
Abstract
Importance:
Selective serotonin reuptake inhibitors (SSRIs) and cognitive behavioral therapy are the first-line treatments for pediatric obsessive-compulsive disorder (OCD) populations. Due to their limited effectiveness, additional treatment options are needed. A new potential pharmacological medication treatment avenue for OCD is intravenous (IV) ketamine.
Objective:
This study aimed to establish the feasibility, acceptability, and preliminary efficacy of an IV ketamine infusion for the treatment of refractory OCD in adolescents.
Design:
In this clinical pilot trial, every participant received IV ketamine infusion. Symptom severity and side effects were assessed daily for 2 weeks following the infusion.
Setting:
Study procedures were conducted at the New York State Psychiatric Institute, including a combination of in-person visits and phone calls.
Participants:
Five adolescents with OCD (age M, SD: 16.6 ± 1.5), who had previously failed trials of first-line treatments were enrolled.
Intervention:
All participants received an IV infusion of 0.5 mg/kg ketamine hydrochloride.
Main Outcomes and Measures:
A multimethod approach was applied, including physiological, self-report, and clinician-rated measures. To assess feasibility and acceptability, vital signs, electrocardiogram suicidality, self-reported adverse events, and dissociative symptoms were obtained. Obsessive-compulsive (OC) (Yale-Brown Obsessive Compulsive Challenge Scale, CY-BOCS) and depressive symptom severity, as well as global clinical impression, were assessed to investigate preliminary efficacy.
Results:
The mean (SD) pre- and 14-day posttreatment CY-BOCS were 29 (5.5) and 26.2 (5.6). There were no incidents of abnormal vital signs, mortality, or suicidal ideation in the 2 weeks following the infusion. All participants experienced mild dissociative symptoms in the 40 minutes after the IV ketamine infusion. Descriptively, OC symptom severity decreased immediately after the infusion but was not maintained over the course of the study.
Conclusions and Clinical Significance:
Ketamine is well-tolerated in adolescents with OCD and therefore appropriate for further efficacy testing.
Trial Registration:
ClinicalTrials.gov Identifier: NCT02422290.
Key Points
Introduction
Obsessive-compulsive disorder (OCD) is a disabling illness that often begins by adolescence and persists into adulthood (Nazeer et al., 2020).
The first-line treatments for pediatric OCD are the following: serotonin reuptake inhibitors, cognitive behavioral therapy, or the combination of both of these treatments (Pediatric OCD Treatment Study [POTS] Team, 2004). However, for treatment-refractory OCD there have been no new classes of Food and Drug Administration (FDA)-approved medications to treat youth with OCD since the development of selective serotonin reuptake inhibitors (SSRIs) over 40 years ago, and for some SSRIs, they provide only limited symptom relief (Kotapati et al., 2019). Thus, there is a need for alternative treatments in adolescents with OCD. In this study, we evaluated the feasibility, tolerability, and preliminary efficacy of intravenous (IV) ketamine, a medication that modulates glutamate in the brain, as a rapid treatment for obsessive-compulsive (OC) symptoms in adolescents. Our rationale for studying IV ketamine in adolescents diagnosed with treatment-refractory OCD is threefold. First, glutamatergic dysfunction in the cortico-striato-thalamo-cortical circuit is implicated in underlying OCD based on animal, genetic, imaging, and pharmacological studies (Karthik et al., 2020). Second, ketamine is FDA approved for anesthesia and chronic pain in children, adolescents, and adults (Kararmaz et al., 2004), which provides dosing and safety data for youth. Third, data from a small randomized controlled trial of unmedicated adults with OCD had a near cessation of obsessional thoughts during an IV ketamine infusion; these effects were maintained in half of the patients for up to 1 week (Rodriguez et al., 2013). These findings lead to two questions: (1) Is this type of study acceptable and feasible in youth? (2) Are IV ketamine’s effects similar in youth?
Methods
We recruited five adolescents (M = 16.6. years; SD = 1.52) with a principal OCD diagnosis who had previously failed at least one adequate trial of an SSRI or clomipramine and a course of cognitive-behavioral therapy (CBT/exposure and response prevention). Exclusion criteria included a history of violence, psychotic symptoms, posttraumatic stress disorder, autism spectrum disorder, pediatric autoimmune neuropsychiatric disorder, hypersensitivity or intolerance of ketamine, medical condition that might increase risk, adverse reaction to anesthesia, as well as current eating disorder and illicit drug use. Four out of five participants were female, and four out of five were Caucasian. The study was approved by the Institutional Review Board at the New York State Psychiatric Institute, and data were collected from March 2015 until February 2018 at the aforementioned institution. The first three participants enrolled completed a medication washout period before obtaining the IV ketamine infusion. To ease participants’ burden and after review of the literature, study procedures were changed to allow participants concurrent use of other medications with ketamine, including fluoxetine and clomipramine. After obtaining assent from adolescents and consent from their caregivers, each participant received an IV infusion of 0.5 mg/kg ketamine hydrochloride over a course of 40 minutes and was observed for 2 hours after the infusion. Following the day of the infusion, participants were closely monitored for a 2-week period through phone calls and in-person visits. Upon completion, participants were offered 3 months of open treatment for OCD (i.e., medication management and/or CBT) as clinically indicated.
