
Abstract
Objective:
Current standards for treatment of anorexia nervosa (AN) in children and adolescents include Family-Based Treatment and nutrition restoration. The use of aripiprazole for AN has been detailed through case series and one retrospective review analyzing the change in outcomes on body mass index and weight restoration. The goal of this descriptive study was to evaluate the impact of aripiprazole on food avoidant behaviors (FABs) and to describe prescribing patterns, including dosing and tolerability.
Methods:
This was a retrospective, descriptive, matched, cohort study of pediatric patients with AN admitted to an eating disorders program (EDP) between January 1, 2018, and December 31, 2023. Patients were included in this study if they had a diagnosis of AN and were started on aripiprazole for eating disorder cognitions. Patients were matched 1:2 to a control group based on age, sex, and length of stay.
Results:
A total of 42 patients on aripiprazole were analyzed and matched to 84 controls. Aripiprazole was associated with a reduction in FABs with a mean change over the evaluated time period of 3.5 versus 0.9 (p = 0.026). The mean starting dose of aripiprazole was 1.9 mg/day, with a mean discharge dose of 2.8 mg/day. Aripiprazole was overall well-tolerated.
Conclusion:
Aripiprazole was associated with an improvement in FABs among children and adolescents admitted to an EDP. Additionally, low-dose aripiprazole improved weight, likelihood of achieving target weight, and was well-tolerated.
Introduction
Anorexia nervosa (AN) is a life-threatening mental health condition characterized by weight loss achieved through dieting, fasting, and/or excessive exercise (restrictive type) or through self-induced vomiting, misuse of laxatives, or diuretics (binge-eating/purging type) (American Psychiatric Association, 2022). These behaviors are accompanied by severe cognitive distortions and obsessive preoccupations regarding eating, weight gain, food, and/or body image. While the neurobiology of AN is not completely understood, an imbalance of serotonin and dopamine may explain alterations in satiety and food-related reward/motivation (Frank et al., 2023; Marzola et al., 2015). Knowing that AN has the highest mortality rate of any mental health condition, timely identification and treatment are critical (American Psychiatric Association, 2022; Couturier et al., 2020; Crone et al., 2023; Hornberger et al., 2021).
While Family-Based Treatment (FBT) and weight restoration are mainstays of treatment among children and adolescents, interest exists in evaluating the role of atypical antipsychotics for severe cognitive distortions and obsessive preoccupations that often complicate treatment, interfere with participation in FBT, and/or worsen clinical outcomes (Frank, 2016; Frank et al., 2023, 2017). Among atypical antipsychotics, aripiprazole, olanzapine, quetiapine, and risperidone have been studied in youth with AN. Olanzapine is well-studied, with seven double-blind, randomized, controlled trials evaluating its use in youth or adults with AN (Attia et al., 2019; Bissada et al., 2008; Brambilla et al., 2007b, 2007a; Kafantaris et al., 2011; Mondraty et al., 2005). Results are mixed for weight gain and eating disorder (ED) cognitions, with notable increases in sedation, fasting blood glucose, liver function tests, prolactin, and total cholesterol. In a double-blind, placebo-controlled study, risperidone did not demonstrate improvements in core ED symptoms or time to reach 90% of ideal body weight (Hagman et al., 2011). Quetiapine did not demonstrate a difference in ED symptoms or body mass index (BMI) in the only double-blind, placebo-controlled study (Powers et al., 2012).
While olanzapine is the most widely studied atypical antipsychotic, evidence is mixed regarding its effectiveness, and high rates of side effects may contribute to frequent medication discontinuation (Attia et al., 2011, 2019; Bissada et al., 2008; Brambilla et al., 2007a, 2007b; Kafantaris et al., 2011 Spettigue et al., 2018). Additionally, risperidone and quetiapine have not demonstrated consistent benefit (Hagman et al., 2011; Powers et al., 2012). Aripiprazole has gained interest given its unique mechanism as a dopamine (D2) receptor partial agonist and favorable side effect profile, including lower risk for sedation, metabolic side effects, and elevations in serum prolactin, in comparison to other atypical antipsychotics (Frank, 2016).
