
Abstract
Purpose:
The aim of this study was to compare pain response and hematologic toxicity between single and multiple therapies with 186Re-HEDP under zoledronic acid in patients suffering from painful osseous metastases from prostate or breast cancer.
Materials and Methods:
Forty-five (45) patients received multiple therapies of 186Re-HEDP (n = 77), under a stable regimen of analgesics and zoledronic acid, far off other therapeutic manipulations, and with no extraosseous disease progression. Hematologic status and pain indices were followed up regularly.
Results:
Evaluable patients (n = 12), received 31 186Re-HEDP therapies. After the first treatment with 186Re-HEDP, the mean percentile decrease for hemoglobin was 4.7%, for white blood cells was 21.4%, and for platelets was 12%. After multiple therapies, the respective declines were 7.0%, 16.0%, and 23.4%. With respect to baseline blood counts, only thrombocytes showed a tendency for greater decrease after repeated treatments, yet not of clinical significance. Favorable clinical response occurred after the first therapy in 10 of 12 patients (83.3%), after multiple doses in 15 of 19 (78.9%), and overall in 25 of 31 (80.6%) of 186Re-HEDP therapies. Significant post-therapy improvement in pain indices was observed in all cases, regardless of the number of therapeutic doses.
Conclusions:
Retreatments with 186Re-HEDP under zoledronic acid provide continuing effectiveness in metastatic bone pain and are safe enough, if an acceptable baseline hematologic status exists.
Introduction
Treatment with 186-rhenium-l,l-hydroxyethylidene diphosphonate (186Re-HEDP) has long been proven safe for palliation of bone pain in patients with widespread osseous metastases. 1 –3 Theoretically, 186Re-HEDP has the optimal characteristics of a radiopharmaceutical for treatment of metastatic bone pain: (1) a relatively short physical half-life (90 hours), (2) beta-emission, (3) gamma-emission proper for imaging, (4) selective bone localization, (5) rapid blood clearance and low extraosseous uptake, (6) low cost and ready availability, and (7) good chemical stability. 4 Bone marrow toxicity is the main dosage-limiting factor, seen mainly as thrombocytopenia, 1 –7 rather than leucopenia. 6,7 The toxicity of 186Re-HEDP is usually reversible, 4,5 with marrow recovery times typically ranging from 4 to 8 weeks. 5,7 –9 The combination of 186Re-HEDP and biphosphonates (especially the newer agent, zoledronic acid) in patients with painful bone metastases proved a more effective analgesic option, 10 in accord with results regarding also 188Re-HEDP, 1189Sr-chloride, 12 and 153Sm-EDTMP therapies. 13,14 On the basis that systematic studies evaluating the effect of 186Re-HEDP combined with biphosphonates, especially when concerning repeated doses of the radiopharmaceutical are scarce, the aim of this retrospective study was to evaluate and compare pain response and hematologic toxicity of single and multiple therapies with 186Re-HEDP combined with zoledronic acid in the same group of patients.
Materials and Methods
Study population
Forty-five (45) patients (33 males, 12 females), suffering from disseminated bone metastases from prostate and breast cancer, respectively, and who received 77 therapies of 186Re-HEDP under a stable regimen of zoledronic acid, were studied. Radionuclide treatment was administered according to the current guidelines of the European Association of Nuclear Medicine, as described thoroughly by Bodei et al.
15
Their medical records were analyzed retrospectively, according to the following additional requirements regarding the follow-up period: Pain or pain relapse that required 2 or more doses of 186Re-HEDP per patient; stable regimen of conventional analgesics; consistent regimen of biphosphonate therapy (zoledronic acid: Zometa®; Novartis Pharma AG, Basel, Switzerland/Novartis Pharmaceuticals Corp., East Hanover, NJ), given no sooner than 2 weeks before or after any 186Re-HEDP therapy; with a dose of 4 mg once every 4 weeks for at least 2 months; and chemotherapy or radiotherapy having not been administered for at least 2 months before the first dose of 186Re-HEDP and 2 months after the second one—if on hormonal therapy, having been on a stable regimen for not less than 3 months.
Patients who had or developed visceral metastases or rapidly progressive metastatic disease, sooner than 3 months after last therapy, were also not included in the analysis. Thus, for in-study patients, the possibility of the development of extraosseous painful sites during the study period, and also of any paliative or toxical effects of synergic therapies other than the combination of 186Re-HEDP and zoledronic acid, was diminished. Eligible patients should also not have been receiving type IV analgesics (i.e., parenteral narcotics or sustained-release morphine) prior to 186Re-HEDP therapy or during the follow-up period, while types II–III analgesia (i.e., oral narcotics) or type I (i.e., non-narcotics) was allowed.
186Re-HEDP administration
All patients were treated with a standard dose (1295 MBq) of 186Re-HEDP (Mallinckrodt/Tyco Healthcare, Petten, The Netherlands). 186Re-HEDP was delivered in the form of a single dose of 1295 MBq prelabeled kit (total volume, 1.2 mL) and administered slowly through a running intravenous (i.v.) saline drip. All patients were hydrated for 6 hours before and after they received 186Re-HEDP therapy to accelerate the clearance of radioactivity from the renal system. All patients were hospitalized during the day of administration in an isolated room at the Department of Nuclear Medicine, 401 General Army Hospital (Athens, Greece), according to local safety regulations, and then were followed and examined biweekly, usually as outpatients. Patients undergoing more than one treatment received the standard dose for all subsequent retreatments. Admission criteria and procedure modalities were the same as in the first therapy. A maximum ceiling of total administered activity was not established.
