
Abstract
Objectives/Background:
Multiple factors influence symptom severity in Attention Deficit/Hyperactivity Disorder (ADHD). We examined four of these: diet, sleep hygiene, exercise, and lighting, in the International Collaborative ADHD Neurofeedback (ICAN) randomized clinical trial, which found large significant improvement with both active neurofeedback and control condition without treatment difference.
Methods:
A total of 142 participants aged 7–10 had breakfast and lunch intake and exercise recorded at each neurofeedback session. Parents completed the Children’s Sleep Habits Questionnaire (CSHQ). Parents and teachers rated inattention on Conners3. Lifestyle changes were correlated with inattention changes.
Results:
At baseline, CSHQ correlated with parent-rated inattention (r = 0.17, p = 0.04), and length of sleep correlated with teacher-rated inattention (r = 0.20, p = 0.03). From baseline to treatment end food group variety (p = 0.029, d = 0.22) and sleep problems (p < 0.0001, d = −0.49) improved significantly, exercise time and protein intake marginally (p = 0.06 − 0.08). Parent-rated inattention improvement correlated with CSHQ improvement (Rho = 0.26, p = 0.002) and marginally with protein intake increase (Rho = 0.18, p = 0.06). The three components of the light-emitting-diode (LED)-induced circadian pathway hypothesis were significant.
Conclusions:
Most measures improved, but few significantly. How much they impact classroom attention remains unclear. Although parent ratings of inattention improvement correlated with sleep problems improvement, composited parent/teacher ratings (primary outcome) did not. The circadian pathway hypothesis associated with LED lighting was supported. These findings warrant further studies examining the role sleep hygiene can play in improving ADHD symptoms. Meanwhile, attention to sleep hygiene seems appropriate in any treatment plan for ADHD.
Introduction
This report explores four lifestyle factors (diet, sleep hygiene, lighting, and exercise) and their relationship to inattentive symptoms of Attention Deficit/Hyperactivity Disorder (ADHD) and improvement thereof in a double-blind randomized controlled trial (RCT) of neurofeedback. One aim is to examine how lifestyle improvements might account for some of the significant large improvements in the control group.
The International Collaborative ADHD Neurofeedback (ICAN) study, a NIMH-funded two-site double-blind RCT (n = 142), found large, significant improvement in the primary outcome, a composite of parent- and teacher-rated inattention, for both neurofeedback and the control treatment (d = 1.5, p = 0.001) without significant difference between them (The Neurofeedback Collaborative Group, 2021). The primary paper noted the need to probe for possible factors explaining the large control-group improvement.
One explaining factor could be lifestyle factors such as diets, sleep characteristics, light exposure, and exercise. These may vary with geography, (Voight, 2024) economy, culture, religion, age, sex, and intervention, as well as between clinical and non-clinical populations. Studies have shown several patterns regarding lifestyle differences between children with ADHD and their typically developing peers.
For example, children with ADHD consume diets with significantly fewer essential nutrients than their peers without ADHD (Martin, 2018, Durá-Travé and Gallinas-Victoriano, 2014). A randomized clinical trial of a multinutrient formula for ADHD found a 54% response rate for multinutrients vs. 18% for placebo (Johnstone et al., 2022). Breakfast is an especially important meal even for children without ADHD, as illustrated by students who started receiving a balanced breakfast with improved essential nutrient intake improving both academic performance and psychosocial functioning (Kleinman et al., 2002). Complete dietary patterns, such as the Mediterranean diet, have lower adherence rates in children with ADHD; on average they consume less fruit, vegetables, whole grains, and fish (rich in omega-3 fatty acids), and skip breakfast more often than children without ADHD (Rios-Hernández et al, 2017). The severity of ADHD symptoms correlated inversely with vegetable and fruit intake (Robinette et al, 2023).
A second lifestyle factor that may play a critical role in ADHD is sleep. Studies comparing sleep in individuals with and without ADHD found ADHD associated with multiple sleep disturbances, including longer sleep onset latency, shorter sleep time, and delayed evening melatonin increase (Coogan and McGowan, 2017; Scarpelli et al., 2019; Becker, 2020; Bondopadhyay et al, 2022). Suppression of melatonin, a sleep-inducing hormone, is associated with greater arousal and delay of sleep onset (Münch et al., 2006).
Sleep-related differences between children with ADHD and their typically developing peers may be explained by comorbid psychiatric disorders, stimulant medication, or simply the manifestation of ADHD symptoms (Bijlenga et al., 2019). ADHD can cause sleep problems intrinsically, sleep problems can cause or exacerbate ADHD symptoms, and the two may interact (Hvolby, 2015). By providing sleep hygiene education, researchers were able to improve ADHD symptomology as well as sleep quality (Peppers, Eisbach, Atkins, et al., 2016). Thus, improving sleep hygiene may benefit ADHD.