Current data to support the use of aripiprazole includes case series and a retrospective review suggesting positive outcomes on obsessive thoughts related to food, body image, fear of eating, weight restoration, and an increase in BMI/BMI percentile (Frank et al., 2017; Tahıllıoğlu et al., 2020; Thorey et al., 2023; Trunko et al., 2011). This study aims to evaluate the role of aripiprazole in children and adolescents with a high number of FABs that interfere with meal completion and progression through treatment.
Methods
Study design
This was a retrospective, matched, cohort study and descriptive analysis of pediatric patients with AN at the eating disorders program (EDP) at Children’s Hospital Colorado in Aurora, Colorado, between January 1, 2018, and December 31, 2023. This study was approved by the Colorado Multiple Institutional Review Board with a waiver of informed consent.
ED treatment and participants
The EDP at Children’s Hospital Colorado is a day treatment program employing a modified version of FBT (i.e., caregivers in charge of food selection), highly structured meal support, multi-family groups, and treatment coordination with interprofessional child and adolescent psychiatry and adolescent medicine teams. Some youth are referred from the community, while others are admitted following stabilization of acute medical concerns. Target body weight is determined by a registered dietitian and the treatment team, based on a variety of clinical factors including review of growth curve trends and weight loss prior to admission. Weight trends are monitored throughout treatment, with caregivers adjusting nutrition to meet target weight goals.
Based on previously evaluated quality improvement data, most youth with anorexia nervosa—restricting type (AN-R) in this program are treated with thiamine, zinc, a multivitamin, and supportive gastrointestinal medications (e.g., constipation, nausea, heartburn treatment) on initial medical admission. Once admitted to the EDP, every patient is evaluated and followed by a psychiatric provider (child psychiatrist or advanced practice provider). Psychotropic medications may be recommended during treatment as an adjunct to FBT and the milieu-based group therapy, which utilizes the Unified Protocol.
Patients were included in this study if they had a diagnosis of AN and were started on aripiprazole for ED cognitions. Patients were excluded if they were started on aripiprazole for other indications than AN (e.g., major depressive disorder) or took aripiprazole for less than 10 days, based on previously published literature suggesting a lack of clinical effect during this time frame (Frank et al., 2017). Those who were treated with aripiprazole were matched 1:2 to those not treated with aripiprazole or another antipsychotic during the ED treatment program (Fig. 1).
