
Abstract
Besides bone marrow, the kidneys are often dose-limiting organs in internal radiotherapy. The effects of high-linear energy transfer (LET) radiation on the kidneys after alpha-radioimmunotherapy (α-RIT) with the alpha-particle emitter, 211At, were studied in nude mice by serial measurements of the glomerular filtration rate (GFR). The renal toxicity was evaluated at levels close to the dose limit for the bone marrow and well within the range for therapeutic efficacy on tumors. Astatinated MX35-F(ab′)2 monoclonal antibodies were administered intravenously to nude mice. Both non-tumor-bearing animals and animals bearing subcutaneous xenografts of the human ovarian cancer cell line, OVCAR-3, were used. The animals received approximately 0.4, 0.8, or 1.2 MBq in one, two, or three fractions. The mean absorbed doses to the kidneys ranged from 1.5 to 15 Gy. The renal function was studied by serial GFR measurements, using plasma clearance of 51Cr-EDTA, up to 67 weeks after the first astatine injection. A dose-dependent effect on GFR was found and at the time interval 8–30 weeks after the first administration of astatine, the absorbed doses causing a 50% decrease in GFR were 16.4 ± 3.3 and 14.0 ± 4.1 Gy (mean ± SEM), tumor- and non-tumor-bearing animals, respectively. The reduction in GFR progressed with time, and at the later time interval, (31–67 weeks) the corresponding absorbed doses were 7.5 ± 2.4 and 11.3 ± 2.3 Gy, respectively, suggesting that the effects of radiation on the kidneys were manifested late. Examination of the kidney sections showed histologic changes that were overall subdued. Following α-RIT with 211At-MX35-F(ab′)2 at levels close to the dose limit of severe myelotoxicity, the effects found on renal function were relatively small, with only minor to moderate reductions in GFR. These results suggest that a mean absorbed dose to the kidneys of approximately 10 Gy is acceptable, and that the kidneys would not be the primary dose-limiting organ in systemic α-RIT when using 211At-MX35-F(ab′)2.
Introduction
In internal radiotherapy, bone marrow, lungs, and kidneys are considered to be tissues at risk. Thus, the absorbed doses to these organs limit the activity that can be administered. We have previously performed preclinical alpha-radioimmunotherapy (α-RIT) studies, using 211At-labeled MX35-F(ab′)2 monoclonal antibodies, 1,2 and are currently evaluating this bioconjugate in a phase I clinical trial for ovarian carcinoma. 3 The use of F(ab′)2 fragments in RIT has been shown to be associated with a slightly higher uptake in the kidneys 4 –7 than with a whole IgG antibody. The distribution of F(ab′)2 fragments within the kidneys is not well known and neither are the renal-cell types at risk or their sensitivity to high linear energy transfer (LET) radiation. Since the kidney is a highly complex organ, with different functional compartments organized in specific substructures, an unfavorable distribution of the bioconjugate could result in a local, functionally detrimental level of absorbed dose, due to the short range of alpha particles. A very inhomogeneous dose distribution could have a significant effect on renal function, if functional subunits, such as glomeruli, for instance, are affected. This article describes the effects on renal function after internal irradiation with the alpha-particle emitter, 211At, providing information on the renal impairment after systemic α-RIT with 211At-MX35-F(ab′)2.
Studies on the toxicity of radiation to the kidneys require a long-term follow-up due to the slow turnover rate of renal cells. 8 At a clinical follow-up of a patient treated with 90Y-DOTATOC, Cybulla et al. found progressive renal failure 15 months after the last treatment. 9 Several studies on the effects of radiation on kidneys from internal irradiation have recently been presented within the field of peptide-receptor radionuclide therapy. Analysis of creatinine in serum as an indicator of renal function is a frequently used endpoint for renal toxicity in humans. Valkema et al. reported that several patients showed a decline in creatinine clearance of more than 40% per year following peptide-receptor radiation therapy with 90Y-DOTATOC, 10 with cumulative mean absorbed renal doses of approximately 27 Gy. In a study on radiation-dose distribution in human kidneys, Konijnenberg et al. used data from autoradiography to generate isodose curves and dose-volume histograms. 11 They concluded that for high-energy β-emitters (e.g., 90Y), the kidney dosimetry could be based on average Medical Internal Radiation Dose (MIRD)-based dose models, while for low-energy β-emitters (e.g., 177Lu) and Auger-emitters (e.g., 111In), the dose distribution would be highly dependent on the distribution of activity within the kidney's substructures. Future improvements in dosimetry for the kidneys require multiregional model approaches, as described in MIRD Pamphlets 19 and 20, 12,13 and will require better methods for the estimation of activity concentrations in separate compartments in the kidney over time. 14
The aim of this animal study was to evaluate the acute and long-term effects of irradiation on the kidneys after α-RIT with the alpha-particle emitter, 211At. The main endpoint chosen was the glomerular filtration rate (GFR), which was serially measured up to 67 weeks after astatine administration, using the 51Cr-EDTA method. Other measures used were blood analysis (serum creatinine and urea), urine analysis (proteins and erythrocytes), and morphology, using light microscopy. Systemic α-RIT was performed by intravenous (i.v.) administration of the alpha emitter, 211At, bound to the monoclonal antibody (mAb), MX35-F(ab′)2. A range of mean absorbed doses were delivered to the kidneys by using single or multiple injections and varying the activity in each injection to evaluate the relation between dose and effect. The animals used in this study were also included in another study, aimed at determining the therapeutic efficacy of repeated α-RIT on subcutaneous (s.c.) xenografts. Therefore, the present study includes data from both tumor-bearing and non-tumor-bearing animals.
