
Abstract
Objective:
The purpose of this article was to review the safety, tolerability, and effectiveness of clozapine in youth and young adults with autism spectrum disorder (ASD) and/or intellectual disability.
Methods:
An IRB-approved retrospective chart review of youth and young adults with autism and/or intellectual disability who were prescribed clozapine between January 2012 and June 2020 was completed. Information was collected from 1 year before through 1 year after clozapine initiation related to medications prescribed, hospitalizations, emergency department (ED) visits, and Clinical Global Impressions-Severity and Clinical Global Impressions-Improvement (CGI-I) ratings. Adverse effects and reasons for stopping clozapine were documented.
Results:
Fifty-eight patients were included in analysis. Forty patients remained on clozapine through June 2020 and 18 did not. Most patients were prescribed clozapine for treatment of irritability. Reasons for stopping clozapine included side effects, continued behavior concerns, difficulty with blood draws, and improvement in symptoms. For those who remained on clozapine for the duration of the review period, the number of hospitalizations and ED presentations for psychiatric concerns or medical concerns potentially related to clozapine significantly decreased in the year following clozapine initiation compared with the year prior (2.13 vs. 3.48, p = 0.010). There was a significant reduction in CGI-I scores from 3.96 to 2.53 (p < 0.001) from clozapine initiation to 1 year later. There was a nonsignificant trend toward reduction in use of multiple antipsychotics simultaneously from time of clozapine initiation to 1 year later in those who remained on clozapine (38.5% vs. 25%, p = 0.232).
Conclusions:
Use of clozapine for treatment-refractory irritability in youth and young adults with ASD and/or intellectual disability is generally well-tolerated. Observed benefits included a decrease in number of hospitalizations and ED visits and a decrease in CGI-I score in the year after clozapine initiation.
Introduction
Irritability, aggression, and self-injurious behaviors (SIBs) can be unsafe and debilitating behaviors, both important and challenging to treat. Irritability is a nonspecific distress sign that can indicate any number of medical or psychiatric concerns, so the workup of any child with irritability should be comprehensive (Carlson et al., 2023). When individuals with autism spectrum disorder (ASD) present with clinically impairing behaviors within the symptom cluster of irritability, self-injury, and aggression that remain severe despite ruling out medical causes, optimizing communication, and utilizing behavioral and sensory measures, medication can be beneficial for treatment and for maintaining safety.
While irritability is not a diagnosis in itself, it is recognized by the U.S. Food and Drug Administration (FDA) as a treatment target for autistic individuals, for whom comorbidity is common but not always clear (Hossain et al., 2020). Medications do not treat the core symptoms of autism; however, the atypical antipsychotics risperidone (McCracken et al., 2002) and aripiprazole (Shea et al., 2004) are FDA-approved for treatment of irritability in autistic individuals. For patients who do not benefit from a therapeutic trial of these FDA-approved medications, there are off-label options (Fosdick et al., 2017; Henneberry et al., 2021; Lamy et al., 2020). While other off-label medications are often utilized prior to prescribing clozapine due to clozapine’s side effect profile and monitoring requirements, clozapine is one off-label option that shows promise for autistic individuals with severe, treatment-refractory symptoms (Chen et al., 2001; Gobbi and Pulvirenti, 2001; Lambrey et al., 2010; Wink et al., 2016).
Clozapine is an atypical antipsychotic indicated for treatment-resistant schizophrenia and for reducing suicidal behavior in patients with schizophrenia or schizoaffective disorder (Clozaril (clozapine) prescribing information, FDA). It was FDA-approved for treatment-resistant schizophrenia in 1989 after a study showed significant improvement in patients who were refractory to other antipsychotic medications (Kane et al., 1988). Evidence continues to support its use as the “gold standard” for treatment-resistant schizophrenia (Lally and MacCabe, 2015; Siskind et al., 2016). Improved cognition and decreased violence are also seen after clozapine initiation in adults with schizophrenia (McQueen et al., 2021).
