meier nonparametric survival curves for each category of adherence: (1) adherent, (2) waning adherence, (3) intermittent adherence, and (4) nonadherence. A parametric Cox proportional hazards model was estimated to evaluate the impact of clinical and demographic variables on the time to first nonadherence.
Models were estimated via posterior simulation using Hamiltonian Monte Carlo sampling with the Turing.jl package using Julia (version 1.9) (Bezanson et al., 2017). Coefficient posterior means are expressed ± their standard deviations, and findings were considered statistically significant at the 1% threshold (i.e., p < 0.01).
Results
Sample characteristics
Patients (N = 33) were 14.5 + 1.8 years of age, and 64% were girls (n = 21). The majority (88%) were White, and patients had a mean baseline PARS score of 17 ± 2. Anxiety disorders were often comorbid, with 94% of patients meeting the DSM-5 criteria for GAD. Additional demographic characteristics are shown in Table 1.
Demographic and Clinical Characteristics
CDRS-R, Children’s Depression Rating Scale-Revised; PARS, Pediatric Anxiety Rating Scale; ADHD, attention-deficit/hyperactivity disorder; GAD, generalized anxiety disorder.
Classification of adherence patterns
Based on the calculated within-cluster sum of squares and silhouette score, as well as through visual confirmation of the clustering assignments, partitioning around medoids clustering with either DTW or Fréchet distance provided optimal classifications. The unsupervised and clinician-determined clustering both identified four distinct adherence patterns, and good concordance (n = 27, 82% for DTW, n = 29, 88% for Fréchet) in clustering assignments was observed between approaches. Disagreements in classification were reviewed, and final assignments were made based on agreement between four investigators. The results of the unsupervised analysis are available in the supplementary material (Supplementary Fig. S1, S2, S3 and S4). The final classifications of adherence patterns in the 5-day moving average are shown in Figure 1. Individual adherence patterns are shown in Supplementary Figure S5. Patients described as “adherent” (N = 16, 48%) demonstrated consistent adherence throughout the study period, with relatively few deviations from the one capsule per 24-hour regimen. The adherence pattern was stable, indicating high compliance with the prescribed regimen. A subset of patients—classified as “waning adherence”—initially demonstrated consistent adherence but began to exhibit nonadherence as the treatment progressed (N = 12, 36%). Early in the study, these individuals adhered closely to the prescribed regimen, but adherence waned over time, leading to more frequent missed doses later in treatment. A third group of patients displayed intermittent adherence throughout treatment, characterized by episodes of nonadherence interspersed with periods of adherence (classified as: “intermittently adherent”). These individuals often returned to adherence after lapses, but their overall pattern was inconsistent (N = 2, 6%). The fourth group, labeled “nonadherent” (N = 3, 9%), exhibited early and frequent deviations from the prescribed regimen. These individuals showed significant adherence variability, with numerous missed doses throughout the treatment period. The characteristics of the patients within each of these adherence groups are shown in Table 1, and no patients discontinued treatment because of nonadherence.
