
Abstract
Background:
Although randomized clinical trials (RCTs) have investigated several treatments for social communication difficulties and repetitive behavior in autism, none has yet shown consistent superiority over placebo. Placebo response in autism RCTs may impede the ability to detect meaningful treatment effects.
Objective:
We sought to identify individual-level predictors of placebo response in Study of Oxytocin in Autism to improve Reciprocal Social Behaviors (SOARS-B), a 24-week RCT of intranasal oxytocin for social impairment in autistic youth. In our primary analysis, we examined predictors of change in the Aberrant Behavior Checklist-modified Social Withdrawal (ABC-mSW) score at 24 weeks in SOARS-B participants taking placebo. Secondary analyses examined predictors of ABC-mSW change at 12 weeks and of Clinical Global Impressions-Improvement at 24 and 12 weeks. We also examined predictors of response among SOARS-B participants taking oxytocin.
Methods:
For each analysis, we first used lasso (least absolute shrinkage and selection operator) regression to identify potentially influential predictors from a large group that included demographic factors, rating scale data, and prescribed medications. We then estimated an unpenalized linear regression model for the outcome of interest that included only variables retained by the optimal lasso. We considered variables with statistically significant coefficients to be influential predictors.
Results:
Higher baseline ABC-mSW score was the only significant predictor of greater ABC-mSW change in the placebo group at 24 and 12 weeks.
Conclusions:
In SOARS-B, higher baseline severity on a measure of reciprocal social communication predicted greater placebo response. This is consistent with the finding that lower social communication adaptive functioning was associated with greater placebo response in recent RCTs of balovaptan for social impairment in autism. However, it contrasts with findings from a trial of citalopram for repetitive behavior in autism, in which lower baseline severity of a composite of autistic and mood symptoms predicted greater placebo response. This may indicate that different factors contribute to placebo response in different symptom domains.
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by two core features: impaired social communication and restrictive/repetitive behaviors (American Psychiatric Association, 2022). ASD is common, affecting 2.8% of U.S. children (Maenner, 2023), and associated with diminished quality of life (van Heijst and Geurts, 2015). Although numerous randomized clinical trials (RCTs) have investigated pharmacological treatments for the core features of the diagnosis, none has yet been identified that clearly and consistently separates from placebo. This could indicate a need to look further afield for promising treatments. Importantly, it also raises questions about placebo effects in ASD RCTs.
The placebo response in ASD trials has been substantial. A meta-analysis of 1315 autistic individuals randomized to placebo across 25 RCTs reported a placebo effect size of 0.34–0.56 standardized mean change (SMC) (Masi et al., 2015). Consistent with this, a subsequent, larger meta-analysis of 2360 individuals taking placebo across 86 ASD RCTs reported a reduction in core symptoms from 0.26 to 0.46 SMC, with 16%–22% rated “much improved” or “very much improved” on the Clinical Global Impressions-Improvement (CGI-I) scale by study clinicians (Siafis et al., 2020). This placebo effect size is on par with those reported in schizophrenia (0.22–0.44 SMC) and obsessive–compulsive disorder (0.22–0.41 SMC) (Huneke et al., 2024).
In RCTs of treatments for DSM diagnoses generally, the strongest predictors of an increased response to placebo include year of publication (as placebo response in most behaviorally defined conditions has progressively increased over the last several decades), an unbalanced design in which more patients are assigned to treatment than placebo, and lower symptom severity at baseline (Weimer et al., 2015).
In autism RCTs specifically, meta-analyses of trial-level data have reported that a clinician (as compared with caregiver)-administered outcome rating, a longer trial duration, a larger sample size, more study sites, well-concealed group allocation, a core symptom cutoff for inclusion, and study location in Iran (as compared with the United States), all may predict an increased response to placebo across patients in a study (Masi et al., 2015; Siafis et al., 2020).
