
Abstract
Radiopharmaceutical agents are utilized for imaging and treatment in nuclear medicine. Ionizing radiation produces free radicals in the cell that can induce damage to the DNA and lead to side-effects and/or secondary tumors. Radioprotective agents are useful in eliminating or reducing the severity of deleterious cellular effects, which are caused by exposure to internal and/or external irradiation in patients or staff personnel. There are two strategies for the potential use of radioprotective agents in patients, including agents used in patients for selective protective effects, such as reducing mocusitis, myelotoxicity, and kidney damage induced by ionizing radiation in radioiodine and radiolabeled peptide therapy. Second, radioprotective agents can reduce chromosomal aberration induced by gamma- or beta-rays and reduce the risk of tumors in personnel and patients.
Introduction
Irradiation properties of radiopharmaceuticals are used for imaging and treatment in the practice of nuclear medicine. Radioisotopes with mainly beta decay are used for treatment of tumor cells, in this way; the beta-particle causes cell damage, although the distribution between tumor and normal cells varies. Radiopharmaceuticals that produce gamma decay are used for imaging purposes. Ionizing radiation produces free radicals by passing within cells and interacting with water molecules. These free radicals can cause damage to critical macromolecules, such as DNA. The cellular DNA damage leads to disruption in cellular function, mutation, and cancer. 1 Patients and personnel are exposed to radiation in the nuclear medicine venue, and because radiation damages cells and organs, it is important that these people protect biologic systems from radiation-induced cell toxicity. Radioprotective agents are pharmacologic compounds that protect cells when administered before or during exposure to radiation. These agents may be utilized to eliminate or reduce the severity of deleterious cellular effects caused by direct internal exposure that patients receive or indirect external exposure that the personnel receive. Ideally, these agents should provide selective protection of normal cells over cancer cells. There are many radioprotective agents designed to protect against external irradiation, and these agents were used in radiotherapy. 2 Thiol compounds are the main radioprotective agents that have been tested for this purpose. Amifostine is a powerful radioprotective agent, compared with other agents, and it has been approved by the U.S. Food and Drug Administration (FDA) for mitigating side-effects (e.g., xerostomia) in patients undergoing radiotherapy with external beam. However, this drug has limited use in clinical settings due to its side-effects and toxicity. 3,4 There are several articles in the literature discussing the efficacy of radioprotective agents in external irradiation and radiotherapy. 2,5 Although many patients and personnel are exposed to radiopharmaceutical, as well as low, doses of external irradiation, there are currently no review articles discussing the potential utility of radioprotective agents in the practice of nuclear medicine. This review is focused on radioprotective agents that reduce the side-effects induced by radiopharmaceuticals and ionizing radiation and that may be useful in nuclear medicine.