Materials and Methods
Experimental design
To achieve high mean absorbed doses to the kidneys, while at the same time ensuring that the levels were safe for the bone marrow, administration was repeated up to three times. A wide range of mean absorbed doses to the kidney was achieved by combining varying amounts of injected activity with a varying number of injections. Data were obtained from a total of 177 animals, divided into experimental groups of 6–10 animals, as summarized in Table 1. The majority of the animals (119) were initially tumor carriers. The tumors were surgically removed after 40–80 days, depending on their rate of growth, allowing a long-term study also of the tumor-carriers.
Six to 10 animals per group. Groups 1 through 12 were initially tumor carriers.
Total dose from all injections.
Radionuclides and labeling
The alpha-emitter, 211At, was produced at the Cyclotron and PET Unit, Rigshospitalet (Copenhagen, The Netherlands) and isolated from the activated target by a dry distillation method, as described previously. 15 Subsequent astatination of the antibody was performed by using the m-MeATE-method described by Lindegren et al. 16 The injection solution of 51Cr-EDTA was obtained from GE Healthcare, Ltd. (Bucks, UK).
mAbs and cell lines
The F(ab′)2 version of mAb, MX35, produced by Strategic BioSolutions (Newark, NJ), was developed and kindly provided by the Memorial Sloan-Kettering Cancer Center (MSKCC; New York NY). Initial immunochemical characterization of the MX35 antigen has identified it as a membrane-associated glycoprotein of 95 kDa, expressed on the cell surface of ∼90% of human epithelial ovarian cancers.
17
Further characterization has shown that MX35 recognizes the sodium-dependent phosphate-transport protein 2b (NaPi2b) in human cancer cells.
18
The human ovarian cancer cell line, NIH:OVCAR-3 was obtained from the American Type Culture Collection (Manassas, VA) and cultured at 37°C in cell-culture medium [RPMI-1640, supplemented with 10% fetal calf serum (FBS), 2 mM of
Animals
Female nude mice (Balb C nu/nu; Charles River, Kisslegg, Germany) were used and were followed for up to 67 weeks. The animals (age, 4–6 weeks) were allowed 1 week of acclimatization upon arrival. They were fed ad libitum and otherwise maintained in compliance with guidelines of the Swedish Animal Welfare Agency. Upon any sign of poor health or a weight loss of > 10%, the animal was sacrificed. S.c. tumors were established by xenografting with two bilateral s.c. injections [2107 NIH:OVCAR-3 cells in 0.4 mL of phosphate-buffered saline (PBS)] in the scapular region. Tumors were then allowed to grow for 6–12 days, reaching a volume of approximately 50 mm3, at which point the astatinated antibodies were injected. The tumors were surgically removed 40–80 days after astatine administration, depending on their size.
Alpha-radioimmunotherapy
Tumor and nontumor carriers in groups of 6–10 animals received varying amounts of activity (four levels, including controls) via an injection of astatinated antibody in a tail vein. The injections were given one, two, or three times at intervals of 7–14 days. The amounts of activity administered in each injection and to each group are given in Table 1 and ranged from 360 to 1530 kBq. The combination of four levels of administered activity with up to three injections resulted in 12 different mean absorbed doses to the kidneys for the tumor carriers (0–15 Gy) and 8 for the nontumor carriers (0–12 Gy). The control animals received nonradiolabeled antibody only.