Less is known about what factors could make a particular autistic patient more likely to respond to placebo, with only two studies to date having investigated participant-level RCT data. One, analyzing data from STAART, a 12 week trial of citalopram for repetitive behavior in autism that included 76 children and adolescents randomized to placebo across six sites, found that lower severity of disruptive behavior, core and mood symptoms, and caregiver strain all predicted an increased placebo response (King et al., 2013). Another, analyzing data from three multicenter trials of the vasopressin antagonist balovaptan for social impairment in autism (VANILLA, a 12-week trial that included 75 adults randomized to placebo across 26 sites; V1aduct, 24 weeks, 158 adults, 46 sites; and aV1ation, 24 weeks, 122 children and adolescents, 41 sites), found that poorer adaptive function at baseline, a cooccurring diagnosis of attention-deficit/hyperactivity disorder or depression, enrollment at a commercial (as compared with academic) site or at a site in Europe (as compared with a site in the United States or Canada), and enrollment in a 12 (as compared with 24) week study all predicted increased placebo response (Tobe et al., 2023).
Some predictors of increased placebo response, such as study site, trial duration, or baseline symptom severity, have consistency across trial-level and/or participant-level analyses. Other predictors, such as cooccurring conditions or adaptive behavior, are less consistent. We sought to investigate individual-level predictors of placebo response in the large multisite Autism Centers of Excellence network Study of Oxytocin in Autism to improve Reciprocal Social Behaviors (SOARS-B) trial. SOARS-B was a 24-week double-blind placebo-controlled RCT of intranasal oxytocin for social impairment in autistic children and adolescents aged 3–17 years. The study did not identify a treatment-related difference in social functioning between oxytocin and placebo groups (Sikich et al., 2021). Conceptually, this may allow for analysis of response predictors in the oxytocin group as a potential replication sample.
We hypothesized that we would be able to identify influential predictors of placebo response and that those predictors would be more consistent with those identified in the studies of balovaptan for social impairment than those identified in the study of citalopram for repetitive behavior.
Methods
Study sample
SOARS-B (NCT01944046), conducted from August 2014 to November 2017 across seven academic centers in the United States, enrolled 290 autistic children and adolescents, 146 of whom were randomized to oxytocin and 144 of whom were randomized to placebo. Totally, 125 individuals in each group completed the 24 weeks of the study. Just under half of participants (n = 132, 46%) were minimally verbal. Further details of the sample and methods are given elsewhere (Sikich et al., 2021; Spanos et al., 2020). The study was approved by the institutional review boards of each participating academic center (Columbia University, Duke University, Icahn School of Medicine at Mount Sinai, Massachusetts General Hospital, Seattle Children’s Hospital, University of North Carolina-Chapel Hill, and Vanderbilt University).
Measures
Outcomes
Change in Aberrant Behavior Checklist modified Social Withdrawal
The Aberrant Behavior Checklist (ABC) is a 58-item caregiver-report rating scale that is widely used to gauge treatment effects in autism clinical trials (Aman et al., 1985; Provenzani et al., 2020). Each item asks the reporter to indicate the severity of a symptom on a scale from 0 (not at all a problem) to 3 (a severe problem). The ABC-modified Social Withdrawal (mSW) subscale comprises 13 ABC items that probe social functioning and is a modified version of a Lethargy/Social Withdrawal subscale that included an additional three items indexing lethargy. A score may range from 0 to 39, with a higher score reflecting greater social impairment (Sikich et al., 2021). Change in ABC-mSW score at 24 weeks was the primary endpoint of SOARS-B and was how we defined “response” in our study’s primary analysis. In secondary analyses, we also examined predictors of ABC-mSW change at 12 weeks.
Clinical Global Impressions-Improvement
The CGI-I is a clinician-report rating scale that asks the clinician how much an individual’s condition has changed relative to their baseline from the beginning of treatment (Busner and Targum, 2007). A score may range from 7 (“very much worse”) to 1 (“very much improved”), with a score of 4 indicating no change. CGI-I score is commensurate with other measures of social communication in autistic youth when assessing treatment outcomes (Toolan et al., 2022). We conducted secondary analyses that examined predictors of CGI-I change at both 24 and 12 weeks.
Baseline predictors
We selected the following baseline predictors a priori based on prior publications and availability in our dataset.
Demographic factors
Age, sex (assigned at birth), ethnicity (Latine vs. non-Latine), and race (White, Black, Asian, or more than one race) were assessed as predictors.