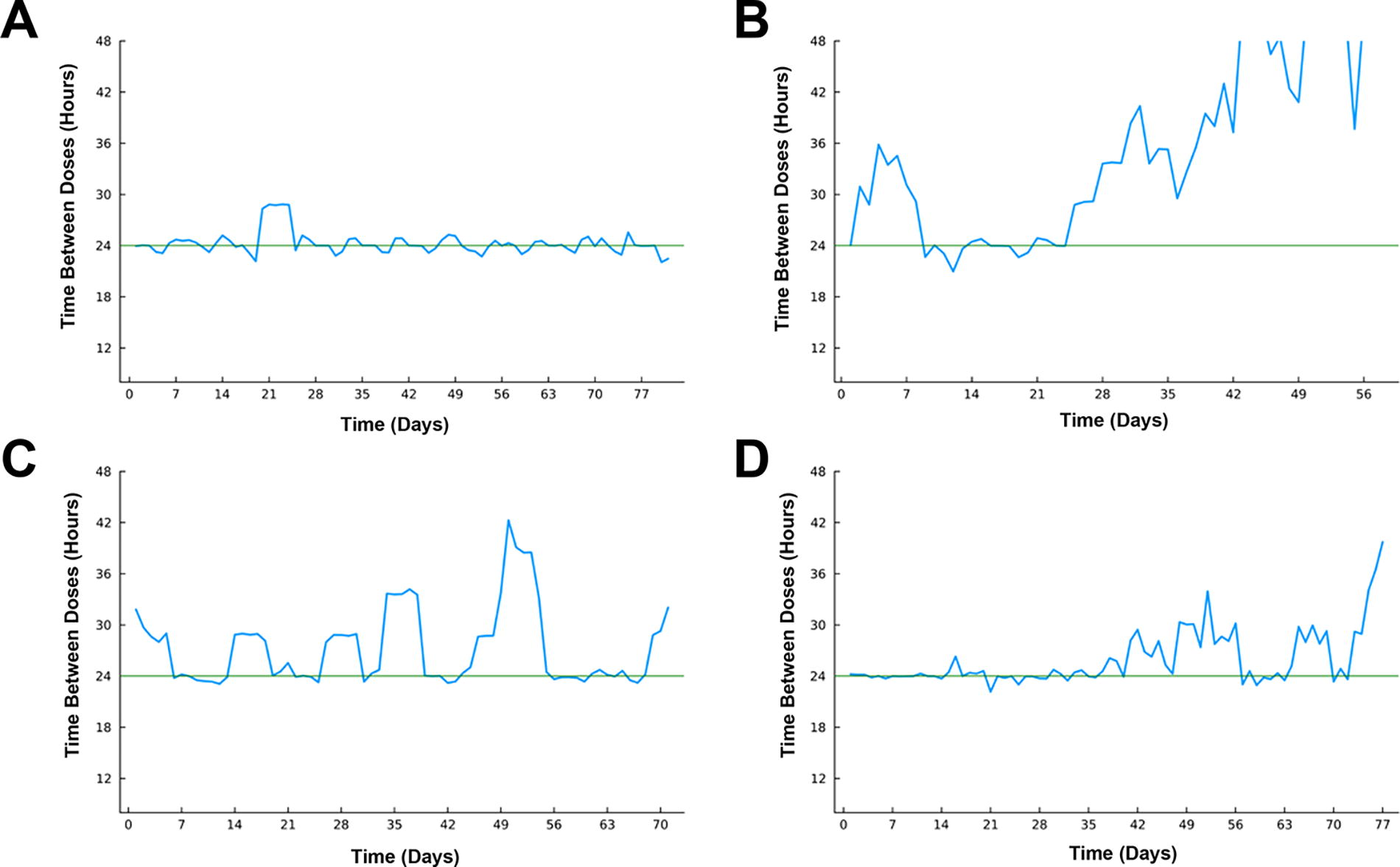
Representative adolescents demonstrating qualitative adherence patterns. Blue lines represent the 5-day moving average of time since the last dose. Adherent patients had consistent adherence over the study period with relatively few excursions from the one capsule per 24-hour measure
Influence of diagnosis and comorbid symptoms on adherence
The influence of diagnosis on a 5-day moving average of adherence was examined in a logistic regression. Having social anxiety disorder was associated with a lower likelihood of having adherence (
Logistic Regression for 5-Day Moving Average of Nonadherence in Adolescents Receiving Escitalopram
Estimated coefficients reflect the effect of a variable on the probability of adherence. Findings that are statistically significant at the 1% threshold (i.e., p < 0.01) are italicized.
ADHD, attention-deficit/hyperactivity disorder; ARI, Affective Reactivity Index; CDRS, Children’s Depression Rating Scale; GAD, generalized anxiety disorder; PARS, Pediatric Anxiety Rating Scale.