Clozapine has a unique, widespread mechanism of action that is still not fully understood (Khokhar et al., 2018). It involves activity across a variety of receptor types including dopaminergic, muscarinic, gamma-aminobutyric acid (GABA)ergic, serotonergic, and adrenergic effects, as well as possible modulation of glutamatergic neurotransmission (Daskalakis and George, 2009; Jann, 1991). Clozapine’s use in schizophrenia raises the question as to whether its unique effectiveness might confer benefit for additional severe and otherwise treatment-resistant psychiatric presentations as well.
Clozapine does carry a risk of significant side effects, including agranulocytosis, orthostatic hypotension, seizures, myocarditis, cardiomyopathy, and increased mortality in elderly patients with dementia. In the United States, prescribing and dispensing clozapine had required use of the FDA-mandated Clozapine Risk Evaluation and Mitigation Strategy (Clozapine REMS) program due to the need for close monitoring for agranulocytosis. Use of the REMS program allowed for rapid detection of agranulocytosis and is credited for the reduction in the incidence of death from clozapine-induced agranulocytosis to around 0.05%, according to a meta-analysis of clozapine-treated adults (Li et al., 2020). In February 2025, the FDA announced that use of the REMS program was no longer required, though continued monitoring of absolute neutrophil count according to frequencies outlined in prescribing information is still recommended. Constipation can be a more common concern with the use of clozapine. If untreated, severe constipation can lead to bowel obstruction and death (Hibbard et al., 2009).
There is no current FDA approval for the use of clozapine in children and adolescents. A literature review cites promising evidence of clozapine efficacy in severe psychotic and nonpsychotic symptoms in the pediatric population (Rachamallu et al., 2019). There is also no current FDA approval for the use of clozapine in individuals with autism. Evidence for its use in the treatment of irritability in ASD is limited to case series and reports. A recent scoping review, mostly from case reports, suggests common side effects but general tolerability and effectiveness for treatment-refractory disruptive behaviors, psychosis, catatonia, and mood symptoms in individuals with ASD (da Rosa et al., 2024). In a series of six patients over age 16 with ASD (Beherec et al., 2011), all tolerated clozapine and continued to benefit from it 11 years later (Rothärmel et al., 2018). In another case study, clozapine seemed effective and well-tolerated for a child and a young adult with ASD and treatment-resistant catatonia (Thom and McDougle, 2022). Other case reports and series demonstrate that clozapine is effective and well-tolerated for treatment of severe irritability and aggression in adolescents with autism (Chen et al., 2001; Gobbi and Pulvirenti, 2001; Lambrey et al., 2010; Wink et al., 2016) and in a young adult with autism (Gobbi and Pulvirenti, 2001).
For certain autistic children, adolescents, and young adults with severe and refractory irritability, aggression, and SIB, we believe off-label use of clozapine can be clinically indicated but only after consideration that the possible benefits outweigh the potential adverse effects of clozapine, as should be the case with prescription of any medication. Clozapine is typically not pursued as an off-label treatment option for youth with ASD unless irritability, aggression, and/or SIB remain severe despite implementation of structural and behavioral interventions, as well as despite trials of other more evidence-based and lower-risk medications, including risperidone and aripiprazole. With adherence to clinical and laboratory monitoring, it is our clinical experience and the hypothesis of this retrospective case series that clozapine is usually well-tolerated in children, adolescents, and young adults with autism and/or intellectual disability and can be effective for treatment-refractory irritability, aggression, and SIB.
Here, we examine youth and young adults with neurodevelopmental disorders who were prescribed clozapine, with the goal of further assessing the safety, tolerability, and effectiveness of clozapine in this patient population.
Materials and Methods
We performed an Institutional Review Board (IRB)-approved retrospective chart review of youth and young adults with ASD and/or intellectual disability who were prescribed clozapine by a child and adolescent psychiatrist between January 2012 and June 2020, either in an inpatient psychiatric hospital or in an outpatient psychiatric setting within a single large academic children’s hospital system. Patients of any age were included, as long as they had a diagnosis of ASD and/or intellectual disability. Data were reviewed through June 2020, or for at least 1 year after clozapine initiation in those who were prescribed clozapine after June 2019, to allow for at least 1 full year of available data after clozapine initiation for all patients reviewed. Clinical notes, problem lists, prescription history, hospitalizations, emergency department (ED) visits, flowsheets, and growth curves were reviewed.
