
Abstract
Objectives:
Investigators and government agencies have expressed concern about the high percentage of foster youth who receive psychotropic medication, the number of psychotropic medications prescribed, and the extended duration for which many foster youth receive psychotropic medication. One contributor to the duration of medication use is the absence of clear guidelines for de-prescribing in pediatric psychiatry. The present study evaluated whether medication review letters crafted by medical professionals and sent to caregivers prompted a reduction in psychotropic medication in foster youth.
Methods:
The caretaker or caseworker of 52 foster children, 38 males, under 16 years of age, who received medication through Medicaid, was sent a letter assessing the use of psychotropic medication and identifying areas of concern. Recipients were encouraged to discuss the letter with the child’s prescriber. These children had been referred to a university-affiliated organization that provided behavioral interventions to other children, but the children in the present study did not receive behavioral interventions from the organization. The use of psychotropic medication was assessed for 18 months before and 24 months after the letter was sent. The control group had comparable demographics and medication-use parameters. The trajectories of medication count before and after a letter (for cases) or a “phantom” letter (for controls) was sent were compared.
Results:
The medication review letter precipitated a decrease in medication count over the year after the letter was sent for 9- to 12-year-olds. For 13- to 16-year-olds, an increasing trend in medication use was halted. No effect was seen for 5- to 8-year-olds. No such changes occurred in the control groups.
Conclusions:
A single personalized letter, tailored to a child’s medication list, was provided to caregivers to share with prescribers. This decreased or halted an increase in the use of psychotropic medications for children in foster care who were 9 years old or older.
Introduction
Psychotropic medications are routinely used in the United States to treat emotional and behavioral issues seen in children and adolescents in foster care. Overall, children in foster care are more likely to be prescribed psychotropic medication (Keefe et al., 2023). Among children in foster care, 8%–35% received psychotropic medication (Leslie et al., 2010, 2011) (Keefe et al., 2023). In one of the first studies to highlight this practice, Zito et al. (2008) found that of the foster-care youth receiving any psychotropic medication, 72.5% received two or more such medications. The odds ratio for receiving psychotropic medication was about seven times higher for children in foster care than for controls receiving medication through Medicaid. The prevalence is even higher for children in treatment foster care, where nearly 60% of a sample of 240 children and adolescents had received psychotropic medication in the previous 2 months (Brenner et al., 2014). In that sample, children receiving any psychotropic medication were more likely to have seen some form of treatment service (case management, social or school services outpatient treatment, or a psychiatric visit), than children receiving no medication, perhaps reflecting a greater severity of cases that led to the use of such services. Children with a recent psychiatric visit, however, were less likely to experience “Questionable Polypharmacy” 1 than those merely receiving two or more medications.
Variables such as male sex, older age, and behavioral problems have been linked to increased psychotropic medication usage (Leslie et al., 2011), an observation also noted by Warner et al. (2014). These studies indicate that psychotropic medication usage by foster children and adolescents is common, especially among children with problem behaviors severe enough to necessitate treatment. Moreover, once a regimen of psychotropic medication has been prescribed, the rate of deprescribing (reducing the dose or removing a medication if it is determined to be unsafe or no longer needed) is slow, especially for antipsychotics and psychomotor stimulants (Palmer et al., 2023).
Oversight systems have been implemented to keep pace with the use of psychotropics. The Child and Family Services Improvement and Innovation Act, 20 U.S.C. § 112–134 (2011) mandated the monitoring of psychotropic medication use in foster care systems. Since the passage of this legislation in the United States, nearly every state has implemented one or more oversight processes (e.g., Mackie et al., 2017). In a review, Mackie et al. (2021) reported several approaches to reducing the use of psychotropic medication, including peer reviews, letters, and prior authorization processes. In one example, consulting meetings between a prescriber and a child and adolescent psychiatrist yielded significant decreases in polypharmacy, off-label prescribing, and related problems during the 1-year study period for children in a state Medicaid system (Perry et al., 2019). The study was time-limited and resource-intensive, so its sustainability is uncertain. In another, a set of safety standards for attention deficit hyperactivity disorder (ADHD) medications was developed. Pharmacies did not fill first-time prescriptions that failed to meet these standards but refills were allowed while a review of medical records was undertaken. Consultation with the prescriber occurred upon request.
Knowledgeable caregivers are an important component of both prescribing and deprescribing. Although many caregivers reported that they understood why their child received psychotropic medication, only one-third of the 44 caregivers felt knowledgeable about potential problems with long-term use of psychotropic medication (McLaren et al., 2021). This might be related to McLaren et al.’s observation that approximately half of the caregivers stopped providing their child psychotropic medication sooner than recommended by their prescriber. This practice raises problems and suggests that informed deprescribing of psychotropic medication should involve a shared decision-making process with the caregivers.
The present study was designed to determine the impact of a single, individualized letter sent to a guardian with encouragement to share it with the prescriber. The study differs from previous studies in several ways. The letters were requested by individuals with knowledge of the case, such as caseworkers or caregivers. The letters were sent to caregivers and were coupled with suggestions about how to speak with prescribers. They were tailored to the client’s specific prescription regimens, included all psychotropic medications, and were carefully written to be respectful, collegial, and supportive. The letters frequently suggested reconsideration of some psychotropic medications used and were written by a child and adolescent psychiatrist or psychiatric mental health nurse practitioner associated with a state-funded, university-affiliated team called the Alabama Psychiatric Medication Review Team (APMRT) (Luna et al., 2018).
The letters’ impact on the time course of the number of psychotropic medications was tracked using data provided by Medicaid. These values were compared with those of propensity-matched children receiving Medicaid support for psychotropic medication (Austin, 2011). A key feature of the control group is that they were yoked to the cases (those receiving a letter) based on when, relative to commencing psychotropic medication use through Medicaid, the letters were sent. Thus, a trajectory across months before and after the cases received the letter could be compared to a similar time span before and after a phantom letter for the controls.
Methods
Cases and matched controls
The APMRT received referrals for medication reviews from county caseworkers, foster parents, or advocates who submitted a request for medication review via the team’s website or a direct request from the State Department of Human Resources. The APMRT provides behavioral interventions and medication reviews to foster children and their families but the participants in this study received only the medication review; no behavioral interventions were delivered.