Pain assessment
The scoring of bone pain was performed according to previously validated methods. 8,16 –18 In particular, a pain score was calculated for all patients by multiplying the severity of pain by its frequency, both on a 4-point scale. Briefly, the intensity (mild, 1 point; moderate, 2 points; severe, 3 points; and unbearable, 4 points) and frequency (occasional, 1 point; intermittent, 2 points; frequent, 3 points; and constant, 4 points) of pain for all major sites of osseous pain were defined. A pain score index (PSI), equal to pain intensity times pain frequency (range, 0–16), was then calculated for each painful site, and the maximum of all regional PSI was finally entered in the pain-response result analysis. The Karnofsky performance status score (KS) was also assessed in a scale of 0–100 19 (Table 1).
Image analysis
Imaging studies were performed before each treatment. They included computed tomography (CT), plain radiographs of chest and of abnormal areas, and radioisotope bone scan. All patients underwent bone scintigraphy with 99mTc-labeled diphosphonates within 1–3 weeks preceding 186Re-HEDP injection in order to document the extent of osteoblastic metastatic disease and to correlate pain sites with pathological foci. The total number of lesions was determined by visually counting each discrete lesion; according to Soloway's scoring method, 20 a Soloway score index (SSI), which evaluates the severity of overall skeletal involvement with metastases, was attached to each bone scan as follows: grade I, less than 6 bony metastases (a lesion occupying the entire vertebral body was counted as two lesions); grade II, 6–20 metastases; grade III, more than 20 metastases, but not a ≪super scan≫ (i.e., diffuse symmetric skeletal uptake with no visualization of the kidneys); grade IV, ≪super scan≫ or its equivalent (involvement of more than 75% of the ribs, vertebrae, and pelvic bones).
Toxicity evaluation
For the assessment of hematologic toxicity, the World Health Organization (WHO) criteria 21 were used. Toxicity was defined as the absolute nadir level at the fourth week after each therapy with 186Re-HEDP, as well as the maximal percentile decrease after treatment in hemoglobulin (HGB), leukocyte (WBC), and platelet (PLT) count with respect to pretreatment levels.
Follow-up evaluation
Post-treatment data were compared with pretreatment data (baseline). Due to the small number of the patients (N = 12) and 186Re-HEDP therapies (N = 31), data of prostate and breast carcinomas were pooled. The following variables were monitored at predetermined intervals: (1) blood chemistry parameters (HGB, WBC, PLT, serum creatinine, liver enzymes, electrolytes, and serum levels of tumor markers)—every week for the first month after each therapy and then at 2 and 3 months; (2) clinical status, pain mapping, PSI, and KS (the same time with each blood exam); and (3) bone scanning findings, with SSI estimation (at 1–3 weeks before each therapy and then at 3 months). No additional treatment intervention or alterations in continuing therapy at that time, other than the clear need to prevent impending pathologic fracture, were allowed. With respect to pain, four levels of response were considered, according to a modified classification of Dafermou et al., 8 as reported (Table 2).
This modification was based on the assumption that the analgesic score was considered unchanged for all participants of the study throughout the follow-up period. For statistical reasons—to avoid small grouping—the aforementioned four groups of pain response were also pooled into responders (levels 2–4; reduction of pretherapy pain score values equal or more than 25%) and nonresponders (level 1; reduction of pretherapy pain score values less than 25% or increase). Pain-regression duration was also documented in all patients; survival estimations were not among the aims of the study, though.
Statistical analysis
Pretherapy values of HGB, WBC, and PLT counts, and KS, PSI, and SSI were considered as the major pretherapy parameters of significance and were entered in regression analyses, 22 –24 to find any possible correlations with the degree of post-therapy pain response; Pearson's correlation coefficient (r) was quantified to find the strength of the associations. Continuous variables with evident normal distribution were expressed as the mean ± 1 standard deviation (SD), otherwise with the median value and numeric range; categorical variables were expressed as numbers or proportions. Post-therapy HGB, WBC, and PLT count-drop comparison, with the baseline data, was done by the paired t-test. The paired comparison between pain response levels after each therapy was assessed by the use of the Z-test. Frequency differences for categoric data comparisons among groups were tested by chi-square analysis. To compare differences in PLT drop, pain, and scintigraphic scoring between various pain-response levels, the Wilcoxon-Mann-Whitney test for unpaired nonparametric variables was applied. Spearman's rank-order correlation coefficient test was also used to examine the response to therapy after each treatment. Values of p < 0.05 for all tests were considered significant. 25
Results
Thirty-three (33) of the 45 studied patients (73.3%; 25 males, 8 females), who received 46 therapies, were not evaluated, because they presented disease progression, increased analgesic consumption, underwent radiotherapy or chemotherapy before the second dose of 186Re-HEDP, or were not given a second dose at all. Thus, the final number of evaluated patients was 12 (26.7%; 8 males, median age: 74 years, range 67–85; 4 females, median age 61 years, range 39–85), who received 31 therapeutic doses (Fig. 1). Seven (7) of these patients, though, received further therapies with 186Re-HEDP after having been given chemo/-radiotherapy, thus they were subsequently excluded; the remaining 5 patients were not given such treatments at all (Fig. 1).

Patients in/out of study protocol in relation to the number of therapies given to each.