Basic Concepts and Radiation Damage
Ionizing radiations consist of several different types of electromagnetic rays, such as gamma- and X-rays, or different particles, including beta-particles, alpha-particles, and neutrons. Ionizing radiation exposure is generally measured in terms of absorbed dose (i.e., the average energy deposited per unit mass). The unit of absorbed dose is the gray (Gy), in which 1 Gy equal to 1 J kg−1. There are two types of exposure to ionizing radiation: external and internal irradiation. Gamma and X-ray exposure are the two main types of external irradiation. Exposure to ionizing radiation, such as gamma-rays, may occur as a result of radiologic medical procedures, such as radiation therapy for treatment of various types of cancer. Internal irradiation occurs when a radionuclide enters the body and localizes in critical organs. Once deposited, the radioactive materials decay in the form of gamma- and beta-rays and irradiate tissues. Damage induced by ionizing radiation is dependent on some critical biochemical parameters, such as local oxygen pressure and the local concentrations of radical scavengers in the tissue constituents, that it is caused the primary damage (i.e., the number of primary DNA lesions). 6,7 Two modes of radiation action in the cell are direct and indirect action (Fig. 1). In the direct action, radiation may directly hit a particularly sensitive atom or molecule in the cell. The damage from this insult is irreparable, and the cell either dies or is caused to malfunction. In the indirect action, radiation can damage a cell indirectly by interacting with water molecules in the body. Tissue dose or biologically effective dose reflects the amount of carcinogen that has directly interacted with cellular macromolecules at a target site. It can be assessed from the amount of DNA and protein damage (i.e., strand breaks, DNA adducts, and protein adducts) in the target tissue or by extrapolating from damage levels found in surrogate tissues, such as white blood cells. Experiments have shown that, in general, DNA damage levels in target tissues and nontarget cells are proportional to the external dose. This class of markers is more mechanistically relevant to carcinogenesis than internal dose, since it takes into account differences in metabolism (activation versus detoxification) of the compounds, as well as the extent of repair of carcinogen-altered DNA. DNA and protein adducts are measures of exposure to carcinogenic compounds. They are mechanistically linked to cancer, as they cause DNA damage and mutations in important genes, such as genes coding for growth control or damage-repair enzymes. 