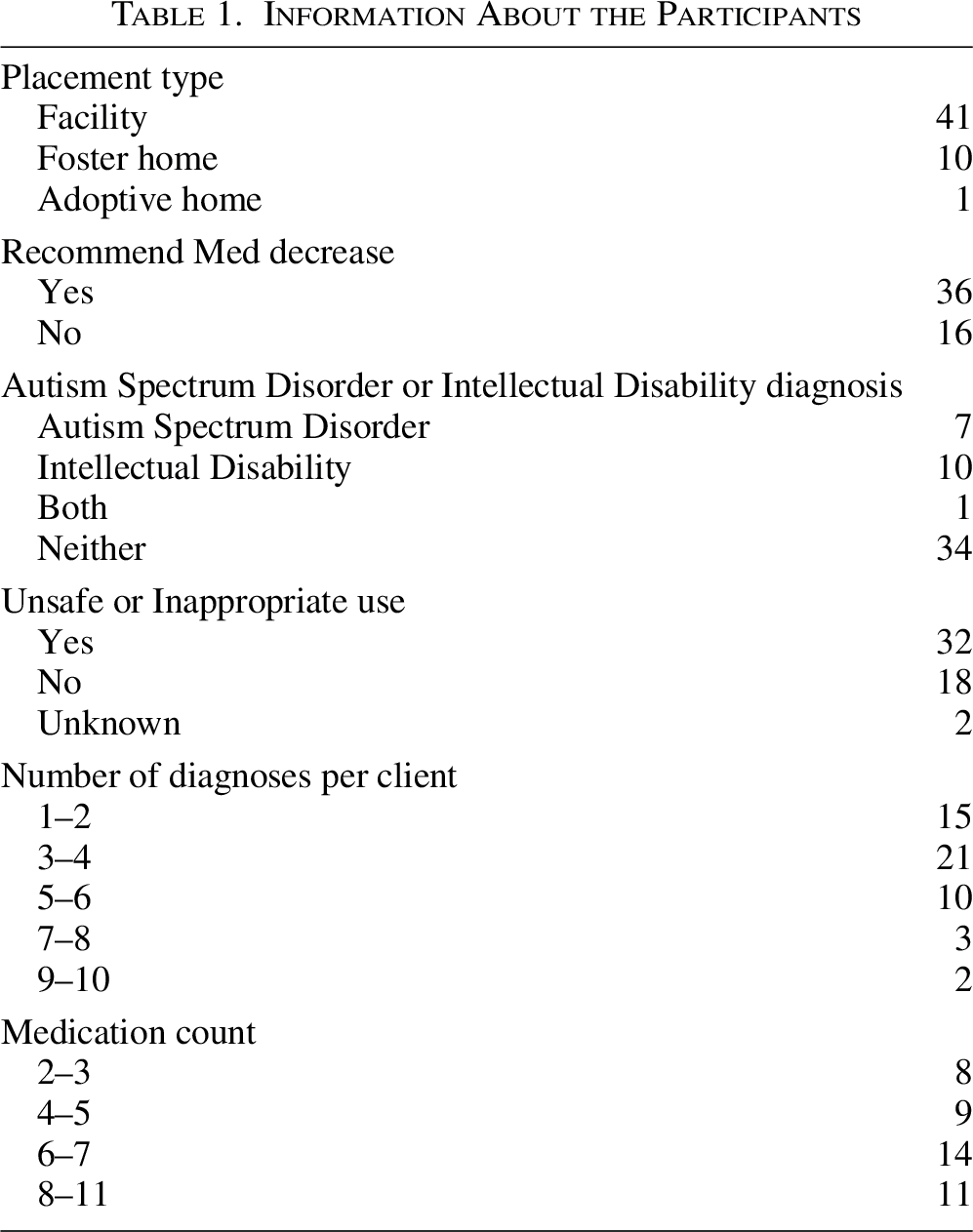
Table 1 contains additional information about the clients in this study. Most were placed in a residential facility, were prescribed six or more medications, received a recommendation for a medication reduction, received prescriptions that were unsafe (usually because of interactions with other medications) or received medications inappropriate to their diagnosis. Seventeen cases had a diagnosis of autism spectrum disorder or intellectual disability. The correlation between the number of diagnoses and the medication count was 0.18 (confidence intervals, −0.10, 0.44) so this correlation was not distinguishable from zero.
Information About the Participants
There were 28 separate prescribers for the 52 referrals. Two prescribers were represented four times, one was represented three times, four were represented two times, and 18 were represented once. For 15 cases the prescriber was unknown.
Figure 1 shows the percentage of clients with different diagnoses. The most common diagnosis was ADHD, seen in 71% (37 cases) of the clients. Diagnoses seen only one time in this group and classified as “other” were learning disability, reading disorder, math disorder, sibling relational disorder, schizophrenia, dysthymia, avoidant personality, cannabis use disorder, sleep disorder, and schizoaffective disorder.