Another sleep factor may be the absence of strong zeitgebers (time-givers, rhythmically occurring natural phenomena acting as a cue to regulate circadian rhythms). Variati in natural daylight is the strongest zeitgeber (Roenneberg and Merrow, 2016; LeGates et al. 2014; Wright et al., 2004; Vollebregt et al., 2019). The introduction of electricity-saving light-emitting diodes Paranthesis is for Light Emitting Diode (LED) and increased time spent on smartphones, tablets, etc. has increased exposure to short wavelength blue light (∼450–490 nm) similar to daylight, irrespective of the time of day, thereby weakening variation in daylight as zeitgeber.
Non-natural exposure to blue light after dusk prevents the major circadian clock (suprachiasmatic nucleus) from signaling the pineal gland, thereby delaying the production of the sleep hormone melatonin and subsequent sleep onset (Vollebregt et al., 2019; Bijlenga et al., 2019; Wright and Lack, 2001). Five hours of evening LED short-wavelength light significantly suppressed the evening rise in melatonin, resulting in subsequent daytime sleepiness, which affected the ability to sustain attention (Cajochen et al., 2011). Even 30 minutes of blue light exposure before sleep resulted in high alertness and decreased Electroencephalogram (EEG) slow wave activity (Hvolby, 2015). A pathway that integrates the sleep related findings described above are visualized in Figure 1: Artificial evening blue light exposure postpones sleep onset by delaying melatonin production; delayed sleep onset results in reduced sleep duration by fixed societal demands for morning awakening, which results in (aggravated) ADHD inattention symptoms (Vollebregt et al, 2019) (Arns and Vollebregt, 2019; Bijlenga et al., 2019). This sequence is the circadian pathway (Fig. 1).

Three-component pathway is hypothesized where LED light exposure increases the amount of sleep onset delay, which in turn decreases the amount of sleep, which ultimately leads to worsening of attention. Results from the current data are depicted where each graph corresponds to the part of the pathway in the same-shaded panel. The left graph depicts the percentage of children that had more or less than 50% LED light exposure during the 1.5 hours before bedtime, split for children that at least sometimes required more (yes) than 20 minutes to fall asleep vs. consistently less than 20 minutes (no). The middle graph depicts daily sleep amounts for children split into the same sleep onset delay groups. The right graph depicts the correlation between inattention rated by teachers on the Conners3 scale and the daily sleep amount. LED = light-emitting-diode.
A final lifestyle factor related to ADHD is physical activity. Compared to children without ADHD, those with ADHD are less likely to engage in physical activity regardless of sex and medication use (Kim, Mutyala, Agiovlasitis, et al., 2011). This may be due to the movement skills deficit, and the skill learning gap hypothesis (Harvey et al., 2007). Children with ADHD have a rate of co-occurring developmental coordination disorder up to 50% (Barkley, 1990; Ericsson and Starkes, 2003; Reid, Harvey, Lloyd, et al., 2002, Ho et al. (1996). Moffitt (1990) found that children with ADHD ages 3 to 15 have significantly lower motor development scores on the Bayley Scale (Bayley, 1969) and McCarthy Motor Scale (McCarthy, 1972) than those without ADHD. Patients with ADHD usually struggle with consistent and automatized multi-step skills learning (Wall, 2004; Kowalski and Sherrill, 1992). These deficits may explain why children with ADHD are less drawn to physical activity than their peers and are less successful in, and rewarded by, organized sports. The link between physical activity and ADHD is bidirectional. Not only does childhood ADHD predict later physical inactivity in adolescence, but children with reduced physical activity also tend to exhibit adolescent inattention (Khalife et al., 2014).
Despite a lower likelihood of engaging in physical activity, it may be particularly beneficial for children with ADHD. It increases levels of dopamine (Marques et al., 2021), essential for both motor and cognitive functions; and dopamine is hypothesized to be low in ADHD. Increased dopamine could improve ADHD impulsivity and inattention (Di Ligro et al., 2019). Physical activity can also increase brain-derived neurotrophic factor. This protein, found predominantly in the hippocampus, helps maintain healthy neurons and plasticity necessary for learning and memory (Zhang et al., 2018; Demirci et al., 2024; El-Saied et al., 2024). A meta-analysis suggested that physical activity, especially open-skill activity, could benefit inattention and to some extent hyperactivity/impulsivity (Xie et al., 2021).
In sum, lifestyle factors such as diet, sleep characteristics, light exposure, and exercise may play a role in ADHD symptomatology and possibly treatment. The current study explored how lifestyle factors may explain improvement in a group of ADHD children who received a control treatment designed to be inert. We hypothesized that:
Protein breakfast consumption, dietary balance, good sleep hygiene, amount of exercise, and proportion of non-LED lighting would correlate negatively at baseline with inattention severity. The better these lifestyle factors, the lower the inattention severity. Because of the psychoeducation about the importance of diet and the inquiring about diet, sleep, and exercise at each treatment visit, breakfast protein consumption at breakfast, dietary balance, and sleep hygiene would improve over the course of treatment. Due to the expected relationship between ADHD symptomatology and lifestyle factors, we expected a positive correlation between improvement of inattentive symptoms and improvement in breakfast protein consumption, dietary balance, sleep hygiene, and exercise. We hypothesized that the circadian pathway would be supported by significant correlations between the amount of LED lighting and sleep onset delay (SOD), between sleep delay and sleep length, and between sleep length and teacher inattention ratings.