Patients who were still taking clozapine in June 2020 were included in the group considered to have remained on clozapine. Those who were no longer taking clozapine by June 2020 were included in the group considered to have discontinued clozapine. For those who remained on clozapine through June 2020, data on body mass index (BMI), medications prescribed, numbers of hospitalizations and ED visits, Clinical Global Impressions-Severity (CGI-S) ratings, and Clinical Global Impressions-Improvement (CGI-I) ratings were collected at 1 year before through 1 year after clozapine initiation, regardless of total duration on clozapine. For those who stopped clozapine prior to June 2020, data were collected from 1 year prior to clozapine initiation through date of clozapine discontinuation.
Demographic information included age, sex, race, and BMI. Charts were searched to confirm diagnoses of ASD and/or intellectual disability. Other psychiatric and medical diagnoses were obtained from the problem list at the time of clozapine initiation. Psychiatric diagnoses were categorized into groups including anxiety disorders, ASD, bipolar disorder, depression, impulse control disorders, intellectual disability, psychotic disorders, and posttraumatic stress disorder. BMI data were gathered for each patient at the date closest to clozapine initiation, for patients who had BMI data available. For those who remained on clozapine, BMI data were gathered at the date closest to 1 year after clozapine initiation. BMI Z-scores were calculated for patients up to 20 years old using the CDC growth reference.
For all patients, medications at the time of clozapine initiation as well as number of psychiatric hospitalizations and ED visits in the year prior to clozapine initiation were recorded. Medications were categorized into groups including antipsychotic, mood stabilizer, alpha-2 agonist, selective serotonin reuptake inhibitor (SSRI), medication used to target sleep, stimulant, and propranolol. Adverse effects possibly related to clozapine, as indicated in clinical notes, were documented. For patients who stopped clozapine prior to June 2020, the length of time on clozapine as well as the reason(s) for stopping clozapine were recorded. For those who remained on clozapine through June 2020, medications at 1 year after clozapine initiation, as well as number of hospitalizations and ED visits for psychiatric concerns or medical concerns potentially related to clozapine in the year after clozapine initiation, were recorded.
Clinical response was also evaluated through the CGI-S scale and CGI-I scale. These scales are clinician-rated assessments of symptoms severity and treatment response, ranging from 1 to 7. Where available, CGI data were extracted from clinical notes and from flowsheets within the EMR. CGI-S and CGI-I scores were noted from the time of clozapine initiation. For those who remained on clozapine, CGI-S and CGI-I scores were also recorded from 1 year after clozapine initiation. For those who stopped clozapine, CGI-S and CGI-I scores were collected from the time of the decision to stop clozapine.
Data analysis was performed with Microsoft Excel and GraphPad Prism 10. BMI Z-scores were compared via paired t-test; individuals were excluded from this comparison if either pre or post-BMI were unavailable. Contingency analyses were performed using chi-square with Bonferroni adjustment for multiple comparisons where indicated. For individuals where both pre- and post-CGI scores were available, CGI scores were compared via Wilcoxon paired signed-rank tests with Bonferroni adjustment. CGI scores were compared across continuation and discontinuation groups via Mann–Whitney U test.
Results
A total of 66 patients with autism and/or intellectual disability who were prescribed clozapine by a child and adolescent psychiatrist were identified. Five patients were excluded due to no available follow-up information in the EMR. Three patients had two separate trials of clozapine and were not included in the data analysis. Thus, 58 patients were included in analysis; 40 patients had remained on clozapine for the time period assessed, and 18 patients had not.