The overall follow-up period of the study was 50 months (December 2003 to February 2008). The follow-up period of each patient (median 11.8 mole; range, 6–20 mole) started immediately before the first therapy with 186Re-HEDP and lasted until 3 months after the last in-protocol therapy (2nd or 3rd), regardless of any subsequent 186Re-HEDP doses that might have been given after (Fig. 1). The median interval between dose administrations was 5.6 months (range, 3–15). In responders, decrease in pain usually occurred within 1–3 weeks after treatment; in the best of cases, clinically evident pain relief lasted throughout the follow-up period. The mean time to onset of response, mean duration of response, or time to maximum pain relief could not be estimated accurately because of inherent methodologic problems in timepoints definition. Nevertheless, the duration of pain response was more than 3 months in 8 of 12 of single therapies and in 11 of 19 of multiple therapies, with no trend for longer duration of response in either case, or between male and female patients.
Side-effects
The treatment was generally well-tolerated. Flare reaction was the only side-effect, seen in only 1 female patient (8%), being also a good responder to therapy. The pain intensity caused by this flare reaction lasted about 4 days, was relatively mild, and required no additional analgesics. None of the patients presented, at any significant degree, the typical hypocalcemic side-effects of zoledronic-acid therapy, either.
Hematologic toxicity
Hematologic toxicity was common, but confined to a mild, mostly grade I and, less commonly, grade II cytopenia, according to the WHO classification 21 ; it was assessed from the decrease observed mainly in PLT and secondary in WBC count and HGB values. In general, the overall profile of hematologic toxicity observed after administration of the standard dose of 186Re-HEDP was consistent with general experience regarding the use of this radiopharmaceutical for bone-pain palliation purposes. Hematologic toxicity after first therapy (N = 12) was compared to the overall toxicity after multiple therapies (N = 19). The median values (range) of HGB level, WBC, and PLT counts before first treatment with 186Re-HEDP were 12.9 (10.2–15.4) g/dL, 7.3 (5.4–9.7) × 109/L, and 198 (127–306) × 109/L. Respective values after first treatment were 12.3 (9.8–15.2) g/dL, 5.7 (3.8–7.7) × 109/L, and 171 (92–194) × 109/L. Accordingly, respective values before and after multiple therapies were 12.6 (9.9–15.3) g/dL and 11.8 (9.6–13.5) g/dL, 6.4 (4.2–8.9) × 109/L and 5.3 (3.9–7.4) × 109/L, and 191 (107–242) × 109/L and 147 (74–196) × 109/L (Figs. 2–4).
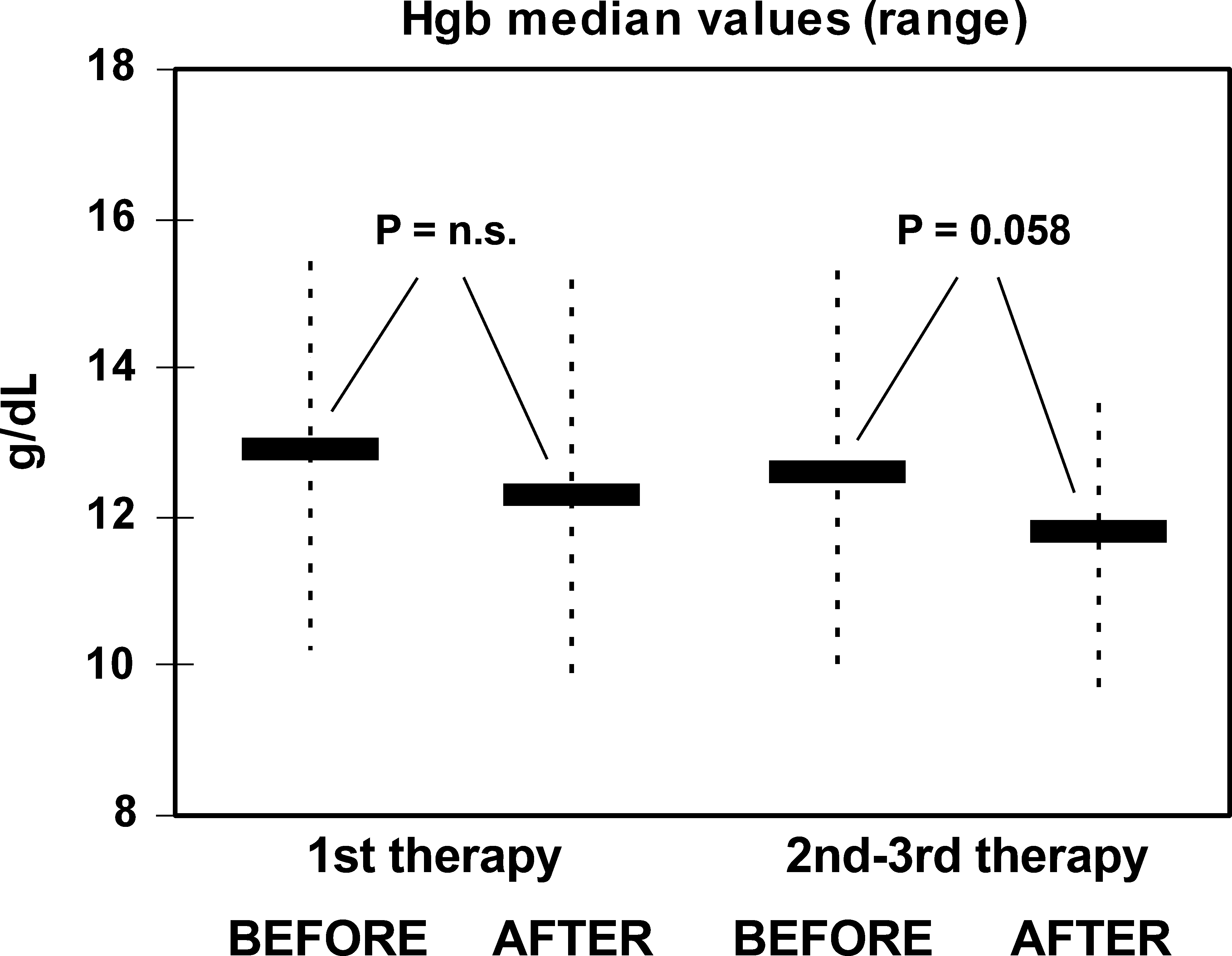
Respective changes in hemoglobin/leukocyte/platelet median values before and after first and second and third therapies with 186Re-HEDP.
