
Abstract
Objective:
To describe the rates and predictors of youth and parent satisfaction following engagement in one of three evidence-based treatments or a placebo control for youth anxiety.
Method:
In a multisite randomized controlled trial (RCT) of youth ages 7–17 (n = 426) and parents (n = 429) comparing cognitive behavioral therapy (CBT), sertraline (SRT), the combination of the two (COMB), and placebo (PBO), we examined satisfaction at the end of acute treatment and assessed predictors including clinical change, pretreatment expectations, reactions to treatment assignment, and therapeutic relationship using multiple hierarchical linear regressions.
Results:
Satisfaction was high across all treatments. Both parents and youth reported the highest satisfaction with COMB, followed by CBT and SRT, and the least satisfaction with PBO. Parents were more satisfied than youth, and remitters were more satisfied than nonremitters. In CBT-containing arms, a stronger child–therapist relationship at week 6 predicted greater parent and youth satisfaction. Higher expectations of improvement at pretreatment predicted greater youth, but not parent, satisfaction in CBT and SRT.
Discussion:
Posttreatment, youth and parents report greater satisfaction with combination therapy over the monotherapies and PBO. Satisfaction patterns largely mirror clinical outcomes. An early strong youth-reported therapeutic alliance is key to satisfaction in CBT, highlighting the importance of child–therapist alignment when selecting anxiety treatments.
Keywords
Introduction
Pediatric anxiety disorders are common, costly, and increasing in prevalence (Baxter et al., 2013; Polanczyk et al., 2015; Racine et al., 2021; The U.S. Surgeon General’s Advisory, 2021; Wehry et al., 2015). Cognitive behavioral therapy (CBT) and psychopharmacological treatments (primarily selective serotonin reuptake inhibitors [SSRIs]) are first-line, effective interventions, either alone or in combination (Walkup et al., 2008). However, less is known about youth and parent satisfaction at the end of acute treatment for these evidence-based treatments. A greater understanding of satisfaction rates across CBT, SSRI, combination treatments, and a placebo comparison, as well as the clinical and process variables that predict satisfaction, may help both clinicians and families in their treatment decision making.
Satisfaction is an important outcome in psychological and pharmacological treatments for youth mental health problems (Hoagwood et al., 1996; Proctor et al., 2011). It has been linked to engagement-related factors, including retention and increased participation in treatment (Danko et al., 2016; Lindsey et al., 2014). Satisfaction also contributes to therapeutic alliance and treatment acceptability (Fjermestad et al., 2016; Gerdes et al., 2021; Ormhaug et al., 2015; Weisz et al., 2017). Moreover, it has been linked to parent- and youth-reported clinical outcomes, such as parental stress and clinical improvement (Acri et al., 2016; Brumley et al., 2021). A systematic review of treatment satisfaction with CBT for youth with anxiety or depression indicates that satisfaction tends to be moderate to high (Choque Olsson et al., 2021). A comparison of CBT, SSRI, and combination therapy in treatment for adolescents with depression indicated that satisfaction was high and undifferentiated across all groups, with parents and adolescents reporting similar rates (Dudley et al., 2005). Missing from the literature, though, is a comparison of parent and youth satisfaction across gold-standard pediatric anxiety treatments and an exploration of its predictors.
Treatment expectations, preferences, and the quality of the therapeutic alliance can powerfully influence satisfaction with anxiety treatment. While understanding of caregiver and youth anxiety treatment is growing (Brown et al., 2007; Mak et al., 2017), these preferences do not always align with treatment efficacy. For instance, although combination therapy (CBT + medication) leads to greater improvement in children’s anxiety than CBT alone (Walkup et al., 2008), many parents still prefer CBT over medication (Brown et al., 2007). Across treatment types, positive expectation of treatment effectiveness from parents, youth, and clinicians is associated with better clinical outcomes (Norris et al., 2019). In qualitative studies, parents emphasize the importance of trusting in their clinician when making treatment decisions (Mak et al., 2014). Additionally, a stronger therapeutic alliance also predicts better outcomes in CBT for anxious youth (Chiu et al., 2009; Cummings et al., 2013).
Satisfaction studies to date have evaluated the average between-group differences in satisfaction, and few, if any, have investigated predictors of satisfaction (particularly in youth anxiety) such as therapeutic alliance and treatment expectations (Auby, 2016; Chiu et al., 2009; Fjermestad et al., 2016; Ormhaug et al., 2015). Furthermore, how patients’ improvement influences satisfaction has received little attention and produced inconsistent results (Nauphal et al., 2021; Viefhaus et al., 2019). Integrating clinical outcomes (e.g., treatment response), treatment expectations, and a therapeutic relationship measure may help to clarify how clinical and process variables predict satisfaction.
The Child/Adolescent Anxiety Multimodal Study (CAMS; Walkup et al., 2008) is the largest randomized controlled trial (RCT) for youth anxiety disorders. CAMS is uniquely situated to assess satisfaction across common anxiety treatments because it includes pill placebo (PBO) and the three most common evidence-based youth anxiety treatments (Walter et al., 2020): SSRI (sertraline; hereinafter referred to as SRT), CBT (Coping Cat or C.A.T. project based on developmental level), and combined SRT and CBT treatment (COMB). Using separate data from parents and children, we (1) characterized and compared rates of satisfaction across reporters, interventions, and remission status and (2) examined clinical predictors (e.g., changes in severity, impairment, and symptoms) and process predictors (e.g., expectation of treatment, reaction to treatment assignment, and therapeutic relationship) of posttreatment satisfaction. Given documented differences in youth- and parent-reports, we expected similar differences here, although we hypothesized no specific direction (Marsh et al., 2020). Similarly, we expected different rates of satisfaction based on intervention (higher preferences for COMB) and remission status (higher satisfaction for remitters). Based on the existing literature, we expected that a more positive therapeutic relationship would predict higher satisfaction (Chiu et al., 2009; Karver et al., 2018; McLeod, 2011).