Estimation of the mean absorbed dose to the kidneys
Since the majority of the animals were tumor carriers (113 of 177), biodistribution data for 211At-MX35-F(ab′)2 from our previous study
19
on tumor-bearing animals were used to estimate the mean absorbed dose to the kidneys. The mean values of renal uptake (% injected activity/g of tissue) in the kidneys at different times postinjection were used to calculate the cumulated activity concentration, (
Determination of GFR
Measurements of the GFR were performed serially on the animals from week 8 after the first astatine injection up to week 67. Following a single i.v. injection of 0.08–0.12 mL of 51Cr-EDTA in a tail vein (∼150 kBq), three blood samples were collected from each animal (10, 20–30, and 40–50 minutes postinjection) from a tail vein. The blood was collected in capillary tubes (50 μL) and centrifuged to separate the plasma from the cell fraction. After measuring the volume of the plasma fraction, each tube was divided mechanically to separate the two fractions. Both parts of the capillary tube were placed in a test tube. Before measuring the activity in a gamma-counter, the part of the capillary tube containing the plasma fraction was rinsed with water (200 μL) in order to minimize geometric errors. The activity concentration of 51Cr in plasma was calculated and plotted on a semilog scale as a function of time postinjection. Assuming a one-compartment model, an exponential fit was made, and the area under the curve (AUC), was calculated from the intercept on the y-axis, i, and the gradient of the slope, m: AUC = i/m. Finally, the GFR was calculated (in mL/min) as GFR = Q/AUC, where Q is the amount of activity injected.
Blood and urine analyses
Serum creatinine and urea were analyzed in each animal at the time of sacrifice. Protein and erythrocytes in the urine were scored 11 and 17–18 weeks after astatine administration, using Multistix® reagent strips (Bayer Diagnostics Manufacturing, Cardiff, UK). To monitor the bone marrow toxicity, white blood cell (WBC) counts were measured, as described by Elgqvist et al., 20 on groups 1 through 12 (5 animals per group). Typically, WBC was measured after the first injection on day 5 or 6 (representing the nadir) and on days 10–12 (representing recovery) prior to the next injection.
Histologic examination
At the time of sacrifice, each animal was dissected and 1 kidney was removed, fixed in 4% formaldehyde, and embedded in paraffin. Sections (5 μm) were cut and stained with hematoxylin and eosin, according to standard protocols, to analyze possible pathologic changes in the morphology of the glomerular, tubular, vascular, and interstitial compartments, using light microscopy. Histologic evaluation of the tissues was performed by a renal pathologist.
Results
Radiolabeling of antibody MX35-F(ab′)2
Following astatination, the immunoreactive fraction of the antibody was in the range of 0.85–0.95 and the radiochemical purity was >95%.
Biodistribution and estimation of the mean absorbed dose to the kidneys
The biodistribution of 211At-MX35-F(ab′)2 in the kidneys and blood from our previous study 19 is presented in Figure 1, showing a fast uptake in the kidney, followed by an exponential decrease, similar to that of the blood. Using these data on renal uptake, the calculated mean absorbed dose to the kidney was found to be 3.89 Gy per MBq of 211At injected. The strategy of repeated injections of 211At gave a range of mean absorbed doses to the kidneys of 1.5–15.2 Gy in the different groups of animals.

The time-activity curves of 211At-MX35-F(ab′)2 in blood and kidneys, based on data from our previous study19 on tumor-carrying nude mice. %IA/g is plotted as a function of time after injection. Data are corrected for radioactive decay to the time of administration and given as means ± standard error of the mean.
Determination of GFR
The results reported in this study regarding the GFR were derived from a total of 430 GFR measurements on a total of 177 animals. The majority had tumors (119 animals), and a total of 310 GFR-measurements were made on these animals. An example of a GFR plot showing the plasma clearance from 10 individuals in a control group 34 weeks after treatment is presented in Figure 2. The fitted exponential curve used to estimate the GFR is shown for 1 individual. The GFR of the animals in all groups were estimated serially throughout the study. Due to the complexity of GFR estimations in mice, it was not possible to analyze all the study groups at exactly the same time after astatine administration. At the time of the first estimate of GFR (11 weeks after the first injection), signs of poor health and dehydration were seen in the group having received the highest level of activity (mean absorbed dose to the kidney of 15 Gy), and blood sampling and GFR estimation were not possible.

Example of a semilog plot of the 51Cr-EDTA plasma concentration versus time, used to estimate the glomular filtration rate (GFR). The filled symbols (♦) represent data from a GFR measurement on 1 individual animal, and the corresponding regression line giving the slope and intercept is shown (dotted line). Individual GFR data from the other animals in the same study group on this occasion are also given in the plot (+).