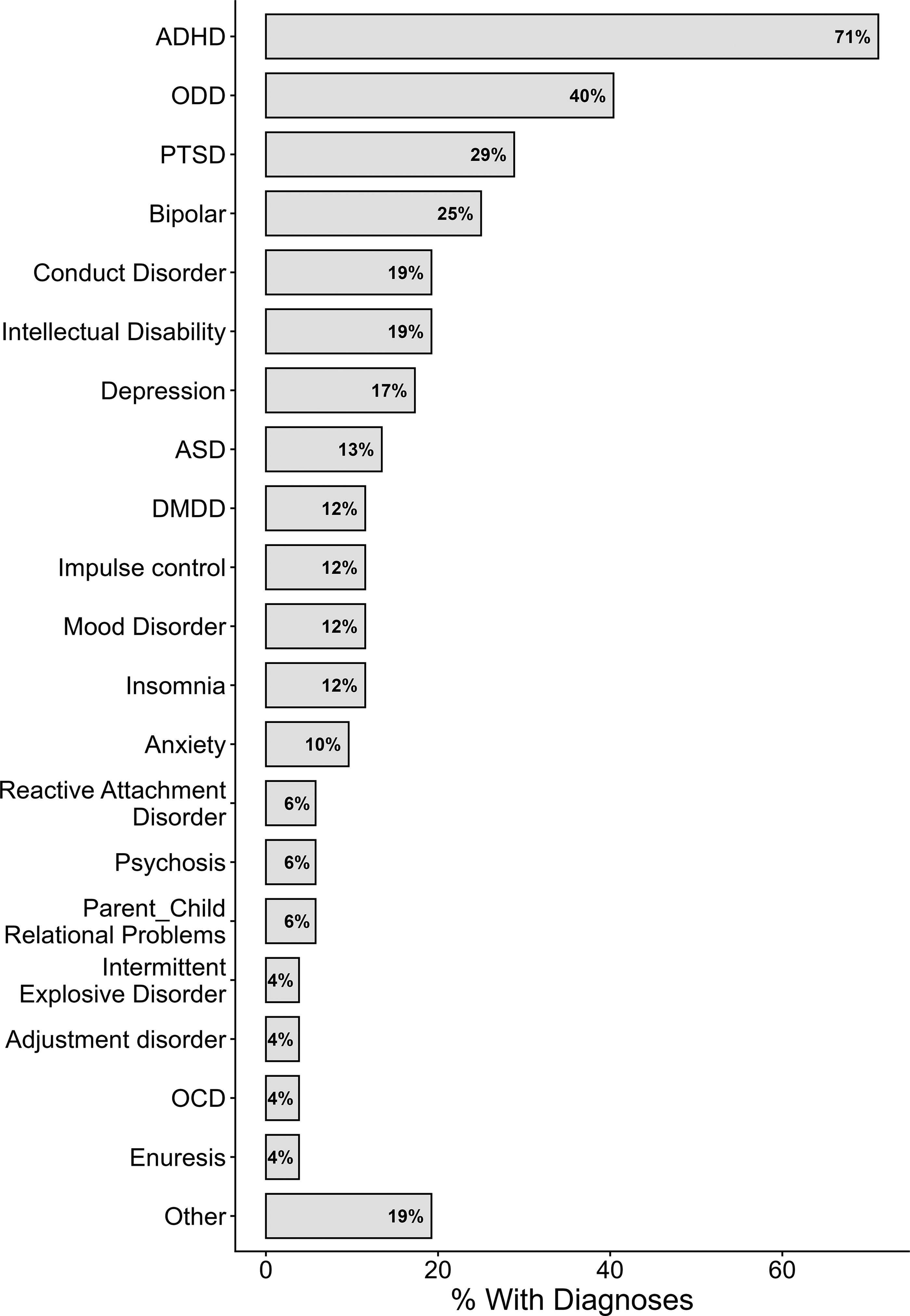
Each horizontal bar represents the proportion of cases (horizontal axis) that contained the diagnosis shown on the vertical axis. The actual percentage is shown inside the bar. The “other” category contains diagnoses received by only one participant. See the text for a list of these diagnoses. The numbers sum to greater than 100% because participants usually received more than one diagnosis. ADHD, Attention Deficit Hyperactivity Disorder; ASD, Autism Spectrum Disorder; DMDD, Disruptive Mood Dysregulation Disorder; OCD, Obsessive Compulsive Disorder; ODD, Oppositional Defiant Disorder; PTSD, Post Traumatic Stress Disorder.
The 52 referrals, 14 females and 38 males, were divided into three age groups; 5–8, 9–13, and 14–16 years old, containing 20 (5 females), 18 (4 females), and 14 (5 females) individuals, respectively, based on their age at referral. As compared with Medicaid clients statewide (Table 2), the cases used more medications (2.7 vs. 1.7/per month), cost more ($323 vs. $204/month), and received medications from Medicaid for more months (36.1 vs. 11.2 months), and for a longer period of time (40.4 vs. 14.6 months from entry into Medicaid until last recorded month).
Description of Clients Receiving Letters (Cases), Matched Controls, and All Cases (Matched and Unmatched) in the State Medicaid Database

The count of months with Medicaid coverage.
The span of Medicaid coverage, from the first to the last month listed.
A mix of propensity and exact matching was used to identify two controls for each case using the MatchIt package (Ver 4.2.0) in R (Ver 4.1.1), (Ho et al., 2011). Nearest-neighbor propensity matching was based on age at intake, months of Medicaid coverage, Medicaid coverage span, and number of medications taken in the first month. Exact matching was conducted for sex, race, and the use of antipsychotic medication or drugs used for ADHD (stimulants such as amphetamine and methylphenidate, or alpha-2 agonists such as guanfacine or clonidine) was prescribed. There were two medication classes: “AA” antipsychotic or ADHD medication and “other” for clients who did not receive these medications. AA medications were singled out because of their frequency of use in this population and their relatively high cost (Cohen et al., 2017; Keefe et al., 2023; Palmer et al., 2023). All patients and controls received medication through Alabama Medicaid. Supplementary Appendix SA1 contains a list of the medications used and their classification. A summary measure of the quality of matching, the standardized mean difference between cases and controls on these measures, changed from a mean of 0.45 (averaged across all the variables) before matching to 0.015 after matching. A low number reflects good matching.
The study was approved by the University’s Institutional Review Board. The
Medication review letters
Within 48 days (mean, range 2–122 days) of receiving a referral, either a board-certified psychiatric mental health nurse practitioner or a board-certified child, adolescent, and adult psychiatrist completed and submitted a medication review letter to the referral source, foster parent/guardian, or case worker. The letter required ∼30–60 minutes to complete. Only one letter was provided for each referral and there was no follow-up. The letter was sent with the encouragement to share it with the prescriber. Training for speaking with prescribers was available through a web video or by individual counseling. Each letter included client-specific information obtained from the child’s caseworker, foster parent, or guardian. Medical jargon was avoided so the information could benefit all parties. Supplementary Appendix SA2 contains two sample letters to foster children who received differing amounts of psychotropic medication.