6 Ionizing radiation can directly induce ionization in DNA, causing direct damage. However, the majority of damage from low LET (linear energy transfer), such as gamma-rays, occurs in an indirect manner via the formation of free radicals and H2O2, which are precursors of oxidative damage. The energy deposited in the water leads to the creation of unstable, reactive free radicals and oxygen species, such as hydroxyl free radicals and hydrogen peroxide. These free radicals and toxic substances can interact with critical macromolecules, such as DNA, proteins, or cell membrane, and can induce cell damage as well as tumor induction (Fig. 1). 6 When living cells or organisms are irradiated, OH radicals are generated in cells or tissue, which leads to many DNA lesions, including oxidative DNA base products. Both ionizing radiation and oxidative stress generate free radicals near DNA. Most of these radicals (R·) interact with oxygen, forming peroxyl intermediates (ROO·). Most of the products are eliminated by nucleotide excision repair, while a small fraction remains in the DNA. The biologic effects of radiation arise mainly from damage-induced in DNA molecules. Important types of DNA damage are DNA single- and double-strand breaks, base damage, intra- and intermolecular cross-links, and multiply damaged sites. As far as epigenetic damage or modifications of other cell constituents are concerned, cytoplasmic changes and mitochondrial or membrane damage may also play a role in certain types of radiation effects, but the importance of these for radiation-induced cancer is disputed. 6,7
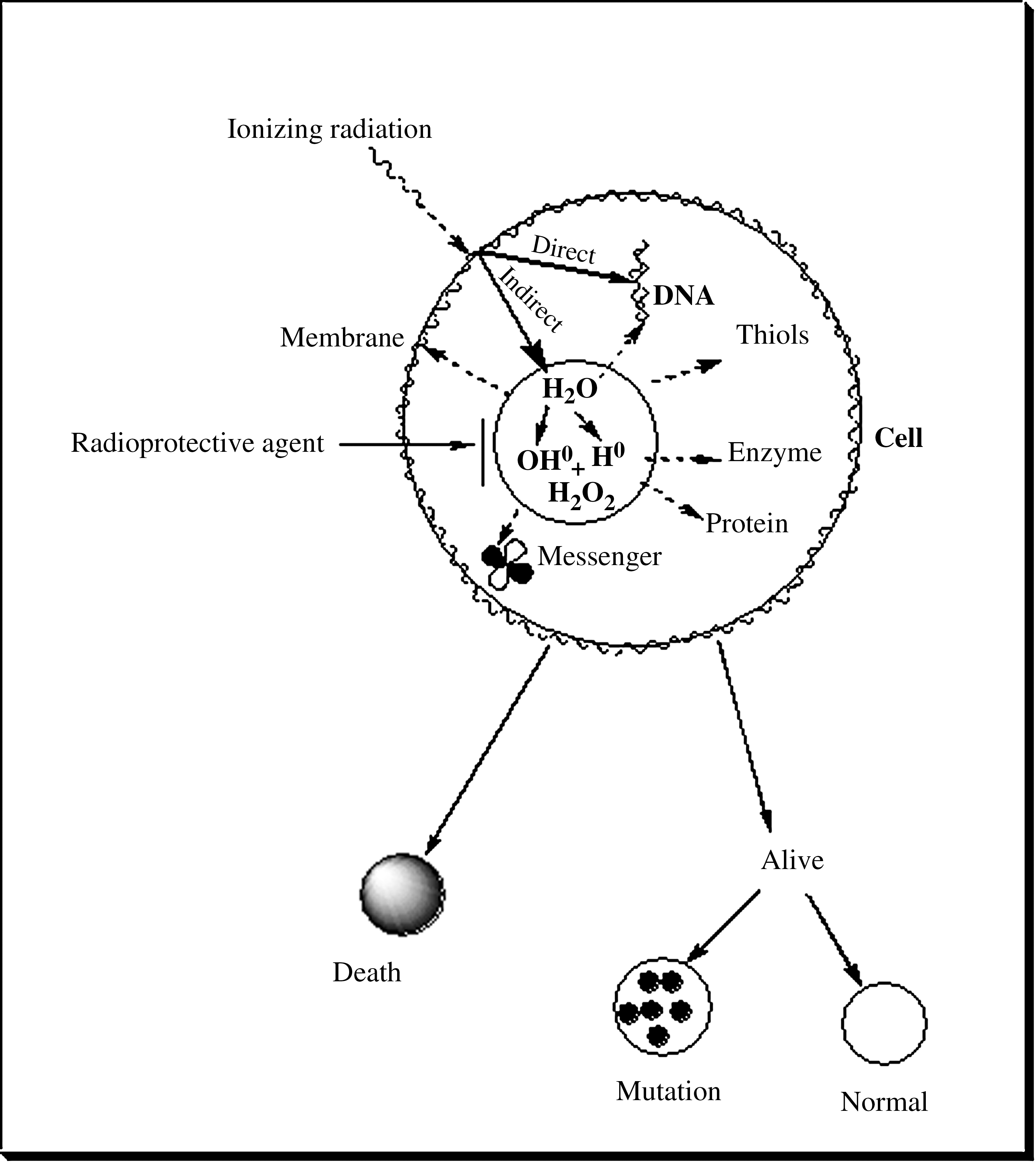
The effect of ionizing radiation on critical macromolecules in cells by direct and indirect pathways. Radioprotective agents scavenge free radicals to reduce the side-effects of radiation.
Exposure to high amounts of ionizing radiation results in damage and acute injury to hematopoietic, gastrointestinal, or central nervous systems, depending on the radiation dose. 7 The hematopoietic system has a high level of cell turnover, and it is one of the most radiosensitive tissues in the body. These acute injuries are caused by acute exposure to high levels of ionizing radiation, such as in radiotherapy and radiologic accidents. However, these toxicities do not result from low-dose exposure, such as with a diagnostic scan in nuclear medicine or radiologic imaging with X-ray. 7
Exposure to low doses of ionizing irradiation causes damage to cellular DNA, including DNA strand break, cellular dysfunction, and cell death. It is currently accepted that DNA strand breaks may be repaired. However, inappropriately repaired DNA breaks are primarily responsible for the induction of chromosomal abnormalities, gene mutations, and secondary tumors. 5,6
Diagnostic techniques in nuclear medicine apply radioactive tracers that emit sufficient gamma-rays from within the body. Because these agents remain in the body for some time, they must have a half-life that is short enough to decay soon after imaging is completed. The radioisotope widely used in medicine is technetium-99m (99mTc) with 140 keV of energy. In addition, radiopharmaceuticals used in positron emission tomography (PET) imaging have two 511-keV energies. 