
Abstract
Objective:
Weight loss is a well-documented adverse effect of psychostimulants. Given their frequent coprescription with second-generation antipsychotics (SGA) in pediatric patients, this study aims to examine whether concomitant use of psychostimulants mitigates SGA-associated weight gain in children and adolescents.
Method:
This study utilized the IQVIA Ambulatory electronic medical record-U.S. database (2016–2021) to identify patients aged 6–17 years who initiated an SGA. Those who started psychostimulants within 7 days of SGA initiation and maintained ≥90 days of use were classified as concomitant users, while those who initiated psychostimulants later with ≥90 days of overlap were add-on users. Patients never prescribed psychostimulants were SGA-only users. After adjusting for the baseline covariates using propensity scores, 6- and 12-month body mass index (BMI) z-score trends following psychostimulant initiation were compared between (1) concomitant and SGA-only users and (2) add-on and SGA-only users, using a linear mixed-effects regression model.
Results:
The results of linear mixed effect regression models indicate that concomitant users experienced a 0.0143 less monthly BMI z-score increase (p = 0.0063) compared with the SGA-only users over the 6 months following psychostimulant initiation. Similarly, add-on users had a significantly lower rate of weight gain compared with SGA-only users (β = −0.0463, p < 0.0001). When the follow-up period was extended to 12 months, the sensitivity analyses for both concomitant and add-on users were consistent with their primary analyses.
Conclusions:
Concomitant and add-on psychostimulants appear to mitigate SGA-associated weight gain in children and adolescents. Further investigation is needed to understand their effectiveness and safety relative to other interventions for antipsychotic-associated weight gain.
Introduction
Antipsychotic-associated weight gain (AAWG) is one of the most bothersome side effects, affecting up to 60% of children treated with second-generation antipsychotic (SGA) (Patel et al., 2017). While the exact causes of AAWG are still under investigation, increased appetite and reduced fat breakdown are believed to play significant roles (Correll et al., 2011). This weight gain increases the risk of developing type 2 diabetes, high blood pressure, dyslipidemia, and cardiovascular disease (Galling et al., 2016; De Hert et al., 2011; McIntyre and Jerrell, 2008). Management strategies include lifestyle modifications, such as dietary changes and exercise, as well as pharmacological intervention, including metformin, H2 antagonists, and monoamine modulators (Agarwal et al., 2022).
As much as 20% or more of children prescribed psychiatric medication may receive one or more psychiatric drugs concurrently (Medhekar et al., 2019). Among those prescribed SGAs, psychostimulants ([Dextro/Lisdex] amphetamine and [Dex] methylphenidate), primarily used for attention-deficit/hyperactivity disorder (ADHD), are the most frequently coprescribed psychiatric medications in the pediatric population. Kreider et al. reported that 22% of children receiving SGAs also used psychostimulants concomitantly (Kreider et al., 2014). Our own analysis of electronic medical records (EMR) data found that approximately 31% of patients prescribed SGAs were also prescribed psychostimulants (Chen et al., 2023b).
Weight loss is a well-recognized adverse effect of psychostimulants, primarily attributed to their role in appetite suppression and increased calorie expenditure (Efron et al., 1997; Fast et al., 2021; Schwartz et al., 2014; Storebø et al., 2016). A longitudinal study of children aged 3–18 years found that those taking psychostimulants had a body mass index (BMI) that was 0.7616 kg/m2 lower than those not treated with psychostimulants (Schwartz et al., 2014). Additionally, Fast et al. reported that half of overweight or obese children aged 6–17 years experienced significant weight loss within 1 year of psychostimulant treatment (Fast et al., 2021).
It is known that prescribers often take advantage of medication side effects to achieve other clinical goals, such as a prescriber selecting an antidepressant that induces sleepiness for a depressed patient who also has sleep difficulty. Given that psychostimulants are often coprescribed with SGAs in children, it is worthwhile investigating whether the risk of SGA-associated weight gain is reduced in patients also prescribed psychostimulants. If psychostimulants are found to help mitigate SGA-associated weight gain, this potential benefit should be added to the clinical discussion of strategies for managing SGA-associated weight gain.
The research question has been examined in three published studies. Calarge et al. (2009) examined the impact of risperidone on metabolic factors in a cohort of 99 children who were taking risperidone for an average of 3 years. They found that psychostimulant coprescription was more common in children with a normal BMI (77%) compared with those who were overweight or obese (50%) (Calarge et al., 2009). Similarly, another observational cohort study by van der Esch et al. (2021) found that using concomitant psychostimulants alongside SGAs was associated with a lower BMI z-score at 15 weeks and beyond 52 weeks of follow-up in 144 young patients (van der Esch et al., 2021). In contrast, in a post hoc analysis of the data from a 6-week trial in children with conduct disorder-related diagnoses including ADHD, Aman et al. (2004) found that participants with ADHD who were prescribed both a psychostimulant (at the baseline) and risperidone had similar weight gain compared with those receiving risperidone without a psychostimulant (Aman et al., 2004).
While these studies provided valuable insight, they have notable limitations. The studies by Aman et al. and Calarge et al. were not specifically designed to assess the effect of psychostimulants on SGA-associated weight gain, and their findings are based on post hoc analyses. Additionally, both studies focused exclusively on risperidone users, limiting their application to other SGAs. Although the study by Vand der Esch et al. was well-designed, it did not account for the potential influence of comedications on weight changes. Furthermore, all three studies have relatively small sample sizes, which may limit the generalizability of their findings.