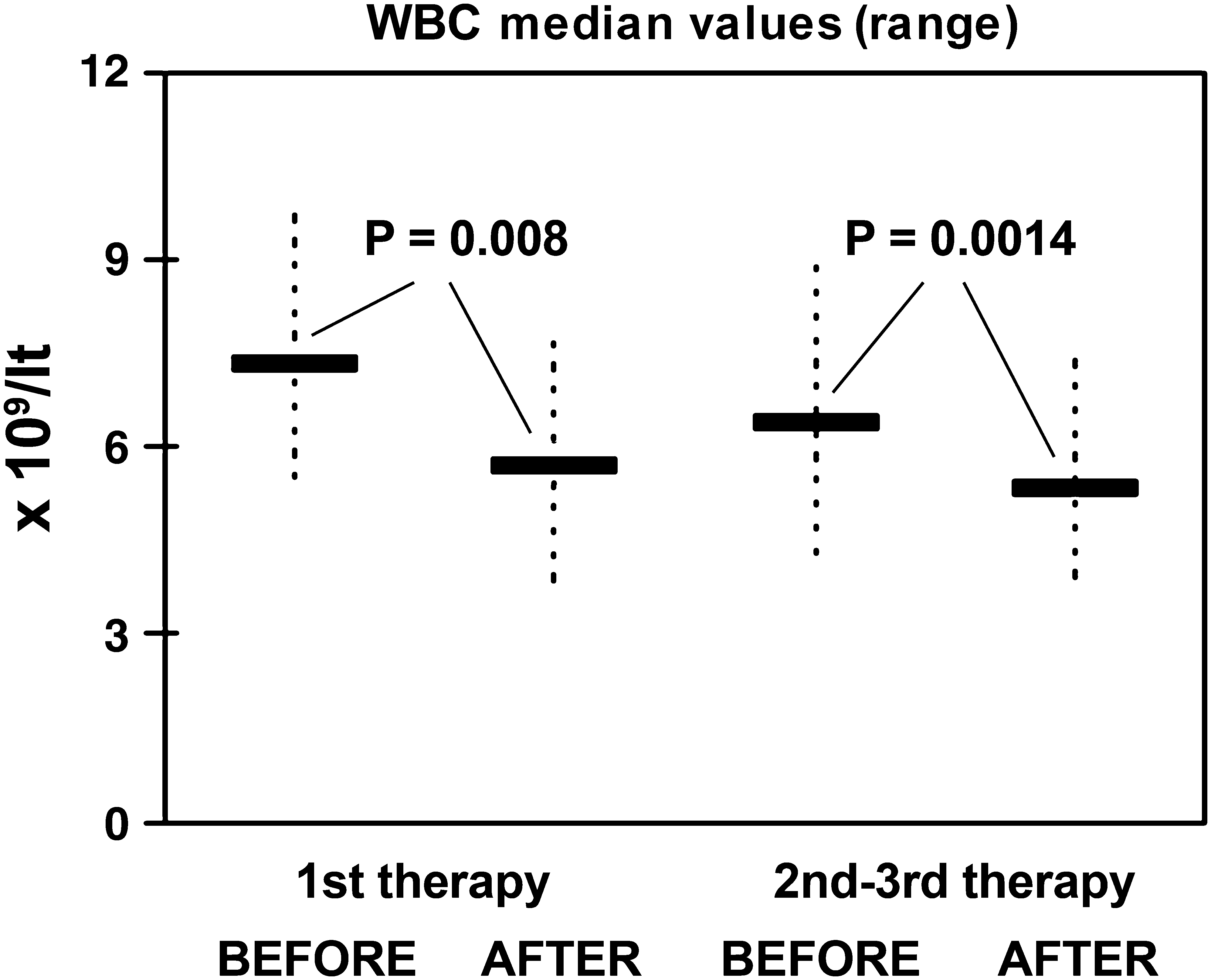
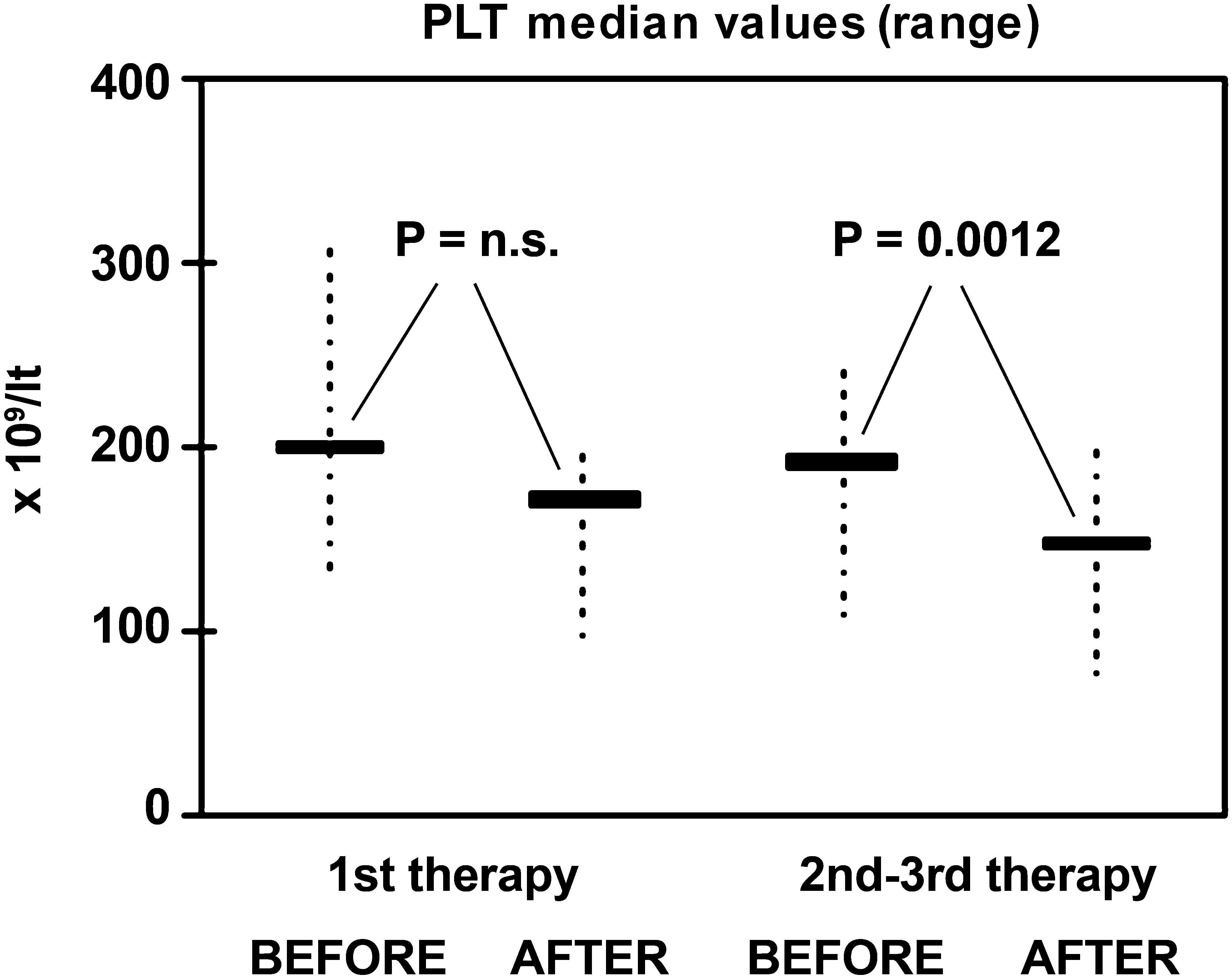
Half of the patients (6/12) presented with mild anemia (grade I; HGB = 10–12.5 g/dL) before the first dose of 186Re-HEDP, but none with leucocytopenia (i.e., <4 × 109 leukocytes/L), or thrombocytopenia (<100 × 109 platelets/L). After the first therapy, anemia was observed in 1 more patient (7/12; 61.3%, 5 grade II; 8–10 g/dL), leucocytopenia in 2 (2/12; 16.7%, 1 grade II), and a mere grade I thrombocytopenia (75–100 × 109 platelets/L) in another 1 patient. Of the 19 patients proceeding to a second or third dose, 8 initiated with anemia (42.1%, 1 grade II), but also none with leuco-thrombocytopenia. After the second or third therapy, anemia was found in 4 more patients (12/19; 63.2%, 4 grade II), grade I only leucocytopenia in 1 (5.3%), and thrombocytopenia in 4 (21.1%, 2 grade II, i.e., 50–75 × 109 platelets/L). Nonetheless, cases of severe post-therapeutic hematologic toxicity (grade III–IV anemia, leucocytopenia, or thrombocytopenia, according to WHO criteria) were not observed. The mean percentage of decrease for HGB values after the first therapy was 4.7% (95% confidence intervals [CI] 1.8%–7.6%; p = n.s.), for WBC 21.4% (95% CI 11.3%–31.5%; p = 0.07), and for PLT 12% (95% CI 7.4%–16.6%; p = n.s.). After multiple therapies, the respective decline for HGB was 7.0% (95% CI 3.4%–10.6%; p = 0.058), for WBC 16.0% (95% CI 7.6%–24.4%; p = 0.0014), and for PLT 23.4% (95% CI 7.6%–39.2%; p = 0.0012). With respect to baseline HGB, WBC, or PLT blood counts, only thrombocytes showed a tendency for higher decrease after repeated treatments (p = 0.024).