Methods
Design and participants
We first investigated the baseline relationship of inattention ratings with protein breakfast consumption, dietary balance, sleep hygiene, the proportion of LED lighting, and the amount of exercise. Second, baseline lifestyle variables were related to changes in inattention ratings from baseline to treatment end, regardless of treatment assignment. Third, we determined how effective a nutritional brochure, coupled with repeated attention to food intake, was in changing nutritional consumption in children with ADHD by comparing dietary measures before and after treatment. Similarly, the change before to after treatment was investigated for sleep hygiene and exercise. Finally, we explored the relationships of treatment-related changes in exercise, dietary, and sleep measures with changes in inattention ratings.
Data were acquired from the ICAN RCT of neurofeedback in children aged 7–10 with inattentive or combined-type ADHD. Parents gave informed permission and children informed assent using forms and procedures approved by the Ohio State University institutional review board.
Children (n = 142) diagnosed with Diagnostic and Statistical Manual (DSM) −5 ADHD inattentive presentation or combined presentation (based on structured clinical interviews by doctoral-level clinicians) and with T scores 65 or higher on inattentive items of the Conners3 scale rated by both parents and teachers were randomized to 38 sessions of neurofeedback or an identical-appearing control condition in which reinforcement was based on a pre-recorded EEG rather than the child’s own EEG. The neurofeedback consisted of downtraining theta power and uptraining beta power, theta:beta ratio neurofeedback. Regardless of the treatment group, all participants received one-to-one coaching at each session, inhibition of rewards during muscle artifact, and dietary instruction. Nutrition, sleep, and exercise were monitored at each visit, implicitly underscoring their importance.
For study inclusion, children had to have normal-range Vitamin D levels, and randomization was delayed for supplementation if necessary. They also needed a theta-beta power ratio ≥4.5 at EEG electrodes Cz or Fz, based on Monastra et al. (Monastra et al., 1999). Exclusion criteria included the presence of a comorbid disorder requiring psychoactive medication other than stimulants, a medical disorder requiring systemic chronic medication with confounding psychoactive effects, convergence insufficiency, sleep apnea, restless legs syndrome, IQ <80, or an antipsychotic in the 6 months prior to baseline, fluoxetine in the 4 weeks prior, atomoxetine in the 3 weeks prior, or other psychiatric medication (except stimulants) in the 2 weeks prior to baseline.
Measures
Inattention
Both primary caregivers and teachers completed the Conners 3rd Edition rating scale (C-3: P and C-3: T, Conners, 2008) at baseline, mid-treatment, and treatment end, to measure inattentive symptoms. The primary outcome was the composite parent/teacher DSM-5 inattentiveness subscale. However, since teachers observed the children the most after breakfast and after recess exercise, and parents saw children on waking and at bedtime, separate parent and teacher inattentiveness ratings were also analyzed. The 43 children who were taking stimulants for their ADHD had to discontinue medication for 5 days, including at least three school days, before each assessment. Thus, all inattention ratings were unmedicated.
Diet
At baseline, participants and their parents were given a nutritional “Eat Smart’ brochure emphasizing the importance of protein for breakfast. The brochure gave examples of protein-dense foods such as meat, cheese, milk, eggs, peanut butter, and nuts. These determined which foods counted as “protein-dense” when coding data from the session form. Participants were asked what they had eaten for breakfast, lunch, and afternoon snack and these were recorded at each treatment session. Three treatment sessions were averaged for each of the nutrition assessments: sessions 1–3 for baseline, sessions 17–19 for mid-treatment, and sessions 37–39 for treatment end. The average number of protein-dense breakfast foods consumed each day, number of days out of three with at least one protein-dense food for breakfast, and number of food groups out of four (grains, meat/proteins, dairy, and fruits/vegetables) they ate over the course of breakfast, lunch, and snack each day were calculated at baseline, mid-treatment, and end of treatment.
Sleep
Parents filled out the Children’s Sleep Habits Questionnaire ([CSHQ]; Owens, Spirito, McGuinn, 2000) at baseline, mid-treatment, and treatment end, the measure of sleep hygiene. The CSHQ was designed for children 4–12 years old. It includes 48 items rated by caregivers. The Total Sleep Disturbance Score has 33 items. In addition, raters are asked the total hours their child slept in a day and the total number of minutes awake after sleep onset. SOD was operationalized as the SOD subscale from the CSHQ: Falling asleep within 20 minutes was scored with usually, sometimes, or never/rarely; these were dichotomized as usually = no sleep delay; sometimes and never/rarely = sleep delay.