Influence of clinical characteristics on adherence patterns
More severe anxiety at baseline, as reflected by PARS score, was associated with a lower likelihood of adherence (
A panel regression model was used to estimate the magnitude of these effects in terms of missing hours of medication (beyond once daily dosing). In this model, the patient’s actual adherence was compared with perfect adherence (i.e., taking the medication every 24 hours), and the largest effect among diagnostic variables was for social anxiety disorder, which increased the average time that a patient was nonadherent by approximately 16% (
Time to first nonadherence event
Time to the first episode of nonadherence differed across adherence groups (Fig. 2). However, the time to the first nonadherent period was not associated with baseline anxiety severity (
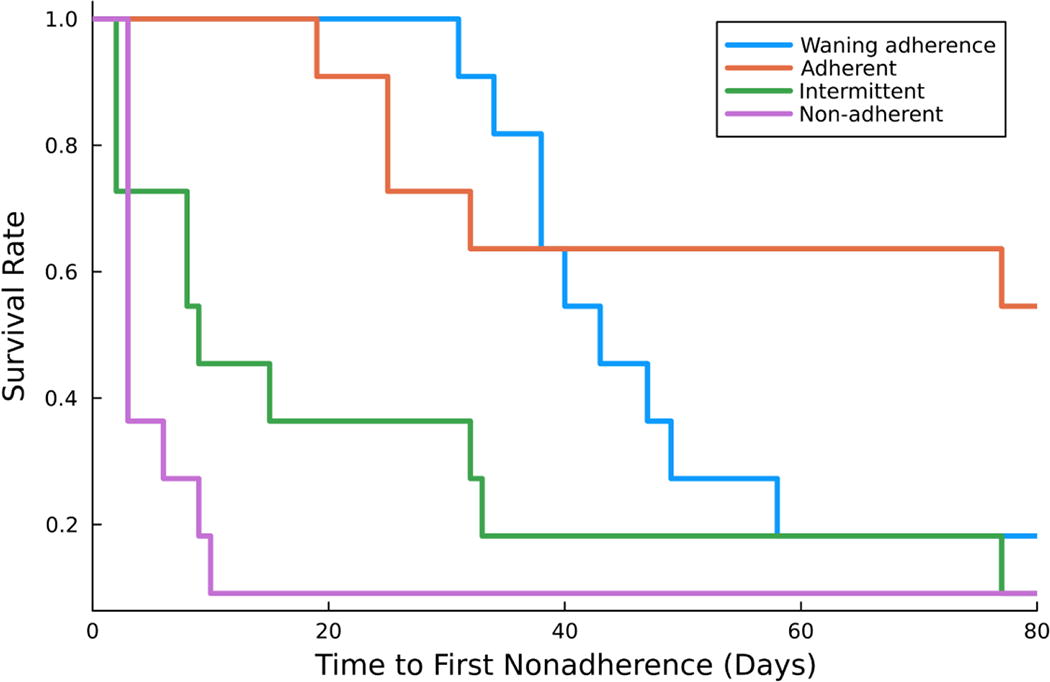
Time to first nonadherence. Survival curves depicting the time to first >30-hour deviation in dosing among the four adherence categories. The red line represents patients classified as adherent, and the green line represents those intermittently adherent. The blue line represents patients with waning adherence, and the purple line represents those with nonadherence.
Discussion
This is the first study to evaluate patterns of adherence using daily data in youth with anxiety disorders and identify clinical and demographic features that predict adherence over an acute treatment period. These preliminary findings, if replicated, may lay the groundwork for improving treatment outcomes in adolescents with anxiety disorders, as adherence and missed doses affect medication exposure (concentration over time) in youth (Baumel et al., 2024; Strawn et al., 2021b). SSRI exposure is associated with efficacy (Taurines et al., 2013) and tolerability (Poweleit et al., 2024; Reinblatt et al., 2009; Strawn et al., 2020) in youth. In addition, the predictors of adherence identified herein may have implications for how specific clinical features might be addressed to improve adherence and how the pathophysiology of these features (e.g., more severe anxiety, irritability) might directly impact adherence.
In our study, more severe anxiety and greater irritability predict lower adherence. Using these features—which can be easily measured in clinical settings—may help to identify patients needing additional support and tailored interventions, including reminders from clinicians, utilization of electronic interventions such as pill reminder apps, or adherence monitoring by parents or guardians. In addition, the relationship between these features and lower adherence could have implications beyond risk stratification. It is possible that adolescents with more anxiety may also experience anxiety related to the medication or be anxious about experiencing side effects. More severe anxiety is associated with threat bias in youth (Britton et al., 2011; Roy et al., 2008; Shechner et al., 2012; Warner and Strawn, 2023; Waters and Craske, 2016). Youth with more severe anxiety see ambiguous or benign situations as threatening; they overgeneralize, which results in safe stimuli being treated as threatening (Strawn and Stahl, 2023; Waters and Craske, 2016). This ultimately contributes to avoidance—which may represent missed doses in the case of medication. More severe anxiety is further associated with executive functioning deficits such as working memory, monitoring, planning, and task-switching difficulties (Shanmugan et al., 2016; Baumel et al., 2022) (Castagna et al., 2019; Moran, 2016; Sylvester et al., 2016; Tobias and Ito, 2021), which could contribute to more difficulty taking the medication consistently. However, this possibility would require direct assessment.
