
Abstract
Objective:
Pharmacoepidemiologic research shows increasing use of polypharmacy to manage behavioral treatment of youth. Methods to increase precision, for example, competing risk analysis, to capture psychotropic patterns of concomitant stimulant treatment changes over time have not been explored.
Methods:
A retrospective cohort study was derived from Medicaid enrollment data, prescription drug, and clinician-reported diagnosis claims data from 2007 to 2014. Youths aged 2–17 years with 1–7.5 years of continuous enrollment who were new users of stimulants were followed. Major outcomes include detailed changes of concomitant use according to the number of psychotropic classes (NPC); competing risk assessment of patient factors according to NPC; and time factors related to changes in NPC.
Results:
Among 30,294 new stimulant users, 75.5% remained on stimulant monotherapy and 24.5% had stimulant concomitant regimens. Among the latter, great flux was observed, revealing exposure to combinations changed substantially across time. As a proportion of all changes, retention of the maximum NPC was observed for 65.3% of 2 concomitant classes, 56.2% of 3 concomitant classes, and 57.1% and 56.2% of 4 and 5 concomitant classes, respectively. Median duration according to NPC showed a linear decrease in time from 223 days for 2 classes, 172 days for 3 classes, 141 days for 4 classes, and 113 days for 5 classes combinations. By contrast, the path to maximum NPC regimens took median times of 491-833 days as NPC increased from 2 to 4 concomitant classes. Competing risk analysis demonstrated significantly increased hazard ratios according to the number of concomitant classes for 12–17-year-olds, patients with foster care or disability coverage, and those with 3–4 years of continuous enrollment.
Conclusions:
Detailed NPC changes illustrate great flux in concomitant stimulant patterns among Medicaid-insured youth. Competing risk analysis brings more precise patient characteristics risk information to assess NPC changes compared with a binary model.
Introduction
Stimulants have been the most common psychotropic medication class for the treatment of pediatric attention-deficit/hyperactivity disorder (ADHD) for more than 25 years. Clinician-reported ADHD diagnosis and stimulant usage in community-treated populations have increased substantially in the United States. For example, Zhang et al. assessed 1999–2015 national data and found ≥2 psychiatric diagnoses grew from 57.8% to 77.7% of youth across 17 years. Also, stimulants from 1990 to 2010 were the most common psychotropic class among youth with polypharmacy (concomitant use) regimens (77.8%–82.1%) (Zhang et al., 2021). Similarly, in a national survey of physician office visits across 12 years, Girand et al. found ADHD medication (essentially stimulants) virtually doubled from 4.8% to 8.4% and ADHD psychotropic polypharmacy increased from 16.8% to 20.5% (Girand et al., 2020).
In recent years, stimulant polypharmacy including antipsychotics (Raman et al., 2018; Sultan et al., 2019; Varimo et al., 2023), antidepressants (Girand et al., 2020), and alpha-agonists (Lohr et al., 2018) has grown substantially, particularly among publicly insured youth. Some articles reflect negatively on polypharmacy. However, Chen et al. noted that “Despite the paucity of evidence for and against polypharmacy, in some situations short-term polypharmacy is clearly appropriate or even necessary. For example, to cross-titrate two drugs.” (Chen et al., 2011). In this study, we use “stimulant concomitant treatment” [with (inter-class) psychotropic classes] to describe stimulant “polypharmacy.” Notably, physicians can appropriately prescribe concomitant regimens according to FDA guidelines (Roberts et al., 2003). However, complex regimens in vulnerable populations, for example, foster care youth, receive monitoring oversight at both federal (GAO, 2017) and state (ColoradoDUR, 2017) levels.
To address the evolution of patterns of concomitant stimulant regimens, that is, the change from stimulant monotherapy to 2, 3, 4, or 5 as the number of psychotropic classes (NPC) used, we undertook a retrospective cohort analysis among those with at least 1 and up to 7.5 years of continuous Medicaid enrollment. With rare exception (Winterstein et al., 2017), previous studies have been limited to a cross-sectional framework, typically annual trends, (Chen et al., 2011; Davis et al., 2021; Soria Saucedo et al., 2018; Spencer et al., 2013; Wu et al., 2018; Zito et al., 2020) as opposed to a longitudinal framework. In this study, we aimed to capture the patient’s longitudinal journey through concomitant stimulant use based on a detailed temporal sequence of NPC changes: patients usually start with stimulant monotherapy and if the prescriber determines that a stimulant isn’t sufficiently effective, s/he may prescribe additional concomitant psychotropic class(es). The NPC may reduce over time, for example, if symptoms diminish or complex regimens bring adverse effects.