Pain response
Overall, favorable post-therapy clinical response (levels 2–4) occurred in 25 of 31 therapies (80.6%), ranging from mild response (level 2; in 9 therapies, 29%), to good (level 3; in 10 therapies, 32.3%), and to excellent (level 4; in 6 therapies, 19.4%). Unfavorable response (level 1) occurred in the remaining 6 of 31 therapies (19.4%). After the first therapy, overall favorable response was reported in 10 of 12 therapies (83.3%; level 2 in 2, level 3 in 6, and level 4 in 2). After the second or third therapy, these values turned to 15 of 19 (78.9%; and, respectively, to 7, 4, and 4 for the various levels of favorable response) (Fig. 5). Z-score analysis could not reveal significant percentile differences among various response levels between single and multidose therapies, meaning that the percentage of patients with a significant improvement in pain indices was not related to the total number of therapeutic doses administered.
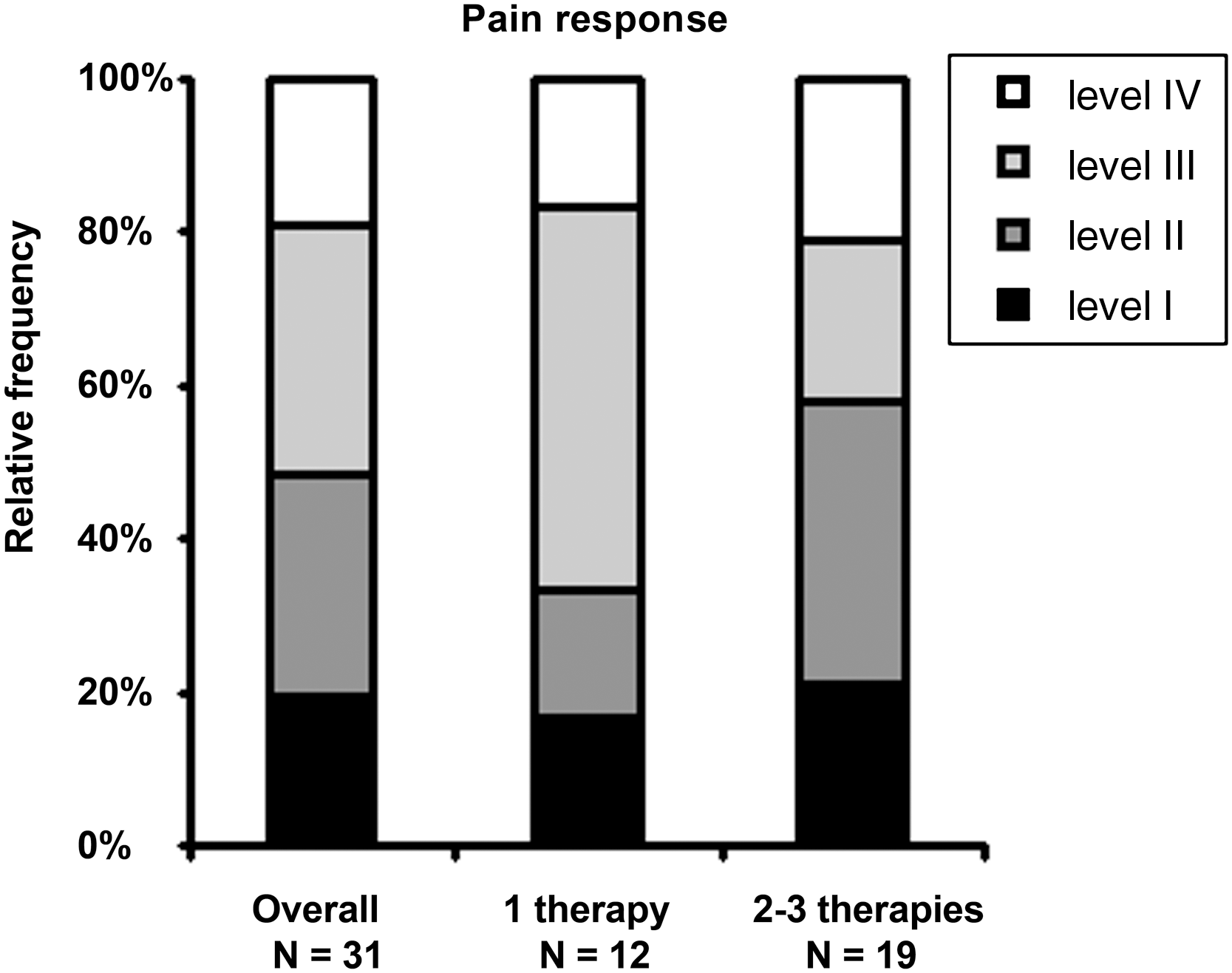
Relative frequency of various degrees of pain palliation, in terms of pain score index decrease (<25%; response level I, 25%–50%; response level II, 50%–75%; response levels III and IV >75%) in patients receiving single or multidose therapies, as well as overall.
Types II–III analgesics (i.e., oral narcotics) were being received by 3 patients, another 4 were under mild analgesia (type I), while 5 patients were not receiving analgesic medication at all. No apparent relation was seen between analgesic consumption and pretherapy pain scores or post-therapy pain response. The median pre- and post-therapy values of KS in the total therapy group, in patients after the first 186Re-HEDP therapy and in patients after multiple therapies, were 80.6 and 88.4, 77.5 and 87.5, and 82.6 and 89, respectively (Fig. 6). Significant improvement in KS post-therapy was observed in all cases (Spearman's r = 0.71–0.82; p < 0.01), although KS scoring could not reveal (z-score analysis) significant percentile differences in improvement rates between single and multidose 186Re-HEDP therapies.