Primary outcomes to assess the feasibility and safety of the IV ketamine infusions were participant-reported adverse events, vital signs, electrocardiogram, suicidality assessed via the Columbia-Suicide Severity Rating Scale (Posner et al., 2011), and dissociative symptoms assessed via the Clinician Administered Dissociative States Scale (CADSS) (Bremner et al., 1998). OCD and depressive symptom severity were assessed via self-report using a Visual Analogue Scale for the presence of obsessions (OCD-VAS), the Yale-Brown Obsessive Compulsive Challenge Scale (YBOCCS) (Goodman et al., 1989), and the Children’s Depression Rating Scale-Revised (CDRS-R) (Poznanski et a.l, 1985), as well as via clinician ratings using the Children’s Yale-Brown Obsessive Compulsive Scale (CY-BOCS) (Scahill et al., 1997) and Clinical Global Impressions Scale (CGI) (Guy, 1976). Treatment satisfaction was assessed via the Client Satisfaction Questionnaire 14 days following the infusion (Larsen et al., 1979).
Results
Demographics, safety and feasibility
Table 1 provides sample demographics and descriptions. There were no dropouts, and every participant completed all study visits. None of the participants had abnormal vital signs during the IV ketamine infusion, and there were no incidents of mortality or suicidal ideation in the 14 days following the infusion. All participants reported dissociative symptoms, and two participants reported dizziness following the start of the infusion (see Fig. 1). The dissociative symptoms assessed via CADSS were mild in severity both at 20 minutes (M = 9.6; SD = 7.1) and 40 minutes into the infusion (M = 7.4; SD = 4.8). Three out of five participants experienced a transient asymptomatic increase in the QTc readings as compared to baseline that remained within normal limits per physician calculation. All returned to baseline QTc readings. However, one participant was referred for a pediatric cardiology consultation as a precaution. Parent and adolescent treatment self-reported treatment scores were 25.75 (SD = 7.46) and 22.75 (SD = 6.18), respectively.
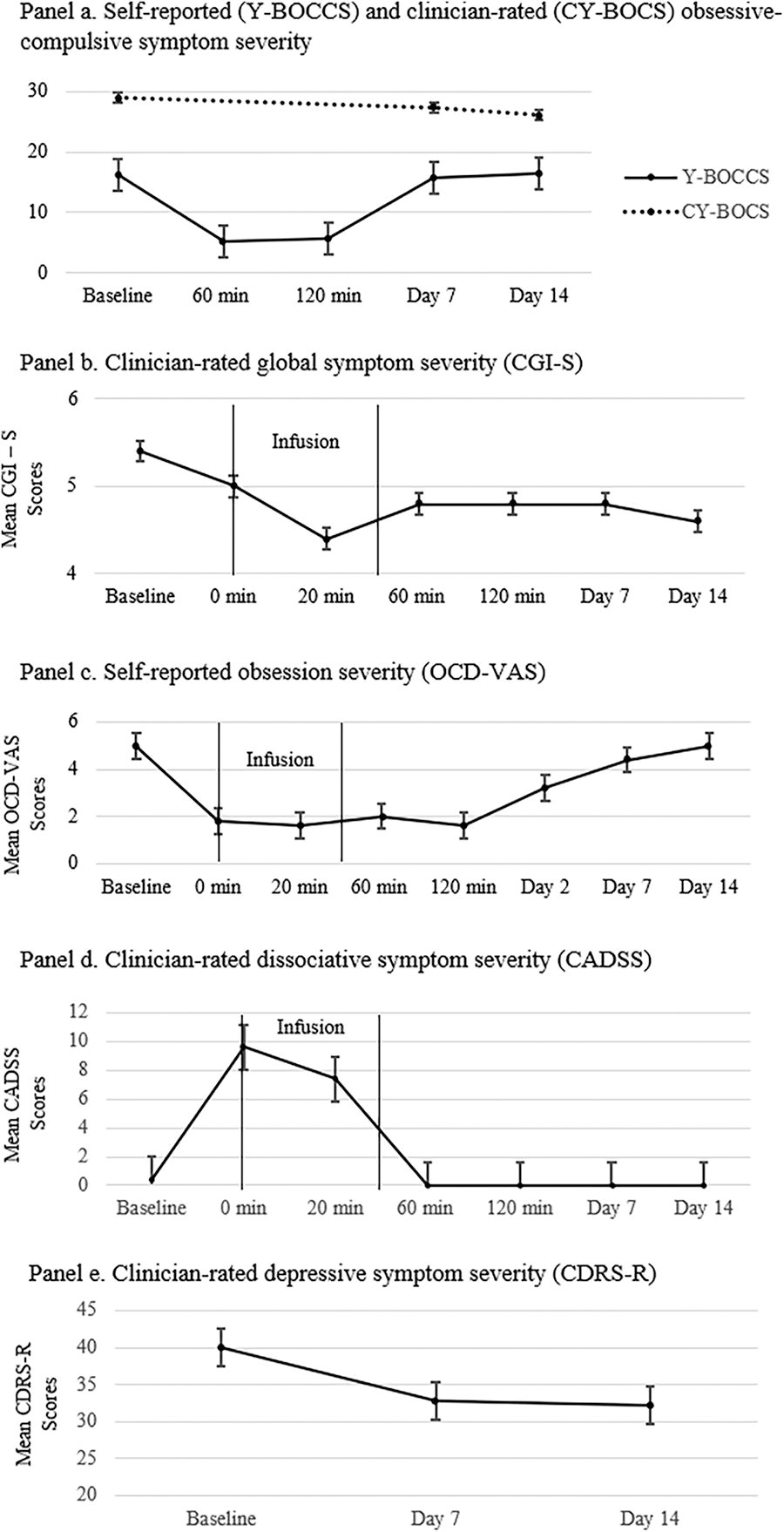
Symptom severity following intravenous ketamine infusion. Note. Y-BOCCS = Yale-Brown Obsessive Compulsive Challenge Scale; Y-BOCCS scores range from 0–40. CY-BOCS = Children’s Yale-Brown Obsessive-Compulsive Scale; CY-BOCS scores range from 0–40. CGI-S = Clinical Global Impression-Severity Scale; CGI-S scores range from 1–7. OCD-VAS = Obsessive-Compulsive Disorder-Visual Analogue Scale; OCD-VAS scores range from 0–10. CADSS = Clinician-Administered Dissociative States Scale; scores range from 0–92. CDRS-R = Children’s Depression Rating Scale-Revised; CDRS-R scores range from 17–113.