Study site
The study’s six sites (site 1: Duke, site 2: Mount Sinai School of Medicine, site 3: Massachusetts General Hospital, site 4: Vanderbilt University, site 5: Seattle Children’s Research Institute, and site 6: Cornell) were assessed as predictors.
Baseline ABC-mSW
We assessed ABC-mSW score at baseline as a predictor.
Clinical Global Impressions-Severity
The CGI-Severity (CGI-S) is a clinician-report rating scale that asks the clinician to assess the severity of an individual’s illness relative to other individuals they have seen with the same diagnosis (Busner and Targum, 2007). A score may range from 1 (“normal, not at all ill”) to 7 (“among the most extremely ill patients”), with a score of 4 indicating that the individual is “moderately ill.”
Social Responsiveness Scale, Second Edition
The Social Responsiveness Scale, Second Edition (SRS-2) is a 65-item parent-report rating scale that assesses autistic traits (Constantino, 2012). Each item describes a behavior or characteristic and asks the reporter to rate it on a scale from 1 (“not true”) to 4 (“almost always true”). A raw score may range from 65 to 260, with a higher score reflecting greater impairment.
Stanford-Binet Intelligence Scales, Fifth Edition, Abbreviated IQ
This abbreviated measure of IQ is a combined measure of nonverbal fluid reasoning and verbal knowledge and reflects an individual’s general level of cognition (Roid, 2003). Stanford-Binet Intelligence Scales, Fifth Edition, Abbreviated IQ (SB5 Abbreviated IQ) has been shown to have utility as an approximation of full-scale IQ in autistic youth (Twomey et al., 2018). Note that a substantial minority of participants (n = 46, 16%) did not have SB5 Abbreviated IQ data available because of age or lack of ability. We accounted for this using mean imputation and, in sensitivity analyses, by excluding SB5 Abbreviated IQ as a predictor. Notably, of the 244 participants with IQ data, a substantial minority (n = 85, 35%) had an IQ <70.
Body mass index z-score
Body mass index (BMI) assesses an individual’s weight in relation to their height. Since raw BMIs are difficult to interpret in youth, we converted them to z scores based on Centers for Disease Control (CDC) growth charts (Kuczmarski et al., 2002).
Prescribed medications
The presence of an active prescription for one or more medications from each of several categories—alpha agonist, anxiolytic, antidepressant, anticonvulsant, antipsychotic, stimulant, sleep aid, and gastrointestinal medication—was assessed as a predictor.
Analyses
As an initial step, we compared outcomes, baseline ABC-mSW, and baseline predictors across oxytocin and placebo groups. We also computed placebo and treatment response rates, with “response” defined as a CGI-I score of at least “much improved.” We then conducted primary, secondary, and replication analyses.
In our primary analysis, we attempted to identify the strongest predictors of ABC-mSW change at 24 weeks among SOARS-B participants who received placebo.
In secondary analyses, we attempted to identify the strongest predictors of ABC-mSW change at 12 weeks, as well as the strongest predictors of CGI-I score at 12 and 24 weeks among SOARS-B participants who received placebo.
In oxytocin group analyses, we attempted to identify the strongest predictors of both ABC-mSW change and CGI-I score at 24 and 12 weeks among SOARS-B participants who received oxytocin.
We also conducted two sets of sensitivity analyses. First, we repeated all analyses with SB5 Abbreviated IQ excluded as a predictor. This allowed us to include all 290 study participants, rather than only the 244 with SB5 Abbreviated IQ data.
Second, we repeated all analyses using a wider range of baseline predictors that added the other subscales of the ABC (Irritability, Stereotypy, Speech, and Hyperactivity), the Socialization and Communication subscales of the Vineland Adaptive Behavior Scales, 2nd Edition, and the Objective, Subjective Internal and Subjective External subscales of the Caregiver Strain Questionnaire.
Statistical approach
We conducted each analysis in two steps. In the first step, feature selection, we used lasso (least absolute shrinkage and selection operator) regression to identify which predictors described above were potentially most influential in determining the outcome of interest. Lasso is a type of linear regression that adds a penalty term to the model. The penalty term causes coefficients that are less “important” (i.e., those that contribute little or nothing to the model’s predictive power) to shrink to zero. The regularization parameter, λ, determines the strength of the applied penalty (Tibshirani, 1996).