In the case of multiple possible events, for example, increasing from monotherapy to 2, 3, 4, or 5 NPC and then back to a lower NPC or monotherapy, where one event can be affected by other events, competing risk analysis can provide more detailed patient information into the likelihood of each NPC option and in relation to patient characteristics risk factors.
Methods
Data source
The data source comprises the 2007–2014 Medicaid administrative claims data from a mid-Atlantic state, which included enrollment files, outpatient and physician claims files, and dispensed prescription drug files. The files in the data source were linked together via an encrypted identification number.
The enrollees’ sociodemographic characteristics, monthly Medicaid enrollment status, and Medicaid eligibility category are included in the enrollment files. The clinician-reported psychiatric diagnoses are based on the ICD-9-CM codes located in the outpatient physician claims files. The prescription dispensing information such as national drug codes, dispensing date, days supplied, and quantity supplied are included.
This study was reviewed and approved by the Institutional Review Board of the University of Maryland, Baltimore.
Study design and study population
We used a retrospective cohort design to reflect the NPC changes in new stimulant users with up to 7.5 years of follow-up in the database. The design allowed us to detail the patient’s journey through concomitant treatment and to assess the association between patient characteristics and the probability that a stimulant user would have additional dispensing for psychotropic drug classes. A graphical depiction of patterns of NPC changes is shown in Supplementary Figure S1.
The Medicaid enrollment data were generated based on each patient’s monthly Medicaid enrollment status. To be eligible for a full-year enrollment, the patient had to be enrolled at least 10 months per year (Zito et al., 2013). The patient’s daily stimulant usage was calculated based on the stimulant dispensing dates, days supplied, and allowable 15-day gaps for prescription refills. Based on daily stimulant usage in the database, we built a daily stimulant usage string for up to 7.5 years for each patient in the study within their continuous enrollment period. Following the same methodology, daily usage of the other six psychotropic classes was calculated as well. All patients were followed to the end of drug therapy or end of 2014, whichever came first.
Psychotropic medication and concomitant use
Psychotropic medications were grouped into seven classes according to the classification system of the American Hospital Formulary Service (AHFS, 2024): antipsychotics, anxiolytics, antidepressants, anticonvulsant-mood stabilizers, stimulants, selected alpha-agonists, and lithium (Supplementary Table S1).
Stimulant concomitant use was defined conservatively as at least 60 consecutive overlapping days of stimulant use that included the concomitant use of ≥1 other psychotropic class.
We defined five mutually exclusive groups in which we classified each patient’s maximum NPC taken concomitantly with stimulants: stimulant monotherapy; concomitant stimulant therapy with 2–5 NPCs.
Outcome measures
Patient characteristics and diagnostic factors of stimulant monotherapy and concomitant users
Patient characteristics included age group at initial start of stimulants (2–5 years old, 6–11 years old, 12–17 years old), gender, race/ethnicity (White, African American, Hispanic, Native American/Asian/Pacific Islander, and Unknown), Medicaid eligibility category (foster care, State Children’s Health Insurance Plan, supplemental security income [SSI], and temporary assistance for needy families [TANF] for youth eligible by family income at or below the federal poverty level) and length of continuous Medicaid enrollment (1–2 years, 3–4 years, 5–6 years, 7–8 years).
For psychiatric diagnoses, we grouped ICD-9 codes for clinician-reported diagnoses into 11 categories (Supplementary Table S2).
Maximum NPC
Supplementary Figure S1 illustrates complexity of stimulant users’ changes according to NPC. Among new stimulant users, some patients changed to 2 NPC over time, some changed to 3, 4, or 5 NPC, while others continued stimulant monotherapy until the end of the study. During the change, patients received additional psychotropic class(es) until maximum NPC, decreased to a lower NPC, or remained at the same NPC. Among the various changes, 468 patients (1.5%) had 2 or more of the same NPC. For example, a change from 2 NPC increased to 3 NPC and then decreased to 2 NPC and increased to 3 NPC again. A sensitivity analysis showed no significant difference between the average change time of multiple changes and the first change time (data not shown). In such cases, we kept the first change.
Duration of concomitant change
In each change, duration of concomitant use (days) was calculated based on the start date of stimulant monotherapy or NPC and the start date of next level of NPC or the last date of the study period.