Methods
Child/Adolescent Anxiety Multimodal Study
CAMS was a large (N = 488) multisite efficacy trial comparing COMB, CBT, SRT, and PBO in the treatment of youth anxiety disorders. Participants were aged 7–17 years. All youth participants met criteria for generalized anxiety disorder (GAD), social phobia (SOP), and/or separation anxiety disorder (SAD) based upon Diagnostic and Statistical Manual for Mental Disorders (4th ed.; DSM-4; American Psychiatric Association, 1994). After eligibility was determined but prior to randomization, families met with a study principal investigator to ensure understanding and willingness for randomization. Participants were randomized to 12 weeks of COMB (n = 140), CBT (n = 139), SRT (n = 133), or PBO (n = 76) in a 2:2:2:1 ratio.
Participants receiving CBT, those in the CBT and COMB arms, met with their therapist for fourteen 60-minute sessions over 12 weeks. Participants in the pharmacotherapy arms, SRT, PBO, and COMB, met with their prescribers for a first 60-minute session in week 1 and then 30 minutes in weeks 2–4, 6, 8, 10, and 12. Due to the study design, participants in CBT and COMB arms were not blind to their assigned study group, whereas those in the SRT and PBO arms were blinded to which of the two arms they were in. All independent evaluators were blind to participants’ assigned treatment group throughout. Additional CAMS study methodology and outcomes have been described elsewhere (Compton et al., 2010; Kendall et al., 2010; Walkup et al., 2008).
Recruitment occurred at Duke University Medical Center, New York State Psychiatric Institute—Columbia University Medical Center—New York University, Johns Hopkins Medical Institutions, Temple University, University of California, Los Angeles, and Western Psychiatric Institute and Clinic—University of Pittsburgh Medical Center. The protocol was approved and monitored by institutional review boards at each center and by the data and safety monitoring board of the National Institute of Mental Health.
The Current Study
Participants
All available youth and parent satisfaction data from the CAMS trial were used (N = 429 parent and N = 426 youth reports) across the four intervention groups. Children and adolescents were aged 11.1 ± 2.8 years, were 49.9% female (n = 217), mostly White (n = 47; 79.8%), and not Hispanic (n = 385; 88.5%). At baseline, 34.7% (n = 151) met DSM-4 criteria for SAD, 51.7% (n = 225) had SOP, and 55.2% (n = 240) had GAD. A significant number of youth met criteria for two (41.8%) or three (36.3%) anxiety disorders.
Thirty-eight CBT therapists (Mage = 30.1 ± 4.4 years) participated in the CAMS study, representing doctoral candidates, social workers, and clinical psychologists. Clinicians were mostly White (92%) and female (84%). Therapists held master’s (37%) or doctorate (58%) degrees in psychology and on average had 5.6 ± 2.4 years of experience treating anxious youth (Podell et al., 2013). Prescribers in the pharmacotherapy arms were psychiatrists and nurse clinicians with experience in medicating children with anxiety disorders and were certified in the study pharmacotherapy protocol (Walkup et al., 2008).
Measures
Outcome: Satisfaction
Patient Satisfaction Questionnaire
The Patient Satisfaction Questionnaire (PSQ) is an eight-item youth (PSC-C) and parent (PSC-P) assessment of satisfaction. Questions such as “How satisfied are you with the amount of help you have received?” and “How would you rate the quality of care you received?” are answered on a 4-point scale with scores of 1 or 2 indicating lack of satisfaction and scores of 3 or 4 indicating satisfaction and then summed (range 8–32). Measurements were taken at 12 weeks, immediately postacute treatment. For those in the SRT and PBO arms, ratings were gathered before unblinding.
Predictors: Clinical variables
Clinical Remission on the Clinical Global Impressions–Severity scale (Guy, 2000)
The Clinical Global Impressions–Severity (CGI-S) is a clinician-administered measure of clinical severity and is rated on a scale of 1 (not at all ill) to 7 (extremely ill). CGI-S scores can be used to assess change in symptoms over time and reflect remission (i.e., scores of 1 or 2; Ginsburg et al., 2011). This study used the CGI-S provided by independent evaluators (blind to intervention group assignment) at baseline and 12 weeks.
Child Anxiety Impact Scale (Langley et al., 2004)
The Child Anxiety Impact Scale (CAIS) is a 27-item youth-report (CAIS-C) and parent-report (CAIS-P) of anxiety-related impairment across school, social, and home/family functioning. Each item is rated on a 4-point scale, where 0 = not at all and 3 = very much; higher CAIS scores indicate greater impairment (range 0–81). In this study, the sum scores at baseline and at week 12 were used.
Screen for Child Anxiety and Related Disorders (Birmaher et al., 1999)
The Screen for Child Anxiety and Related Disorders (SCARED) is a 41-item youth- and parent-report of anxiety symptoms and generates a total symptom severity score. The SCARED is measured on a 3-point scale where 0 = not true/hardly ever true and 2 = very/often true, where higher scores indicate more severe symptoms (ranging from 0 to 82). Sum scores for youth (SCARED-C) and parent (SCARED-P) at baseline and at week 12 were used.
Predictors: Process variables
Pretreatment expectation
Pretreatment expectation was assessed by asking each child and parent to rate how much improvement they expected if assigned to each of the three active treatments (CBT, SRT, and COMB) on a 7-point scale (1 = very much improved to 7 = very much worse). Lower scores indicated higher expectations about treatment. This measure was administered prior to randomization. For the current analyses, the rating for the treatment the child was assigned to was used. For PBO, the SRT rating was used. Of note, when considering the expectation of improvement in the SRT group, families were aware that this assignment was blinded with the potential to be assigned to PBO and not know it until after the acute treatment period.