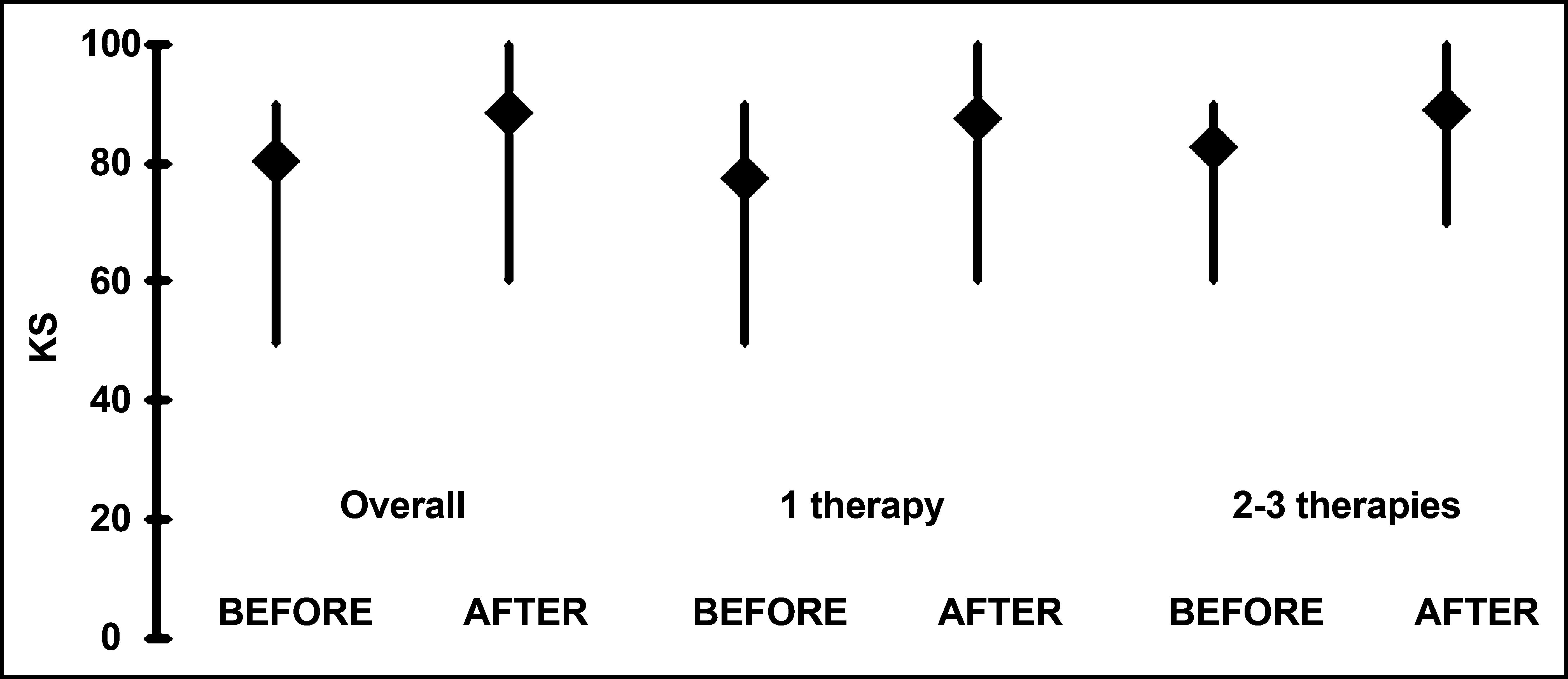
Median pre- and post-therapy values of Karnofsky performance status score in patients receiving single or multidose therapies, as well as overall.
Finally, regarding the bone metastatic load, 3 patients, who received 8 186Re-HEDP therapies, presented with SSI = 1; 2 more patients, who received another 5 therapies, presented with SSI = 2; and the remaining 7 patients, who received 18 therapies presented with SSI = 3. No patients had a ≪superscan≫ image pattern (SSI = 4) either before, or after any therapy, and also none presented a change in SSI grade during the protocol period. Although pain response was observed after all 8 therapies regarding patients with SSI = 1 and after only 17 of 23 (74%) of cases with a more widespread pattern of bone metastases (SSI = 2–3), statistical significance of proportional difference was missed (p = 0.108), probably due to the small patient cohorts. The main characteristics of the above-mentioned demographic, including pre- and post-therapeutic characteristics of the 12 evaluable patients, are summarized in Table 3.
Soloway score index grading, values 0–4.
Analgesic type grading, values 0–4.
Time (months) elapsed since first treatment with 186Re-HEDP.
Pretherapy values of pain score index (PSI) (Karnofsky performance status; KS).
Pain response level, values 1–4.
Maximal percentile decrease after 186Re-HEDP treatment in hemoglobulin (HGB), leukocyte (WBC), and platelet (PLT) count with respect to pretreatment levels.
SSI, soloway score index; PSI, pain score index; WBC, white blood cell; PLT, platelet.