8 It is known that 99mTc emits low-energy Auger electrons, and these electrons carry only a small amount of energy. However, there is evidence indicating that the biologic effects produced by internal Auger emitters may be more severe than expected, based on conventional macroscopic dosimetry of radionuclides incorporated within tissues. Radiopharmaceutical localization at the cellular level plays a significant role in the absorbed dose in the nucleus of the cell in diagnostic nuclear medicine procedures. These nuclear effects may induce gene mutation, chromosomal aberrations, and cellular transformation. Taibi et al. showed that incubation of blood with 99mTc-methoxyisobutylisonitrile (99mTc-MIBI) increased DNA damage during treatment exposure to 9.25 MBq of this radiotracer. 9 The radiogenotoxicity, as measured by chromosomal damage of human lymphocytes by 99mTc at 21.46 MBq/107 cells, is equivalent to 1 Gy of 250 keV X-ray. 10 Thallium-201 (201Tl) has been widely used for cardiology studies. 201Tl decays by electron capture and emits low-energy Auger electrons that produce cytotoxic effects. Increased chromosomal aberrations and sister chromatic exchange is observed 3 days post-201Tl administration in patients with angina pectoris. 11 Chronic exposure to low levels of external irradiation by radiopharmaceuticals from occupational exposure in practicing nuclear medicine has been shown to have genotoxic implications. 12,13 Radionuclide therapy is an appropriate utility of radiopharmaceuticals, which emit mainly beta- or Auger electrons, for treatment of tumor cells. There are several radioisotopes that are utilized in nuclear medicine as therapeutic agents, including 131I (iodide), 90Y (yttrium), 89Sr (strontium), 111In (indium), 186Re (rhenium), 177Lu (lutetium), and 153Sm (samarium). These agents can also be used as tags on chemical compounds, peptides, or monoclonal antibodies for selective accumulation in tumor cells. 14 –16 Beta-emitting radionuclides produce greater toxicity and cellular damage due to the emission of charge particles. Adverse effects of 131I therapy include salivary gland dysfunction, (transient) bone marrow depression, and possibly, hypofertility. This therapy may also cause an elevated risk of leukemia and other secondary malignancies. 16 The side-effects of 131I-metaiodobenzylguanidine (MIBG) treatment include nausea, vomiting, and hematologic effects, particularly thrombocytopenia, neutropenia, and severe oral mucositis. 17 Acute myeloid leukemia was reported in 131I therapy for thyroid cancer. 18 Kumagai et al. reviewed reports regarding risks from iodine therapy and concluded that elevated risks for solid cancers and leukemia secondary to primary tumors were observed after radioactive 131I therapy. 19 However, the association between secondary primary malignancy and radioactive iodine is controversial. 19 –22
Radioprotective Agents