Thus, it remains unclear to what extent the risk of SGA-associated weight gain may be mitigated in children and adolescents who are also prescribed psychostimulants. No study has yet directly examined whether psychostimulant use in children and adolescents prescribed SGAs mitigates SGA-associated weight gain using large real-world data.
Therefore, this study aimed to assess whether concomitant psychostimulant use is associated with a lower risk of AAWG for children and adolescents. By leveraging a national EMR database including more than 30,000 children prescribed long-term SGA and comprehensively controlled confounding factors, including comedications, this study addresses the limits of previous research and provides a more robust analysis of the research question.
Methods
Data source
IQVIA Ambulatory electronic medical record (EMR)-U.S. database is a collection of patient EMRs captured from interactions between a patient and their health care provider. Patient EMRs include a patient’s demographics, problems, vitals, labs, diagnosis, procedures, and prescriptions. The dataset is sourced from over 800 ambulatory practices that cover more than 100,000 physicians. It includes over 82 million patients, with an average history of 3 years, and some dating back to 2006. The database is used in a variety of life sciences and commercial effectiveness studies.
Study sample: Children prescribed SGAs only, concomitantly prescribed SGA and psychostimulant (concomitant users), and prescribed psychostimulant after SGA initiation (add-on users)
Using IQVIA Ambulatory EMR data from 2016 to 2021, we identified a cohort of SGA-naive and psychostimulant-naive children and adolescents (aged 6–17 years) who initiated an SGA regimen and continued it for at least 90 days. To ensure naive status, patients were excluded if they had any SGA prescriptions in the 12 months prior to the index SGA prescription. For those prescribed a psychostimulant, a 12-month washout period was also required before initiation, with the psychostimulant start date designated as the index date. Within this cohort, three mutually exclusive exposure groups were defined: (1) concomitant users—those who initiated psychostimulant therapy within 7 days of SGA initiation and maintained continuous psychostimulant and SGA use for ≥90 days; (2) add-on users—those who initiated a psychostimulant more than 7 days after starting an SGA, with at least 90 days of overlapping use; and (3) SGA-only users: who did not receive a psychostimulant during the study period.
Study design
The effect of psychostimulants on AAWG was evaluated separately in concomitant users and add-on users, each compared with SGA-only users. For the comparison between concomitant users and SGA-only users, the index date for both groups was set at the initiation of SGA treatment. For the comparison between add-on users and SGA-only users, prescription time-distribution matching was applied to minimize immortal time bias, ensuring that SGA-only users were not compared with add-on users whose duration of SGA treatment before stimulant initiation exceeded the total SGA treatment duration of the SGA-only users (Zhou et al., 2005). Immortal time bias occurs in observational studies when a period during which an outcome (such as weight change) cannot occur is misclassified, leading to an overestimation of treatment effects. In this study, if the add-on users were allowed to accumulate time on SGA before starting the psychostimulant, their weight trajectory could differ simply because they had a longer exposure to SGA rather than due to the psychostimulant itself. By matching exposure time, we ensure a fair comparison between groups.
Specifically, each add-on user was matched to an SGA-only user, and the psychostimulant initiation date of the add-on user was assigned as the index date for their matched SGA-only counterpart. In both comparisons, all patients were required to have at least one BMI measurement both before and within 6 months after the index date.
Follow-up period
All individuals were followed until the earliest of: 6 months after the index date, discontinuation of SGA, or discontinuation of the psychostimulant.
Study outcome
All available BMI z-score measures during the follow-up period were included in the analysis. We examined the slope of the BMI z-score trajectory after the index date, comparing these changes between those prescribed SGAs only and those prescribed both SGAs and psychostimulants. BMI z-score was calculated using weight and height, standardized by age- and sex-reference values based on CDC growth charts criteria (0 to <20 years) (Kuczmarski et al., 2002). In addition, the last recorded BMI z-score was used to calculate the clinically significant weight gain during the follow-up period, which was defined as the change in BMI z-score from baseline exceeding 0.5 (Correll and Carlson, 2006).
Statistical analysis
The chi-square test for categorical variables and analysis of variance for continuous variables were employed to compare patient characteristics between those prescribed an SGA-only and those prescribed both an SGA and a psychostimulant. Individual-level and group-level changes in BMI z-score 6 months after the initiation of SGA were graphically presented using spaghetti plots and Lowess curves (Cleveland, 1981).
We compared changes in the slopes of BMI z-score after the SGA initiation between the SGA-only group and the SGA and psychostimulant group, using the linear mixed-effects regression approach (Naumova et al., 2001), which incorporated missing and irregular data in the longitudinal study. Given that our group assignment was not randomized, the intergroup differences were adjusted by a propensity score (PS). In our analysis, we used inverse probability of treatment weighting to calculate the PS for both the study and comparison groups. This PS estimated the likelihood of receiving psychostimulant treatment among all pediatric SGA recipients using predictors derived from two distinct timeframes: the 6-month baseline before and at the index date. Study predictors collected during the baseline period encompassed patient demographic variables, such as age, sex, and race, along with geographic region, baseline BMI z-score, baseline weight status, family history of mental disorders, patient diagnoses, and concomitant medications. Predictors identified on the index date included the individual index SGA and the specialty of the SGA prescriber.