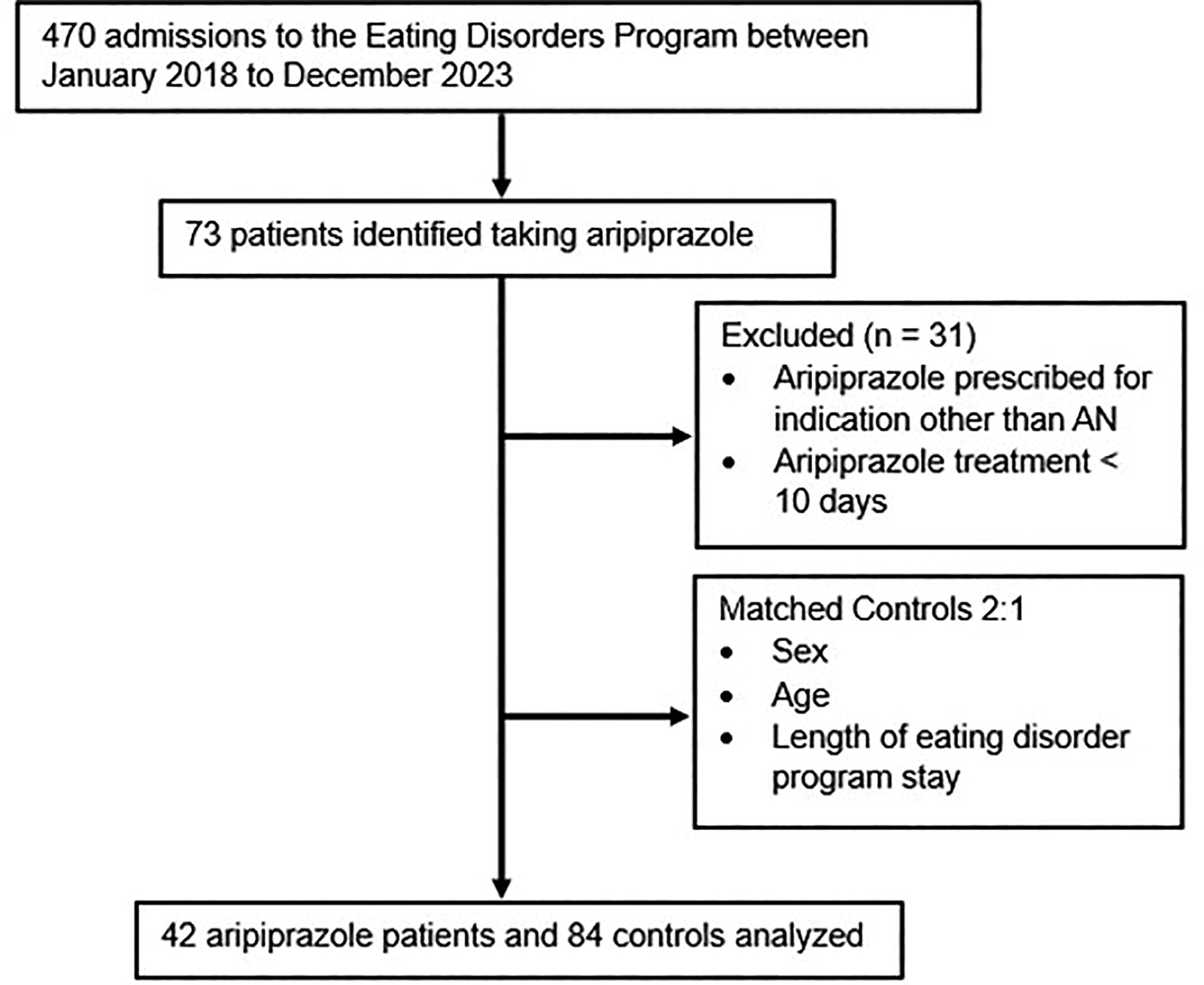
Study flow.
Study outcomes
The primary outcomes were to evaluate the impact of aripiprazole treatment on (1) change in food avoidant behaviors (FABs) and (2) weight gain among youth with AN. FABs were measured using the Ease of Eating Scale (EOES) (Supplementary Fig. S1), an objective measure to evaluate the frequency and severity of 14 specific FABs (e.g., small bites, time between bites, food refusal), assess improvement in ED behaviors, and determine level of support needed (Hagman, 2006). The EOES is used to rate FABs at each meal/snack during EDP, with a range of 0–42 (0 = best; 42 = worst). All EDP staff are trained to score the EOES. The total score is used to determine required level of meal supervision and personalize meal coaching. Data were collected from the electronic health records and represented as a daily mean of FAB scores, to most clearly represent a change over time.
Secondary outcomes were to describe (1) aripiprazole prescribing in this EDP, (2) aripiprazole tolerability in youth with AN, (3) the use of concomitant psychotropic medications in youth, (4) change in BMI in youth prescribed aripiprazole, (5) time to achieve target weight, and (6) change in percent of target body weight.
Data collection
Data collected from the electronic medical record (EMR) included: age, sex, race, ethnicity, primary Diagnostic and Statistical Manual of Mental disorders, 5th edition (DSM-5) diagnoses, medical comorbidities, weight, BMI, percent of target weight, FABs, nutritional supplementation, daily caloric intake, aripiprazole prescribing information, and current psychotropic medications. Primary outcome data, including FABs, weight, and percent target weight, were collected on admission (T0), upon initiation of aripiprazole (T1), halfway between aripiprazole initiation and discharge (T2), and discharge from the program (T3).
Once this information was collected for patients treated with aripiprazole, controls were identified from a randomized list of patients admitted to the EDP during the same time frame. Controls were analyzed for inclusion based on matching criteria of (1) age (±1 year), (2) sex assigned at birth, and (3) length of ED program stay (±2 weeks). The length of treatment was chosen to serve as a proxy for the severity of AN symptoms. Given high rates of psychiatric comorbidities and antidepressant prescribing in our EDP population, these could not be used as matching criteria.