Radioprotective agents are useful in eliminating or reducing the severity of deleterious and cellular effects of ionizing radiation in cells. A radioprotective agent has several characteristics, including significant protection, preferable route of administration, low toxicity, and compatibility with other drugs that are administered to patients. 2 Reactive free radicals, such as hydroxyl radicals, hydrogen radicals, and hydrogen peroxide, are the main toxic substances produced by ionizing radiation during the passing of cells. Scavenging and elimination of free radical species are the main mechanisms for radioprotectors (Fig. 1). Free radical scavenging effects of these compounds remove and detoxify products of water radiolysis and reactive oxygen species (ROS) before these toxic substances interact with critical macromolecules, such as DNA. Radioprotective agents can induce hypoxia and consumption of oxygen in cells, which decrease the levels of ROS and hydrogen peroxide. The extent of radiation damage to an organ is directly related to the level of oxygenation of that organ. It should be noted that this hypoxia occurs at the cellular, rather than the systemic, level. Thiol-containing compounds have these effects in radioprotection. 23 The mode of action for another class of radioprotective agents involves stimulation, proliferation, and modification of the function of hematopoietic and immunopoietic stem cells. High doses of irradiation cause damage and suppress bone marrow cells. Hematopoietic tissue damage causes reduction of neutrophil and platelet numbers in circulating blood cells, which leads to septicemia, hemorrhage, anemia, and death. Cytokines can stimulate hematopoietic stem cells and thus regenerate bone marrow damages induced by ionizing irradiation. Cytokines and 5-androstenediol (as natural hormone) are included in this category; these agents stimulated myelopoiesis and enhanced circulating meutrophil and platelet numbers. 2
Aminothiols and compounds containing free or potential sulfhydryl (SH) groups are known to be the first class of radioprotective agents that have excellent radioprotective effects. These compounds scavenge free radicals, transfer hydrogen, and induce a hypoxia, which can protect cells against side-effects induced by ionizing radiation (Fig. 2). 24,25
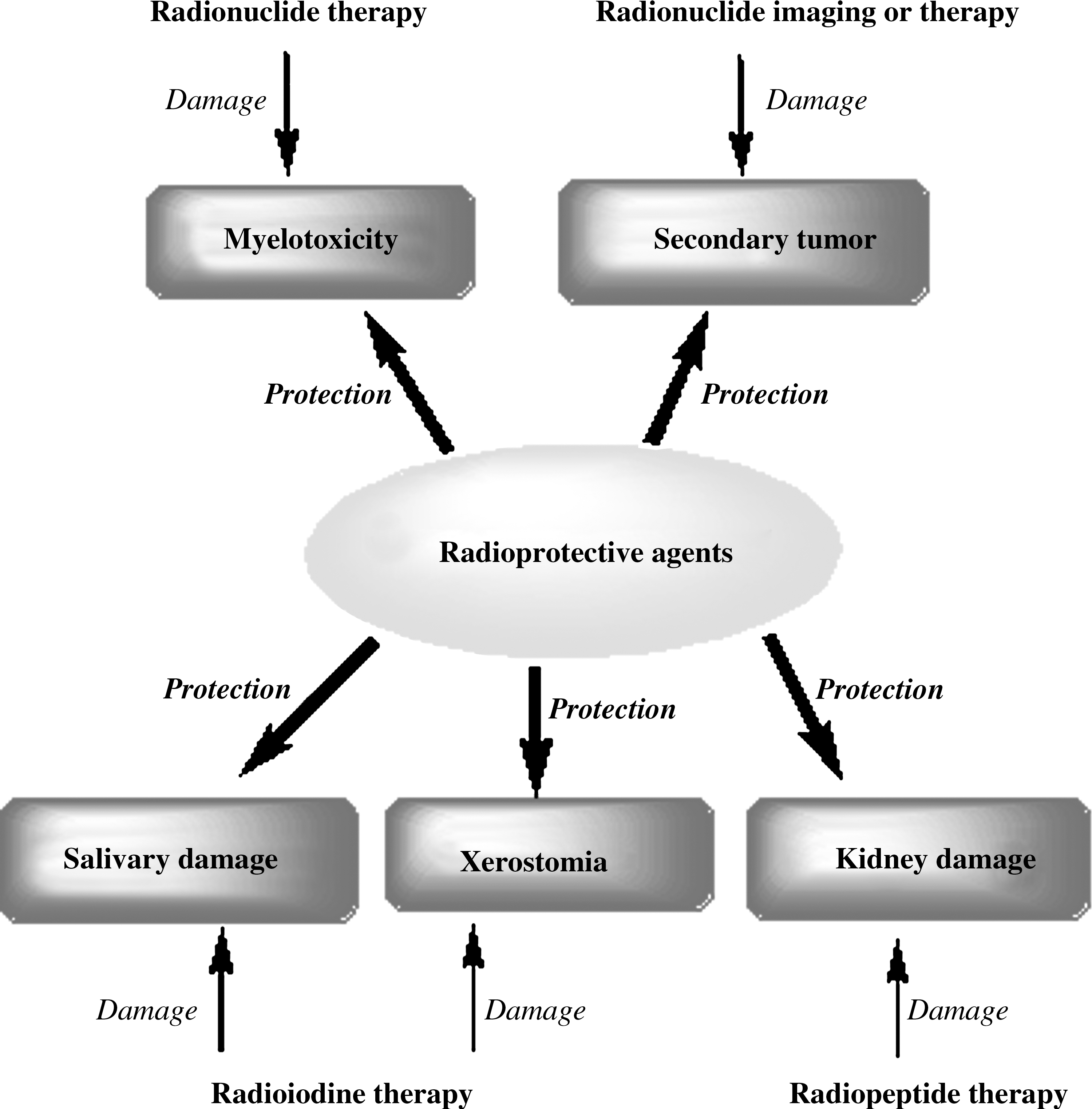
Radiopharmaceuticals induce side-effects under diagnostic or therapeutic application in patients. The main organs damaged are shown in oblongate boxes for the purpose of each radionuclide therapy. Radioprotective agents can protect organs from damage by different mechanisms. Further details are given in the text.
Selective Protective Effects
Xerostomia and salivary gland damage