Sensitivity analysis
Prior studies have consistently shown that the rapid weight gain associated with SGAs typically occurs within the initial 6 months of treatment, after which the rate of increase tends to stabilize (Lyu et al., 2024a, 2024b). To account for potential longer-term effects, we conducted a 12-month follow-up as a sensitivity analysis for both concomitant users and add-on users, providing additional insight into weight trajectory beyond the primary analysis.
All statistical tests were conducted at a significance level of 0.05. All analyses were performed using SAS (version 9.4, SAS Institute Inc., Cary, NC).
Ethics statement
The study has been approved by the University of Houston Institutional Review Board.
Results
Study sample characteristics
As shown in Figure 1, 2359 concomitant users, 531 add-on users, and 6703 individuals prescribed an SGA-only who met the inclusion criteria of the study were identified.
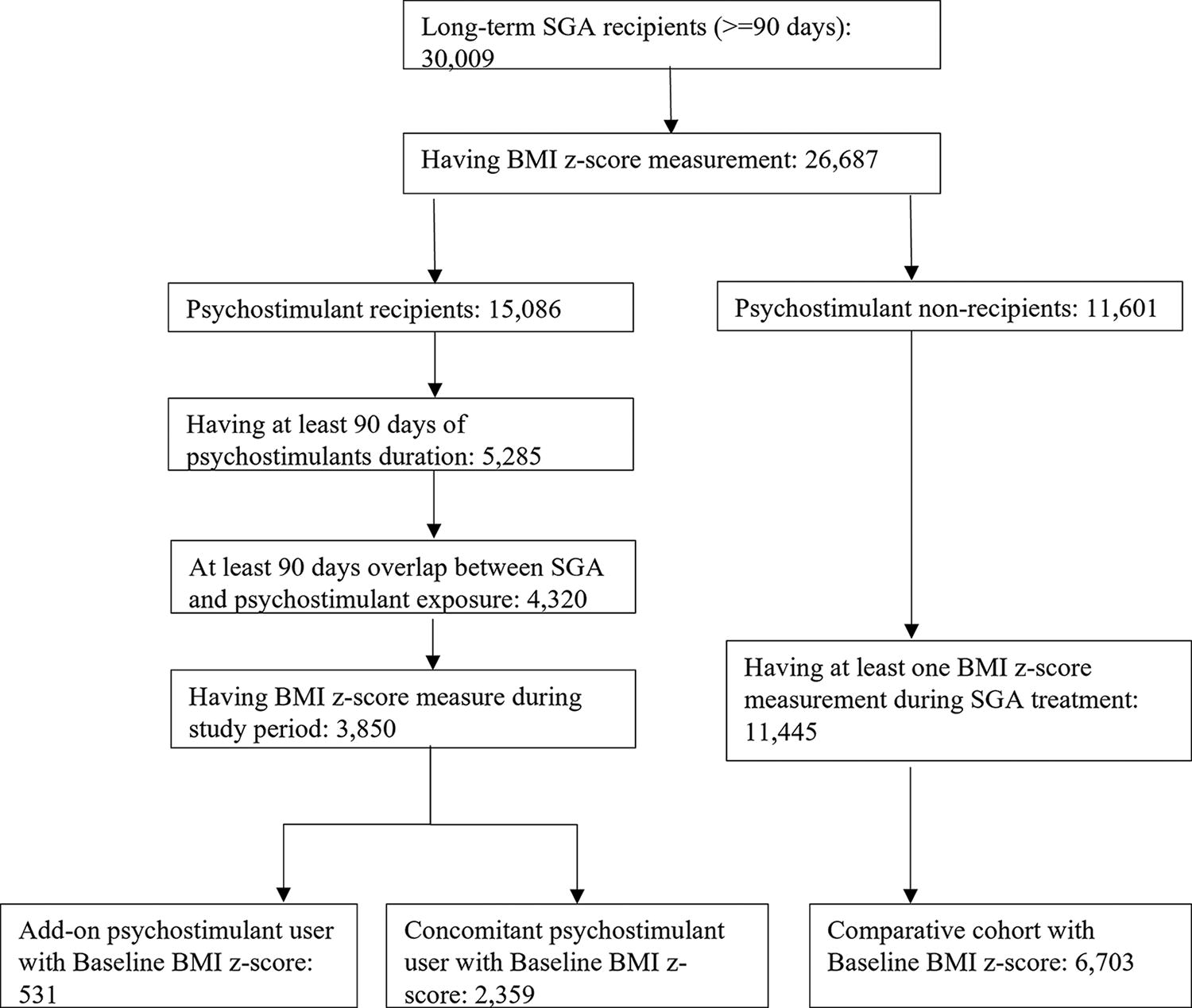
Flowchart of study cohort formation: pediatric patients prescribed both SGA and psychostimulant and prescribed SGA-only. The diagram details the inclusion and exclusion criteria, initial patient counts, and final cohort sizes for each group. Patients were identified from the IQVIA Ambulatory EMR-U.S. database and stratified based on prescription history and the availability of BMI z-scores during the study period. BMI, body mass index; EMR, electronic medical record; SGA, second-generation antipsychotic.