To evaluate the relationship between GFR and absorbed dose at different times after the first astatine injection, all the GFR measurements made throughout the study were divided into two major time intervals (8–30 and 31–67 weeks after first injection). This evaluation was done separately for the non-tumor- and tumor-bearing animals. Estimates of the GFR for each level of absorbed dose (mean ± standard error of the mean; SEM) in each time interval were plotted versus the calculated corresponding mean absorbed dose to the kidneys. As can be seen in Figure 3, these four dose-effect plots, representing the two time intervals after the first injection, show a clear dose-response relation between GFR and mean absorbed dose. The absorbed doses causing a 50% reduction in GFR was estimated from linear fits to these plots, using the slopes and intercepts, and the results are shown in Figure 4. For the tumor-bearing animals, the absorbed doses causing a 50% reduction in GFR during the early and late time intervals were 16 ± 3.3 and 7.5 ± 2.4 Gy, respectively, indicating a reduction progressive with time. The corresponding absorbed doses for the non-tumor-bearing animals were 14 ± 4.1 and 11.3 ± 2.3 Gy. The rate of decrease in GFR with absorbed dose (as estimated from the linear fits) for the non-tumor-bearing animals were 3.6 ± 1.1 and 4.4 ± 0.8 %/Gy for the early and late time intervals, respectively. The corresponding rate of decrease the tumor-bearing animals were 3.0 ± 0.6 and 6.6 ± 0.6 %/Gy. Although no statistical test was carried out on these data derived from linear fits, no major differences could be seen between the data derived from tumor- and non-tumor-bearing animals. Finally, we compared the GFR in the same individual animals (tumor-bearing animals) early after administration to that at a later time (separated by 35–50 weeks), by dividing the GFR at the later time by that at the earlier time for each individual. Figure 5 shows the mean values of this GFR ratio plotted as a function of mean absorbed dose to the kidney.
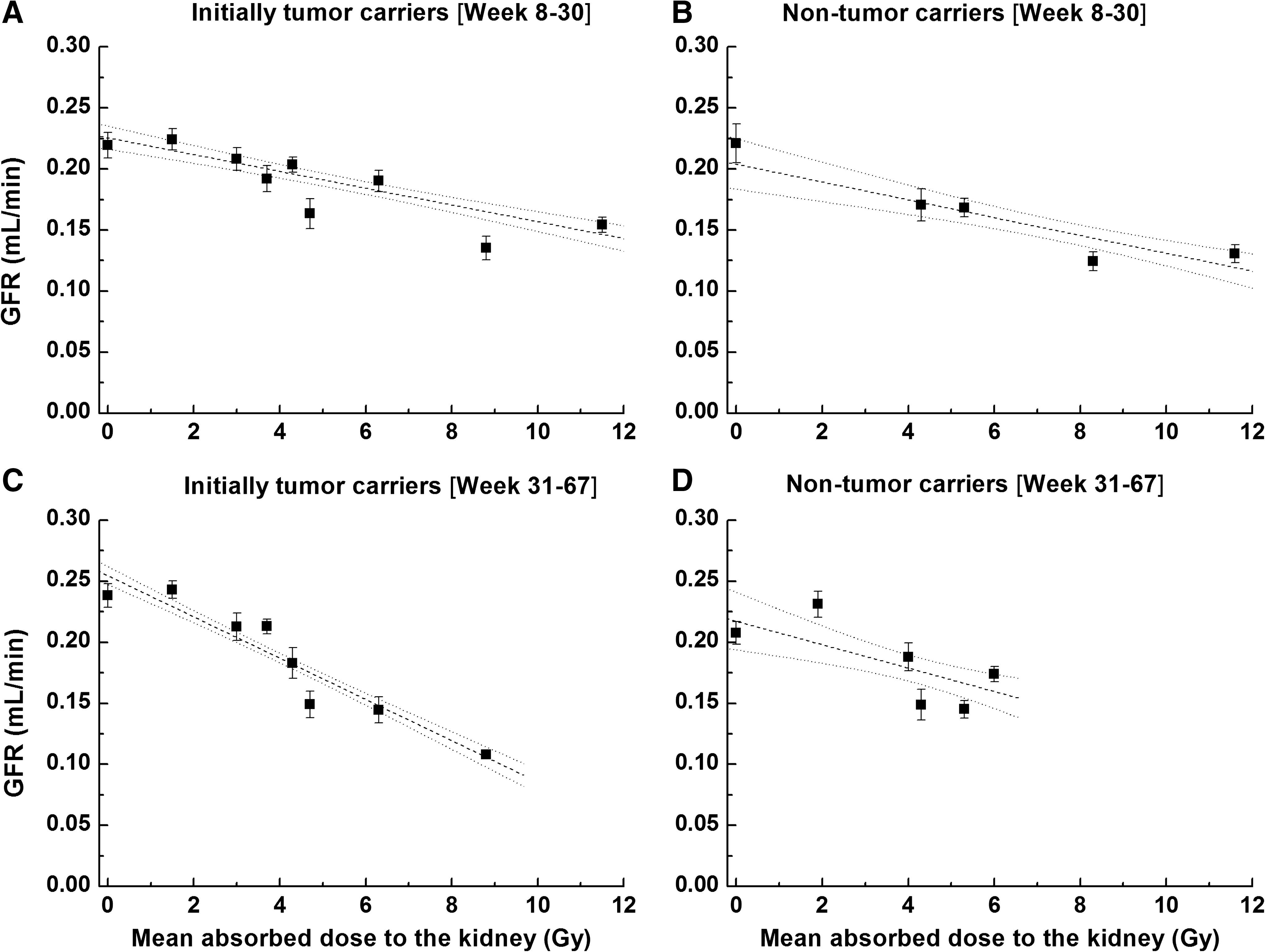
Glomular filtration rate estimates (means ± standard error of the mean) from each dose group plotted as a function of mean absorbed dose to the kidneys. Panels
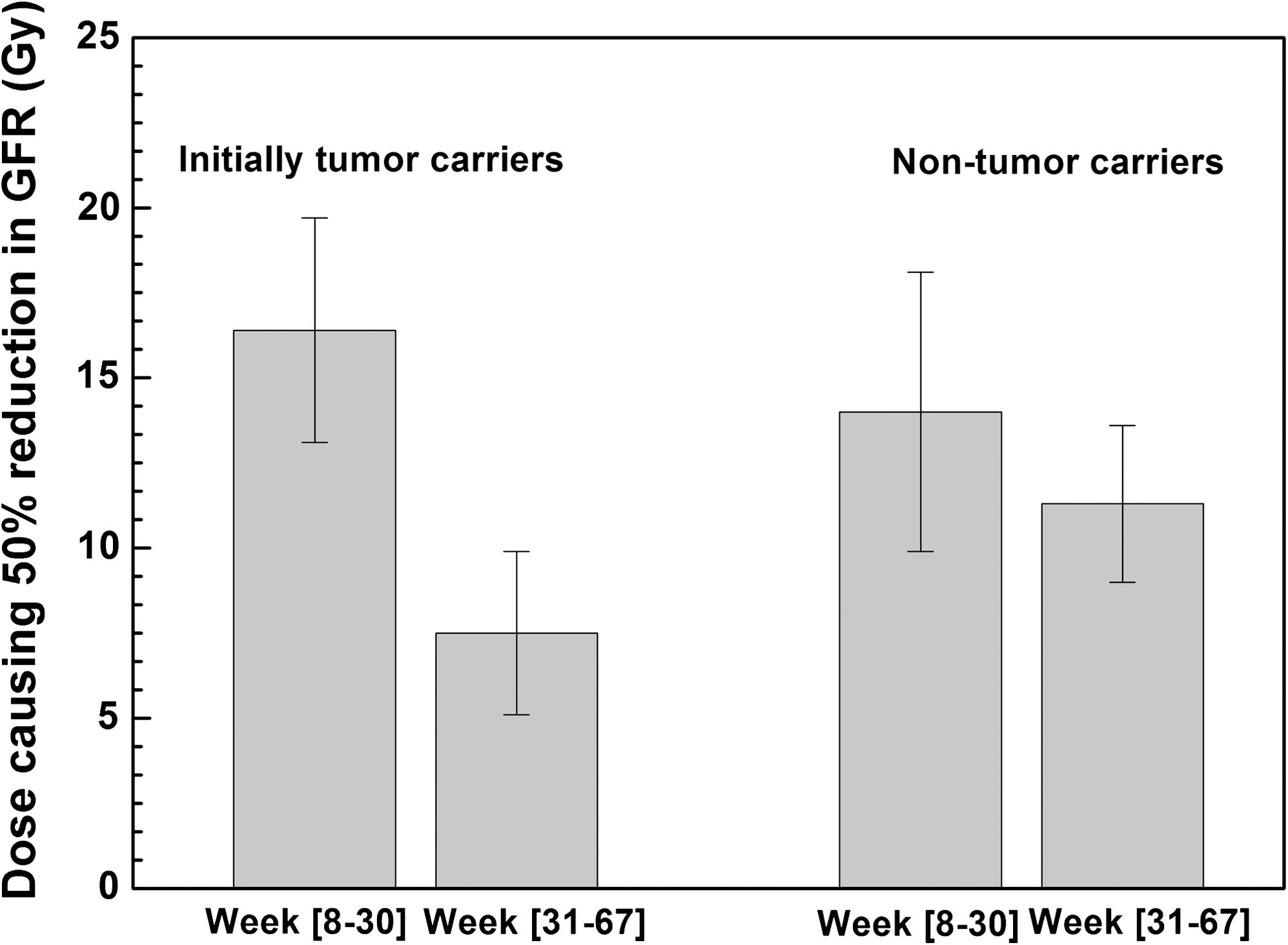
Comparsion of the absorbed doses causing a 50% reduction in glomular filtration rate at two time intervals (8–30 and 31–67 weeks) after the administration of 211At. The absorbed doses (± standard error) were estimated from the linear fit, using the slopes and the intercepts, of plots A through D in Figure 3.