Amifostine is the most powerful radioprotective drug in the class of thiol-containing compounds. It has been used in clinical trials and is approved by the FDA as a radio- and chemoprotector. 3,4 Chemoprotective agents are compounds that prevent side-effects induced by anticancer and chemical hazardous. Amifostine is a prodrug that is dephosphorylated by membrane-bound alkaline phosphatase to its pharmacologically active metabolite. It enters the cells, binds to oxygen and hydroxyl free radicals, and detoxifies the potentially damaging molecules produced by radiation. Although amifostine increases survival rates in mice (30-day lethality model), 25 it also protects patients from xerostomia during radiotherapy with external beam. There are several reports demonstrating protective effects on salivary gland function by amifostine in patients treated with radioiodine therapy. In patients who were treated with 500 mg/m2 of amifostine intravenously prior to a high dose of radioiodine treatment, salivary gland function was not significantly reduced, and xerostomia did not occur. Parenchyma damage in salivary glands induced by a high dose of radioiodine therapy can be reduced significantly by amifostine. 26 –29 The protective effect of amifostine was also observed in rabbits treated with this drug for parenchyma damage in salivary glands induced by high doses of radioiodine therapy. 29 While these findings are promising, further studies are needed to establish the protective effects of amifostione on salivary damage induced by radiopharmaceutical with therapeutic effects.
Pilocarpine hydrochloride is mainly a nonselective muscarinic agonist with mild β-adrenergic action and has a broad range of pharmacologic properties. These properties include increased secretion from the exocrine glands (i.e., the sweat, salivary, and intestinal glands), which reduces the feeling of dry mouth in patients with preserved exocrine tissue. 30 Pilocarpine has been shown to reduce the severity of salivary dysfunction and associated oral symptoms during radiation therapy. 31 However, Gornitsky et al. found no rescuing effects of pilocarpine to salvage salivary gland function during radiation therapy of patients. 32 Few studies have examined the efficacy of pilocarpine on salivary gland damage due to radioiodine therapy for thyroid cancer while being administrated before 131I therapy. Silberstein found that pilocarpine had no significant effect on the prevalence of sialadenitis, stomatitis, xerostomia, or dysgenusia in patients undergoing 131I therapy. 33 Pilocarpine was administered during radioiodine therapy in order to promote the discharge of iodine from the gland and to reduce the absorbed dose by reducing the required time to half, and a nonsignificant trend of reduced salivary gland side-effects was found. 34 The effects of short-term usage of pilocarpine treatment were investigated on salivary gland impairment in patients following radioiodine treatment for thyroid cancer. Pilocarpine administration produced a short-term increase in salivary output, along with negligible side-effects. 30 However, this study utilized only 5 patients. Considering the controversial studies on the protective effects of pilocarpine in salivary gland impairment, it is necessary to perform further studies with a larger number of patients (Fig. 2).