Reaction to Treatment Assignment
Immediately following randomization and prior to the initiation of treatment, each child and parent rated their reaction to their assignment on a 5-point scale (1 = extremely disappointed to 5 = extremely pleased). Of note, COMB and CBT assignments were unblinded. Assignment to the medication-only groups left participants blind to whether they were in SRT or PBO.
Child’s Perception of the Therapeutic Relationship
The Child’s Perception of the Therapeutic Relationship (CPTR) is a 10-item youth-report of the quality of the therapeutic relationship. Questions such as “How much do you like your therapist?” are answered on a 5-point scale, with higher scores indicating a warmer therapeutic relationship and more positive perceptions of the therapist. For analyses, the mean CPTR score (ranging from 1 to 5) from the 6-week timepoint was used. In the CBT arm, ratings pertained to the CBT therapist. In the SRT and PBO arms, they pertained to the prescriber. In the COMB arm, children rated both the CBT therapist and the prescriber with scores averaged for analyses. See Cummings et al. (2013) for additional descriptive statistics of the CPTR and associations with outcomes.
Missing data
All available youth and parent satisfaction ratings were included in analyses. As previously described, missing clinical outcome data (CGI-S, CAIS, and SCARED at 12 weeks) were imputed using a multiple imputation approach (Ginsburg et al., 2014; Walkup et al., 2008).
Data analysis
Analyses were conducted in SPSS v30, and we used an alpha level of .05 for all statistical tests. To characterize satisfaction rates by intervention group, reporter, and remission status, we first examined descriptive statistics (means, standard deviations, and ranges). Possible covariates of age and gender were assessed with correlations and independent sample t-tests. Next, we investigated satisfaction differences across intervention groups for parents and then children with analysis of variance (ANOVA) and post hoc comparisons. Due to a significant Brown–Forsythe test, we used a conservative post hoc approach to analyzing differences across intervention groups (Sauder and DeMars, 2019). Dunnett T3 is equipped to handle pairwise comparisons for uneven group sizes and unequal variances (Sauder and DeMars, 2019). Student’s t-tests were used to compare satisfaction rates for parents and youth (paired sample t-tests), and remitters (CGI-S < 3) versus nonremitters (independent sample t-tests).
Pearson correlations examined associations between process variables and satisfaction for parents and youth by intervention group. Next, multiple hierarchical linear regression models were built to assess clinical predictors and significant process predictors for each intervention group and reporter. In these models, predictors are added to the model in blocks, which allows for examination of how a set of predictors (e.g., T1 and T2 clinical level from three measures) account for variance in the criterion. Assumptions of hierarchical regression were assessed and met (Tabachnick et al., 2019). Tests of collinearity were all met with Variance Inflation Factors <5. Step 1, the baseline model, assessed for baseline effects of clinical severity (CGI-S), impairment (CAIS-C/P), and symptoms (SCARED-C/P) on youth and parent satisfaction (PSQ-C/P). Step 2, the clinical change model, assessed the additive and overall predictive value of change in clinical outcome measures by including the 12-week severity, impairment, and symptom ratings. Step 3 assessed the additive and overall predictive value of including pretreatment expectation, reaction to assignment, and/or the youth’s report of week 6 therapeutic relationship (CPTR) when indicated by Pearson correlations.
Results
In Table 1, we present descriptive statistics for parent and youth satisfaction for all participants and then by intervention group and remission status. Child’s age was not associated with parent (r[420] = −.009, p = 0.855) or youth satisfaction (r[423] = −.074, p = 0.129). Satisfaction did not differ based on child gender (parent: t[423] = −.108, p = 0.914; child: t[420] = .038, p = 0.970).
Descriptive Statistics on the Patient Satisfaction Questionnaire by Reporter and by Remission Status
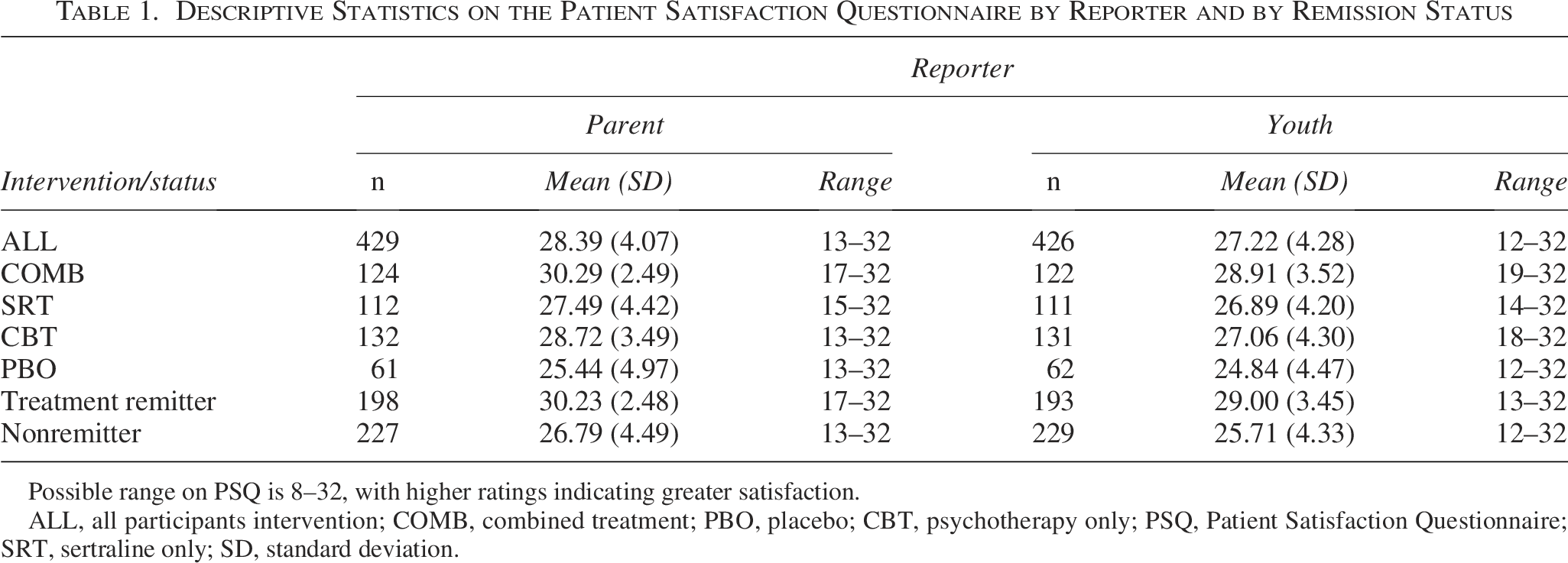
Possible range on PSQ is 8–32, with higher ratings indicating greater satisfaction.