Time to maximum NPC
Time to maximum NPC was calculated from the start date of stimulant or initial NPC and start date of maximum NPC. The median and interquartile range (IQR) of time to maximum NPC were calculated.
Event of interest and hazard ratio using competing risk analysis
Maximum 2 to 5 NPCs are the events of interest in the competing risk analysis, and stimulant monotherapy is used as the reference group. Finally, the adjusted sub-hazard ratios (SHRs) for patient characteristics in relation to NPC regimen changes were assessed using a competing risk model described further in the section “Statistical Analysis.”
Statistical analysis
The demographic characteristics and clinician-reported psychiatric diagnosis in the monotherapy group, maximum 2, 3, 4, and 5 NPCs were assessed (number and percent). Characteristics between different groups were compared using χ2 test for categorical variables.
The number and percent of patients with NPC changes were calculated. Duration of NPC changes was calculated and presented as median, minimum, maximum, and IQR. The linear trends for patient characteristics within the maximum NPCs were tested using the Cochran-Armitage trend test.
The association between patient characteristics and various maximum NPC regimens was assessed by competing risk analysis using Fine and Gray’s proportional hazards regression model (Supplementary Fig. S3). This approach is an extension of the Cox proportional hazard model and accounts for competing events by modeling the effect of the patient characteristics on the sub-distribution hazard.
The association between patient characteristics and NPC is reflected by the SHR, which is the ratio of hazards associated with the cumulative incidence function in the presence of a competing risk. We also tested the linear trends for SHR within NPCs using the Cochran-Armitage trend test.
Binary survival analysis using the Cox regression model was used to assess the association between patient characteristics and any NPC and evaluated hazard ratios of the characteristics. A two-sided p value <0.05 was considered statistically significant. All analyses were done using SAS software (version 14.0).
Results
Maximum NPC
Among 2–17-year-old stimulant users with 1–7.5 years of continuous Medicaid enrollment, 30,294 were new stimulant users with clinician-reported diagnoses (Supplementary Fig. S2). During the follow-up period, 75.5% (N = 22,882) continued stimulant monotherapy while the remaining 24.5% changed to NPC: 16.5% (N = 5,004) had maximum 2 NPC, while 5.4% (N = 1,634), 2.2% (N = 671), and 0.3% (N = 103) had maximum 3, 4, and 5 NPC regimens, respectively (Supplementary Fig. S3).
Patient characteristics in stimulant monotherapy and maximum NPC
Characteristics of the study population are presented in Table 1 according to stimulant monotherapy or maximum NPC. Among monotherapy users, the majority (45.3%) were 6–11 years old; proportionately more were male (66.0%) and African American (46.2%). A majority of patients in the monotherapy group had family income below the poverty level, that is, TANF (55.0%), and had 7–8 years of continuous enrollment (57.3%) (Table 1).
Demographic and Administrative Characteristics of Stimulant Monotherapy Users and Stimulant Concomitant Users Among Those with 1–7.5 Years of Continuous Enrollees
Age is the age of first stimulant use (column 2) or age of first drug/medical service use (column 4).
NPC, number of psychotropic classes; SCHIP, State Children’s Health Insurance Program; SSI, supplemental security income; TANF, temporary assistance for needy families.
Across the maximum NPC for 2, 3, 4, and 5 NPC, the percentages for 12–17-year-olds, White youth, and patients with foster care or SSI coverage, increased linearly. Linear trends were also observed for continuous enrollment of 3–4 and 7–8 years (Table 1).
Concomitant therapy pathways
The pathways for various NPCs are described according to the initial number of concomitant psychotropic classes (Fig. 1A–E). The multiple pathways reveal the rationale for a competing risk analysis. Among the 30,294 stimulant users, 708 patients were excluded because they initiated treatment with NPC. In 29,586 patients who began monotherapy, 22,882 (77.3%) patients continued with stimulants as the only psychotropic medication, 5357 (18.1%) patients switched to 2 NPC, and less than 5% of patients escalated to 3, 4, or 5 NPC regimens (Supplementary Table S3).

Detailed patterns of stimulant monotherapy and concomitant use according to NPCs*. *It is based on each patient began follow up. **Stimulant only transition does not include 708 patients who started the treatment with 2 or 3 or 4 or 5 NPCs. NPC, number of psychotropic classes.