Nakada et al. showed that lemon candy used in close temporal proximity to 131I administration resulted in an enhancement of side-effects on subsequent salivary gland function. Therefore, lemon candy should not be given until 24 hours postradioiodine therapy. 35
Myelotoxicity
Bone marrow is the primary dose-limiting organ in radionuclide therapy or for potential use in radioimmunotherapy and radiopeptide therapy. 131I-MIBG is used for neuroblastoma treatment and the primary toxicity of 131I-MIBG is myelosuppression, particularly thrombocytopenia. 36,37 Thirty-six percent (36%) of patients who are treated with 131I-MIBG experience myelosuppression. Greater activity per kilogram of 131I-MIBG administration is correlated with greater hematotoxicity. Prominent thrombocytopenia is more common than neutropenia due to a selective uptake of 131I-MIBG by platelets and, possibly, mature megakaryocytic as well.36131I-MIBG should be used in combination with other therapies earlier in the course of the disease, with appropriate hematopoietic support for bone marrow recovery, such as platelet transfusion, red blood cell transfusion, and hematopoietic stem cell transplantation. In patients who received a single dose of 177Lu-labeled J591 monoclonal antibodies, thrombocytopenia was shown to occur and to be dose dependent. However, multiple fractioned dosing of this radiopharmaceutical produced lower hematologic toxicity, compared with a single dose. 36 The dose limit for myelotoxicity was found to be 2.59 GBq/m2 for 177Lu-J591 and lower for 90Y-J591, at a dose of 0.65 GBq/m2. 38 For a person with a body surface area of 2.0 m2, 177Lu-J591 (2590 MBq/m2) would deliver approximately 164 cGy to the bone marrow, compared with 90Y-J591 (647.5 MBq/m2), which would deliver 118 cGy to the bone marrow. 39 Based on blood radioactivity, the radiation dose (mGy/MBq) to bone marrow was 3 times higher with 90Y than 177Lu; however, 90Y-J591 may be less stable in vivo, so higher amounts of free 90Y may localize in the bone. 39 Administration of [177Lu-DOTA, try]octreotate to rats was shown to reduce white blood cell and platelet counts in rats treated with single doses of 555 or 278 MBq or with two weekly cycles of 278 MBq. 40 Not surprisingly, dose fractionation with long intervals resulted in significantly higher blood cell counts than dose fraction with a 1-day interval. 40 There are few studies showing the protective effects of drugs on recovery of myelotoxicity when induced by radionuclide therapy. The myeloprotective potential of amifostine was investigated in rabbits that received high doses of 153Sm-EDTMP (ethylenediaminetetramethylene phosphonate) or 186Re-HEDP (hydroxyethylidene diphosphonate) before therapy. Amifostine treatment was readministered every 3–5 days for a period of 8 weeks postradionuclide therapy. Amifostine was found to have a significant cytoprotective effect on platelets in rabbits treated with both radionuclides. Moreover, a single administration of amifostine 10–15 minutes prior to radionuclide therapy clearly reduced cytotoxic effects on platelets, despite the significant radiation exposure of bone marrow cells caused by the radiopharmaceuticals affixed to the bone marrow matrix, 41 though amifostine had no protective effect on leukocyte counts that were reduced by radionuclide therapy. 41 Also, a selective cytotoxic effect on leukocytes has to be observed for amifostine in combination with 186Re-HEDP. 41 Further, significantly reduced bone uptake of 153Sm-EDTMP and 186Re-HEDP was found in amifostine-treated animals, so the researchers did not recommend it for general use in patients undergoing radionuclide therapy of painful bony metastases. 41,42 There are documented studies showing that amifostine has myeloprotective effects in radiation therapy and chemotherapy. 43,45 Further studies are needed in animal models to investigate the efficacy of amifostine on myelotoxicity induced by other radionuclide therapies, such as radiopeptide therapy. Protective and therapeutic drugs that affect proliferation and production of bone marrow cells can be useful for treatment of side-effects involving hematopoiesis. It is necessary to evaluate the efficacy of these agents following radionuclide therapy in animal models (Fig. 2).