There were no significant differences in demographic profile of patients who continued versus those who discontinued clozapine during the study (Table 1). The majority of patients in this study were male (72.4%) and Caucasian (82.8%). Age at time of clozapine initiation ranged from 7 to 31 years old, with an average age of 15.4 years old. The average age of those who remained on clozapine was 15.9 years old at the time of clozapine initiation, and the average age of those who stopped clozapine was 14.4 years old at the time of clozapine initiation.
Clinical and Sociodemographic Characteristics
Patients may have more than one diagnosis.
Anxiety disorders included anxiety and obsessive-compulsive disorder.
Impulse control disorders included oppositional defiant disorder, disruptive mood dysregulation disorder, intermittent explosive disorder, and attention-deficit hyperactivity disorder.
Psychotic disorders included schizophrenia and psychosis not otherwise specified.
PTSD, posttraumatic stress disorder.
Ten patients were prescribed clozapine in an outpatient psychiatry setting, and 48 patients in an inpatient psychiatry setting. Maximum total daily dose of clozapine ranged from 50 to 850 mg per day among all participants and between 187.5 and 850 mg per day for patients remaining on clozapine for the observation period. Mean maximum dose was 483.4 mg daily in the continuation group, and mean maximum dose was 393 mg daily in the discontinuation group (p = 0.053). Indications for initiating clozapine included irritability (51), schizophrenia (2), irritability and psychosis (2), irritability and anxiety (1), irritability and tardive dyskinesia on other antipsychotic medication (1), and irritability and catatonic symptoms (1). See Tables 2 and 3 for individualized information.
Individual Patient Information for Patients Who Remained on Clozapine (n = 40)
CGI-I, Clinical Global Impressions-Improvement; CGI-S, Clinical Global Impressions-Severity.
Individual Patient Information for Patients Who Stopped Clozapine (n = 18)
CGI-I, Clinical Global Impressions-Improvement; CGI-S, Clinical Global Impressions-Severity.
Of the 58 patients, 55 had a diagnosis of an impulse control disorder (oppositional defiant disorder, intermittent explosive disorder, disruptive mood dysregulation disorder, or attention-deficit hyperactivity disorder), 55 had a diagnosis of intellectual disability, and 48 had a diagnosis of ASD. Only six patients had a diagnosis of bipolar disorder, six had a diagnosis of an anxiety disorder, three had a diagnosis of a psychotic disorder (schizophrenia or psychosis not otherwise specified), and no patients had a diagnosis of major depressive disorder. The most common medical diagnoses included constipation in 36 patients and epilepsy in 7 patients.
Baseline BMI was available for 39/40 patients who remained on clozapine and 17/18 patients who stopped clozapine. BMI Z-scores were calculated for patients up to 20 years old using the CDC growth reference, resulting in BMI Z-scores for 32/40 patients who remained on clozapine and 13/18 patients who stopped clozapine. Baseline average BMI Z-score was 1.04 among all participants and was no different between patients who continued and those who discontinued clozapine during the study period. There was no significant increase in BMI Z-score 1 year after clozapine initiation in those who remained on clozapine (Fig. 1). Change in BMI Z-score ranged from a reduction of 0.97 points to an increase of 1.72 points. The seven patients who remained on clozapine and were 20 years old or older at the time of clozapine initiation were unable to have BMI Z-scores calculated due to age. In these seven patients, BMI at 1 year after clozapine initiation was lower for four patients, higher for two patients, and not available for one patient.

BMI Z-score before and 1 year after clozapine initiation in patients who remained on clozapine (n = 32). Note that “pre” refers to time of clozapine initiation and “post” refers to 1 year after clozapine initiation. BMI, body mass index.
Of the 58 patients assessed, 18 stopped clozapine during the observation period. Ten of the 18 patients stopped within the first 6 months of clozapine therapy, and 17 of the 18 stopped within the first 15 months of clozapine therapy. Reasons for stopping included side effects only (three patients), continued behavior concerns only (four patients), a combination of side effects and continued behavior concerns (seven patients), difficulty with blood draws (three patients), or improvement in symptoms allowing for discontinuation of medication (one patient). Side effects which contributed to patients stopping clozapine included tachycardia, constipation, increased appetite, abnormal movements, urinary accidents, skin irritation, and drooling. Only 1 of the 18 patients had concern for neutropenia, and this patient also had concerns related to possible abnormal movements and continued severe behaviors despite clozapine use, so the psychiatrist and family agreed to stop clozapine prior to increasing frequency of lab monitoring. No patients stopped due to seizures or myocarditis.