EDP length of stay was included in matching cases to controls after data analysis was performed. After observing that aripiprazole was often initiated at midpoint of the EDP stay, time points for control data collection were chosen to closely represent similar timepoints. This included admission (T0), 50% through treatment (T1), 75% through treatment (T2), and discharge from program (T3).
Statistical analysis
Descriptive statistics were utilized to analyze patient demographics and clinical characteristics. Given the convenience sample of patients, a power calculation was not performed to determine sample size. Primary outcome data were analyzed using a Student’s t-test. Secondary outcome data were analyzed as descriptive data, using a chi-square test, and/or Student’s t-test. Analyses were not controlled for multiplicity and as such, results should be interpreted in a descriptive manner. Analyses were conducted using IBM SPSS Statistics (Version 29, Armonk, NY).
Results
Patients
Seventy-three (16%) patients admitted to the EDP were prescribed aripiprazole during the study period. Among these, 31 were excluded, leaving 42 patients to be analyzed and matched to 84 controls (Fig. 1).
Most patients were Caucasian, females, with a mean age of 14.1 years and a primary DSM-5 diagnosis of AN-R (Table 1). Major depressive disorder (MDD) was more common among those prescribed aripiprazole (73.8% vs. 44%; p = 0.002), with generalized anxiety disorder (GAD), obsessive compulsive disorder (OCD), social anxiety disorder (SAD), and posttraumatic stress disorder (PTSD), equally represented among groups. Malnutrition (83.3% vs. 66.7%; p = 0.05) and bradycardia (40.5% vs. 9.5%; p = 0.00004) were more commonly reported medical conditions among those prescribed aripiprazole. Notably, baseline weight, BMI, and % of target weight at program initiation were similar among both treatment groups. The average length of EDP admission was 8 weeks (Table 1).
Patient Demographic Information
AN-BP, anorexia nervosa binge—purge type; AN-R, anorexia nervosa—restricting type; BMI, body mass index; DSM-5, Diagnostic and Statistical Manual 5th Edition; GAD, generalized anxiety disorder; LOS, length of stay; MDD, major depressive disorder; NGT, nasogastric tube; OCD, obsessive compulsive disorder; PTSD, posttraumatic stress disorder; SAD, social anxiety disorder; SD, standard deviation.
Study outcomes
Aripiprazole was associated with a reduction in FABs with a mean change from T1 to T3 of 3.5 versus 0.9 in the control group (p = 0.026) (Fig. 2). The mean increase in weight from T1 to T3 was greater among those prescribed aripiprazole, with a change of 4.8 kg compared with 3.1 kg among controls (p = 0.00024) (Fig. 3). Patient-specific percentage of target weight increased by 8.9% among those prescribed aripiprazole compared with 6.1% in the control group (p = 0.0016) (Fig. 4). Additionally, 42.9% of patients in the aripiprazole group discharged at or above target weight versus 29.8% of patients in the control group. The mean time to target weight was 41.2 versus 33.5 days for those prescribed aripiprazole and controls, respectively (p = 0.18).

Aripiprazole improves food avoidant behaviors (FABs). FAB scores are scored at each meal/snack during EDP, with a range of 0–40 (0 = best; 42 = worst). Data are represented as a daily average of FAB scores. Mean change in FAB scores from T1 to T3 was 3.5 (aripiprazole) vs. 0.9 (control group) (p = 0.026).