The letters included (a) a description of the team services; (b) a rationale for the letter; (c) credentials and contact information for the medication experts providing the review; (d) the client’s name, date of birth, age, gender, and current diagnoses; and (e) a comprehensive list of current medications for the client. Each medication was analyzed individually to determine the appropriateness of the patient’s diagnoses (if available), age, health conditions, mental health symptoms, and allergies. Medications were assessed for U.S. Food and Drug Administration-approved indications, dosages, and potential interactions. For each medication, the letter included the approved indication, appropriate dose range, potential side effects, potential benefits, signs and symptoms to monitor with their degree of severity, and known interactions with other medications the child was taking. If a medication was considered unsafe or inappropriate, recommendations for reducing, eliminating, or adjusting the medication strategy were provided.
Data set
Medication information was obtained from a state Medicaid database spanning 47 months from November 2016 to October 2021. The database included the generic and proprietary name for each medication and the date the prescription was filled for every medication dispensed to individuals under 21 years of age in the state Medicaid system. Only psychotropic medications, drugs that cross the blood–brain barrier and act in the central nervous system, were considered for this analysis. A list of psychotropic medications reported is included in Supplementary Appendix SA1. To increase the likelihood that cases and controls began their Medicaid coverage within the months under analysis, we included only clients who were not listed in November and December 2016. Thus, the medication coverage for data analysis was 45 months, between January 2017 and October 2021.
Yoking of controls to cases
The goal of the analysis was to compare monthly trends in medication count before the letter was sent with trends afterward. Because the trends might have unfolded naturally, unrelated to the letter, the two matched controls were yoked to each case based on the number of months elapsed before the medication letter was sent. This created a virtual time at which a control received a “phantom” letter; no actual letter was sent. Figure 2 illustrates the yoking approach. Case 1 received a letter after 5 months of receiving medication through Medicaid. Phase “Before” comprised those 5 months and phase “After” comprised the first 12 months after the letter. The same month (relative to starting Medicaid) was identified for matched controls 1–1 and 1–2 so those phantom letters were yoked to its matching case. Case 2 was sent the letter after 9 months, so the timing of the two phases was different for the case and both controls. As with Case 1, the “Before” phase comprised all months before the letter and the “After” phase comprised the first 12 months after the letter. Such yoking is an exceptional way to match cases with controls on a range of variables and strengthens the similarity of propensity matching to a case-control study.
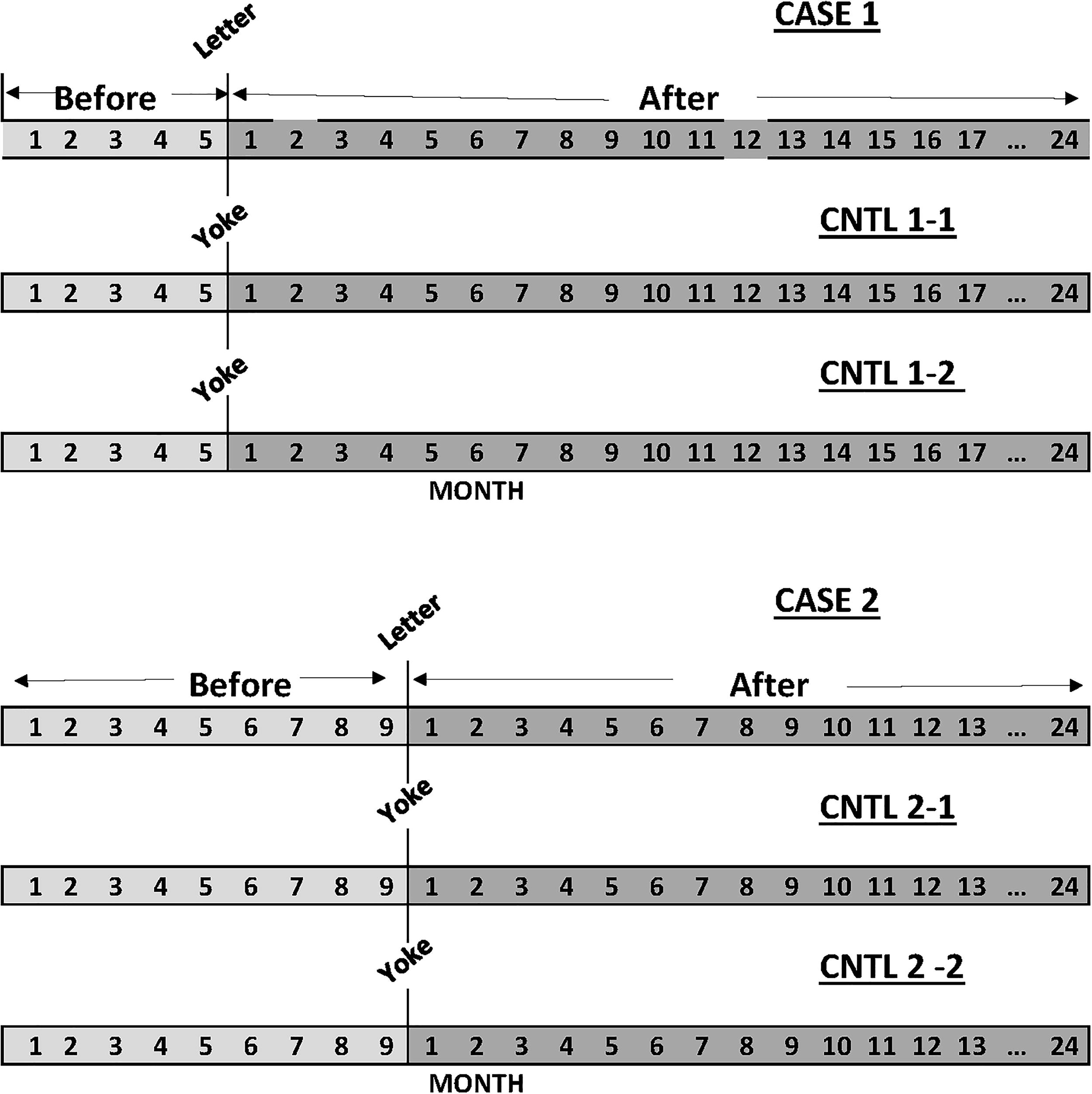
Illustration of the procedure used to yoke two matched controls to each case. The month that the medication consult letter was sent was identified for each case. This is month 5 for Case 1 and month 9 for Case 2. This same month was identified for the pair of controls matched to each case. The months before the letter, real for the cases, yoked for the controls, comprised the “Before” phase, and the months after the letter comprised the “After” phase up to 24 months. Only the cases received a letter.