Among the NPC changes, a majority of patients stayed with NPC: 4080 (65.3%) patients stayed with 2 NPC until the end of the study; 1245 (56.2%) patients stayed with 3 NPC; 425 (57.1%) and 58 (56.2%) patients had 4 and 5 NPC regimens, respectively (Supplementary Table S3).
For patients with a higher NPC, some decreased to a lower NPC, for example, 33 (32.0%) dropped from 5 NPC to 4 NPC, 202 (27.1%) patients dropped from 4 NPC to 3 NPC, and 548 (24.7%) patients dropped from 3 NPC to 2 NPC regimens. Supplementary Table S3 details these patterns.
Time to next NPC
The median, minimum, and maximum (days) for the stimulant and NPC changes are presented in Supplementary Table S4. For patients who started on stimulant monotherapy, the median time was 471 days, time to go to 2 NPC was 448 median days, to 3 or 4 NPC was 334 median days and 365 median days, respectively, and to 5 NPC regimens was median 259 days.
As the NPCs increased, the duration of staying in the same NPC decreased. Thus, the median time of exposure according to the NPC showed a linear decrease in time from 223 days for 2 NPC, 172 days for 3 NPC, 141 days for 4 NPC, and 113 days for 5 NPC.
For patients with a higher NPC, it took more than 1 year to decrease to a lower NPC. For example, 417 median days were used to drop from NPC 5 to NPC 3, and 437 days to drop from NPC 4 to NPC 2.
Time to maximum NPC
The median, minimum, maximum, and IQR (days) for time to maximum NPC are presented in Figure 2 and Supplementary Table S5. Among initial monotherapy users, it took 491 and 577 median days to reach a maximum of 2 or 3 NPCs, respectively, and 833 median days to maximum 4 NPC, and 789 median days to maximum 5 NPC, respectively. The median time to maximum NPC increased in patients with higher NPC (491 days and 577 days for maximum 2 or 3 NPC, and 833 and 789 days for maximum 4 or 5 NPC, respectively). However, there was no significant difference in the maximum time to 3, 4, or 5 NPC (2591 days, 2548 days, and 2555 days), respectively.
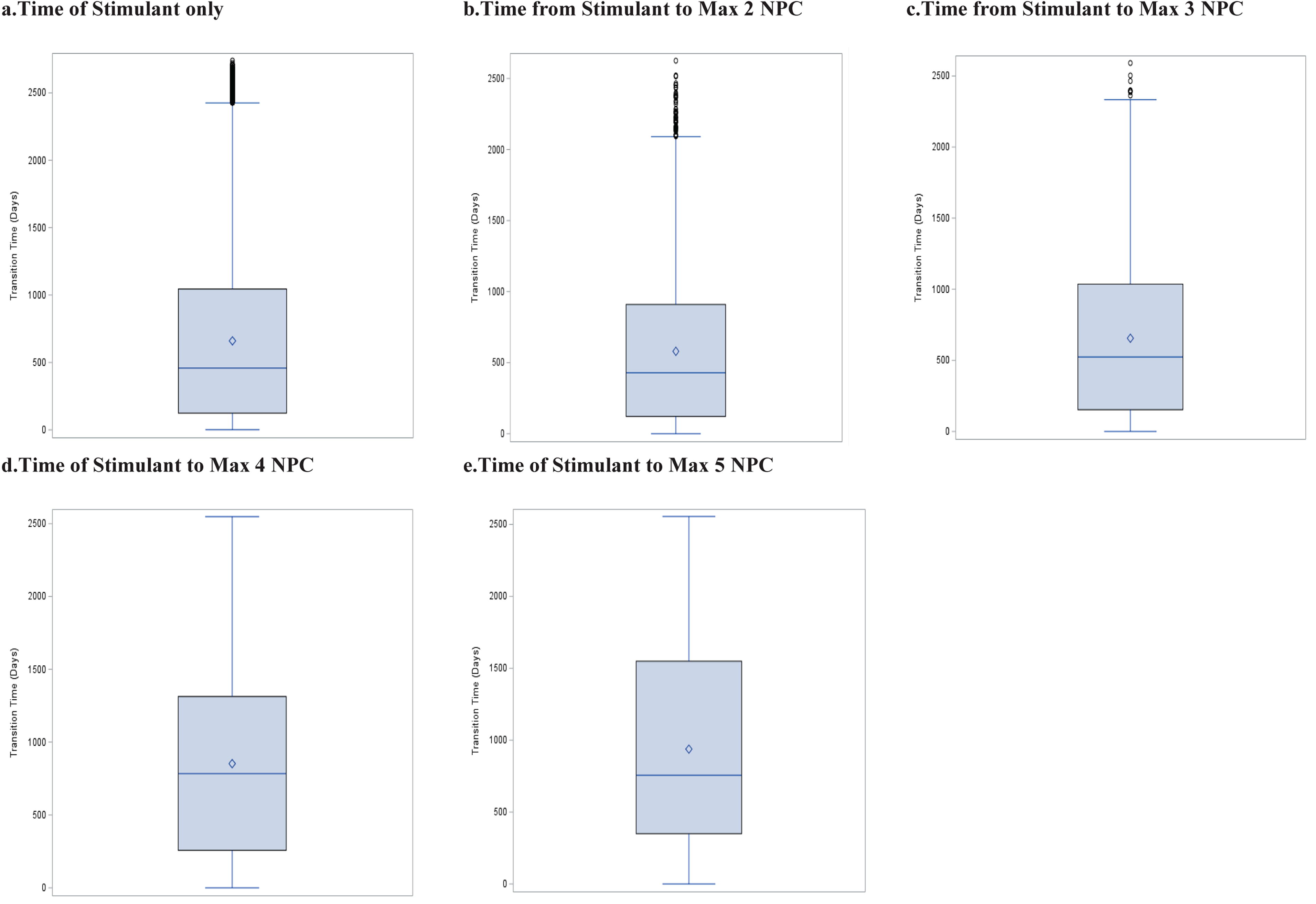
Graphic description of range of time from stimulant to maximum NPC*. *The horizontal line in the box denotes the median value (50th percentile), the diamond represents the mean value, and the blue box contains the 25th to 75th percentiles of data. The whiskers mark the 5th and 95th percentiles, and values beyond these upper and lower bounds are considered outliers. NPC, number of psychotropic classes.