Light exposure
During the screening visit, the demographics form asked the percentage of time the child is exposed to (1) ordinary light bulb (halogen/incandescent light), and (2) energy saving light-emitting diode (LED) lights during the 1.5 hours before bedtime. The percentage of LED lights was used for analyses.
Exercise
At each treatment session (which occurred late afternoon or early evening) how much self-reported exercise the child had that day was recorded. The minutes of exercise were extracted from the session form and averaged for three sessions at baseline, three at mid-treatment, and three at treatment end, similar to diet variables.
Statistical analysis
Because the focus of this study is on lifestyle effects regardless of treatment and because between-treatment analyses have already been reported as nonsignificant, all analyses are on the whole sample. Statistical tests used SAS 94 and IBM SPSS Statistics for Macintosh, Version 24 ((IBM, Armonk, NY). The significance level was set at p < 0.05 for these exploratory analyses and effect sizes are reported as Cohens d for comparison between assessments and r or rho for correlations.
First, Spearman correlations were calculated to explore the relationship that diet, (a balanced diet [number of food groups] and protein consumption), sleep (total sleep problems on CSHQ), light exposure (% LED lighting before bedtime), and exercise (average minutes/day) at baseline had with baseline inattentiveness and with the change in inattentiveness scores. Next, one-sided paired t-tests determined if significant changes occurred in diet, exercise, or sleep from baseline to the end of treatment. Finally, changes in diet, sleep, and exercise from baseline to treatment end were related to changes in inattention ratings.
The proposed circadian pathway was tested by checking whether the component associations were significant. Data from participants for which data for all path components were available were used. Although these analyses do not definitely indicate the direction of relationships, results from previous studies make the direction indicated by the arrows in Figure 1 most likely.
Results
Baseline correlations of lifestyle factors with inattention
Table 1 shows correlations of inattention ratings with the lifestyle measures at baseline (Table 1).
Correlations of Baseline Lifestyle Measures with Baseline Inattentive Symptoms (Primary Outcome): Spearman’s Rho
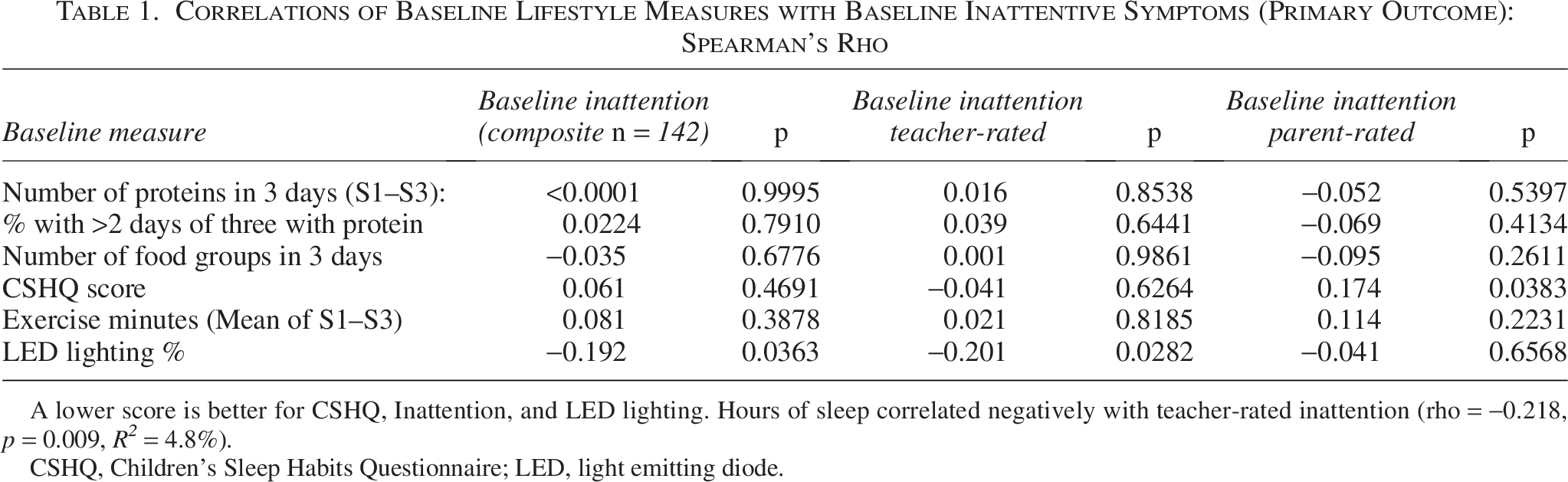
A lower score is better for CSHQ, Inattention, and LED lighting. Hours of sleep correlated negatively with teacher-rated inattention (rho = −0.218, p = 0.009, R2 = 4.8%).
CSHQ, Children’s Sleep Habits Questionnaire; LED, light emitting diode.