Comparison of the glomular filtration rate (GFR) in the same animal at different points in time. GFR at 42–50 weeks divided by GFR at 8–10 weeks (within the same individual animal) is plotted as a function of the mean absorbed dose to the kidneys. Data are given as means ± standard error of the mean (n = 42).
Urine analysis
In most of the animals, the urine was analyzed (tumor- and non-tumor-bearing animals combined) at two different times after the first 211At injection, using reagent strips for proteins and erythrocytes. At 11 weeks (n = 110), indications of hematuria (∼10–80 erythrocytes/μL) were seen for all levels of absorbed dose above 5 Gy. After 18 weeks (n = 95), no hematuria was seen. No relation was seen between absorbed dose and proteinuria from using the reagent strips.
Blood analysis
At the time of sacrifice, blood was collected and prepared for the analysis of creatinine and urea (n = 145 and 146, respectively, tumor- and non-tumor-bearing animals combined). The unirradiated animals had creatinine serum levels (mean ± SEM) of 12.8 ± 0.65 μmol/L and urea levels of 8.3 ± 0.3 mmol/L. A dose-dependent increase was found for serum creatinine (Fig. 6A), up to a level of 21.4 ± 0.75 μmol/L for the group with an estimated mean absorbed dose to the kidneys of 15.2 Gy. No clear dose dependency could be seen for urea (Fig. 6B). The bone marrow suppression during and after treatment with α-RIT followed the pattern reported by Elgqvist et al., 20 with the lowest WBC of 1–2 × 109/L 5–6 days after treatment with 1400 kBq. The values in groups that were analyzed 12–14 days after the last injection had recovered to normal levels of approximately 5–9 × 109/L. The group given 2 injections of 1400 kBq still had a WBC of 3 × 109/L 13 days after the last injection, and the animals given 3 injections of 1400 kBq had a WBC of 0.8 × 109/L 6 days after the third injection.

Levels of creatinine (
Histologic findings
Renal tissues from control animals not exposed to radiation showed unremarkable histology, with patent glomerular capillaries, no tubular atrophy, no vascular changes, and inconspicuous interstitium. The histologic changes of the irradiated kidneys were overall subdued. None of the glomeruli were sclerosed, and no necrotic areas and no inflammatory infiltrates could be seen, regardless of exposure to radiation or time of sacrifice (Fig. 7A). Two patterns of renal damage could were discovered, though. The kidneys exposed to the highest level of absorbed dose (15.2 Gy) demonstrated a discrete increase in the amount of mesangial matrix as well in the number of mesangial cells. Increases in the thickness of the glomerular basal membrane was noted, along with a reduction in the number of patent glomerular capillaries, which was interpreted as an endocapillary swelling. A focal proliferation of mesangial cells was also seen. Some of the glomeruli were reduced in size and appeared presclerotic. This is consistent with the observed focal distribution of mesangiocapillary proliferation (Fig. 7C). The animals exposed to a moderate degree of radiation (8.8 Gy) demonstrated similar glomerular changes, although at a lesser degree, regardless of the time frame. However, the animals that received 8.8 Gy and were followed for an extended time (sacrificed at 37 weeks), as compared to the animals sacrificed at week 20, did, however, show focal areas of cortical tubular atrophy (Fig. 7B). Thus, the development of tubular atrophy is a process that requires time and, as judged from the material of this study, the histologic changes require at least 6 months to develop.

Kidney sections (5 μm) stained with hematoxylin and eosin. In panel
Discussion
The use of alpha-emitters in RIT for the treatment of micrometastatic disease is promising, as indicated by preclinical studies, 1,2,21 as well as by recently initiated clinical trials. 3,22 Both bone marrow and kidneys are dose-limiting organs and the use of small carriers (i.e., antibody fragments and peptides) has underlined the risk of renal toxicity in internal radiotherapy. We have used a F(ab′)2 fragment of the mAb, MX35, in an animal model of α-RIT to evaluate renal toxicity following high-LET irradiation with the alpha-emitter, 211At, at levels of activity well within the range of tumor efficacy. 19 The strategy employed in this study was to use levels of absorbed dose to the bone marrow that were close to those that would induce severe myelotoxicity. The activity administered was maximized by using up to 3 injections (at intervals of 7–14 days), thereby allowing the bone marrow to recover between successive injections. The resulting WBC counts were consistent, with the mice receiving the lower activities exhibiting some myelosuppression, followed by recovery, and those receiving multiple injections with high 211At activities exhibiting more severe myelosuppression.