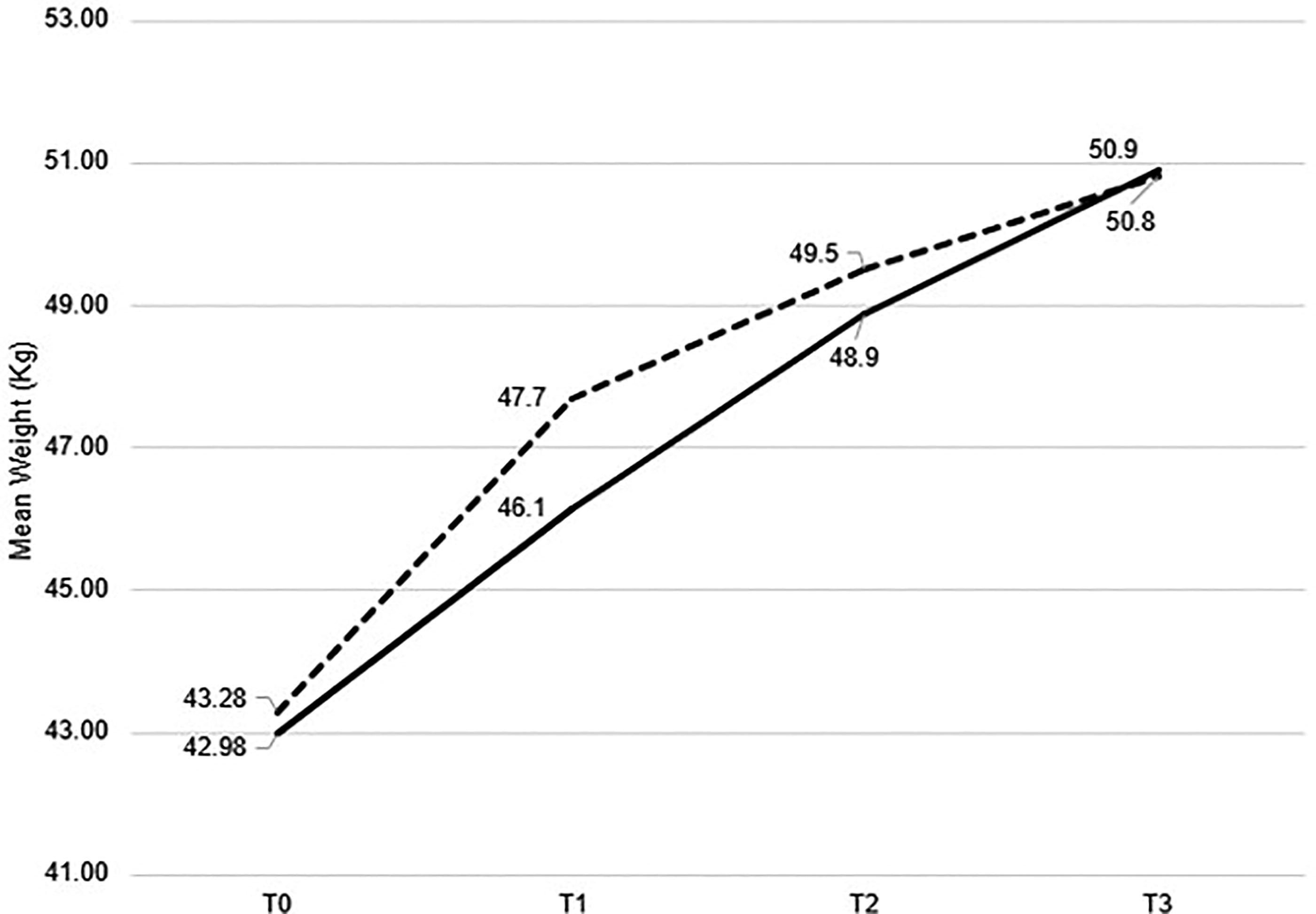
Aripiprazole-associated weight gain. The mean increase in weight from T1 to T3 was greater among those prescribed aripiprazole, with a change of 4.8 kg compared with 3.1 kg among controls (p = 0.00024).

Aripiprazole increases the likelihood of achieving target weight. Patient-specific percentage of target weight increased by 8.9% among those prescribed aripiprazole compared with 6.1% in the control group (p = 0.0016).
Concomitant medications were commonly prescribed, including a multivitamin, zinc, and gastrointestinal support (e.g., PPI/H2RA, simethicone, antinausea) (Table 2). Antidepressants were more often prescribed in those treated with aripiprazole (81% vs. 61.9%; p = 0.03). Additionally, antianxiety medications (e.g., lorazepam or hydroxyzine) were more often prescribed in the aripiprazole group (61.9% vs. 39.3%; p = 0.02).