Table 1 compares the demographic, clinical, and provider characteristics between concomitant users and SGA-only users, while Table 2 presents these comparisons between add-on users and their matched SGA-only counterparts. In both comparisons, psychostimulant recipients were younger, with a higher proportion aged 5–12 years than SGA-only users (concomitant vs. SGA-only: 60.1% vs. 39.1%, p < 0.001; add-on vs. SGA-only: 65.7% vs. 42.2%, p < 0.001). A greater proportion of psychostimulant recipients were males (concomitant vs. SGA-only: 71.7% vs. 50.1%, p < 0.0001; add-on vs. SGA-only: 63.5% vs. 55.0%, p = 0.0086), had a higher prevalence of an ADHD diagnosis (concomitant vs. SGA-only: 68.0% vs. 22.2%, p < 0.0001; add-on vs. SGA-only: 53.1% vs. 13.0%, p < 0.0001), and were less likely to developed clinically significant weight gain (concomitant vs. SGA-only: 68.0% vs. 76%, p < 0.0001; add-on vs. SGA-only: 72% vs. 79%, p < 0.0001) during the 6-month follow-up period compared with SGA-only users.
Demographic, Clinical, and Practice Characteristics of Children and Adolescents Prescribed SGA Only and Prescribed SGA and Concomitant Psychostimulant

Obesity was defined as having a BMI z-score larger than 1.64, which corresponds to greater than the 95th percentile, as per the cutoff defined by the CDC. Overweight was defined as having a BMI z-score between 1.03 and 1.64, corresponding to a BMI 85th percentile but <95th percentile. Normal weight was defined as a BMI z-score under 1.03, corresponding to below the 85th percentile.
Clinically significant weight gain was defined as the change in BMI z-score from baseline exceeding 0.5.
Hyperglycemia/diabetes includes type 1 or type 2 diabetes and abnormal blood glucose.
Schizophrenia-related diagnosis includes schizophrenia, schizoaffective disorder, and psychosis.
Weight loss medication includes Bupropion-naltrexone, Liraglutide, Orlistat, and Phentermine-topiramate.
Mental health specialty includes child psychiatry, psychiatry, and psychology according to the code book of the IQVIA database.
ADHD, attention-deficit/hyperactivity disorder; BMI, body mass index; SD, standard deviation; SGA, second-generation antipsychotic.
Demographic, Clinical, and Practice Characteristics of Children and Adolescents Prescribed SGA Only and Prescribed SGA and Add-on Psychostimulant

Obesity was defined as having a BMI z-score larger than 1.64, which corresponds to greater than the 95th percentile, as per the cutoff defined by the CDC. Overweight was defined as having a BMI z-score between 1.03 and 1.64, corresponding to a BMI 85th percentile but <95th percentile. Normal weight was defined as a BMI z-score under 1.03, corresponding to below the 85th percentile.
Clinically significant weigh gain was defined as the change in BMI z-score from baseline exceeding 0.5.
Hyperglycemia/diabetes includes type 1 or type 2 diabetes and abnormal blood glucose.
Schizophrenia-related diagnosis includes schizophrenia, schizoaffective disorder, and psychosis.
Weight loss medication includes Bupropion-naltrexone, Liraglutide, Orlistat, and Phentermine-topiramate.
Mental health specialty includes child psychiatry, psychiatry, and psychology according to the code book of the IQVIA database.
ADHD, attention-deficit/hyperactivity disorder; BMI, body mass index; SD, standard deviation; SGA, second-generation antipsychotic.
The median duration of psychostimulant use was 482 days (interquartile range [IQR]: 253–859 days) in the concomitant user group and 395 days (IQR: 161–772 days) in the add-on user group. During the 6-month follow-up period, an average of two BMI z-score measures were available in the concomitant user group and three in the SGA-only group. An average of four BMI z-score measures were available in the add-on user group and two in the matched SGA-only group.
Change of BMI z-score trajectory associated with concomitant and add-on psychostimulant initiation
Figure 2 visually presents the unadjusted BMI z-score trajectories for concomitant users and SGA-only users during the 6 months following the index date, using spaghetti plots and Lowess curves. The adjusted estimated changes in BMI z-scores associated with concomitant psychostimulant use, as determined by the linear mixed model, are presented in Table 3. After adjusting for PS estimated from baseline covariates, concomitant users did not have a statistically significant change in BMI z-score over time (p = 0.0517). In contrast, SGA-only users displayed a positive weight gain trajectory, with an average monthly BMI z-score increase of 0.0232 (p < 0.0001). Compared with the SGA-only users, concomitant users experienced a 0.0143 less monthly BMI z-score increase (p = 0.0063) during the post-index period.