ALL, all participants intervention; COMB, combined treatment; PBO, placebo; CBT, psychotherapy only; PSQ, Patient Satisfaction Questionnaire; SRT, sertraline only; SD, standard deviation.
Comparing satisfaction rates across interventions
An ANOVA revealed significant differences in parent satisfaction across intervention groups, F(3, 425) = 25.51, p < 0.001. The effect size for the overall comparison was
Post Hoc Dunnett T3 Tests Comparing the Patient Satisfaction Questionnaire by Intervention Group for Parents and Youth
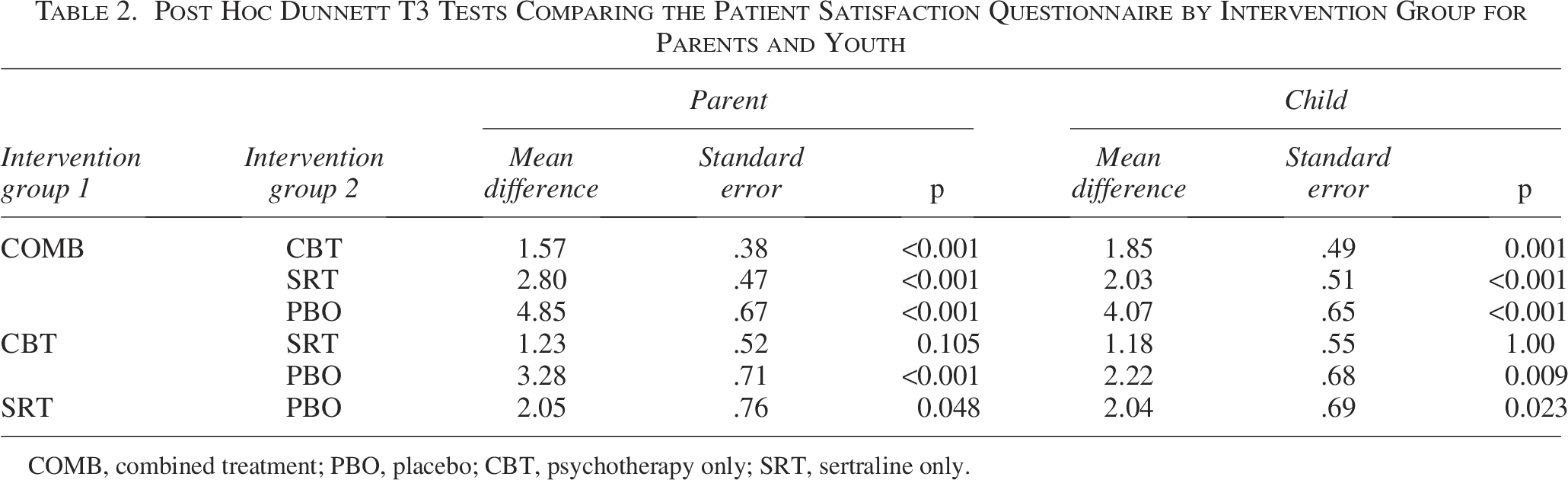
COMB, combined treatment; PBO, placebo; CBT, psychotherapy only; SRT, sertraline only.
Youth also reported the most satisfaction with COMB, followed by CBT and SRT, and then PBO. The ANOVA for youth-reported satisfaction and subsequent Dunnett T3 test revealed a significant difference in youth satisfaction across intervention groups and an identical pattern of comparisons, F(3, 422) = 14.27, p < 0.001 (see Table 2, columns 5 and 6). The effect size for the overall comparison was
Comparing satisfaction rates by reporter and remission status
Parent and youth satisfaction scores were highly positively correlated (r = .50, p < 0.001), yet significantly different (t[419] = 5.51, p < 0.001, Hedges’s g = 4.18) with parents reporting higher satisfaction (M = 28.39, SD = 4.07) than youth (M = 27.23, SD = 4.28). For parent-report, remitters (M = 30.23, SD = 2.48) reported significantly higher rates of satisfaction than nonremitters (M = 26.79, SD = 4.49; t[423] = −9.57, p < 0.001, Hedges’s g = 3.70). For youth-report, remitters (M = 29.00, SD = 3.45) were likewise more satisfied compared to nonremitters (M = 25.71, SD = 4.33; t[420] = −8.53, p < 0.001, Hedges’s g = 3.96).
Correlations and regressions examining predictors of satisfaction between interventions
Pearson correlations between process variables and parent and child satisfaction are reported in Table 3.
Pearson Correlations of Process Variables and Satisfaction (Parent and Child Report) by Intervention Group

For pretreatment, expectation and reaction to assignment correlations are among the same raters.
*p < 0.05, **p < 0.01, ***p < 0.001.