Secondary Outcomes
AD, antidepressant; GI, gastrointestinal; MVI, multivitamin; SD, standard deviation; SNRI, serotonin norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor.
Aripiprazole prescribing trends are described in Table 3. The mean starting dose was 1.9 mg/day with a mean discharge dose of 2.8 mg/day. Sedation and dizziness were most commonly reported (19%), with the majority (52.4%) not reporting any side effects. Overall, there was a low rate of monitoring for (14.3%) and metabolic labs (e.g., lipid panels) (26.2%). The majority (97.6%) of patients who were prescribed aripiprazole continued on the medication at discharge (Table 3).
Aripiprazole Prescribing
ECG, electrocardiogram; EPS, extrapyramidal symptoms; GI, gastrointestinal; MG, milligrams; SD, standard deviation.
Discussion
Given the high utilization of psychotropic medications in individuals with AN, there is a need for more effective and better-tolerated alternatives. Our study evaluated the impact of aripiprazole in children and adolescents, 11–18 years of age, with AN admitted to an Eating Disorder Partial Hospitalization Program. Aripiprazole was typically initiated at program midpoint among patients with persistent cognitive rigidity, thought distortions, and obsessive preoccupations pertaining to food, and/or high FAB scores, which contributed to challenges in tolerating FBT and/or weight restoration. Starting and discharge doses of aripiprazole were low (≤5 mg/day) and most often administered twice daily to minimize the risk for nausea/vomiting (Findling et al., 2008). This differs significantly from previous studies that describe the use of higher doses (2.5–15 mg/day) (Tahıllıoğlu et al., 2020; Trunko et al., 2011).
Aripiprazole has demonstrated improvements in ED cognitions and weight gain in three case series (Frank, 2016; Tahıllıoğlu et al., 2020; Trunko et al., 2011) and one retrospective case-control study (Frank et al., 2017). The first published case series (N = 4 adolescent females) described improvements in cognitive flexibility and ED preoccupations surrounding weight gain after initiation of aripiprazole (2–5 mg/day). Self-reported improvement in symptoms was described within 1 week of aripiprazole initiation, with total duration of treatment ranging from 3 to 12 months (Frank, 2016). Among a group of nine patients who were previously treated with an antipsychotic, aripiprazole was associated with an increase in medication compliance, improved medication tolerability, and improved ED outcomes. Reasons for prior antipsychotic discontinuation included increased appetite with olanzapine and galactorrhea, sedation, or increased appetite with risperidone (Tahıllıoğlu et al., 2020). Increase in BMI, reductions in comorbid anxiety and depression, and reductions in fear of eating, obsessive ED thoughts, and cognitive rigidity were reported by eight females (15–55 years old) treated with aripiprazole 5–15 mg/day in a third case series (Trunko et al., 2011). Finally, in a retrospective, case-control study, aripiprazole (n = 22) was associated with a greater increase in BMI (6% higher) and BMI percentile (20% higher) compared with controls (n = 84) (Frank et al., 2017). While these studies are limited by small sample sizes and lack of rigorous study methodology, they provide important descriptive information regarding aripiprazole dosing, tolerability, and role in individuals with AN (Thorey et al., 2023).
Neurobiological mechanisms help explain why aripiprazole may be a more effective treatment strategy, compared with in-class alternatives (e.g., olanzapine). Current evidence suggests heightened responsiveness in brain reward circuits and hypersensitive dopamine systems as possible links to AN symptomatology (Frank, 2016; Frank et al., 2023, 2017). As a D2 partial agonist, aripiprazole is thought to decrease and desensitize DA receptors over time, resulting in attenuation of reward system responsiveness, habituation to refeeding and fear extinction, reduced conditioned fear response, and reduced cognitive rigidity and body image distortions. Additionally, D2 partial agonists are thought to improve learning and anxiety among malnourished females who are of low weight and in a low estrogen state (Frank, 2016; Frank et al., 2023, 2019).