Statistical model
A 2-month moving average was applied to the monthly medication counts to smooth fluctuations that could arise when, for example, two prescriptions were filled in 1 month and none in the subsequent month. If one prescription was filled on the first day of the month, a second was filled on the last day (to be used the next month), and no prescription was filled on the subsequent month, the moving average would smooth this to one prescription per month: two prescriptions divided by 2 months. The monthly medication count was not normally distributed but had a long right tail representing a small number of relatively large values. Evidence for this skew can be seen in Table 2, where the standard deviations are quite large relative to the mean. Examination of several possible continuous distributions revealed that a log-linear distribution fit the medication count well.
The results were analyzed with a generalized linear mixed-effects model using glmer in the lme4 package (ver. 1.1–27.1) in R. When the smoothed monthly medication count was the dependent variable, a Gaussian distribution with a log link was used for modeling, which modeled the medication count as a log distribution and prevented the modeling algorithm from generating numbers less than or equal to zero. The independent variables medication letter (True for cases and False for controls), phase (before or after the medication letter), number of months in a phase (rescaled to a Z score), and age group served as fixed effects (predictors). The number of months in a phase started at one for the first month in Medicaid and was reset to one the month after the letter was sent, marking the beginning of the “After” phase. The best model was identified using a model-comparison approach (Burnham and Anderson, 2002; Newland, 2019). Many fixed-effects models were examined, including those containing a five-way interaction among medication class, phase month, age group, medication letter, and phase as well as all combinations of four- and three-interactions among these variables. Multiple random-intercept and random-slope models based on phase, month-within-phase, interventions received, and different combinations and interactions among these variables, with the client always nested in phase, were constructed and examined. Using the models that converged, the best model was selected based on the Akaike information criterion, corrected for a small sample (AICc) (Burnham and Anderson, 2002; Newland, 2019).