Patients with increased irritability—a relatively nonspecific but transdiagnostic symptom linked with greater impairment—had more nonadherence. While the mechanisms underlying this association are unknown, being more irritable may reflect more severe pathology or an endophenotype of the anxiety disorders (Evans et al., 2021), but may also relate to the family system. More irritable youth may struggle to maintain routines, including taking medication. They may be more resistant to or react with frustration or anger to family members’ reminders and support.
Among the anxiety disorders in this sample, social and separation anxiety disorders were more likely to be nonadherent. Interestingly, in the CAMS, which evaluated youth (N = 488) randomized to cognitive behavioral therapy (CBT), sertraline, CBT + sertraline, or placebo, patients with social anxiety and separation anxiety did best when CBT was a component of their treatment (Compton et al., 2014). In contrast, those with GAD tended to need sertraline as a component of treatment to maximize response. The “key ingredient” of these disorders suggests that specific aspects of these two disorders could benefit from the additional support provided by CBT that may promote adherence through either a synergistic reduction in anxiety or through work related to cognitive distortions. In addition, avoidance is a hallmark feature of both separation and social anxiety disorders, and this may have also contributed to engagement with pharmacotherapy—reflected in this study as nonadherence.
Being older was associated with reduced adherence. Future studies may evaluate the way in which older adolescents might benefit from more structured support systems like reminders, adherence-enhancing technologies, or greater involvement from family members. This finding, if replicated, may have developmental implications. Adolescence represents a period of cognitive and emotional maturation during which the adolescent learns to manage self-care and a period in which they disengage from parents as they establish a distinct sense of self. During this time, they are less dependent on parental approval and begin making more of their own decisions (Delgado and Strawn, 2018). Parents may increasingly allow the adolescent to manage tasks independently. However, our data regarding adherence suggest that this is a time when parents may increase engagement and increase monitoring and support of medication rather than relying on the adolescent’s nascent autonomy related to medication taking.
In this study, expecting the SSRI to be helpful was associated with increased adherence. This finding is of interest in that treatment expectations in a large trial of anxious youth also predicted the magnitude and trajectory of placebo-related improvement (Strawn et al., 2017) and overall improvement in other studies of psychotherapy in anxious youth (Wu et al., 2020). This finding also replicates the relationship between adherence and expectation of treatment success observed in sertraline-treated youth in the CAMS. Furthermore, in adults, the expectation of a positive effect of treatment in and of itself may decrease anxiety (Benedetti, 2002), which, given the relationship between greater anxiety and nonadherence, could indirectly improve adherence. Expectations for treatment success may represent a cognitive trait that could be augmented clinically as we discuss the data and evidence supporting treatment and check clinician ambivalence and uncertainty related to the likelihood that a treatment will work. Importantly, negative expectations (i.e., threat bias) are often present in anxious youth (Britton et al., 2011; Roy et al., 2008; Shechner et al., 2012; Warner and Strawn, 2023) and may be associated with less response to treatment. Adherence may be the mechanism linking negative expectations to decreased treatment response.