For those who remained on clozapine for the duration of the review period, average length of time on clozapine was 34 months, with the longest duration being 78 months. Data were collected from 1 year before through 1 year after clozapine initiation, regardless of total duration on clozapine. Of the 40 patients who remained on clozapine for the duration of the review period, the number of patients who were on a mood stabilizer or alpha-2 agonist was lower at 1 year after clozapine initiation as compared with at the time of clozapine initiation (Table 4). Of those taking antipsychotics, at the time of clozapine initiation, 15/39 (38.5%) were on multiple antipsychotics simultaneously. The one patient not on an antipsychotic medication immediately before initiating clozapine had tapered off paliperidone a few weeks prior to initiation of clozapine. At 1 year after clozapine initiation, 10/40 (25%) were on multiple antipsychotics simultaneously. Thus, there was a trend toward reducing antipsychotic polypharmacy for those who remained on clozapine, from 38.5% to 25%, though this was not statistically significant (p = 0.232). The number of patients who were on an SSRI or a medication used to target sleep increased, and the number of patients who were on a stimulant medication or propranolol remained the same.
Psychotropic Medications for Patients Who Remained on Clozapine (n = 40)
Patients may be on more than one medication.
Included any antipsychotic, including clozapine.
Medications used to target sleep included mirtazapine, trazodone, tricyclic antidepressants, Z drugs, and benzodiazepines. At time of clozapine initiation, of the nine patients on trazodone, one patient was on daytime and evening trazodone as opposed to only evening trazodone. One year after clozapine initiation, of the 13 patients on trazodone, 1 patient was on daytime and evening trazodone as opposed to only evening trazodone.
SSRI, selective serotonin reuptake inhibitor.
Of the 40 patients who remained on clozapine for the duration of the review period, the number of hospitalizations and ED presentations for either psychiatric concerns or for medical concerns potentially related to use of clozapine significantly decreased in the year following clozapine initiation compared with the year prior to clozapine initiation. The average number of hospitalizations or ED presentations in the year prior to clozapine initiation was 3.48, whereas the average number of hospitalizations or ED presentations in the year after clozapine initiation was 2.13 (p = 0.010). Of the 40 patients in this group, 27 had fewer hospitalizations and ED visits in the year after clozapine initiation compared with the year before, 7 had the same number of hospitalizations, and 6 had an increased number of hospitalizations.
Of the 40 patients who remained on clozapine, CGI-S was available for 33 patients at time of clozapine initiation and for 31 patients 1 year later. CGI-I was available for 25 patients at time of clozapine initiation and for 31 patients 1 year later. Twenty patients had CGI-S and CGI-I data at both time points. Of the 18 patients who stopped clozapine, CGI-S was available for 15 patients at time of clozapine initiation and for 11 patients at time of clozapine discontinuation. CGI-I was available for 12 patients at time of clozapine initiation and for 12 patients at time of clozapine discontinuation. Ten patients had CGI-S and CGI-I data at both time points.
Both groups (those who remained on clozapine and those who stopped clozapine) had the same mean CGI-S of 5.73 at time of clozapine initiation (Table 5). In those who remained on clozapine, 1 year after clozapine initiation, mean CGI-S was 5.58, and mean CGI-I was 2.52. In those who stopped clozapine, at the time of decision to stop clozapine, mean CGI-S was 5.82, and mean CGI-I was 3.50. CGI-S was not significantly different between groups at the end of clozapine treatment (p = 0.53). CGI-I was not different between continuation and discontinuation groups at time of initiation of clozapine (p = 0.884) but was significantly lower in the continuation group at 1 year after initiation versus the discontinuation group at the time of discontinuation (p < 0.01). For the 20 patients in the continuation group for whom both initial and 1-year CGI-I data were available, paired analysis showed a significant reduction in CGI-I scores by the 1-year timepoint of continued clozapine use (p < 0.001) (Fig. 2).