To find an optimal model (i.e., a model with an optimal value of λ), we used a grid search approach. We randomly split the dataset into training and test sets (with 70% of individuals in the training set). We then estimated 391 lasso models on the training set, one for each λ value in the range of 0.1–4.0, incrementing each time by 0.01. We evaluated the performance of each model on the test set. The optimal model was that which produced the lowest root mean square error.
In the second step, validation, we estimated an unpenalized linear regression model for the outcome of interest that included only the features (i.e., baseline predictors) retained by the lasso model (i.e., those with nonzero coefficients) as predictors. We considered any predictors in the unpenalized model with statistically significant regression coefficients to be influential predictors of the outcome.
We considered only variables identified in both the lasso analyses and with statistically significant coefficients in the linear regression model (defined as p < 0.05) to be influential predictors of the outcome.
Software and data
We conducted all analyses in R 4.3.3. Analytic scripts are available at https://github.com/amandeepjutla/2024-soars-placebo and a container environment to run them is at https://quay.io/repository/ajutla/2024-soars-placebo. Data are available in National Institute of Mental Health (NIMH) Data Archive (NDA) SOARS-B collection (#2009) at https://nda.nih.gov/edit_collection.html?id=2009.
Results
Treatment group comparisons
We found no statistically significant differences across placebo and oxytocin groups in terms of baseline characteristics, including age, sex, ethnicity, race, study site, baseline ABC-mSW, CGI-S score, SRS-2 raw score, SB5 Abbreviated IQ, BMI z-score, or medications, or did we identify differences in outcomes, including ABC-mSW and CGI-I at 24 and 12 weeks. Among participants who received placebo, 23.4% were at least “much improved” by CGI-I score at 24 weeks, and 18.4% at 12 weeks. Among those who received oxytocin, response rates were statistically indistinguishable at 26% and 16%, respectively (Table 1).
Comparison of Placebo and Oxytocin Groups
M Standard deviation (SD), Wilcoxon rank sum test.
n (%), Pearson’s chi-squared test.
n (%), Fisher’s exact test.
CGI-I score of at least 2 (“very much improved”) or 1 (“much improved”).
Based on n = 244 (n = 122 placebo, n = 122 oxytocin) with SB5 Abbreviated IQ data.
ABC-mSW, Aberrant Behavior Checklist-modified Social Withdrawal; BMI, body mass index; CGI-I, Clinical Global Impressions-Improvement; CGI-S, Clinical Global Impressions-Severity; IQ, intelligence quotient;SRS-2, Social Responsiveness Scale, 2nd Edition; SB5, Stanford-Binet, 5th Edition.
Primary analysis
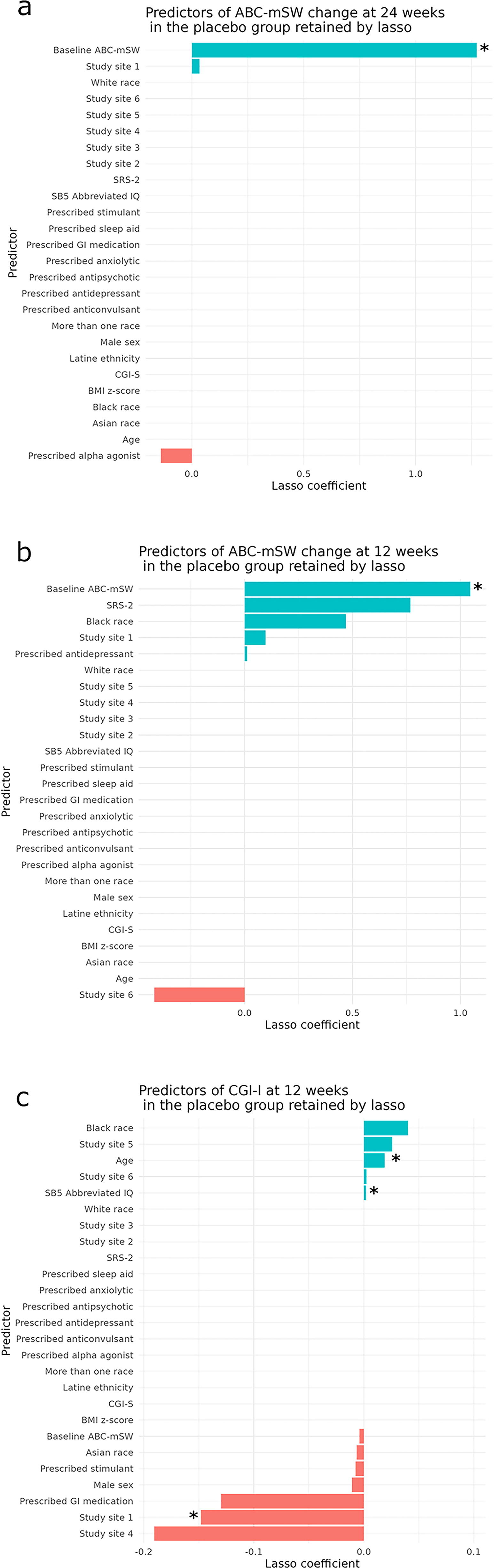