While this is the first study to evaluate antidepressant daily adherence in youth with anxiety disorders, other studies have used different approaches to examine psychotropic adherence (e.g., drug levels, pill counts, self-report measures, and a combination of these) (McVoy and Levin, 2023) in children and adolescents with other disorders (Sanchez et al., 2021). In youth with mood disorders, a qualitative study recently demonstrated several factors related to nonadherence, including motivation, denial of illness, side effects, negative relationships with clinicians, beliefs regarding benefits, as well as caregiver support and involvement (Forthun et al., 2023). Similarly, in a cohort of 1485 youth treated with mood stabilizers, nonadherence (defined as missing 30% of doses weekly) was associated with forgetting, side effects, being embarrassed to take medications, and “preferring to do something else” (Klein et al., 2024). However, in youth with bipolar disorder, adherence does not appear to be related to the severity of the affective symptoms, and symptoms vary significantly, but encouragingly, monitoring adherence in and of itself may be associated with approximately 5% improvement in adherence (Sajatovic et al., 2023). These findings suggest that monitoring adherence and attending to risk factors identified herein and more general psychosocial strategies (e.g., psychoeducation, motivational interviewing, and cognitive behavioral strategies) (McVoy and Levin, 2023) could improve adherence. Our findings also raise the possibility that some individuals may exhibit early adherence, which significantly wanes over time. This pattern has been described in other disorders in youth (e.g., epilepsy) and underscores the importance of ongoing monitoring of adherence.
While this is one of only several examinations of adherence using daily electronic monitoring in adolescents and the first to do so in a prospective clinical trial with high-dimensional data, there are several limitations. First, the total number of participants is small and only includes adolescents, which limits the ability to examine many covariates and to generalize to children and young adults. However, despite the sample consisting of 33 patients, this longitudinal sample includes 2115 observations, representing a relatively large dataset with an average of 64 data points per patient and high-frequency (daily) sampling for most patients. Second, because patients were required to have moderate to severe anxiety symptoms and not to have significant treatment resistance, the generalizability to individuals with less severe anxiety or mixed anxiety and depressive disorders is limited. Third, the clinical trial structure, which included more frequent assessments and support than typical clinical care, may have influenced adherence, and the use of a single SSRI, escitalopram, may limit generalizability. Fourth, we could not evaluate the impact of the time of year (e.g., during school months or summer break) on adherence due to the lack of variation within each patient’s sampling interval. Most patients had data collected predominantly during the summer months without school or during the school year, limiting our ability to assess seasonal effects. Fifth, this sample lacks diversity, which may have precluded our ability to examine the specific impact of race and ethnicity. Sixth, the small number of patients with specific comorbidity patterns (e.g., social anxiety disorder and separation anxiety disorder) in each adherence group, combined with the limited availability of efficacy measures during specific treatment phases (early vs. late), prevents us from determining whether poorer adherence in patients with social or separation anxiety is linked to reduced early efficacy of escitalopram. Seventh, we were limited in our ability to assess family variables, including family dysfunction and poor parent–child communication, and lack of parental involvement in medication routines which, in other studies, predicts poor adherence to medication adherence (Brinkman et al., 2012). Last, factors related to the clinician–patient–family relationship could not be explored in the current study. However, short and infrequent appointments, dissatisfaction with a clinician, and a lack of patient understanding of pharmacotherapy have been historically associated with nonadherence (Charach and Gajaria, 2008; Hamrin et al., 2010).
Conclusions
This study demonstrates four distinct adherence patterns of adherence among adolescents with anxiety disorders: “adherent” (48%), who maintained consistent adherence throughout the study; “waning adherence” (36%), who started with good adherence but became less consistent over time; “intermittently adherent” (6%), who showed fluctuating adherence with periods of both adherence and nonadherence; and “nonadherent” (9%), who frequently deviated from the prescribed regimen early on.
Clinical Significance
This is one of the first studies to demonstrate that individual factors such as having social anxiety disorder, higher baseline anxiety, being older, and greater irritability were associated with decreased adherence while being female and having higher expectations for treatment efficacy predicted better adherence. These findings underscore the potential importance of addressing specific clinical characteristics to optimize adherence in adolescents with anxiety disorders. It will be important for future, larger studies to evaluate clinical characteristics associated with specific adherence groups to inform future efforts at increasing adherence.
Footnotes
Disclosures
J.R.S. has consulted to AbbVie (Cerevel), Otsuka, MindMed, and Alkermes. He has served on advisory boards to Genomind, receives royalties from Springer Publishing and Cambridge University Press, UpToDate, and material support from Myriad. He has received research support from MindMed and honoraria from Medscape and Neuroscience Education Institute. L.B.R. has received research funding and consulted for BTG Specialty Pharmaceuticals. The other authors have no real or potential conflicts of interest.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.