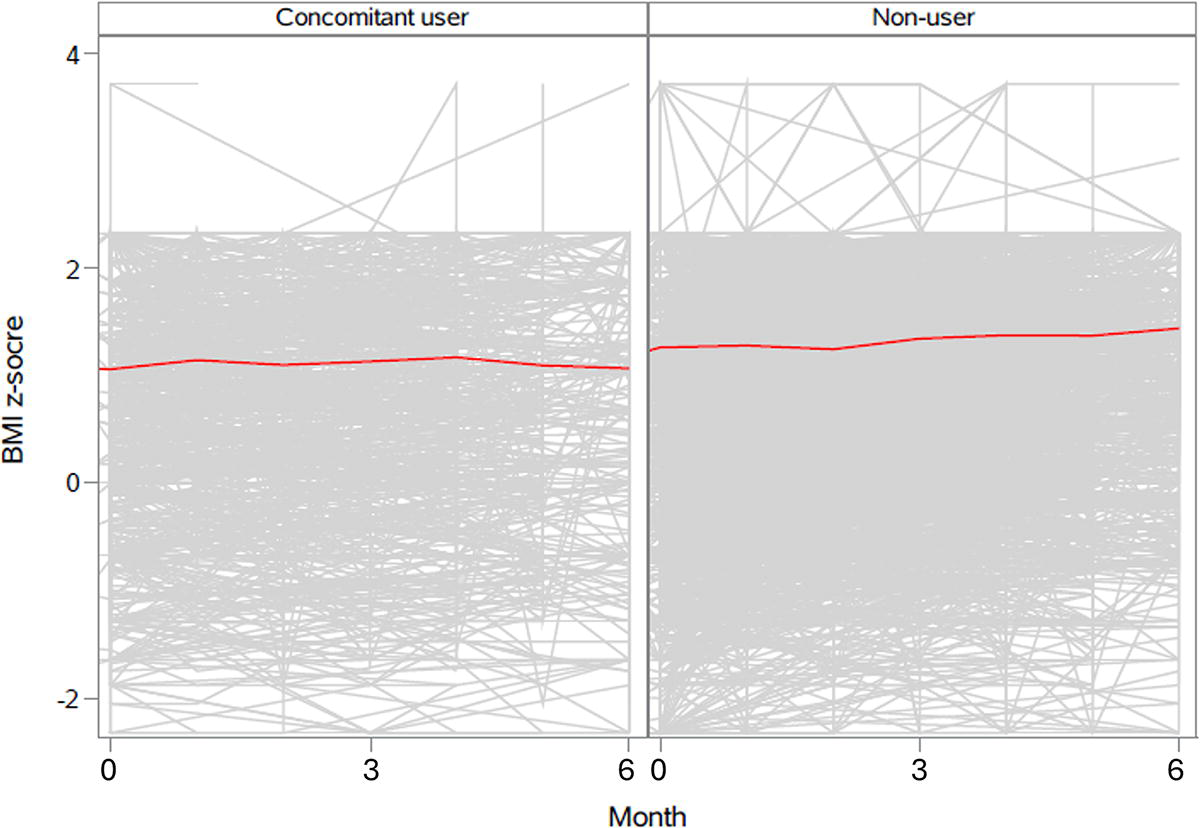
Spaghetti plots and Lowess curves of BMI z-score trajectories 6 months after the initiation of concomitant psychostimulant, pediatric patients prescribed both SGA and psychostimulant and prescribed SGA-only. This figure presents spaghetti plots and locally weighted scatterplot smoothing (Lowess) curves depicting BMI z-score trajectories over 6 months following the initiation of concomitant psychostimulant therapy. The analysis includes pediatric patients prescribed concomitant psychostimulants, as well as those prescribed SGAs only. Individual patient trajectories are shown in the spaghetti plots, while the Lowess curves illustrate overall trends in BMI z-score changes within each group. BMI, body mass index; SGA, second-generation antipsychotic.
BMI z-score Trends, 6 Months after Psychostimulant Initiation, Children and Adolescents SGA Concomitant/Add-on Psychostimulant, and Prescribed SGA Only, from Linear Mixed-Effects Model with Propensity Score Adjustment
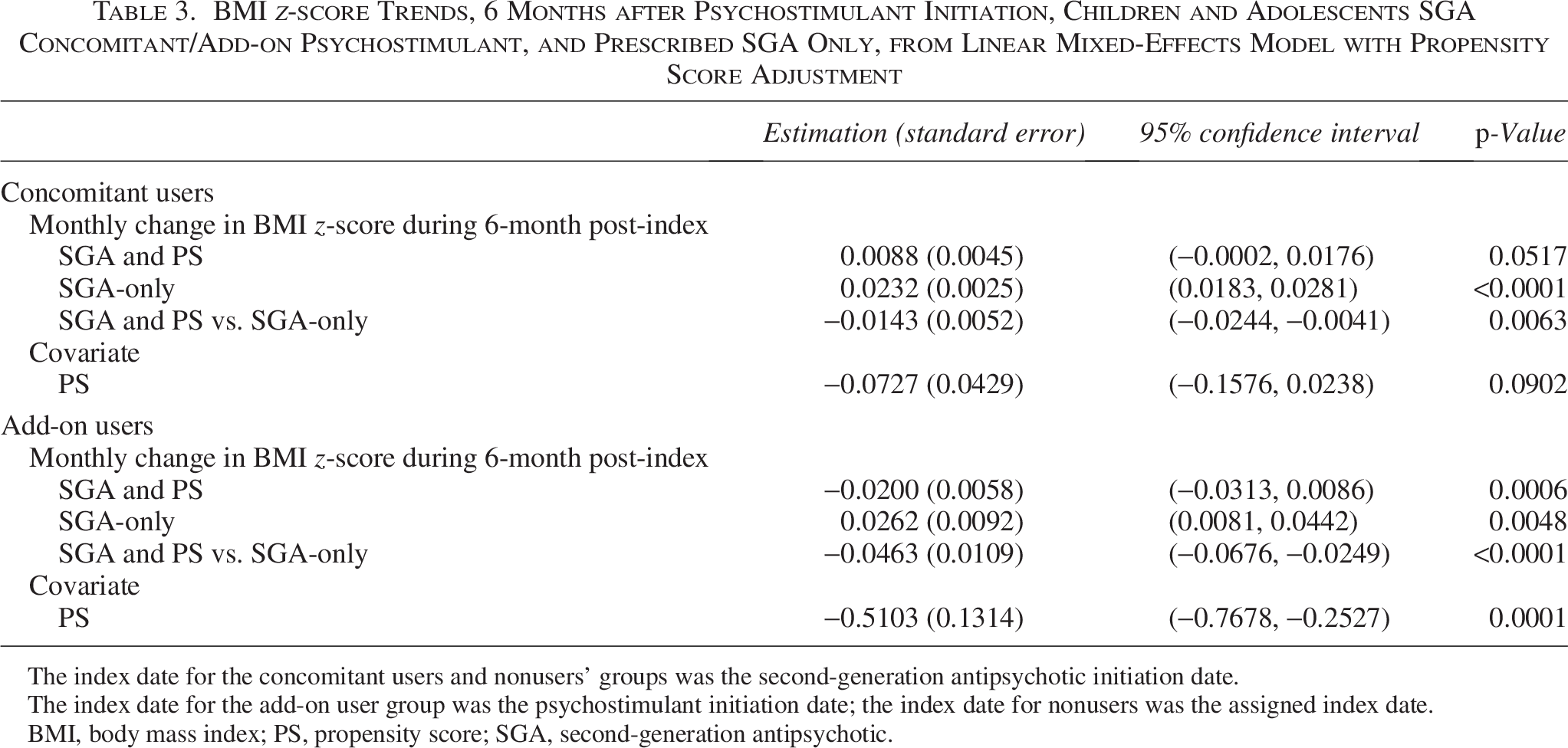
The index date for the concomitant users and nonusers’ groups was the second-generation antipsychotic initiation date.