The final model for medication count included a five-way interaction among all variables and lower-level interactions among the independent variables. The random-effects structure for the top two models used a random intercept and nesting of the client within the phase (1|Client + 1|Client:Phase). This allowed the intercept for each client to depend on the phase and the month within the phase. This model was far better than the second-best model. With an AICc difference of 827, the second-best model has a low probability (e−827/2 = 2.6 × 10−18) of being a better fit. All other models provided even poorer fits.
Results
Monthly medication count
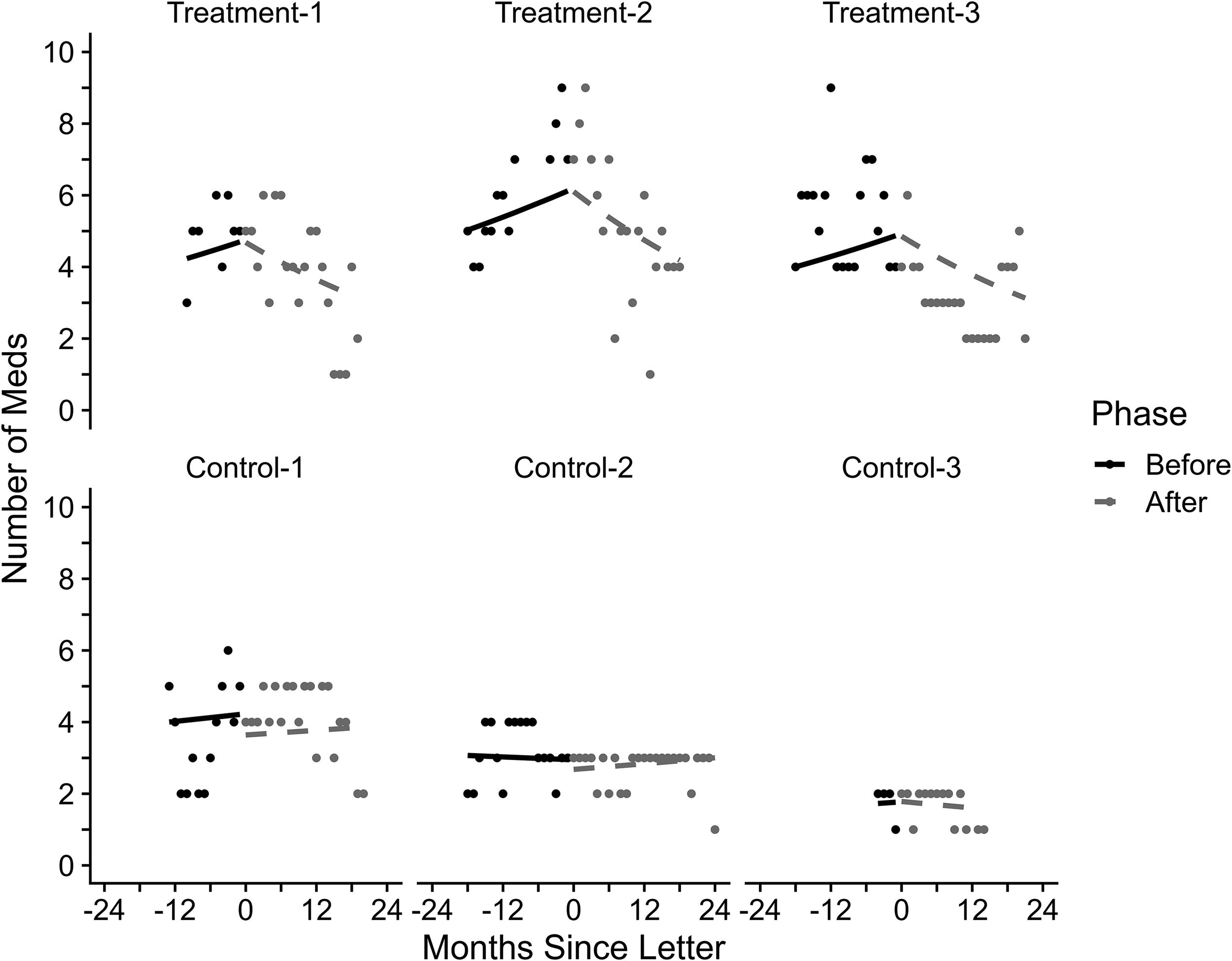
Figure 3 shows the monthly medication count before and after the letter for the three age groups as well as for AA and other medications across the entire data set. The age groups were based on the age at the beginning of the study. The top row shows the cases that received the letter, and the bottom row shows matched, yoked cases that did not receive a letter. Individual symbols show the geometric mean of medication count. The geometric mean was chosen for display because it corresponds to the analysis of the log medication count. There was a main effect of age group, with 9- to-12-year-olds (t = 2.3, p = 0.02) and 13- to 16-year-olds (t = 2.15, p = 0.03) having more medications than the youngest age group. There was no main effect of intervention (Med review vs. yoked control) or of class of concern (AA vs. other) (ps > 0.15), but there were important interactions involving these terms. Only those involving intervention and medication classes are reported. There was an interaction among intervention, phase, phase month, and age group for the 9- to 12-year-olds (t = 2.84, p = .0044) and 13- to 16-year-olds (t = 3.54, p = 0.0039). The slope of the curve describing the change in medication count before the letter was sent was positive while that slope was negative after the letter was sent, reflecting an increasing medication count before the letter and a decreasing count after the letter for those two age groups. This is visible in the top row of Figure 3. There was no consistent change in the slope for those who did not receive a letter. Medication class (AA vs. other) did not interact with these terms, indicating that the change in medication count was similar for both classes.
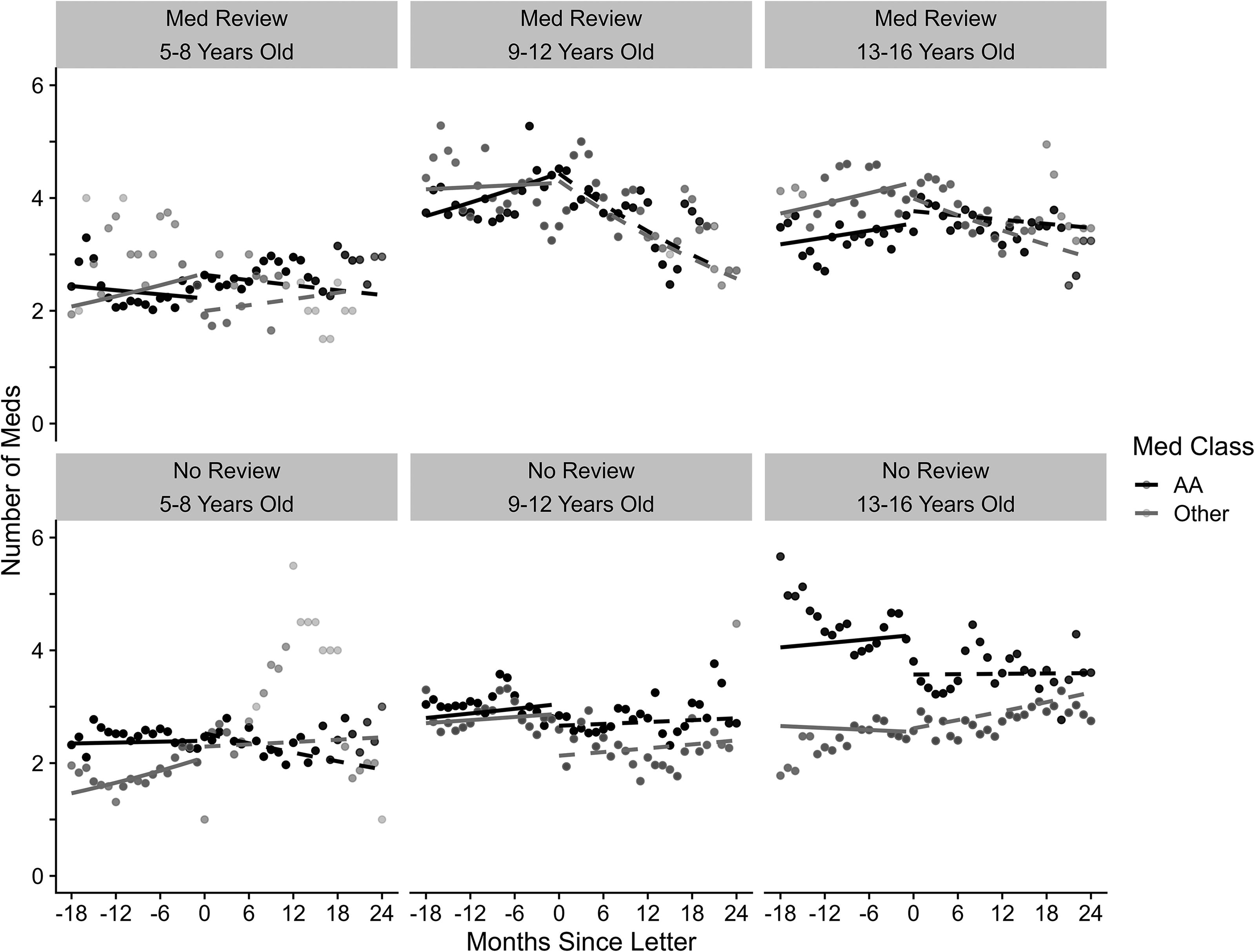
Time course of the number of medications used by clients who received a medication consult letter (top row) and controls who did not (bottom row) for three age groups. The thick, solid lines show the time course of medication count before the letter was received. The thick, dashed, shows the modeled medication count after the letter for clients and the equivalent (yoked) time for the controls. The black line shows AA medications, antipsychotics, and those used to manage ADHD. The gray line shows other medications. Small symbols show the geometric mean of the monthly medication count. ADHD, attention deficit hyperactivity disorder.