CSHQ total sleep problems score correlated significantly with parent-rated inattention (rho = 0.174, p = 0.038) and hours of sleep with teacher-rated intention (rho = −0.218, p = 0.009), both in the expected direction, but LED lighting with inattention in the direction opposite of expected that is, the worse the CSHQ, the worse the inattention, and the more sleep, the less the inattention, but the greater the percentage of LED lighting, the less the inattention. Other correlations were nonsignificant.
Changes by treatment end
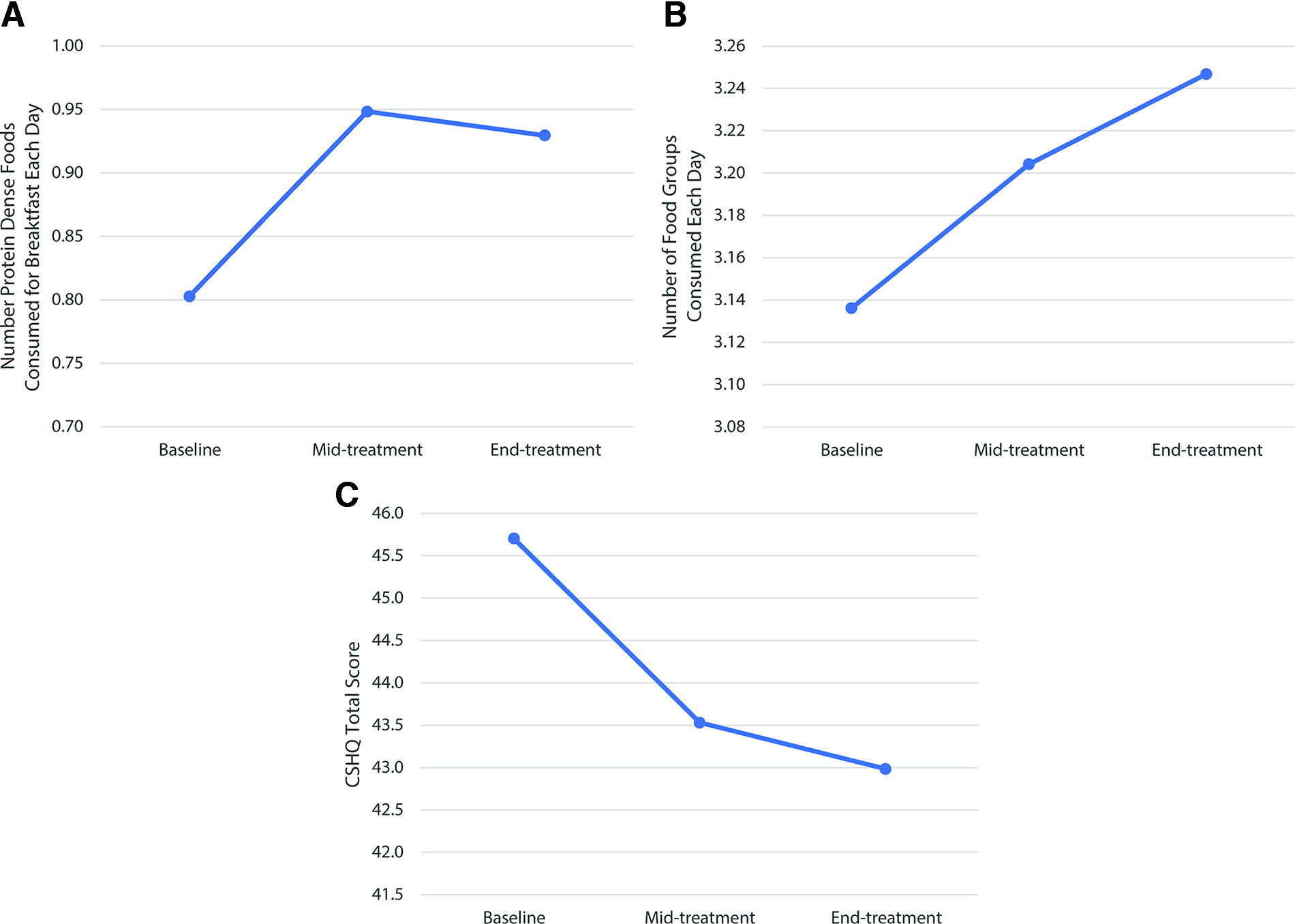
Table 2 and Figure 2 show changes in the lifestyle measures. All showed trends of improvement, but only CSHQ (p = 0.0001, d = 0.49) and number of food groups p = 0.029, d = 0.216) were significant (Table 2), (Fig. 2).