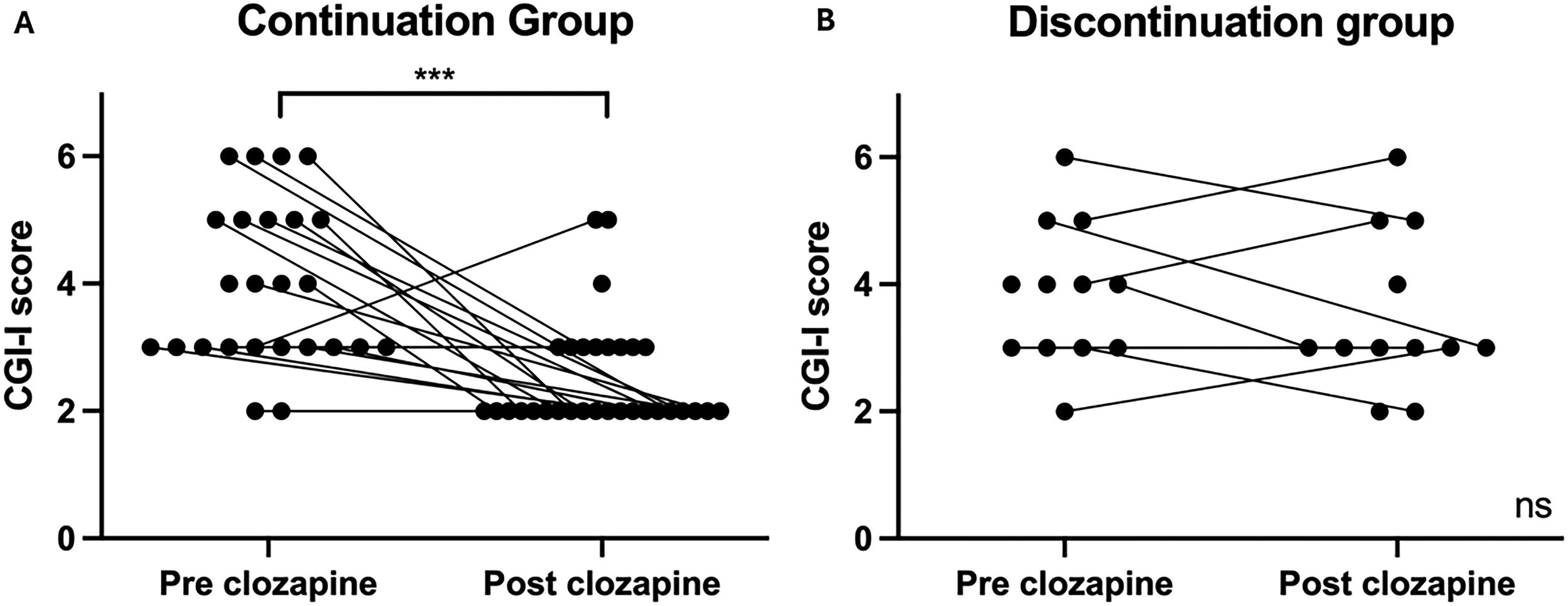
Individualized CGI-I scores. CGI-I scores were collected during clinical encounters. Note that “pre” refers to time of clozapine initiation. “Post” refers to 1 year after clozapine initiation in the continuation group and to time when decision was made to discontinue clozapine in the discontinuation group.
Mean CGI-S and CGI-I Scores
significant difference in CGI-I at initiation compared to CGI-I 1 year later for those who remained on clozapine, p <0.001.
CGI-I, Clinical Global Impressions-Improvement; CGI-S, Clinical Global Impressions-Severity; SD, standard deviation.