Clinician-reported psychiatric diagnosis in stimulant monotherapy and concomitant users
The frequency of psychiatric comorbid diagnoses according to NPC is presented in Supplementary Table S6. Large increases in clinician-reported comorbid psychiatric diagnoses are associated with concomitant regimens. For example, manifold increases in bipolar disorder (941% increase), schizophrenia (739% increase), and autism (457% increase) were observed in maximum 5 NPC compared with stimulant only.
Competing risk analysis for stimulant monotherapy to maximum NPC
Table 2 shows the adjusted SHR for patient characteristics in a competing risk model and in a binary model (columns 8 and 9). In the competing risk model, compared with stimulant monotherapy, there was a linear relationship between several patient characteristics and 2, 3, and ≥4 NPC: age group 12–17 (HR = 0.71, p < 0.001), White race (HR = 1.34, p < 0.001), patients in foster care (HR = 1.50, p < 0.001) and SSI (HR = 1.02, p < 0.05), and with 3–4 years continuous enrollment (HR = 1.09, p < 0.05).
Adjusted Sub-Hazard Ratio for Stimulant Monotherapy to Maximum NPC Using Competing Risk Model Compared with Binary Model (Columns 8 and 9)
CI, confidence interval; NPC, number of psychotropic classes; SCHIP, State Children’s Health Insurance Program; SSI, supplemental security income; TANF, temporary assistance for needy families.
The results from the binary analysis showed several risk factors are correlated with any NPC (2, 3, 4, and 5 NPC): White (HR = 1.46, p < 0.001), patients with foster care (HR = 2.03, p < 0.001), SSI (HR = 1.43, p < 0.001), 3–4 years of continuous enrollment (HR = 1.18, p < 0.001). Nevertheless, the impact of these factors was substantially increased in the competing risk model.
Common concomitant stimulant regimens
The various combinations of psychotropic classes in 2, 3, 4, and 5 maximum NPC were investigated. In summary, 85% of the maximum 3 NPC, 88% of the maximum 4 NPC, and 90% of the maximum 5 NPC had a regimen that included a stimulant with at least one antipsychotic dispensing for 60 or more days of concomitant use (Table 3).
Top Three NPC Regimens
AA, alpha agonist; ATC-MS, anticonvulsant-mood stabilizer; ATD, antidepressant; ATP, antipsychotic; AX, anxiolytic; NPC, number of psychotropic classes.