While the optimal aripiprazole dosing strategy has not been identified for AN-associated cognitive distortions, obsessive preoccupations, and related behaviors, this and other studies highlight positive results with low doses (Frank, 2016; Frank et al., 2017). At low doses (≤5 mg/day), aripiprazole may predominantly target presynaptic D2 autoreceptors and 5-HT1A receptors, functionally modifying DA release and sensitivity (de Bartolomeis et al., 2015; Tuplin and Holahan, 2017). Whereas, at higher doses, aripiprazole demonstrates high binding affinity for postsynaptic D2 receptors, conferring a higher risk for adverse effects. The impact of this in AN has not been established and warrants further evaluation.
Notably, a diagnosis of MDD and treatment with an antidepressant were more common in those prescribed aripiprazole. Previously published data suggested similar trends, with selective serotonin reuptake inhibitors (SSRIs) frequently co-prescribed for the treatment of MDD predicting higher clinical severity of illness (Couturier et al., 2019; Riquin et al., 2021). Similar to our findings, other studies of aripiprazole in AN found that most adolescents were started on an antidepressant prior to initiation of ED treatment and/or before initiation of aripiprazole (Frank, 2016; Frank et al., 2017; Tahıllıoğlu et al., 2020; Trunko et al., 2011).
While this result might indicate an overall higher burden of mental health symptoms among the aripiprazole group, antidepressants are often prescribed in youth with AN targeting common comorbidities including MDD, GAD, PTSD, and/or OCD (Couturier et al., 2020; Hornberger et al., 2021; Lock, 2019). Notably, current evidence suggests antidepressants do not improve cognitive distortions among individuals with AN, with mixed results on BMI/BMI percentile (Chiu et al., 2023; Frank et al., 2017). While aripiprazole was prescribed for ED cognitions, secondary improvement in MDD cannot be ruled out.
Mean FAB score reductions were greater among those prescribed aripiprazole compared with controls (p = 0.026), suggesting improvement in distress tolerance, cognitive rigidity, thought distortions, and obsessive preoccupations pertaining to food. The mean change of 3.5 points observed in the aripiprazole group indicated improvement in time required to complete a meal or supplement, reduced distress completing a meal, and reduced urges to hide food, cut food into small pieces, or to avoid fear foods, as examples. The use of the EOES and change in observed FABs differs from other studies in which patient report (Frank, 2016; Frank et al., 2017; Trunko et al., 2011) and Clinical Global Impression—Severity scores (Tahıllıoğlu et al., 2020) have been used in previously published literature, highlighting the need for a more standardized, objective approach.
Our study demonstrated a larger mean change in weight among those prescribed aripiprazole compared with controls (4.8 vs. 3.1 kg, p = 0.00024). Additionally, treatment with aripiprazole increased the likelihood of achieving the target weight by program discharge. This is a particularly important finding, as current literature has predominantly described changes in BMI alone. Frank et al. (2017) describe modest improvement in BMI (6% higher at discharge) among those prescribed aripiprazole with clinically relevant improvements in BMI percentile (20% higher at discharge aripiprazole vs. no aripiprazole) among adolescents with AN. While BMI is an important clinical metric, it is well-established that body weight percentiles are more descriptive for children/adolescents as they are standardized to biological sex and age (Hornberger et al., 2021).
In addition to weight gain, time to achieve target weight and likelihood of achieving target weight are important clinical outcomes when considering the use of aripiprazole among adolescents with AN. The course of AN among pediatric patients is variable, with ∼50% achieving full recovery, ∼30% experiencing partial recovery, and ∼20% remaining chronically ill (Harrington et al., 2015; Mysliwiec, 2020). Physiological, psychological, and cognitive impairments associated with AN are significant in early adolescence, given the interruption of critical periods of physical, psychological, and social development (Couturier et al., 2020; Hornberger et al., 2021). While time to achieve target weight did not statistically differ among our cases and controls, youth prescribed aripiprazole were more likely to discharge at target weight (Table 2), highlighting an important functional and developmental outcome.