The index date for the add-on user group was the psychostimulant initiation date; the index date for nonusers was the assigned index date.
BMI, body mass index; PS, propensity score; SGA, second-generation antipsychotic.
Similarly, Figure 3 illustrates the unadjusted BMI z-score trajectories for add-on users and SGA-only users during the 6 months following the index date, using spaghetti plots and Lowess curves. The adjusted estimated changes in BMI z-scores associated with add-on psychostimulant use, as determined by the linear mixed model, are presented in Table 3. After PS adjustment, add-on users exhibited a decreasing BMI z-score trajectory, with an average monthly decline of 0.0200 following psychostimulant initiation (p = 0.0006). In contrast, SGA-only users had a significant weight gain trajectory, with an average monthly BMI z-score increase of 0.0262 (p = 0.0048). During the post-index period, add-on users had a significantly lower rate of weight gain compared with SGA-only users (β = −0.0463, p < 0.0001).
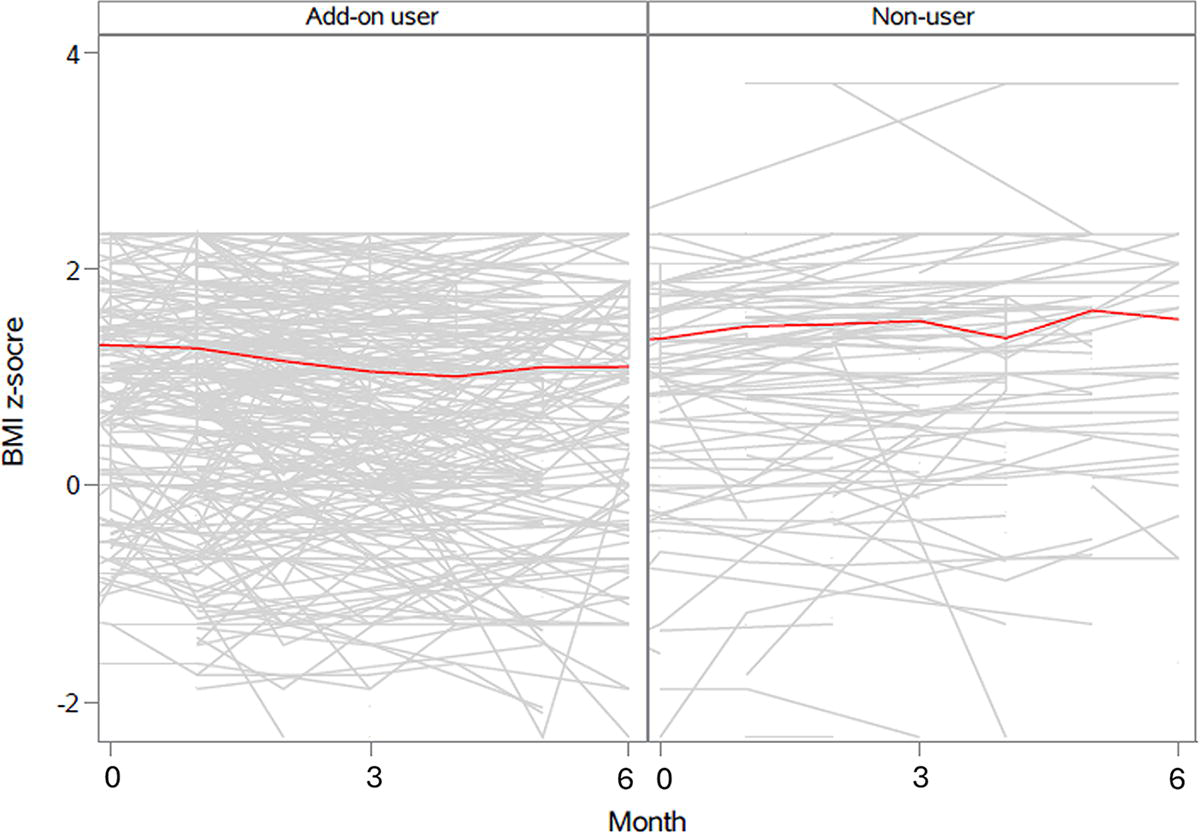
Spaghetti plots and Lowess curves of BMI z-score trajectories 6 months after the initiation of add-on psychostimulant, pediatric patients prescribed both SGA and psychostimulant and prescribed SGA-only. This figure presents spaghetti plots and locally weighted scatterplot smoothing (Lowess) curves depicting BMI z-score trajectories over 6 months following the initiation of add-on psychostimulant therapy. The analysis includes pediatric patients prescribed add-on psychostimulants, as well as those prescribed SGAs only. Individual patient trajectories are shown in the spaghetti plots, while the Lowess curves illustrate overall trends in BMI z-score changes within each group. BMI, body mass index; SGA, second-generation antipsychotic.