The optimal lasso model retained three predictors of ABC-mSW change at 24 weeks in the placebo group: baseline ABC-mSW and study site 1 (both positive predictors) and prescribed alpha adrenergic agonist as a negative predictor (Fig. 1a). Of these, only baseline ABC-mSW was statistically significant in the validation step (Table 2; Fig. 2a), such that, for every one-point increase in baseline ABC-mSW, the decrease in ABC-mSW change at week 24 was 0.31 points greater.
Predictors of ABC-mSW change at 24

Unpenalized linear regression of baseline ABC-mSW vs. change at 24
Validation of Predictors in the Placebo Group
Multiple R 2: 0.17; adjusted R 2: 0.15.
Multiple R 2: 0.24; adjusted R 2: 0.20.
Multiple R 2: 0.28; adjusted R 2: 0.17.
ABC-mSW, Aberrant Behavior Checklist-modified Social Withdrawal; CGI-I, Clinical Global Impressions-Improvement; CI, confidence interval; GI, gastrointestinal; IQ, intelligence quotient; SB5, Stanford-Binet, 5th Edition; SE, standard error.
Secondary analyses
The optimal lasso model retained six predictors of ABC-mSW change at 12 weeks in the placebo group: baseline ABC-mSW, SRS-2, Black race, study site 1, and prescribed antidepressant (all positive predictors), and study site 6 as a negative predictor (Fig. 1b). As at 24 weeks, only baseline ABC-mSW was statistically significant in validation (Table 2; Fig. 2b); for every one-point increase in baseline ABC-mSW, the decrease in ABC-mSW at week 12 was 0.25 points greater.
In analyses with CGI-I as the outcome in the placebo group, the optimal lasso model did not retain any predictors at 24 weeks. At 12 weeks, the optimal lasso model retained several predictors (Fig. 1c), with age and SB5 Abbreviated IQ (positive) and study site 1 (negative) statistically significant in validation (Table 2).
Oxytocin group analyses
In analysis of ABC-mSW in the oxytocin group at 24 weeks, baseline ABC-mSW (a positive predictor) and baseline SRS-2 raw score (a negative predictor) were statistically significant in validation (Supplementary Fig. S1a; Supplementary Table S1). At 12 weeks, baseline ABC-mSW and SRS-2 were again statistically significant, as was participation at study site 2 (negative) (Supplementary Fig. S1b; Supplementary Table S1).
In analyses with CGI-I as the outcome in the oxytocin group, male sex (positive) and participation at study site 5 (negative) were statistically significant at 24 weeks (Supplementary Fig. S1c; Supplementary Table S1), and stimulant prescription was significant at 12 weeks (Supplementary Fig. S1d; Supplementary Table S1).
Sensitivity analyses
When we repeated all analyses with SB5 Abbreviated IQ removed as a predictor, our findings remained consistent across analyses, including for CGI-I at 12 weeks in the placebo group, where age and site effects remained significant predictors.