While rates of patient-reported adverse effects were low, it is important to acknowledge that metabolic and extrapyramidal side effect (EPS) monitoring was not routinely performed (Table 3). These findings may be in part due to ED treatment guidelines not providing unique monitoring recommendations for youth with AN, perceived differences in risk among this patient population, in addition to institution-specific practices (Couturier et al., 2020; Crone et al., 2023; Hornberger et al., 2021). Knowing that youth prescribed atypical antipsychotics are at an increased risk for developing metabolic side effects compared with adults, consideration should be made for routine metabolic monitoring (i.e., hemoglobin A1c and lipid panel) at baseline, 3 months, and 6 months, then annually. Additionally, EPS monitoring should be performed at baseline and every 6 months (Pringsheim et al., 2011).
Our study has several limitations. First, this was a single-center, retrospective, descriptive study that relied on chart review documentation, limiting generalizability. While this study demonstrates improvements in ED behaviors, larger prospective studies are needed to support widespread use of aripiprazole in youth with AN. Second, matching criteria could not account for all confounders in this retrospective review. The exposure time to aripiprazole versus the control group was not evaluated over the exact same time, which could impact results. Comorbidities and concurrent psychotropic medications were challenging criteria to match cases and controls based on the retrospective nature of our study design. Third, given high rates of comorbid MDD and antidepressant prescribing among those prescribed aripiprazole, clinical improvement cannot solely be attributed to the impact of aripiprazole on FABs. Acknowledging this limitation, it is difficult to control for these confounders given high rates of MDD and antidepressant prescribing in the general AN population. Finally, while a validation study is currently in progress, the EOES is not yet a validated tool at the time of article publication. However, the EOES has been used in our EDP since 2006 as a tool to standardize meal observations, determine the level of meal supervision, and identify patient-specific coaching strategies during meals.
More information is needed regarding the safety and efficacy of aripiprazole in children and adolescents with AN. Prospective, randomized, double-blind, placebo-controlled studies are needed to inform the ideal duration of aripiprazole treatment, persistence of aripiprazole effects on cognitive rigidity/distortions regarding food/body image, and long-term tolerability. Ideally, a future study would have patients discontinue other psychotropic medications and evaluate patients over the exact same time period.
While our study used FABs as an objective measure, a standardized rating scale is needed to support clinical decision-making and harmonize data reporting when evaluating atypical antipsychotic response in this patient population. A randomized, double-blind controlled trial is needed to strengthen generalizability and limit confounding impacts on the utility of aripiprazole in AN.
Notwithstanding these limitations, these findings add value to the available literature as the first matched cohort study evaluating the use of aripiprazole in children and adolescents with AN. Utilization of a standardized rating scale to measure improvement in cognitive rigidity and thought distortions provided a standardized, objective assessment of symptom improvement compared with previous studies that primarily relied on subjective patient report (Frank et al., 2017, 2017; Trunko et al., 2011). Finally, to our knowledge, this is one of the largest published reports evaluating the role of aripiprazole in youth with AN and to describe prescribing trends among this unique patient population.
Conclusion
Aripiprazole was associated with a decrease in FABs and an increased likelihood of achieving target weight in an ED treatment program. Additionally, low-dose aripiprazole was well-tolerated. This study provides additional support for the use of aripiprazole, among youth who continue to struggle with meal completion and emotional distress despite engagement in FBT, milieu-based therapy, and use of concomitant medications (e.g., SSRIs). Future studies should evaluate the optimal timing of aripiprazole initiation, dosing strategy, and ideal monitoring protocol.
Clinical Significance
Novel treatment strategies are needed to address core symptoms to improve treatment outcomes in youth with AN. Aripiprazole should be considered for youth with persistent severe cognitive distortions and obsessive preoccupations that interfere with weight restoration and have not improved with engagement in traditional treatment modalities (e.g., FBT).
Footnotes
Acknowledgment
The authors would like to acknowledge Janie Ferren, PharmD, BCPP, for support in reviewing this article.
Authors’ Contributions
I.B. and D.L.S.: Were responsible for conceptualization, methodology, data collection, data curation, statistical analysis, and writing of the manuscript. J.H.: Was responsible for conceptualization, methodology, data curation, and review/editing of the manuscript. K.S. and M.A.S.: Were responsible for conceptualization and review/editing of the manuscript.
Disclosures
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.