Demographics of the Sample (N = 5)
Note. ERP, exposure and response prevention therapy; SSRI, selective serotonin reuptake inhibitors; CY-BOCS, Children’s Yale-Brown Obsessive-Compulsive Scale; CY-BOCS scores ranges from 0–40; CDRS-R, Children’s Depression Rating Scale-Revised; CDRS-R sores range from 17–113. CGI-S, Clinical Global Impression—Severity Scale; CGI-S ranges from 1–7. Y-BOCCS, Yale-Brown Obsessive Compulsive Challenge Scale; Y-BOCCS ranges from 0–40. OCD-VAS = Obsessive-Compulsive Disorder-Visual Analogue Scale; OCD-VAS ranges from 0–10.
Missing score for one participant (n = 4).
Descriptive statistics on preliminary efficacy
We did not conduct hypothesis testing to investigate the efficacy of ketamine due to the exploratory nature of this study as well as the small and uncontrolled sample size. Descriptive data of self-reported and clinician-rated OC symptom severity is visualized in Figure 1 and suggests initial support of a potentially rapid effect of ketamine on OC symptom severity. Participants reported mild-to-moderate depressive symptoms at baseline (M = 40; SD = 9.1) and a decrease in symptoms 14 days after the infusion (M = 32.2; SD = 5.81).
Discussion
The results suggest that IV ketamine is well tolerated by adolescents with refractory OCD. In line with findings from adult samples (Rodriguez et al, 2013; Bloch et al., 2012) the adolescents’ experienced mild transient dissociative symptoms within 1 hour following the infusion, with no participant reporting dissociative symptoms beyond that time point. Descriptive data on the effect of ketamine on OC symptom severity provides preliminary support for a rapid effect as previously reported in adults (Rodriguez et al., 2013; Bloch et al., 2012). Similarly, comorbid depressive symptoms were lower 14 days after the infusion compared with baseline. Although a causal relationship between the IV ketamine infusion and depressive symptom reduction cannot be derived, the results mirror findings from a recent proof-of-concept randomized active placebo-controlled trial with depressed adolescents in which ketamine was well tolerated and had a rapid effect on depressive symptoms with gains maintained over 14 days (Dwyer et al., 2022).
A limitation of this study is the small numbers and open-label treatment of the current five cases, which does not allow causal interpretations of a treatment effect. However, it is the first to explore the safety and potential tolerability of administering IV ketamine to adolescents with refractory OCD. To investigate the safety and efficacy of ketamine for the treatment of refractory pediatric OCD, a potential next step would be to study the use of intranasal esketamine for this population.
Footnotes
Authors’ Contributions
H.S.I.: Writing—original draft and editing. P.K.Y.-L.: Writing—review and editing, project administration. P.H.G.: Writing (minor)—review and editing, supervision, project administration. H.B.S.: Conceptualization (supporting) and editing. M.A.R.: Conceptualization (lead), writing—review and editing.
Disclosures
H.S.I. and P.K.Y.-L. have no disclosures to report. P.H.G. has received royalties from Oxford Press for educational material. In the last 3 years, Dr. H.B.S. has received royalties from UpToDate, Inc and Cambridge University Press and a stipend from the American Medical Association for serving as Associate Editor of JAMA-Psychiatry. M.A.R. serves as a consultant on Data Monitoring Committees for AbbVie, Inc, Everest Clinical Research Corporation, and IQVIA, RDS, Inc. She also serves as a consultant for Carelon RX in the pharmacy and therapeutics committee and has received royalties from UpToDate, Inc, Oxford Press, and the American Psychiatric Association Publishing, Inc. (APPI).