In maximum 3 NPC, the most prevalent combination was “stimulant, antipsychotic and antidepressant.” In maximum 4 NPC, the most prevalent combination was “stimulant, antipsychotic, antidepressant and alpha agonist”; in maximum 5 NPC, the most prevalent combination was “stimulant, antipsychotic, antidepressant, alpha agonist and anticonvulsant-mood stabilizer” (Table 3).
Discussion
To our knowledge, this is the first study using a competing risk methodology for pediatric psychotropic stimulant concomitant treatment illustrating changes in the NPCs across lengthy enrollment periods in a real-world population; the findings show patient characteristic risk factors had a significantly greater impact with a higher NPC. We are unaware of any study that investigated the change from monotherapy to concomitant use in terms of change from 2 classes to 3, 4, or 5 classes. Details of the changes in the NPCs in this study are novel and illustrate the dynamic nature of regimens of stimulants concomitant with other psychotropic classes.
The major findings of this study include: Among new stimulant users, 24.5% had 2–5 NPC regimens within 1–7.5 years of follow-up with a median of 2.2 years for patients to reach a maximum of 5 NPCs. During the follow-up, the majority (49.6%) increased to a higher NPC while 36.3% stayed at maximum NPC and 14.1% decreased their NPC. Patients who started concomitant use took substantial time to change to the next higher or lower NPC or to stay at the same NPC. Concomitant therapy was used for relatively long periods and the treating physician has adjusted the regimen for various reasons. Perhaps if it was not effective or adverse drug events were not tolerated or acute symptoms have resolved. The competing risk model showed that NPC changes brought more risk factor information compared with a binary model. For example, foster care patients were more likely to have ≥4 NPC using competing risk rather than using a binary model which is limited to any NPC (HR 5.66 vs. 2.03, respectively). NPC patterns in this large cohort emphasize the complexity of psychotropic class treatment patterns for youth: the majority (49.6%) of NPC changes involved an increased NPC, while one third (36.3%) stayed at their maximum NPC and 14.1% had a decreased NPC (Supplementary Table S7).
Overall, the findings provide details on the patterns of polypharmacy over time and will generate hypotheses for future research studies on the effectiveness, safety, and tolerability of complex polypharmacy regimens.
Comparison with published polypharmacy (concomitant use) studies
Published studies of the past 15 years have featured inter-class polypharmacy (concomitant use). Polypharmacy has been variously defined as 2 or more concomitant psychotropic classes of medications with an overlapping prescription window of varying duration including 15 days (Wu et al., 2018), 30 days (dosReis et al., 2011; Spencer et al., 2013), 45 days (Soria Saucedo et al., 2018), and 60 days (Chen et al., 2011; Zito et al., 2020). We chose a conservative window of 60 days or more to minimize the chance of intentional switching of drugs. We also conducted a sensitivity analysis for 30-day overlapping windows for concomitant use and observed similar findings (data not shown).
In terms of prevalence, in this study, we found 75.5% of patients had stimulant monotherapy, and 24.5% of patients had stimulant concomitant use. This result aligns with Girand et al.’s finding that ≥2 ADHD drugs + other psychotropic classes increased from 26.0% to 40.7% across 10 years using NAMCS 2006–2015 data (Girand et al., 2020); Chen et al.’s finding that 20.9% of youth with ≥2 polypharmacy occurred among 6–18-year-olds in 2005 Medicaid data from four states (Chen et al., 2011). Zhou et al. found that ≥1 psychotropic concomitant medication occurred in 22.9%–25.0% of children and 25.2–28.2% of adolescents using U.S. privately insured data (Zhou et al., 2020). Zhang et al. assessed national Medical Expenditure Panel Survey (MEPS) data and found that ≥3 class concomitant therapy doubled in 12 years (Zhang et al., 2021).
Distinct from published studies, which use a broad definition of polypharmacy (2 or 3 NPCs) (Zhang et al., 2021), this study focused on specific NPC changes from 2 to 5 classes and evaluated the changes with greater precision. In this study, we described detailed information for providing each NPC change using community treatment data. It demonstrates the complexity of each regimen change: the patients’ polypharmacy journey is in a dynamic pattern. Few patients stayed in the higher NPC suggesting several possibilities: symptoms may have resolved, patients may have experienced adverse drug events or a lack of improvement.