CPTR, Child’s Perceived Therapeutic Relationship at week 6; COMB, combined treatment; PSQ-P/C, Patient Satisfaction Questionnaire–Parent and Child version; PBO, placebo; CBT, psychotherapy only; SRT, sertraline only.
Predictors of satisfaction in COMB
Parent
Neither the Step 1 baseline model (F[3, 117] = .73, p = 0.538) nor the Step 2 clinical change model (F[6, 114] = 1.95, p = .079) was significant. The Step 3 model was significant, F(7, 113) = 2.55, p = .018, with an R2 of .14, indicating that the model explained about 14% of the variance in parent satisfaction with greater child–therapist relationship at week 6 (
Youth
Neither the Step 1 baseline model (F[3, 115] = 2.04, p = 0.112) nor the Step 2 clinical change model (F[6, 112] = 1.82, p = 0.102) was significant. The Step 3 model, which included the child’s pretreatment expectation and the therapeutic relationship measure, was significant, F(8, 110) = 4.08, p < 0.001, with an R2 of .23, indicating that the model explained about 23% of the variance in youth satisfaction. Although the R2 change from Step 2 to Step 3 indicated that the process variables explained significant additive variation in youth satisfaction over the change in clinical outcomes explained by the Step 2 model alone, only the youth’s report of the therapeutic relationship at week 6 was significant (
Hierarchical Linear Regression Investigating Clinical and Process Predictors of Parent and Youth Satisfaction in the Combination Group with Step 3 Coefficients Presented
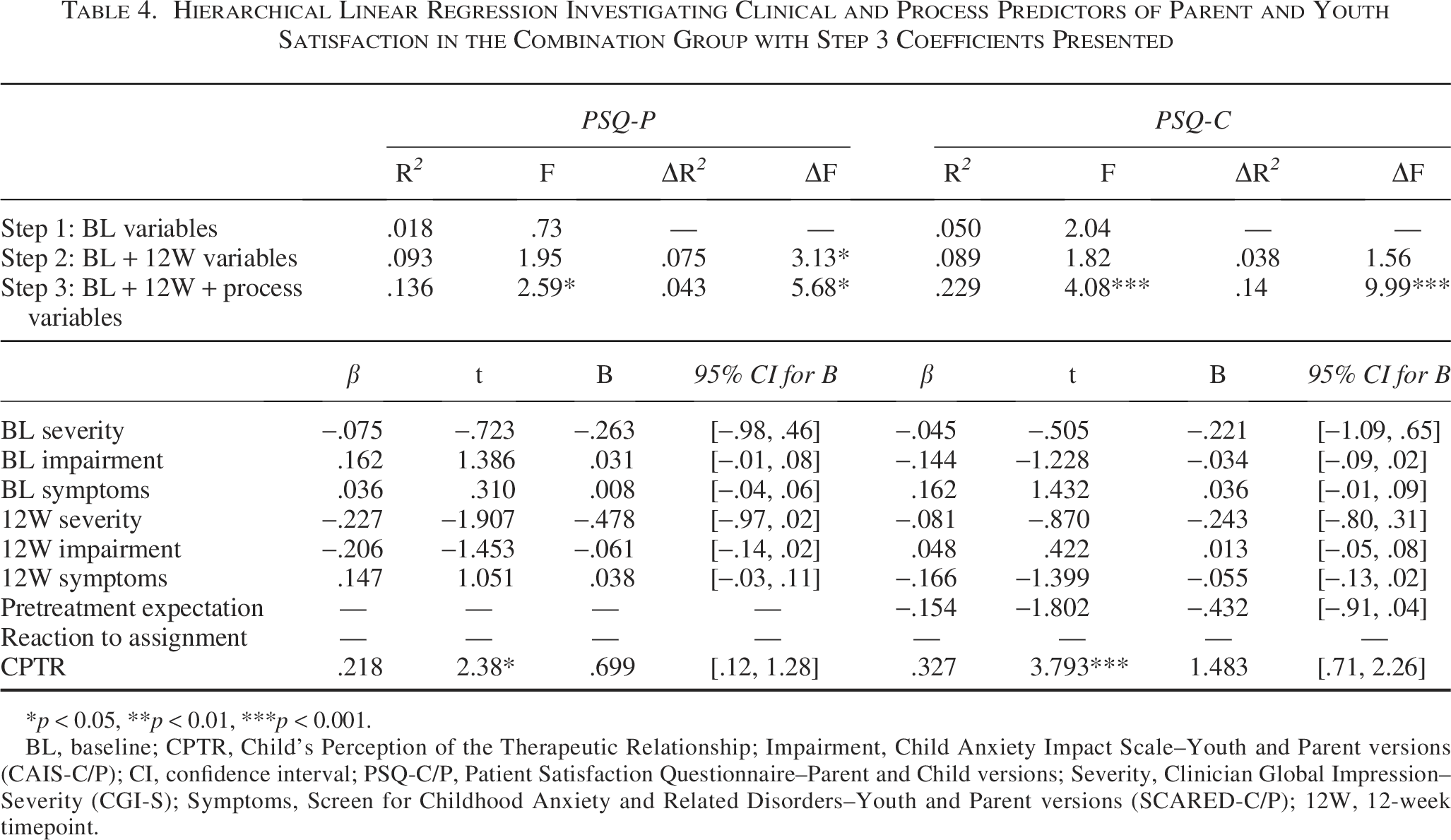
*p < 0.05, **p < 0.01, ***p < 0.001.
BL, baseline; CPTR, Child’s Perception of the Therapeutic Relationship; Impairment, Child Anxiety Impact Scale–Youth and Parent versions (CAIS-C/P); CI, confidence interval; PSQ-C/P, Patient Satisfaction Questionnaire–Parent and Child versions; Severity, Clinician Global Impression–Severity (CGI-S); Symptoms, Screen for Childhood Anxiety and Related Disorders–Youth and Parent versions (SCARED-C/P); 12W, 12-week timepoint.