Change Over Time: Baseline and Treated Scores on Lifestyle Measures
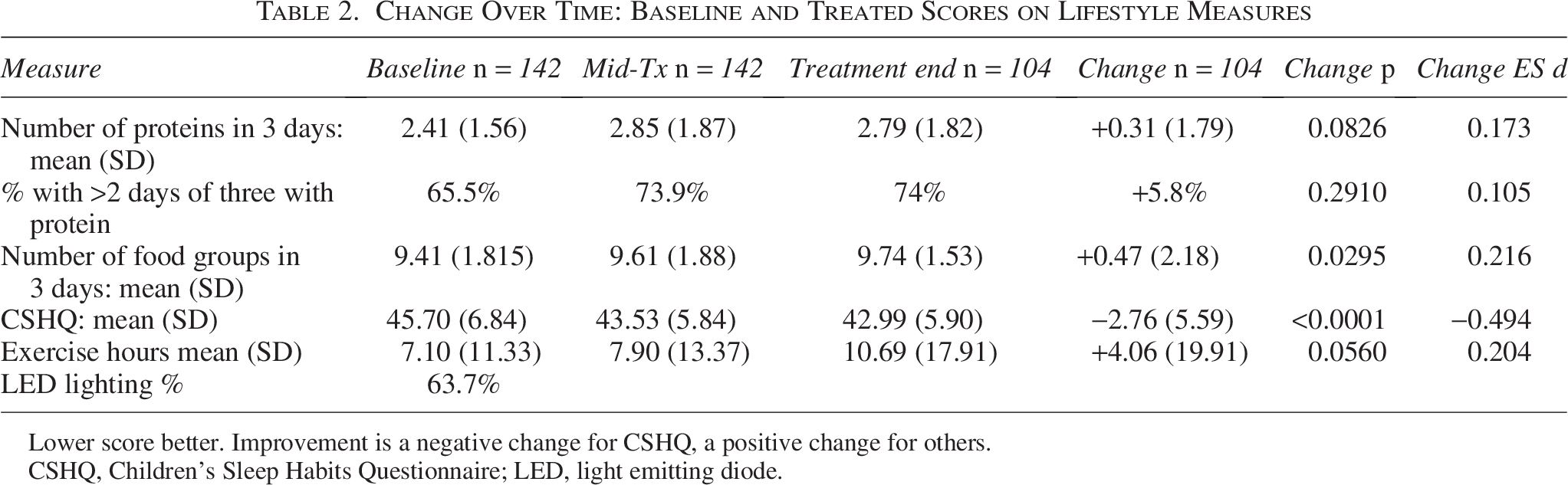
Lower score better. Improvement is a negative change for CSHQ, a positive change for others.
CSHQ, Children’s Sleep Habits Questionnaire; LED, light emitting diode.
Dietary improvement
The variety of food groups consumed increased significantly throughout the study. The total number of food groups (out of 4) consumed in a three-day sample significantly increased from 3.14 to 3.25, suggesting a slightly more balanced diet by the end of the study. The proportion who consumed an average of at least three food groups per day over the three-day sample increased from 71.1% at baseline to 77.5% at mid-treatment and 77.0% at the end of treatment. Overall, 45.2% of participants increased while 31.7% decreased the variety of food groups they consumed. Over the course of treatment, 44.2% of participants increased, while 28.9% decreased the number of protein-dense foods they consumed, and 37.5% increased while 19% decreased the number of days they consumed a protein-dense food (marginal trends).
Sleep Improvement. Figure 2 and Table 2 also demonstrate the improvement in the CSHQ total score from baseline to the end of treatment (a lower score indicates fewer problems, hence better sleep). The mean problem score decreased from 45.7 at baseline to 43.5 by mid-treatment and 43.0 by the end of treatment (p < 0.0005).
Lifestyle factor changes and inattentiveness changes
Table 3 shows the Spearman correlations between changes in lifestyle measures and changes in Conners3 inattentiveness ratings from baseline to the end of treatment (Table 3). Although the tendencies were generally in the expected direction, the only significant correlation of change scores was between CSHQ and parent-rated inattention changes (r = −0.264, p = 0.002). The end-of-treatment CSHQ scores also correlated with parent-rated inattention improvement (r = 0.17, p < 0.05) and end-of-treatment inattentiveness (r = −0.26, p < 0.01), In contrast, teacher inattentiveness ratings did not show any relationship (rho = −0.003, p = 0.976).
Correlations of Inattention Improvement with Change in Lifestyle Measures: Spearman’s Rho

Inattention = caregiver ratings of inattention on Conners3, lower score better. For CSHQ and inattention, improvement has a minus number; for diet and exercise, improvement has a positive number. Therefore positive correlations for CHSQ and negative correlations for diet and exercise are in the expected direction.
CSHQ, Children’s Sleep Habits Questionnaire; LED, light emitting diode.
Causality between sleep hygiene and inattentiveness could not be determined by correlating change in one from baseline to mid-treatment with change in the other from mid-treatment to treatment end because 88.7% of improvement in inattention ratings and 79.9% of improvement in CSHQ occurred by mid-treatment.