Results were also largely consistent when we included a broader range of predictors. In analyses of the placebo group with change in ABC-mSW as the outcome, baseline ABC-mSW (positive) was again the only statistically significant predictor at 24 and 12 weeks. When CGI-I was the outcome, baseline Caregiver Strain Questionnaire (CSQ )Subjective External score (positive) emerged as a statistically significant predictor at 24 and 12 weeks.
In analyses of the oxytocin group with change in ABC-mSW as the outcome, baseline ABC-mSW (positive) was the only significant predictor at 24 weeks, and at 12 weeks only ABC-mSW (positive) and SRS-2 (negative) were significant.
Discussion
We sought to identify the strongest predictors of placebo response in data from SOARS-B, a large, multisite RCT for social impairment in autism that showed no advantage for oxytocin over placebo. Our results are somewhat surprising in that, in contrast with other analyses of placebo response in autism clinical trials, we did not find many such predictors.
In our primary analysis, which examined predictors of change in ABC-mSW score at 24 weeks—the same endpoint used in SOARS-B—we found that, of 26 predictors, only baseline ABC-mSW score, a positive predictor, was influential. This was also the only influential predictor at 12 weeks. Secondary analyses that used CGI-I as the endpoint also did not find many influential predictors of placebo response. At 24 weeks, no predictors were selected by our lasso model. At 12 weeks, we found that age, Abbreviated IQ, and participation at site 1 were significant.
Our finding that greater baseline severity predicted increased placebo response is inconsistent with King et al.’s (2013) finding that lower severity of a composite of autism and mood symptoms predicted greater placebo response. However, it is consistent with Tobe et al.’s (2023) analyses, which found that more functional challenges in social communicative functioning (lower Vineland-II 2DC scores) were associated with a greater placebo response (increases social communicative functioning—higher 2DC scores) with placebo treatment. The similarities in factors predicting placebo response between our study and those analyzed by Tobe and colleagues may reflect challenges measuring changes in reciprocal social interactions in autistic people, challenges related to using outcome measures that do not have a clear threshold for significant improvement, and symptom heterogeneity inherent in autism.
Interestingly, even though placebo and oxytocin groups did not differ in any systematic way in terms of either baseline characteristics or response rate, we identified some predictors in the oxytocin group but not the placebo group. In particular, for CGI-I ratings, male sex and stimulant prescription were significant predictors of change at 24 and 12 weeks, respectively. This is potentially consistent with the animal literature, which suggests oxytocin could have sex-dependent effects (Dumais and Veenema, 2016). It could also be consistent with known interactions between oxytocin and dopamine in the context of social motivation (Love, 2014). The most likely explanation, however, is that the different predictors we found across placebo and oxytocin groups represent random variability. Still, it may be worth considering whether predictors of response in placebo versus active treatment groups in clinical trial data could identify subgroups that may have a clinically meaningful response in a trial that did not have an overall significant finding. This approach would need to be evaluated in other conditions in which a subgroup has actually been identified as having a clinically meaningful response, as has been true in molecularly defined subgroups in cancer, for example (Sachdev et al., 2023). With regard to our findings here, a subsequent study would need to evaluate response specifically in males versus females or in individuals taking stimulant medications.
Our finding that baseline severity on our primary outcome measure (ABC-mSW) predicted improvement on that measure was robust in that we identified it in both placebo and oxytocin groups. The finding is consistent with other data showing a relationship between greater initial severity and response to treatment across several DSM diagnoses, including schizophrenia (Hieronymus et al., 2023), depression (Kraus et al., 2019), and anxiety (de Vries et al., 2016). The relationship has previously been described in ASD as well, though not universally (Grzadzinski et al., 2023). This observation may correspond, in some cases, to regression to the mean, with initial high-severity scores decreasing by virtue of expected fluctuation, at least for symptoms that show some variability across time. Regression to the mean may be a particular concern in studies that, unlike SOARS-B, used baseline scores on the primary outcome measure to characterize the level of severity required for inclusion in the study.
Although we identified some negative predictors of response, these were inconsistent both within and across groups. For example, in the placebo, but not the oxytocin, group, site 1 was a negative predictor of CGI-I score at 12 but not 24 weeks, and in the oxytocin, but not the placebo, group, site 5 was a negative predictor of CGI-I score at 24 but not 12 weeks. These inconsistencies suggest that the negative site effects we identified are most likely to represent random variability.