Predictors of satisfaction in CBT
Parent
The Step 1 baseline model was not significant, F(3, 128) = 0.97, p = 0.41. The Step 2 clinical change model was significant, F(6, 125) = 11.98, p < 0.001, indicating greater clinical improvement predicted by higher satisfaction. The Step 3 model, which included all three process variables, was also significant, F(9, 122) = 9.79, p < 0.001, with the model explaining about 42% of the variance in parent satisfaction (R2 = .42). Among process variables, pretreatment expectation was significant (
Youth
The Step 1 baseline model was not significant, F(3, 127) = 0.40, p = 0.76. The Step 2 clinical change model was significant, F(6, 124) = 4.12, p < 0.001, with greater clinical improvement predicting more satisfaction. The Step 3 model, which included all three process variables, was also significant, F(9, 121) = 8.97, p < 0.001, with an R2 of .40, indicating that the model explained about 40% of the variance in parent satisfaction. Both pretreatment expectations (
Hierarchical Linear Regression Investigating Clinical and Process Predictors of Parent and Youth Satisfaction in the Cognitive Behavioral Therapy Group with Step 3 Coefficients Presented

*p < 0.05, **p < 0.01, ***p < 0.001; +p = 0.053.
BL, baseline; CPTR, Child’s Perception of the Therapeutic Relationship; CI, confidence interval; Severity, Clinician Global Impression–Severity (CGI-S); Impairment, Child Anxiety Impact Scale–Youth and Parent versions (CAIS-C/P); PSQ-C/P, Patient Satisfaction Questionnaire–Parent and Child versions; Symptoms, Screen for Childhood Anxiety and Related Disorders–Youth and Parent versions (SCARED-C/P); 12W, 12-week timepoint.
Predictors of satisfaction in SRT
Parent
The Step 1 baseline model was not significant, F(3, 107) = 0.71, p = 0.548. The Step 2 clinical change model was significant, F(6, 104) = 10.90, p < 0.001, with an R2 of .39 and with greater clinical improvement predicting more satisfaction. The R2 change = .37, p < 0.001, indicated that the Step 2 model explained parent satisfaction outcomes significantly better than the Step 1 baseline model. A Step 3 model was not included due to no significant correlations among process variables and parent satisfaction for SRT.
Youth
The Step 1 baseline model was not significant, F(3, 106) = 0.19, p = 0.90. The Step 2 clinical change model was significant, F(6, 103) = 7.22, p < 0.001, with greater clinical improvement predicting more satisfaction. The Step 3 model, which included pretreatment expectation, was significant, F(7, 102) = 7.06, p < 0.001, with an R2 of .28, indicating that the model explained about 28% of the variance in youth satisfaction. The R2 change = .03, p = 0.034, indicated that the Step 3 model explained satisfaction outcomes significantly better than clinical change alone, with pretreatment expectation being a significant predictor (
Hierarchical Linear Regression Investigating Clinical and Process Predictors of Parent and Youth Satisfaction in the Sertraline Group with Step 2 Coefficients for Patient Satisfaction Questionnaire–Parent and Step 3 Coefficients for Patient Satisfaction Questionnaire–Child Presented

*p < 0.05, **p < 0.01, ***p < 0.001.
BL, baseline; CPTR, Child’s Perception of the Therapeutic Relationship; CI, confidence interval; Severity, Clinician Global Impression–Severity (CGI-S); Impairment, Child Anxiety Impact Scale–Youth and Parent versions (CAIS-C/P); PSQ-C/P, Patient Satisfaction Questionnaire–Parent and Child versions; Symptoms, Screen for Childhood Anxiety and Related Disorders–Youth and Parent versions (SCARED-C/P); 12W, 12-week timepoint.
Predictors of satisfaction in PBO
Parent
The Step 1 baseline model was not significant, F(3, 57) = 0.70, p = 0.56. The Step 2 clinical change model was significant, F(6, 54) = 3.60, p = 0.004, with greater clinical improvement predicting more satisfaction and with an R2 of .29, indicating that the model explained about 29% of the variance in parent satisfaction. The R2 change = .25, p < 0.001, indicated that the Step 2 clinical change model explained satisfaction outcomes significantly better than the Step 1 baseline model. A Step 3 model was not included due to no significant correlations among process variables and parent satisfaction for PBO.
Youth
The Step 1 baseline model was not significant, F(3, 58) = 0.06, p = 0.98. The Step 2 clinical change model was significant, F(6, 55) = 3.68, p = 0.004, with greater clinical improvement predicting more satisfaction and with an R2 = .29, indicating that clinical change accounts for 28% of the variance in child satisfaction. The Step 3 model, which included pretreatment expectation, was statistically significant, F(7, 54) = 3.707, p = 0.002, but the R2 change = .04, p = 0.087, was not significant and indicates that pretreatment expectations does not explain a significant amount of variance in child treatment satisfaction once clinical change has been accounted for. See Table 7 for PBO regression statistics.