Sensitivity analysis
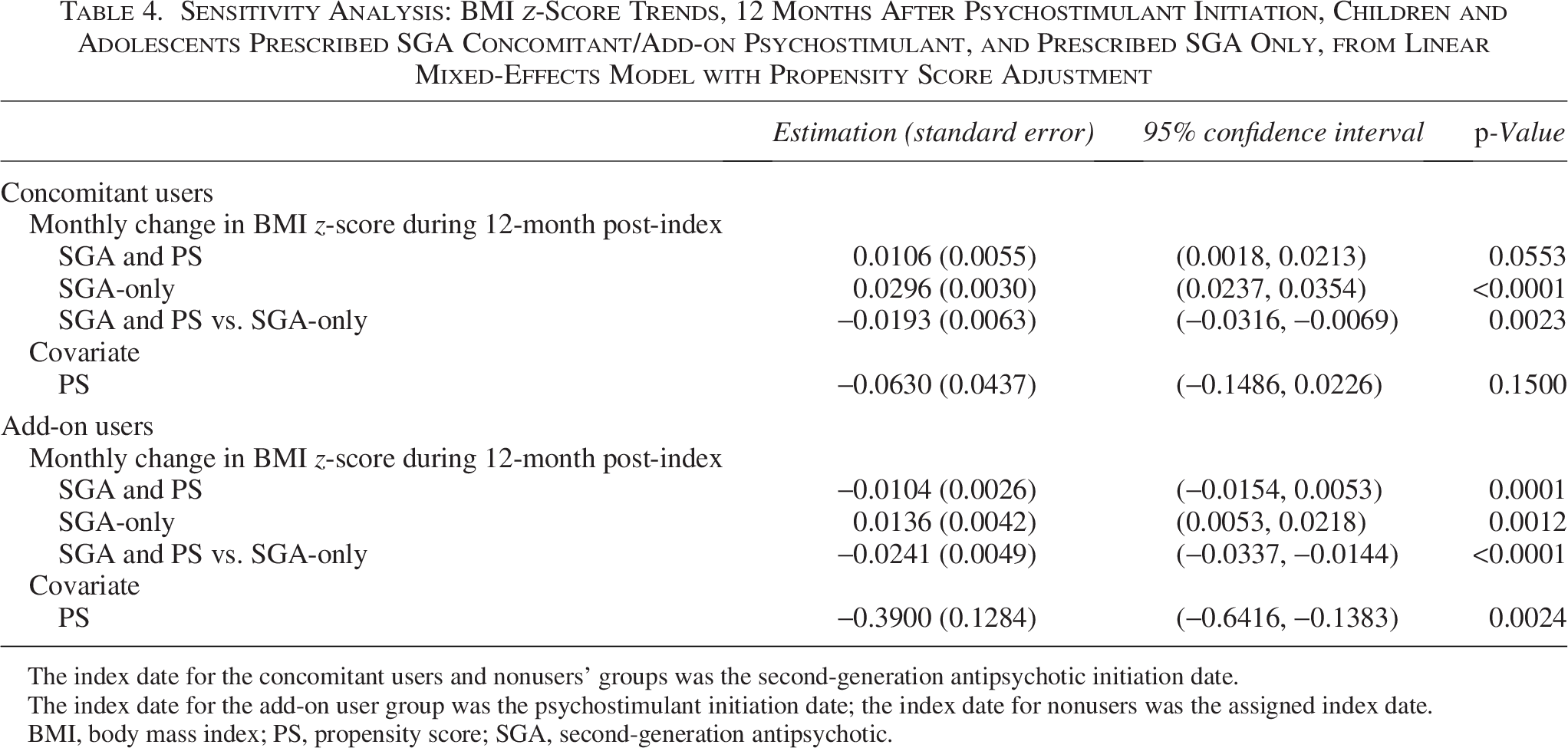
As shown in Table 4, the sensitivity analysis of BMI z-score trajectories was consistent with the primary analysis. Concomitant users did not experience significant weight gain (p = 0.0553), while SGA-only users had a significant average monthly BMI z-score increase of 0.0296 (p < 0.0001). Concomitant users had a significantly lower monthly BMI z-score change compared with SGA-only users (β = −0.0193, p = 0.0023).