Circadian pathway
Data to test all components of the circadian pathway hypothesis proposed by Arns and Vollebregt (2019) were available for 114 children. The percentage of LED light children were exposed to the 1.5 hours before bedtime was not normally distributed, requiring a non-parametric approach to test the difference in LED between children that at least sometimes needed longer than 20 minutes to fall asleep (SOD, yes) vs. children that did not (no). Children with SOD had a significantly higher exposure to LED (71.78 ± 35.50%) than children without SOD (58.38 ± 34.78%) (Independent-Samples Mann–Whitney U test, U = 2089, p = 0.004, d = 0.381). For visual purposes, LED is displayed as a dichotomous variable in Figure 1 (LED exposure <50 vs. ≥50%). Those exposed >50% to LED light were more likely to have SOD with an odds ratio of 2.28 (95% confidence interval [CI]: 1.037–5.013) and relative risk of 1.63 (95% CI: 0.996–2.670) (Fig. 1, left gray shaded panel). Next, the number of hours children slept was compared between having SOD or not, where SOD was thought to diminish the amount of received sleep. Sleep amount was also distributed non-normally, requiring a non-parametric approach. As expected, children with SOD slept significantly less (9.49 ± 0.88 hours) than children without SOD (9.82 ± 0.81 hours) (U = 1190.5, p = 0.019, d = 0.390) (Fig. 1, middle light-gray shaded panel). Finally, the negative impact of low sleep duration on attentional daily functioning was tested by non-parametric correlational analysis. Children with the least amount of sleep indeed had the highest teacher-rated inattention (Spearman’s rho = −0.184, p = 0.050, R2 = 3.4%) (Fig. 1, right non-shaded panel). A sensitivity analysis correlating teacher-rated inattention with sleep duration on the full available sample of n = 142 (rather than only n = 114 for which data for the entire circadian pathway were available) strengthened the findings (Spearman’s rho = −0.218, p = 0.009, R2 = 4.8%). The correlation for parent-rated inattention was non-significant.
Discussion
These analyses cast a wide net exploring lifestyle effects on baseline inattentiveness severity, changes in lifestyle factors over the course of 38 treatment sessions, and effects on changes in inattentiveness severity, with four factors considered: nutrition, sleep, lighting, and exercise.
At baseline, inattentiveness severity correlated with CSHQ total sleep problems (parent-rated inattention) and percent LED lighting (teacher-rated and composite inattention) but not significantly with the other lifestyle factors.
The variety of food groups improved significantly and protein consumption marginally after children and parents were given a nutritional brochure and their diet was monitored at each visit. Thus, further investigation is warranted into the efficacy of a nutritional brochure and repeated inquiry about consumption in changing dietary patterns in children with ADHD.
However, the dietary improvements did not correlate significantly with improvements in inattentive symptoms. The only related significant finding was a weak correlation between the end-of-treatment variety of food groups and improved attentiveness. These correlations indicate that the significantly improved attention in the control group is not mainly due to nutritional improvement. This does not, however, diminish the importance of a balanced diet for children with ADHD.
At baseline, the amount of nightly sleep correlated negatively with teacher-rated inattentiveness. However, the amount of sleep each night remained roughly the same throughout the course of treatment as reflected in reports at each treatment. Nevertheless, the CSHQ total problems showed significant improvement over the course of treatment, reflecting improved overall sleep hygiene. Whether the improved sleep resulted directly from the attention study staff paid to its importance cannot be determined from the available data.
Sleep improvement correlated significantly with parent-rated but not teacher-rated inattention improvement, possibly reflecting differences in caregiver perceptions and/or child behavior between the two settings. However, since the parents filled out both the parent Conners and the CSHQ, we cannot rule out a source factor as a possible explanation. Most of the change in both sleep hygiene and inattentive symptoms occurred within the first 19 sessions of treatment, and future studies may examine this time frame in more detail by administering the CSHQ and Conners more frequently to investigate the direction of causality. An interesting paradox is that at baseline teacher-rated inattention correlated negatively with the amount of sleep but change in teacher-rated inattention did not correlate with CSHQ sleep improvement, though parent-rated inattention did. This may have resulted from the CSHQ total reflecting things other than the amount of sleep.
The circadian pathway hypothesis about LED lighting was upheld if we accept the causality direction from previous publications. It appears that blue-light-emitting lighting (and screens) delay sleep onset, shorten sleep time, and shortened sleep time impairs daytime attention during school hours. Because the measure of lighting was only available at baseline, we could not track change over time. Since these analyses, a recent review (Bauducco et al, 2024) emphasizes the growing importance of cell phones and posits a vicious cycle between disrupted sleep and cell phones in the bedroom (apparently replacing bedtime reading). The revised hypothesis notes that cell phones, in addition to their blue-light emission, may continue disruptive social media and other pings through the night The authors advise keeping phones out of bedrooms. Future studies, in addition to blue light exposure, should also focus on quantifying such sleep-disruptive effects.