Side effects potentially related to clozapine were reported in patients who remained on clozapine, though these side effects did not appear severe enough to prompt discontinuation of clozapine. Side effects noted within the year following clozapine initiation included akathisia, anemia, constipation, drooling, drowsiness, increased appetite, nocturnal enuresis, odd gait, tics, and urinary accidents. The most common side effects were constipation, drooling, and drowsiness.
Discussion
The primary purpose of this article was to review the safety, tolerability, and effectiveness of clozapine in youth and young adults with autism and/or intellectual disability. Previous research has involved smaller case reports or cohorts, so the goal of this research was to assess a larger group of patients, as this appears to be the largest case series to date. Overall, clozapine was well-tolerated in this population, as demonstrated by the majority of patients remaining on clozapine for the time period assessed.
One of the major concerns related to clozapine use is the risk of agranulocytosis. Of the 58 patients reviewed in this study, only one was affected by neutropenia that was a contributing factor in the decision to stop clozapine, though it was not the only factor, and there was not a period of increased lab monitoring to see if labs normalized prior to stopping clozapine. Another concern related to clozapine use is the feasibility of obtaining the required monitoring labs. Of the 58 patients in this study, only 3 stopped clozapine due to difficulty with blood draws, suggesting that this was less of a limitation than might be expected, even in a population that could be thought of to have more difficulty with lab draws than other populations. Many of these patients had access to a specialized neurobehavioral psychiatry clinic including a behavior support team during blood draws, which is likely an extremely helpful component to consider in this population to ensure success of lab draws. Some of these patients also had nurse care managers to assist with reminders about the need for lab draws and to ensure the REMS program and patients’ pharmacies were updated on lab results.
Cardiomyopathy is a risk factor associated with the use of clozapine. Concern for possible myocarditis affected only 1 of the 58 patients in this study. This was based solely on tachycardia and was not a confirmed case of myocarditis. Many of the patients in this sample were thought to be unable to tolerate obtaining a baseline echocardiogram without the need for sedation, which poses its own risks. C-reactive protein (CRP) and troponin appear clinically useful in monitoring for cardiomyopathy, as opposed to monitoring tachycardia alone. The latter appears nonspecific, and if interpreted in isolation, it may lead to unnecessary discontinuation of clozapine due to oversuspicion of myocarditis (Segev et al., 2021). Therefore, our group has come to a consensus to check a CRP and troponin level with weekly CBC monitoring for the first 6–8 weeks of clozapine use, hopefully allowing for earlier recognition of any potential concern for myocarditis.
Weight gain is also a potential side effect of clozapine. Surprisingly, clozapine was not associated with an increase in BMI Z-score during the 1 year after clozapine initiation. Some individuals had weight and BMI increases, while others had reductions. This finding is counterintuitive given that clozapine is associated with weight gain in nearly two-thirds of youth treated with clozapine (Adnan et al., 2022) and associated with weight gain over many years (Henderson et al., 2000). Interestingly, a case series of youth and young adults with neurodevelopmental disorders who were on clozapine also found variable changes in weight (Wink et al., 2016). It is possible that the preexisting pharmacologic treatment with other medications associated with weight increase may have contributed.
Constipation was a relatively frequent occurrence with clozapine treatment, and it should be closely monitored in this patient population, with the consideration to involve primary care or gastroenterology for management when needed.
The number of medications these patients were on speaks to the severity of illness in these youth and young adults. While clozapine is not considered a first-line treatment option, it should be considered as an option for those with severe illness but only after consideration that the possible benefits outweigh the potential adverse effects of clozapine. Observed benefits related to clozapine use included a decrease in number of hospitalizations and a trend toward reduced need for antipsychotic polypharmacy. Access to psychiatric inpatient units has become more limited with the rise in pediatric mental health concerns. Hospitalizations also represent a significant cost to families and the healthcare system, so reducing hospitalizations could allow for reduced healthcare costs. Antipsychotic polypharmacy can increase the risk of side effects, so the possibility for clozapine to allow for a reduction in antipsychotic polypharmacy could potentially lower this risk.