Sensitivity Analysis: BMI z-Score Trends, 12 Months After Psychostimulant Initiation, Children and Adolescents Prescribed SGA Concomitant/Add-on Psychostimulant, and Prescribed SGA Only, from Linear Mixed-Effects Model with Propensity Score Adjustment
The index date for the concomitant users and nonusers’ groups was the second-generation antipsychotic initiation date.
The index date for the add-on user group was the psychostimulant initiation date; the index date for nonusers was the assigned index date.
BMI, body mass index; PS, propensity score; SGA, second-generation antipsychotic.
Sensitivity analysis for add-on users was also consistent with the primary analysis. Add-on users experienced an average monthly BMI z-score decrease of 0.0104 (p = 0.0001), whereas SGA-only users in this comparison had an average monthly BMI z-score increase of 0.0136 (p = 0.0012). Add-on users had a significantly lower average monthly BMI z-score change compared with SGA-only users (β = −0.0241, p < 0.0001).
Discussion
In child and adolescent psychiatry, those prescribed an SGA are often also prescribed a psychostimulant, with proportions ranging from 22% to 31% (Chen et al., 2023b; Kreider et al., 2014). Since psychostimulants may lead to weight loss, it is worth examining the degree to which SGA-associated weight gain might happen to be lower in those also prescribed psychostimulants.
Our investigation revealed that the concomitant and add-on use of psychostimulants may help mitigate SGA-associated weight gain. In our sample, an upward weight change trajectory following SGA initiation was observed in SGA-only users but not among those prescribed concomitant or add-on psychostimulants. After adjusting baseline covariates using PSs, the difference in these weight change trends reached statistical significance.
Despite the statistically significant effect of psychostimulants on AAWG observed in both concomitant and add-on users, the effect size was three times larger in add-on psychostimulant users (β = −0.0463, p < 0.0001) compared with concomitant users (β = −0.0143, p = 0.0063). This difference in effect size may be partially attributed to the distinct SGA recipients prescribed concomitant vs. add-on psychostimulants. The baseline BMI z-score was a mean of 1.09 (standard deviation [SD]: 0.09) for concomitant users at the time of psychostimulant initiation, whereas add-on users had an average baseline BMI z-score of 1.54 (SD: 0.10) on the index date. These findings suggest that psychostimulants may help prevent AAWG in concomitant users, while in the add-on users, they may halt or reduce AAWG that has already occurred.
Moreover, the effects observed in add-on psychostimulant users closely align with findings from our previous investigation into the effectiveness of adjunctive metformin for pediatric SGA recipients (β = −0.053, p = 0.0008) (Chen et al., 2023a). It is important to note that adjuvant metformin has primarily been prescribed to children who were stabilized on an SGA regimen and had experienced significant weight gain. On average, metformin was initiated 401 days (SD: 462 days) after SGA initiation, with a median of 223 days (IQR: 32–635 days). At the time of adjuvant metformin initiation, 83% of children were obese (BMI z-score >1.64), and 34% had either hyperglycemia or diabetes. In contrast, most add-on psychostimulants (76%) started within 90 days of SGA initiation. Although add-on users had a relatively higher BMI z-score than the concomitant users, their weights were significantly lower compared with the adjuvant metformin recipients. It remains unclear whether psychostimulants are more or less effective than metformin in mitigating AAWG. A head-to-head comparison is needed to determine the relative effect of these two interventions on children.
Previous investigations have highlighted that the most significant increase in BMI z-scores often occurs within the first 3–6 months of antipsychotic treatment, while weight gain can continue beyond 6 months, the rate of increase tends to stabilize over time (Lyu et al., 2024a, 2024b; Patel et al., 2017; Rummel-Kluge et al., 2010). To understand the longer-term effect of psychostimulants on AAWG, we further investigated the 12-month follow-up as sensitivity analyses for both concomitant users and add-on users. Our primary 6-month analysis suggested that both types of psychostimulant use may help mitigate AAWG. The sensitivity analysis confirmed these findings, offering additional insight into weight trajectories over time and reinforcing the robustness of the primary analysis.
Several limitations should be acknowledged in this study. First, the observational nature of our study design introduces inherent limitations, and as such, causal relationships cannot be conclusively established. Second, our dataset lacks information on certain influential factors, such as patients’ diets and genetic factors, which could potentially contribute to the observed weight gain associated with SGA (Goto et al., 2019; Memedi et al., 2017). Third, medication adherence was not evaluated in this study. What is more, the potential risks associated with adjunctive psychostimulants, such as drug interactions and habit-forming effects, have not been examined in this study. Lastly, the impact of drug dose on outcomes was not explored in this study, representing an additional aspect that warrants consideration in future investigations.
In conclusion, our study underscores the potential of concomitant and add-on psychostimulants that may mitigate AAWG in children and adolescents undergoing long-term SGA treatments. Further investigation is needed to understand their effectiveness and safety relative to other interventions for AAWG.
Authors’ Contributions
N.L.: Writing original draft, conceptualization, formal analysis and revision. P.J.R., T.J.V., S.A., Y.L., and H.C., reviewing and editing, conceptualization and supervision.
Footnotes
Clinical Significance
These findings offer valuable insights into the management of antipsychotic-associated weight gain (AAWG) in children and adolescents. As AAWG is a significant contributor to poor adherence to second-generation antipsychotics (SGAs), our results may help inform strategies to reduce treatment discontinuation related to AAWG. Ultimately, this could enhance the continuity of care and improve the overall well-being of youth with severe mental disorders.
Disclosures
All authors report no financial relationships with commercial interests.