Hierarchical Linear Regression Investigating Clinical and Process Predictors of Parent and Youth Satisfaction in the Placebo Group with Step 2 Coefficients for Patient Satisfaction Questionnaire–Parent and Step 3 Coefficients for Patient Satisfaction Questionnaire–Child Presented
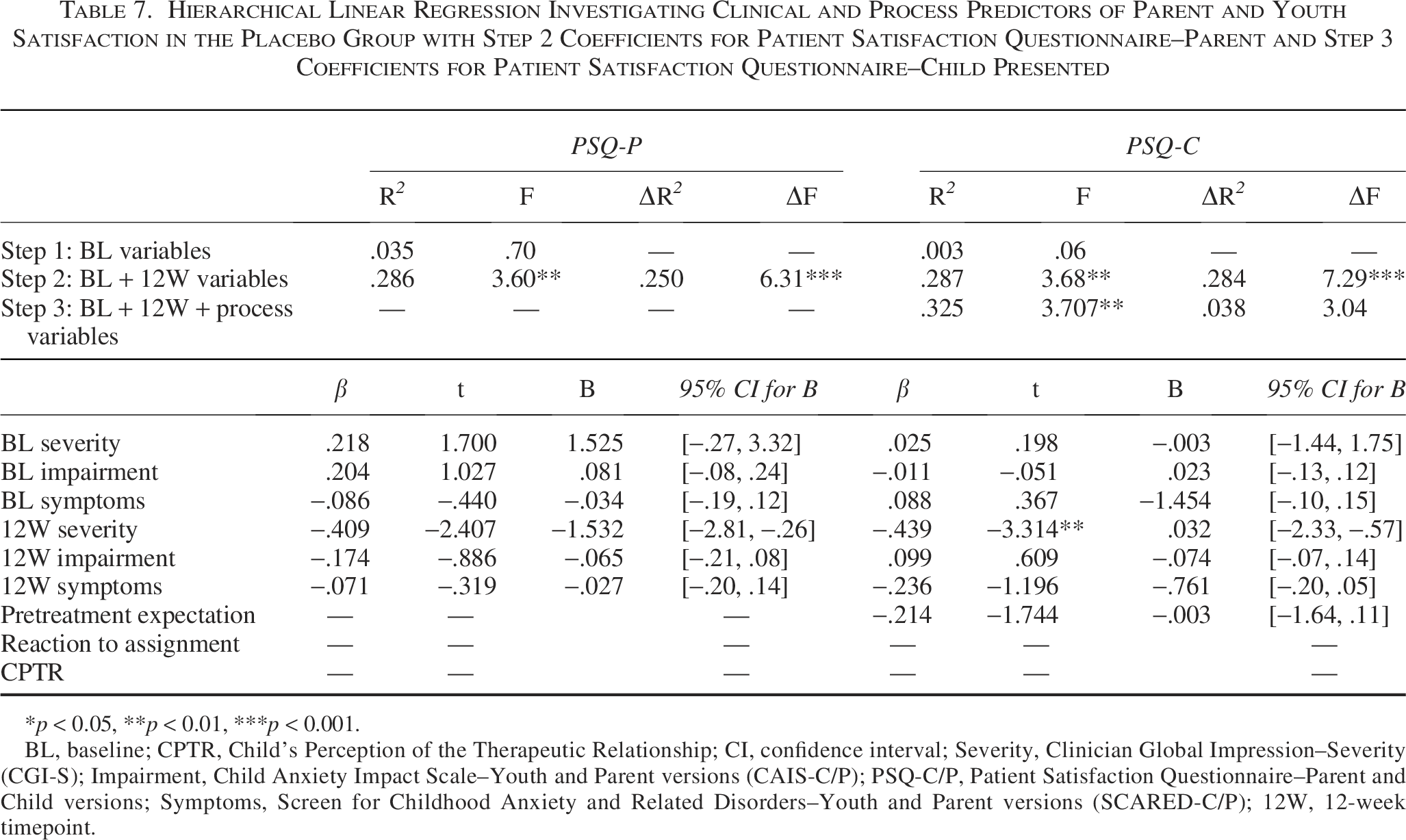
*p < 0.05, **p < 0.01, ***p < 0.001.
BL, baseline; CPTR, Child’s Perception of the Therapeutic Relationship; CI, confidence interval; Severity, Clinician Global Impression–Severity (CGI-S); Impairment, Child Anxiety Impact Scale–Youth and Parent versions (CAIS-C/P); PSQ-C/P, Patient Satisfaction Questionnaire–Parent and Child versions; Symptoms, Screen for Childhood Anxiety and Related Disorders–Youth and Parent versions (SCARED-C/P); 12W, 12-week timepoint.
Discussion
This is the first study to examine youth and parent satisfaction across three evidence-based treatments for children and adolescents with anxiety disorders and to use a placebo control. It is also the first to consider how clinical improvement, treatment expectations, reactions to treatment assignments, and therapeutic relationships influence patient satisfaction.
For both parents and youth, satisfaction rates were high across all four assigned groups; as expected, they mirrored the primary clinical outcomes of the trial with combination treatment, resulting in more satisfaction than all other treatments. There was similar satisfaction with SRT and CBT monotherapy, with the lowest satisfaction reported for placebo. Baseline severity, impairment, and symptoms did not predict satisfaction in any group. Findings from this study have important implications for clinicians wishing to connect youth with anxiety disorders to treatment. Referring clinicians can confidently report that there is a high likelihood that both children and parents will be satisfied with any current evidence-based treatment options—no matter the youth’s baseline severity. Alongside counseling families about the superior clinical response expected with combination treatment, clinicians can also convey that youth and families appear to be most satisfied with it relative to the monotherapies. Indeed, although some families hesitate about medication-containing treatment before initiating care (Lewin et al., 2014) and may prefer CBT (Brown et al., 2007), clinicians may find it helpful to share information about the higher levels of satisfaction for combination treatment when acute care is complete. Of note, it is possible that attrition bias led to inflated treatment satisfaction ratings. However, overall withdrawal rates were low (11%), and efforts were made to collect satisfaction ratings even from those who did not complete treatment (Walkup et al., 2008).
For parents, both expectations about their assigned treatment and their initial reaction to their assignment had surprisingly little impact on satisfaction at the end of treatment. Though reaction to assignment is specific to clinical trials, its lack of association with treatment satisfaction may reduce clinicians’ hesitation to recommend treatments despite families’ initial emotional reactions. In contrast, the youth’s pretreatment expectation mattered in both the CBT and SRT groups. Taking time to address children’s expectations prior to the start of treatment and offer any additional education may be key to improving their satisfaction with treatment.