Estimation of the GFR, the most important clinical parameter describing renal function, from plots of the measured plasma clearance of 51Cr-EDTA, was shown to be feasible in mice, as were serial measurements on the same individual. It was thus possible to study temporal changes on a long-term basis, which is necessary due to the low turnover of renal cells. The study period lasted up to 67 weeks, corresponding to approximately half the lifetime of nude mice. A dose-dependent effect on renal filtration capacity was found and, at 8–30 weeks after the first administration of astatine, the absorbed doses causing a 50% decrease in GFR were 16 ± 3.3 and 14 ± 4.1 Gy in tumor- and non-tumor-bearing animals, respectively. The reduction in GFR progressed with time, and at the later time interval (31–67 weeks), the corresponding absorbed doses were 7.5 ± 2.4 and 11 ± 2.3 Gy, respectively, suggesting that the effects of radiation on the kidneys were manifested late. This was also supported by the histologic findings. Estimates of the mean absorbed dose to the kidneys were based on data from our previous biodistribution study on tumor-bearing mice. 19 The same data were used also for the non-tumor-bearing mice in the present study. A difference in renal biodistribution between tumor- and nontumor carriers cannot be out ruled, contributing to the minor differences seen in the GFR reductions, especially at the late time interval. The study did not allow a proper statistical analysis of the difference in GFR with respect to the presence of a tumor or not.
The molecular weight of the F(ab′)2 fragment is ∼100 kDa, with a Stokes-Einstein radius of 38 Å, which lies within the size range (20–40 Å) 23 for glomerular filtration. 24 If neutral in electrical charge, the molecule would theoretically be filtered, to some degree, presumably 5%–8% of the GFR, meaning that not only the vascular compartments of the renal cortex and glomeruli would be subjected to radiation, but also the tubular compartments. This was supported by the histologic examination. It is interesting to note from the biodistribution data used in this study that, apart from the initial 30 minutes of uptake, the kidney-to-blood ratio of the F(ab′)2 fragment was close to unity during the 44 hours it was studied. This ratio can be compared to that of a whole IgG antibody, which generally has a ratio of 0.2–0.3. The high kidney-to-blood ratio obtained in this study indicates retention of the bioconjugate in the kidney. In an early study of the MX35-antigen, using normal human tissues sections, 25 presence of the antigen was detected in epithelial cells of the kidney collecting ducts. The significance of this for the renal biodistribution of 211At-MX35-F(ab′)2 is uncertain. However, retention of the bioconjugate in the kidney could possibly also be accompanied by protein degradation and cellular accumulation of free 211At (due to its partly metallic characteristics) in the proximal tubules. Despite their molecular weight of ∼100 kDa, renal uptake of F(ab′)2 fragments has been shown to be significant in several studies, especially when they were labeled with radiometals. 4 –7
The estimates of the absorbed dose to the kidneys were based on the mean absorbed dose to the whole volume of the kidney. It is likely, however, that the activity concentration is significantly higher in the cortical compartments, and that the absorbed dose distribution from the short-range alpha particles is heterogeneous. If the deposition of absorbed dose within the kidneys calculated in this study is confined to the renal cortex, the absorbed dose to the cortex would have been 22 Gy when the absorbed dose to the whole kidney was 15 Gy, using the cortex-to-kidney volume ratio factor for human adults of 0.69 given in MIRD Pamphlet No. 19. A study on rats, using stereologic procedures, 26 the dimensions of the renal structures were quantified and a cortex-to-kidney ratio of 0.79 was found.
There are few data on renal toxicity following internal high-LET irradiation with alpha-particle emitters. Jaggi et al. found morphologic and functional changes in mouse kidneys after injection of 225Ac-labeled antibodies, 27 with severe, widespread changes in the tubular cells. Loss of renal function was seen starting 20 weeks after injection, with blood urea increasing progressively up to 36 mmol/L, for an absorbed dose to the whole kidney of 27.6 Gy (and to the cortex of 39 Gy). For absorbed doses up to 15 Gy to the whole kidney (22 Gy to the cortex, when recalculated by using a cortex-to-kidney ratio of 0.69), the maximum level of urea in our study was 14 mmol/L. Jaggi et al. found serum creatinine within normal limits, but our study indicated that levels increased with absorbed dose. Robinson et al. 28 evaluated renal toxicity from α-RIT in 3 mice injected with astatinated diabodies (1665 kBq). One (1) year after treatment, the histopathologic examination revealed signs of renal damage in 2 of the 3 mice.