Fidelity of the random-effects predictions
The ability of the model selected to capture individual patterns of medication count is illustrated in Figure 4. This figure shows individual medication counts and the random-effects prediction for three arbitrarily selected intervention cases (top row) and controls (bottom row). Although there was some month-to-month variability in the individual cases, even after smoothing, it is evident that the individual cases were modeled accurately.
Representative random effects fits for three clients who received the letters and three controls. Data points show the clients’ actual medication count and solid lines show the fit of the random-effects model.
Summary of medication count after the letter
To quantify further the impact of the letter, medication count was assessed the month before the letter was sent and 6, 12, and 18 months after it was received for the 9- to 12- and 13- to 16-year-olds for the groups that received a letter. These are the age groups in which the previous analysis (Fig. 3) showed that the letter changed the trajectory of prescribing. To assess this impact, the medication count was estimated for each client based on the modeled random effects (exemplified in Fig. 4) at these times, and the difference for each client was assessed.
Table 3 shows the mean difference and 95% confidence intervals (CIs) for those who received the letter. The yoked controls are not shown because they showed no change in the trajectory of medication count. (They were analyzed and the results confirmed the absence of a change in trajectory). Bolded, filled entries show where the 95% CI did not include zero, indicative of a significant change. For the 9- to 12-year-olds, a decrease in the AA medications appeared within 6 months and a decrease in other medications appeared after about a year. These levels began to stabilize at a decrease of 1.1 medications after a year, averaged between AA and other medications. For this group, the mean medication count was 4.65 medications when the letter was sent so there was about a 24% decrease in medication count. For the 13- to 16-year-olds, despite a change in the trajectory, there was no evidence of a decrease in medication count; it remained at about the level that it was when the letter was sent.
Difference in Medication Count
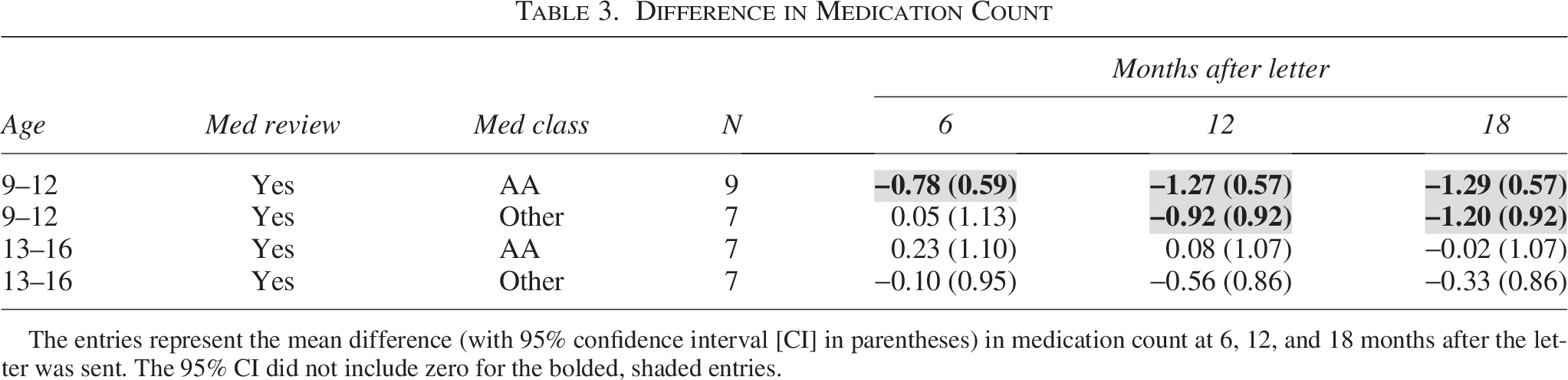
The entries represent the mean difference (with 95% confidence interval [CI] in parentheses) in medication count at 6, 12, and 18 months after the letter was sent. The 95% CI did not include zero for the bolded, shaded entries.
Discussion
Deprescribing psychotropic medications was recommended by the American Academy of Child and Adolescent Psychiatry (AACAP) (2015) and was urged in early consensus documents (Reiss and Aman, 1998), but it remains a difficult policy to implement. Deprescribing entails reducing a dose or removing a medication if it is unsafe or unnecessary. The present study examined the removal of a medication. A review of the literature reported several approaches to deprescribing (Grudnikoff et al., 2018), including administrative reviews, peer reviews, child advocates, and letters (reviewed by Mackie et al., 2017).
One approach to reducing the use of psychotropic medication is prior authorization for psychotropic medication by a judge or review team. In that case, authorization to prescribe a medication must be received in advance. Prior authorization is used in nearly half of the states, usually by Medicaid (Mackie et al., 2017; Mackie et al., 2021). In one study, prior authorization resulted in a 0.47% decline in the use of second-generation antipsychotics among Medicaid clients over the subsequent 2 years among 6- to 12-year-old children, but not in younger children (Stein et al., 2014), as compared with two sets of controls. One control was a similar state that did not require prior authorization, and the second was the use of antidepressants, which were not subject to prior authorization. Prior authorization reduces psychotropic medication use but has several limitations. It inserts a barrier to effective care when psychotropics are warranted, especially among vulnerable populations. When prior authorization is required for antipsychotic and anticonvulsant medication, it increases the use of expensive hospital emergency rooms (Lu et al., 2011). It can also be more cumbersome to change medications or prescribers when change is warranted.
One use of letters is illustrated by Sacarny et al. (2018), who used a peer-comparison approach to target the use of a single antipsychotic medication, quetiapine, in elderly patients on Medicare. The personalized letter compared the prescribers’ rate of prescribing quetiapine with that of professional peers and hinted at the possibility of losing prescribing privileges. It reduced the use of quetiapine but it is possible that another antipsychotic replaced it. Washington State reviewed prescriptions for ADHD medications when certain safety parameters were exceeded and mandated a second opinion from a peer (Thompson et al., 2009). This increased some medications and decreased others, with a net savings of state Medicaid expenses. The largest decreases were in children under 5 years of age.