Additionally, attention to securing a strong early treatment relationship with the child is likely important in influencing ultimate satisfaction with treatment. In both CBT-containing groups, the CPTR at week 6 influenced parent and youth treatment satisfaction at the end of treatment. These results buttress prior findings on the power of the therapeutic alliance—the keystone of evidence-based treatment for youth, regardless of treatment (Roest et al., 2023). Therapeutic alliance with the prescriber in the SRT and PBO groups did not have the same influence. Measuring the therapeutic relationship in all four groups allowed for a comparison; however, study design necessitated that therapists spend more time with families than the prescriber, and this time difference is hard to control for. These findings from therapy-containing groups (combination and CBT) may relate to alliance–outcome associations (Karver et al., 2018; McLeod, 2011). The therapeutic relationship, a major component of the alliance, consistently predicted satisfaction in the context of exposure-heavy treatment.
Selection bias and the generalizability of these findings to other clinical settings are key to consider in this study, given that satisfaction ratings were derived from participants in an RCT where treatments were supervised to achieve optimal quality and provided at no cost. Youth and parents in this clinical trial accepted randomization to any of the four treatment arms as a prerequisite to participating in this study. While this study accounted for participants’ reactions to treatment assignment, individuals with strong treatment preferences may have opted out. Future studies should capture data on those initially expressing interest but declining participation due to treatment preference.
A key advantage of RCTs is the ability to collect a broad array of data—including independent evaluations—which allows for a deeper examination of treatment-related phenomena. In clinical settings, however, the implementation of measurement-based care is often limited by concerns about patient burden (Lewis et al., 2019). The present findings broadly suggest that satisfaction at the end of 12 weeks of treatment is largely driven by clinical improvement. Although youth reported lower satisfaction, on average, both youth and parent satisfaction are shaped by similar factors. These findings raise the possibility that a more streamlined set of measures could still yield meaningful insights into satisfaction without overburdening patients.
While this is one of the first studies to examine treatment satisfaction in children and adolescents with anxiety disorders, there are several important limitations. Satisfaction was measured at a single timepoint (end of acute treatment): It would be valuable to examine satisfaction at follow-up and track changes over time, including for CBT, the possible impact (positive or negative) that introducing exposures may have on reported satisfaction. Although this study draws from the largest sample of anxious youth to date, it is largely homogeneous, which limits our ability to understand the impact of race, ethnicity, socioeconomic status, and other social determinants of health on satisfaction. This is especially important since treatment outcomes differ for psychotherapeutic interventions in minoritized youth with depressive and anxiety disorders (Gordon-Hollingsworth et al., 2015; Strawn et al., 2022).
Conclusions
This study provides important information about how children and parents perceive evidence-based treatments for anxiety after direct experience. While satisfaction mirrored clinical outcomes—highest in combination therapy, followed by CBT and SRT, and lowest with placebo—baseline severity and impairment did not predict satisfaction. Parents’ initial expectations and reactions had little impact on satisfaction, suggesting clinicians need not hesitate in recommending treatments despite families’ initial concerns. In contrast, youth pretreatment expectations significantly influenced satisfaction in the CBT and SRT groups, underscoring the importance of setting realistic expectations and providing early psychoeducation. Additionally, the therapeutic alliance played an important role in CBT-containing treatments, predicting both parent and youth satisfaction. Clinicians may consider emphasizing combination treatment’s superior outcomes and satisfaction rates while addressing youth expectations. Such strategies may enhance engagement, adherence, and overall treatment success.
Clinical Significance
Clinicians can share with families that, at the end of acute treatment, satisfaction is high for parents and children across all three evidence-based treatments for youth anxiety; it is highest for combined treatment, which aligns with clinical response. Youth satisfaction is partly shaped by pretreatment expectations, so offering additional education and addressing youth concerns prior to treatment may be helpful. The early therapeutic relationship between youth and their therapist influences both child and parent satisfaction at the end of acute treatment. Prioritizing an early positive alliance with the patient will likely increase treatment satisfaction for both children and parents.
Footnotes
Disclosures
G.D.M. and R.G.M. have no disclosures. J.C.P. has received research support from the National Institute of Mental Health (NIMH) and the Patient-Centered Outcomes Research Institute (PCORI), advisor fees and equity from Lumate Health; publication royalties from Guilford Press, Oxford University Press, and Elsevier; and travel/speaking honoraria from the Tourette Association of America and International OCD Foundation. In addition, he is part-owner of Virtually Better Health, LLC, a developer of digital evidence-based mental health treatments. J.R.S. has received research support from AbbVie, Alkermes, MindMed, PCORI, and the National Institutes of Health (NIH). He has provided consultation to Alkermes, AbbVie (Cerevel), Intracellular Therapeutics, MindMed, Supernus, Boehringer-Ingelheim and Otsuka. He receives royalties from Springer Publishing, Cambridge University Press, and UpToDate and received material support from Myriad. He serves on an advisory board for Genomind (unpaid). He has also received honoraria from Medscape Live, the Neuroscience Education Institute. P.C.K. receives royalties from the sales of materials related to the treatment of anxiety in youth. S.N.C. receives research support from the NIH and has also received royalties from Elsevier and Academic Press. J.T.M. has received research support from Jazz Pharmaceuticals, PCORI, and the NIH. He has provided consultation to the Coalition for Aligning Science and the University of Texas System. He has received honoraria from the American Academy of Neurology and the American Physicians Institute. J.T.W. receives royalties from Oxford Press and Wolters Kluwer. T.S.P. has received research support from the National Science Foundation, the NIMH, and PCORI. She receives royalities from Elsevier and Oxford University Press.