The differences in dose distribution and dose rate make it difficult to compare the dose-response of renal toxicity in this study with those using beta-emitters or external beam radiotherapy. The kidney tolerance absorbed doses of 23 and 28 Gy generally accepted in external radiotherapy 29 have been derived for the endpoint clinical nephritis (5% and 50% risk of renal failure within 5 years, respectively). We found that a mean total absorbed dose of 7.5–11 Gy caused a 50% reduction in GFR after 31–67 weeks postirradiation, which corresponds to half the lifetime of nude mice. Williams and Denekamp 30 used 51Cr-EDTA to estimate clearance in a study of renal damage in mice after local external irradiation (240 kV X-rays) of both kidneys. Twenty-five (25) weeks after irradiation, they found that the absorbed dose causing a 50% reduction in clearance was 16.6 ± 0.5 Gy. The absorbed doses to the kidneys in their study were homogeneous and the dose rate was high (2 Gy/min), corresponding to 65 Gy, if recalculated to total equivalent dose in 2-Gy fractions (EQD2), assuming an α/β ratio (the dose at which both components in the LQ model of cell killing are equal) of 3 Gy for the kidneys. At approximately the same time postirradiation (8–30 weeks), we found that an absorbed dose of 14 Gy, delivered during ∼12 hours (as estimated from absorbed dose calculation for the first 12 hours), caused a 50% reduction in GFR. As they produce the same biologic effect, these absorbed doses can be used to estimate a theoretic relative biologic effect (RBE) for functional renal damage. With the above X-ray radiation (recalculated to EQD2) as the reference, the estimated RBE for the alpha radiation in our study would be approximately 5.
The effect on renal function found in this study probably reflects cellular damage to both the glomerular and tubular compartments of the kidney. Initial evaluation with digital autoradiography 14 has indicated that the uptake of the 211At-MX35-F(ab′)2 bioconjugate is mostly confined to the renal cortex. Although the absorbed dose in the current study represents mean absorbed doses to the whole kidney, the intrarenal distribution of the astatinated F(ab′)2 fragments is likely heterogeneous, resulting in local absorbed doses substantially higher than the mean value. This could be the case in important functional subunits of the kidney, such as the glomerulus and the proximal tubular cells. Any effect on renal function of this inhomogeneity in the dose distribution is reflected in the reductions in GFR seen in this study.
A mean absorbed dose to the kidneys of approximately 10 Gy seems to be tolerable, corresponding to approximately a 50% decrease in GFR. A 50% decrease in kidney function is routinely accepted in cancer patients being treated with certain chemotherapies. If the biodistribution of the 211At-MX35-F(ab′)2 bioconjugate in humans is similar to that in mice, it is not likely that the kidneys would receive an absorbed dose this high as the administered activity would be limited by the bone marrow. In a previous study, 31 we found a bone marrow-to-blood ratio of 0.58 for 211At-MX35-F(ab′)2. In the current study, the kidney-to-blood ratio was very close to 1, and since the absorbed fraction can be approximated to 1, a mean absorbed dose the kidneys of 10 Gy corresponds to an absorbed dose the bone marrow of approximately 5 Gy. The differences in dimensions between human and murine renal structure (e.g., glomeruli) will probably have a sparing effect in patients, reducing the risk of renal toxicity in humans. Further, with the “excess” renal function in humans, the clinical consequences of the reduced GFR observed in the current animal study is likely to be well tolerated in patients. However, improvements in internal radiotherapy and α-RIT will require better knowledge on dose distribution within the kidneys.
Conclusions
At administered activities close to the limit of severe myelotoxicity and well within the range of therapeutic tumor efficacy, the effects found on renal function after α-RIT with the alpha-particle emitter, 211At, were relatively small, with only minor to moderate reductions in GFR. The results of this animal study suggest that a mean α-particle absorbed dose to the kidneys of approximately 10 Gy is tolerable, corresponding to a decrease in GFR (50%) that could be accepted in patients being treated for cancer. With levels of absorbed dose to functional subunits of the kidney that most likely are substantially higher, it could be suspected that the kidney, and not the bone marrow, would be the primary dose-limiting organ in systemic α-RIT with repeated injections of 211At-MX35-F(ab′)2. However, the findings of this study on GFR do not suggest this.
Footnotes
Acknowledgments
This work was supported by grants from the Swedish Cancer Society, the Assar Gabrielsson Foundation, and the King Gustaf V Jubilee Clinic Research Foundation in Gothenburg, Sweden. The laboratory technicians, Helena Kahu, Elisabeth Warnhammar, and Ingela Claesson, are all gratefully acknowledged for their contributions to this labor-intense animal study.
Disclosure Statement
No competing financial interests exist.