Patient characteristics’ risk factors associated with NPC
Psychiatric polypharmacy has been shown to be associated with male, older, White, and foster care youth, from the traditional binary model analysis: Chiang et al. found ≥3 psychotropic classes were significantly associated with youth who were in foster care (OR = 3.31); among 10–14-year-olds (OR = 1.94) and 15–17-year-olds (OR = 2.41); and among White (OR = 2.0) (Chiang et al., 2024). In another study, compared with 2–3 class polypharmacy, 4–5 class polypharmacy was significantly more likely to occur in males (OR = 1.66) and patients in foster care (OR = 1.66) (Keast et al., 2019).
In this study, the competing risk analysis suggested patients who are 12–17-year-olds, male, White, with 3–4 years of enrollment, and enrolled in foster care or SSI had a higher risk of developing concomitant use in higher NPC than those in the binary model. For example, the hazard of foster care was 3.12 and 5.66 times more likely to have 3 and ≥4 NPC and was 2.03 more likely for any NPCs.
Future research
Numerous authors emphasize off-label use suggesting the possibility of insufficient effectiveness and safety data in community-treated populations. An extensive literature review of concomitant regimens in pediatric psychopharmacology showed 2 NPC regimens (specifically stimulant and alpha agonist) have supportive evidence of effectiveness. Thus, combinations of ≥3 classes should receive targeted interventions to assess benefit-risk (Baker et al., 2021). With respect to safety, complex concomitant therapy increases the likelihood of adverse effects for combinations of 3, 4, or 5 NPCs (Jureidini et al., 2013). Similarly, in a questionnaire survey conducted with parents who filled a prescription for their children, the authors found that adverse events of psychotropic medications were more common and severe with the increasing number of medications use (Hilt et al., 2014). Other studies underscore Baker et al.’s call for the study of the effectiveness and safety of 3 or more class concomitant use. For example, in a 2015 international consensus of pediatric psychopharmacology investigators, research on the effectiveness and safety of commonly used off-label regimens was a leading priority (Persico et al., 2015). Future robust studies should assess the benefits and risks of complex NPC and establish the safety of the considerably long exposures seen in our study of Medicaid-insured youth. Large simple trials are suggested as a design for these studies (Stroup, 2011; Vitiello, 2015). The availability of electronic health records at major academic institutions points the way to conduct robust research that would not break the bank (Castillo et al., 2015) but would generalize to usual treatment patterns in community-treated populations.
Limitations
Several limitations which may bias the results should be noted. First, we focused on a single state Medicaid dataset. The results may not generalize to other state Medicaid populations. Second, there is likely to be information bias on the medication exposure and clinician-reported psychiatric diagnosis. The diagnoses are based on clinician-reported claims data and lack the reliability of research-assessed diagnoses. Third, the psychotropic medication dispensing in Medicaid may not mean the patient actually consumed the drug, although the frequently long exposures to medication in this dataset may reduce the likelihood that medications were not consumed. Fourth, a small group of patients had more than one series of variable changes or had different 2 NPC combinations. For example, 340 (1.12%) of patients had more than one 2 NPC regimen, for example, stimulant and antipsychotic, 102 patients had more than one 3 NPC, and 46 and 5 had 4 NPC and 5 NPC regimens, respectively (data not shown). To reduce the impact of multiple repeat changes from individual patients, we selected only the first transition change. Fifth, the reasons for changing/stopping polypharmacy are unclear and Medicaid claims data do not provide such information. Finally, information on provider type was not available for this study. Thus, the impact of provider type on the diagnosis and prescribing patterns could not be evaluated.
Clinical Significance
The findings of this study provide detailed information regarding patient risk factors’ effect on NPC. For example, the greater impact of foster care was on higher NPCs. In addition, the study estimated the substantial duration of NPCs including the time to maximum NPC. This new information sheds light on the impact of NPC changes. The results suggest close clinical monitoring for higher NPC regimens. Real-world clinical practices in community treatment involving 3 or more concomitant classes may carry risks of unnecessary and lengthy exposures to complex, typically off-label psychopharmacological regimens (Baker et al., 2021; Guthrie et al., 2015; Jureidini et al., 2013). These detailed patterns of NPC add new knowledge for close monitoring of pediatric stimulant psychotropic concomitant use, including NPC changes, time to next or maximum NPC, and on regimen complexity.
Conclusions
Detailed changes illustrate great flux in NPC patterns among Medicaid-insured youth. Competing risk analysis brings greater patient characteristics’ risk information to assess NPC changes compared with a binary model.
Footnotes
Disclosures
The authors declare that they have no relevant or material financial interests that relate to the research described in this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.