Exercise was not emphasized in the ICAN treatment package other than to record the amount for that day at each treatment session. Nevertheless, it did improve over the course of treatment by a marginal trend (p = 0.056). Perhaps simply being asked caused the child and parent to give it more consideration. However, exercise improvement did not correlate with inattention improvement, possibly a power problem because so many children reported no exercise.
Limitations: These exploratory analyses had several limitations. An important limitation is a fact that the lifestyle factors were assessed by self-report and parent observation/ratings, not by objective measures such as actometers, direct measurement of light exposure or food eaten, timing of physical activity, or food frequency questionnaires. Also, participants did not record how much of each food they ate, simply which foods they ate, so logged data was non-quantitative. Data from dinner and any evening snacks were not collected since they did not occur before the neurofeedback sessions. Any participants who were deemed to not be improving after 19 treatment sessions were dropped from treatment per protocol and received alternative therapy. These participants (n = 38) no longer provided food or exercise data and had no data for the three-day sample at the end of treatment. Sleep data were reported by parents and sleep time was estimated based on when the child got into and out of bed and how long the parent thought it took them to fall asleep, without explicit observation of actual sleep. The causal direction in the circadian pathway analysis was assumed from previous publications, not established in this data set. Future RCTs should consider more objective measures of lifestyle.
Overall, with the exception of sleep data, these analyses do not support lifestyle improvements as the main explanation for the highly significant improvement of inattention in the ICAN neurofeedback RCT control group, who did not receive deliberate real-time brain wave training. Nevertheless, the small improvements coupled with favorable safety and cost make attention to diet and exercise in addition to sleep reasonable components of treatment plans for ADHD. Sleep quality and quantity did emerge as a significant possible explanation and possible target of intervention. Other possible explanations are being explored, as well as a deeper dive into the CSHQ data. Meanwhile, one clinical implication, in view of the significant circadian pathway findings and significant CSHQ effect, could be to limit the amount of LED lighting in the evening and keep blue-light-emitting devices out of the bedroom.
Authors’ Contributions
All co-authors reviewed drafts and provided edits to the manuscript. X.P., M.Y., and M.A.V. ran analyses, created tables, and drafted the method and results sections. K.H., I.E.H., M.E.R.-R., C.K., M.A., and J.H. contributed paragraphs to the introduction and discussion, L.E.A. and R.DB. oversaw the manuscript, supervised Kyle Hendrix and Michelle Roley-Roberts during earlier stages of the writing process, and drafted most of the discussion.
Footnotes
Acknowledgment
The authors acknowledge Behnoosh Shahsavaripoor’s and Ashauna Steven’s assistance with the article preparation.
Funding Information
The source of data for this report is from the International Collaborative ADHD Neurofeedback (ICAN) study, a two-site randomized controlled trial funded by NIMH grant R01 MH 100144 to Ohio State University ([OSU]; L.E.A.) with subaward to University of North Carolina at Asheville (R.deB.), by OSU College of Medicine Endowment, and by the Center for Clinical and Translational Science at The OSU (ARRA Pilot Project UL1 RR025755 project 60023888).
Clinical Significance
The American Psychiatric Association (APA) Presidential theme this year is lifestyle factors in psychiatric disorders. Diet/nutrition, sleep, and physical exercise are important issues in most psychiatric disorders, including Attention Deficit/Hyperactivity Disorder (ADHD), the most prevalent child/adolescent disorder. This study used data from a randomized controlled trial of neurofeedback for ADHD to examine how much diet, sleep, lighting, and exercise contributed to the very large improvement in the control group. A significant correlation of sleep improvement with parent-rated inattention improvement (Rho = 0.26, p = 0.002) suggests that clinicians should make sleep hygiene part of any ADHD treatment plan.
Disclosures
L.E.A. has received research funding from Axial, Forest, Lilly, Noven, Otsuka, Shire, Supernus, Roche, Yamo, and YoungLiving (as well as NIH and Autism Speaks), has consulted with Pfizer, Tris Pharma, and Waypoint, and has been on advisory boards for Arbor, Ironshore, Otsuka, Pfizer, Roche, Seaside Therapeutics, Shire. C.K. is the founder and CEO of APEd, Napa California. Dr. deBeus has a private clinic offering neurofeedback. J.H. has received research funding from Forest, Supernus, Roche/Genentech, Otsuka, Axial, YAMO, Young Living, National Institute of Mental Health (NIMH), Autism Speaks, and has consulted with Impel Neuropharma and served on the advisory board for Yamo Pharmaceuticals. M.E.R.-R. has received research funding from NICHD, West Virginia University Foundation Fund and Community Engaged Research Fund, Nebraska Total Care Community Initiative Capacity Building Pathways Program, and UnitedHealthcare Community Initiative Capacity Building Pathways Program. K.H., X.L.P., M.A., I.E.H., and M.A.V. have no disclosures or conflicts of interest to report.