Our study had some limitations. Some of the predictors assessed in the King et al (2013) and Tobe et al (2023) analyses could not be tested in our dataset. In particular, we could not test the replicability of the finding that enrollment at a commercial (as opposed to academic) site predicted increased placebo response because all sites in our study were academic. It is possible that this lack of commercial sites may partially explain the relatively low placebo response rate in SOARS-B, which may also have limited our ability to identify predictors. Additionally, a trial of intranasal oxytocin may also have particular complexities for evaluating placebo response because the oxytocin system may itself play a role in mediating the placebo response (Itskovich et al., 2022). In fact, a previous RCT of oxytocin in autism found that among placebo responders, but not oxytocin responders, clinical improvement was associated with a pronounced posttreatment increase in blood oxytocin levels (Parker et al., 2017). Other mechanistic factors likely include, as noted, regression to the mean, particularly in studies where the same measure used to determine inclusion is used as an outcome measure, the effect of ongoing development on scales that are sensitive to developmental improvements, or the expectancy effect among participants and their families.
Our study represents only the third analysis of individual-level predictors of placebo response in autism clinical trial data. To date, the findings of these three analyses have been discrepant, and this heterogeneity makes it somewhat difficult to draw conclusions about predictors of the placebo response in autism. We hope that our work inspires additional analyses that could allow for such conclusions to be drawn. Developing an understanding of the nature of the placebo response in autistic individuals could be key to overcoming the difficulties investigators have experienced to date in identifying successful treatments for core symptoms.
Conclusions
Our results, taken in context with prior data, indicate that baseline severity on the outcome measure of interest is a meaningful predictor of placebo response in autism in studies focused on improving core social communication challenges. As one concrete implication, this finding suggests that ASD trials should avoid using the primary outcome measure as an entry criterion. Requiring higher baseline severity could increase the likelihood of regression to the mean contributing to apparent placebo response. The relatively lower placebo response and low number of significant predictors of placebo response across our academic sites also align with prior data suggesting that less-experienced sites, including commercial sites, may be more prone to placebo response (Tobe et al., 2023). More data regarding predictors of placebo response are still needed to improve clinical trial design in autism. Investigators conducting autism trials should, if adequately powered, routinely analyze individual-level predictors of placebo response. Eventually, meta-analysis of individual-level response data from multiple trials could reveal factors important for designing future studies.
Clinical Significance
Clinicians should be mindful that placebo effects are likely to contribute to observed improvements. Our data suggest that these effects may be both durable and related to more severe participant or caregiver ratings of impairment.
Footnotes
Acknowledgments
The authors would like to thank all SOARS-B participants and their families.
Authors’ Contributions
A.J. and J.V.-V.W. conceptualized the study. A.J. developed the methodology and conducted data analyses. A.V., S.B., and A.J. drafted the article. All other authors contributed to the SOARS-B data collection and provided critical revisions to the article.
Disclosures
A.J., A.V., S.B., and C.R. have nothing to disclose. J.V.-V.W. has consulted or served on advisory boards for Novartis, Roche Pharmaceuticals, and SynapDx; has received research funding from Novartis, Roche Pharmaceuticals, Forest, Seaside Therapeutics, Janssen, SynapDx, Yamo Pharmaceuticals, MapLight, and Acadia; and has received an editorial stipend from Springer and Wiley. S.-J.K. was involved in clinical trials by Wilson Therapeutics, Clinical Research Associates (CRA), Janssen & Janssen, Roche, Pfizer, Neuren Pharmaceuticals; and has received an editorial stipend from Springer. L.S. has consulted for Roche Pharmaceuticals and Impel Pharmaceuticals and has served as a site PI for Roche. C.J.M.D. has consulted for Acadia Pharmaceuticals and receives royalties from Oxford University Press and Springer. M.P. has received research funding from Takeda Pharmaceuticals. S.M. has done previous contract work for Roche/Genentech. K.B.S. is currently employed by Otsuka-US in Princeton, NJ, and was previously employed by Roche/Genentech.
Supplementary Material
Supplementary Table S1
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.