Discussion
The determination of the palliative effect of the treatment with bone-seeking radiopharmaceuticals is very complex and responses are hard to objectify due to the highly subjective character of chronic pain, as illustrated by studies using 89Sr chloride 26 or 186Re-HEDP. 27 The rate of response may depend upon the pretreatment condition of the patient, the etiology of the bone metastases, differences in the populations treated, extent of the disease, and previous local or systemic therapy. 4
The overall response rate in the 21 studies analyzed by Lam et al. 4 regarding treatments with 186Re-HEDP for painful osseous metastases was 73% (range, 50%–92%), with no significant differences between prostate and breast cancer response rates. Clinical studies using 1295 MBq of 186Re-HEDP have reported response rates from 36% 28 in severely ill breast cancer patients for whom conventional treatments failed treatments up to 92%—this being the highest response rate found in the literature. 30 The post-therapy response rate in the current study ranges from 78.9% to 83.3% (overall, 80.6%); these values are in agreement with most reports of 186Re-HEDP therapies, despite some divergence regarding the efficacy criteria reported in the literature. In accord with the pain-response criteria of the present study, Maxon et al. 1 also used a decline in pain intensity of at least 25% from baseline, taking no account of changes in daily activity and/or use of medication. The subsequent success rate was a very comparable 77%.
The duration of palliative effect is also highly variable. 8 In the present study, two thirds of the patients had pain-response duration longer than 3 months, with no trend for longer response, between single and multiple therapies and also with no difference between males and females. These findings compare favorably to the results of multicenter observations reporting a similar mean painless period in prostate cancer (3.65 months) 30,31 and breast cancer patients (107 days), 4 though others 18 observed a tendency toward a better effect in the former.
Temporary pain flare has generally been reported in approximately 10%, 32 and up to 50%, of patients treated with 186Re-HEDP. 33 The frequency of pain flare reaction observed in our study (8.3%) was not substantially different from that reported by Dafermou et al., 8 who observed that transient phenomenon in 6.5% of 83 cases after 186Re-HEDP administration.
Repeated administration is safe; there is no limit to the total administered activity provided that 1) baseline counts are not very low and are not declining rapidly, and 2) the time interval from previous radionuclide therapy is sufficient to have permitted the recovery of bone marrow. 8 Most researchers agree that results of retreatments are less favorable than those of first therapy, 8,34,35 probably because candidates for retreatment are usually at a more advanced disease stage by the time of the second treatment, present a more compromised general clinical condition, or have shorter life expectancy. 8,35 Others, in agreement with the present study, report further pain relief in patients who had previously responded to the first treatment with 186Re-HEDP, 489Sr chloride, 36,37 or 153Sm-EDTMP. 38 The current trend is toward earlier intervention for patients with longer life expectancies than previous treatment populations. 9 Under this presumption, repeated administrations could lead to an onion-peeling effect of larger metastatic lesions. 3,4 It, therefore, appears that fractionated therapy with these agents will have the ability to reduce the metastatic burden.
Myelotoxicity is cumulative in patients receiving repeated radionuclide therapies for recurrent symptoms, but the toxicity of repeated therapy is not easily distinguished from the effects of underlying tumor progression. 39 Half of the patients in the current study presented with grade I anemia before the first dose of 186Re-HEDP, but none with leuco-thrombocytopenia; after the first therapy, a slight percentile increase was observed in all respective toxicity figures. In the well-known study of Dafermou et al., who used data primarily from 89Sr-chloride, rather than from 186Re-HEDP therapies, 8 but like this study, evaluated also multiple 186Re-HEDP therapies, an overwhelmingly high percentage (95.2%) of the patients presented with baseline anemia, thus indicating a considerably higher degree of marrow aplasia due to previous toxic therapies and/or to tumor invasion, compared to the patients of the present study. The better clinical condition of the evaluated patients in the current study is also demonstrated by the unusually high mean pretherapy KS (77.5–82.6; overall, 80.6). Almost half of our patients proceeded to a second or third therapy with baseline anemia, but also none with leuco-thrombocytopenia. After the second or third therapy, a slight percentile increase was observed in all respective toxicity figures, again without cases of severe post-therapeutic hematologic toxicity. With respect to baseline HGB, WBC, or PLT blood counts, only thrombocytes showed a tendency for greater decrease after repeated treatments. Accordingly, Dafermou et al. 8 reported a toxicity rate for platelets in retreatments almost 2-fold that of the current study (38.9% versus 21.1%), but like it, HGB and WBC were less influenced, and life-threatening events or toxicity in organs other than bone marrow were also not reported.
Specific correlations between any further clinical, biochemical, or imaging pretherapy variables and post-therapy response were not aims of the study, albeit responders to 186Re-HEDP therapies had an insignificantly lower bone metastatic load, in terms of SSI grading.
The present study focused on the comparison of pain response and hematologic toxicity between single and multiple therapies with 186Re-HEDP, in the same group of patients being under a regular regimen of zoledronic acid and during a time period with no evidence of extraosseous disease progression. As a result, this retrospective study has proved that multiple schemes (i.e., two to three) of 186Re-HEDP treatment are additively effective and safe, compared to one scheme of this radiopharmaceutical, in a selected group of breast or prostate cancer patients with painful bone metastases. Accordingly, there was no need for a group of controls, since each patient served as a control of him or herself regarding pain palliation and hematologic toxicity throughout the protocol period.
Conclusions
In conclusion, the current findings suggest that repeated treatments of 186Re-HEDP under zoledronic acid provide continuing effectiveness in metastatic bone pain control and are safe enough if an acceptable baseline hematologic status exists. Thus, repeated combined protocols of 186Re-HEDP and zoledronic acid show promising clinical results with minimal side-effects. Such improved clinical outcomes can expand the role of bone-seeking radiopharmaceuticals beyond their validated analgesic properties for bone pain palliation, 39 while clinical collaborations will optimize radionuclide therapy and increase awareness of its prospective benefits.
Footnotes
Disclosure Statement
No competing financial conflicts exist.
No funding has been received from any institute or organization for this work.