There were three patients not included in this data analysis who had two trials of clozapine. One stopped due to sedation and aggression, one stopped due to recurrent strep throat and urinary tract infections, and one stopped due to a hospitalization involving pneumonia, pleural effusion, and acute kidney injury. All three patients were retried on clozapine, with the time between stopping and restarting ranging from 5 days to 5 months. Two of the three patients then remained on clozapine through the remainder of the study period, whereas the third patient stopped clozapine again for an unknown reason. This suggests that retrial of clozapine can be safely considered for some patients.
This study does have several limitations. It was a retrospective review of real-world clinical cases rather than a prospective or randomized, placebo-controlled trial. It compared those who remained on clozapine to those who stopped clozapine, and it also compared data from before versus after patients were on clozapine. Some patients who were initially prescribed clozapine were lost to follow up and excluded from our analysis. Some data were not available for all patients, most notably involving data around CGI scores. Another limitation is the severity of symptoms in this population, with many patients having been on numerous medications and with significant irritability, aggression, and/or self-injury, so these results could be difficult to generalize.
The study only looked at ED visits and hospitalizations in the 1 year after clozapine initiation, so longer-term outcomes related to ED visits and hospitalizations were not assessed. Regardless of a patient’s duration on clozapine, data analysis was only done on information from 1 year before through 1 year after clozapine initiation. Given that the average length of time on clozapine for those who remained on it for the duration of this study was 34 months, there is likely additional information from beyond 12 months of treatment which could be useful to explore in future studies. The retrospective nature of the study did not allow for reliable assessment of behavioral or symptomatic changes beyond the measures of ED visits, hospitalizations, and CGI data when available. CGI data also speak to the severity of the patient population. However, limitations around interpretation of CGI data include this being a clinical setting rather than a research setting, and the CGI scores were sometimes determined by different providers at different time points. Scores were not always documented at each visit, resulting in incomplete data for many patients, making it difficult to fully interpret the outcomes found on analysis of CGI scores.
Being a retrospective study, it could not control for possible positive effects of increased clinical attention and safety monitoring due to initiation of clozapine. It also could not control for possible improvements occurring naturally over time or for possible benefit from other comprehensive treatment interventions, such as behavioral therapies or community supports, though the presence of CGI-I improvement only in the group that continued clozapine does speak to the utility of the treatment.
Future studies looking at larger samples of youth and young adult patients with autism and/or intellectual disability, following patients over a longer duration, and using additional behavioral outcomes measures would be helpful next steps.
Conclusion
Use of clozapine in youth and young adults with ASD and/or intellectual disability is generally well-tolerated. In the year following clozapine initiation, observed benefits included a significant decrease in number of hospitalizations and ED visits, clinical improvement as shown by significant reduction in CGI-I scores, and a trend toward decreased need for antipsychotic polypharmacy. While clozapine is not considered a first-line treatment option, in youth and young adults with ASD and/or intellectual disability who continue to have severe irritability, aggression, and/or SIBs despite trials of other medications as well as behavioral interventions, clozapine should be considered as an option.
Clinical Significance
We found that use of clozapine in youth and young adults with ASD and/or intellectual disability is well-tolerated and shows possible benefit. These findings suggest using clozapine in this population should be considered if other treatment options are not successful.
Footnotes
Acknowledgments
The authors would like to thank Cincinnati Children’s Hospital Medical Center and the members of the Neurobehavioral Psychiatry team.
Authors’ Contributions
K.H.: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, visualization, writing—original draft, and writing—reviewing and editing. C.F.: Conceptualization, visualization, writing—original draft, and writing—reviewing and editing. K.J.Z.: Data curation, formal analysis, visualization, and writing—reviewing and editing. K.C.D.: Writing—reviewing and editing. M.L.: Conceptualization, data curation, investigation, methodology, resources, supervision, visualization, and writing—reviewing and editing.
Disclosures
M.L. has received past research funding from Impel Pharmaceuticals, Ovid Therapeutics, Roche, and the Simons Foundation. K.C.D. has received past research support from Ovid Therapeutics, Roche, and the Simons Foundation. All other authors have no disclosures or conflicts of interest.