The present study focused on Medicaid clients from a single state and examined all reported psychotropic medications. The clients were enrolled with the APMRT, a state-sponsored team that otherwise delivered behavior-analytic interventions but the clients described here did not receive behavioral interventions. Instead, their caretakers received a prescription letter and were urged to share it with the prescriber. Their involvement in the agency ended when the letter was sent.
The goal was to determine if the letter reduced psychotropic medications and to do this it is necessary to identify the number of drugs prescribed simultaneously. The definition of simultaneity is important but the window for coprescription in published studies has varied considerably. For example, dosReis et al. (2014) included drugs prescribed within the same year as coprescribed, an approach that probably overestimates its prevalence. In contrast, Martin et al., (2003) used a 7-day interval, which could underestimate coprescribing since prescriptions often are valid for 30 days. In the present study, coprescription was assessed on a monthly basis, which aligns with the practice of writing prescriptions for a 30-day supply (Zito et al., 2008). A two-month moving average over was applied to accommodate common situations in which one prescription was filled, say, at the beginning and end of a month, but not the subsequent month. In that situation, the data would show coprescribing in the first month but a reduced medication count in the second month.
A detailed analysis of individual cases (Fig. 3, top) revealed several important results. For APMRT clients, AA medication use by the 9- to 12 and 13- to 16-year-olds increased by ∼1–1.2 psychotropic medications during the period before the letter was sent. “Other” medication use also increased for the 13- to 16-year-olds. In contrast, medication use was steady in the control groups and in both youngest age groups, excepting “other” medications in the controls. It is not known why the APMRT, Med-review clients showed an increase over the months before the letter was sent. One possibility is that they were more likely to receive services than most Medicaid clients. A related possibility is that their cases were more severe than controls, despite matching, and this resulted in an increase in medication use. Recall that this group was referred to the APMRT and received the letter but no behavioral interventions. The 5- to 8-year-olds used fewer psychotropic medications than the two older age groups and this count was unaffected by the letter.
The letter precipitated a decrease in medication use over the months after it was received. The decrease was similar in magnitude in both broad drug classes, although from Table 3 it appears that the AA medications began to decrease 6 months after the letter while “other” medications began to decrease after 12 months. The decrease of about 1.1 medications for the 9- to 12-year-olds represents a reduction of about 24% over the count observed when the letter was sent. For the 13- to 16-year-olds, a rise in medication use seen in the Med review cases was halted by the letter. As compared with the 9- to 12-year-olds, however, there was, at best, a modest decrease in use, a conclusion confirmed by Table 3. The letter had no detectable impact on the 5- to 8-year-olds. These observations resemble a report of an attempt at deprescribing using prior authorization, in which a reduction in medication use occurred among 6- to 12-year-olds, but not among birth- to 5-year-olds (Stein et al., 2014). In the present study, the controls’ medication use mostly remained stable throughout the observation period, implying that no change in state policy occurred that might have influenced medication use in APMRT clients.
The clients in foster care received a wide range of medications, including antidepressants, anxiolytics, anticonvulsants, and those used for mood disorders or sleep disturbances. Medications used for managing ADHD, either psychomotor stimulants or alpha-2 agonists, target the most frequent diagnosis in this population. Antipsychotics are used to manage problem behavior such as that seen with autism spectrum disorders and intellectual disabilities but also seen among individuals in this population without those diagnoses. These two classes of medications raise particular concern because of their side effects profiles and their expense (Cohen et al., 2017). Accordingly, these classes of medication, termed AA medications here, were isolated for analysis. The analysis revealed that the impact of the letter was similar for both the AA and other medications, an important conclusion that might not have been noticed without this separation. The similarity in the effects might be because the personalized letters commented on total medication use and did not emphasize any medication class.
This study has limitations. Although propensity matching permits stronger cause-effect conclusions than correlational studies, it cannot be as strong as an a priori case–control study, even with the yoking procedure used here (Austin, 2011). Second, only the use of psychotropic medications via Medicaid was examined. If a child is adopted, a significant success, and medication use was provided through the adopted family’s private insurance, medication use would not be detected. The separation of AA and other medication classes is not pure. While it did distinguish children who did and did not receive AA medications, the children who received AA medications often received others. Finally, partitioning the population of children into age groups and medication classes reduced the sample sizes. The effects in the 9- to 12-year-olds appear robust, and it persisted with other analyses not reported here. For the teenagers, the letter appeared to reverse an upward trend in this population. However, as seen in Table 3, the decrease after the letter was small and embedded in the variability. A larger study might be necessary to detect the effect, if present in that age group.
In summary, personalized, respectful communication regarding the use of psychotropic medication was sent to caregivers, who were encouraged to share it with their prescribers. The letter changed the trend in psychotropic medication use among children older than 9 years old presenting significant problem behaviors. This approach offers a relatively straightforward approach to deprescribing but exactly how this letter works would be an ideal topic for future research. For example, does the letter sent to caretakers and the recommendation that they use it to speak with the prescriber encourage the caretaker’s assertiveness in speaking with the prescriber? Does it encourage the prescriber to devote more time and attention to the case? A deeper appreciation of whether such an intervention targets the caretaker’s or prescriber’s behavior would point to ways to improve the efficacies of such an approach.
Authors’ Contributions
All authors participated in conceptualizing the project and writing the article. J.T.R. and E.S.R. spearheaded the project. E.S.R. wrote the letters to caregivers. M.C.N. conducted the data analysis, interpreted the results, and spearheaded the writing of the article.
Footnotes
Funding Information
This study was funded by the Alabama Department of Human Resources, Family Services Division.
Data Access Statement
Because of the highly sensitive nature of data regarding children in foster care and those receiving psychotropic medication through Medicaid, the funders of the project forbid the posting of raw data, even in a deidentified form.
Ethical Approval
All procedures performed in this study involving human participants were in accordance with the 1964 Helsinki Declaration and its later amendments and were approved by the Auburn University Institutional Review Board.
Disclosures
The authors have no known conflicts of interest to disclose. On behalf of all authors, the corresponding author states that there is no conflict of interest.