Kidney toxicity
Peptide-receptor radionuclide therapy of somatostatin receptor-positive tumors is currently being performed with using 1,4,7,10-tetraazacyclodode-can-N,N′,N″,N″′-tetraacetic acid (DOTA)-chelated somastatine analogs. These include [DOTA, Tyr] octreotate (DOTA-Tate), with 90Y, 177Lu, and 111In radioisotopes, which have shown great potential in radionuclide therapy.
45
–48
Kidney injury is the main dose-limiting factor of this peptide. Once filtered and rapidly cleared from circulation by glomeruli, these peptides are reabsorbed and retained in the proximal tubular cells. After reabsorption, the radiopeptide is translocated into the lysosomal apparatus. Uptake of these radiolabeled peptides by the tubules diffuses to the immediate area, in addition to neighboring glomeruli, causing irreversible nephrosclerosis and kidney damage.
45,48
–52
With success of this therapy, the aim is to deliver maximum radiation doses to the tumor while maintaining a safe margin for the kidney. Therefore, it is necessary to use methods for reducing renal radioactivity uptake after radiopeptide injection. Preclinical and clinical studies have shown the potential protective effects of the coinfusion of basic amino acids through competition with tubular uptake of the labeled somatostatine analog.
53,54
Cationic amino acids are able to inhibit tubular uptake of filtered peptides. By this mechanism, amino acids reduce reabsorption and retention of radiolabeled peptide in the proximal tubular cells. Administration of mixed amino acids (
Breeman et al. showed that administration of diethylenetriaminepentaacetic acid (DTPA) prior to intravenous admin-istration of 177Lu-DOTA-tyr(3)-octreotate (177Lu-DOTATATE) reduced uptake by epiphyseal plates, increased rapid renal clearance of the formed 177Lu-DOTA, and also reduced accumulation of 177Lu+3 in rat kidney. 48 Amifostine was evaluated as a protective agent during administration of the radiolabeled peptide, 177Lu-DOTA, in rats. Administration of 200 mg/kg of amifostine 30 minutes prior to radionuclide therapy, followed by 25 mg/kg subcutaneously once-daily for 7 days after therapy, largely inhibited the rise in creatinine and the level of proteinuria. However, amifostine did not inhibit the impairment of histologic kidney damage with doses of 555 MBq of 177Lu-DOTA. With the dosage of 278 MBq, proteinuria and histologic damage significantly improved with amifostine treatment. The mechanisms of action by which lysine and amifostine protect kidneys are different. Lysine inhibits the reabsorption of radiolabeled peptide in the proximal tubules, whereas amifostine mitigates oxidative stress and DNA damage induced by radiation (Fig. 2). 56 Hemoglobin concentration was low in the 555-MBq 177Lu-DOTA-treated rats. Amifostine and lysine treatment significantly improved hemoglobin levels. 56 Injection of 0.15 mg/g dimercaptosuccinic acid (DMSA) 30 minutes after the administration of 177Lu-DOTA-tate reduced kidney retention of radiolabeled peptide by 15.6% at 72 hours in rats, while not affecting uptake in other organs. Administration of dimercaptosuccinic acid (DMSA) prior to the 177Lu-DOTATATE chelated the Lu+3. Specifically, the Lu+3 was chemically bound to the DMSA residing in the kidneys, so the kidney uptake and consequent kidney damage were increased. The reduction in renal uptake was observed at 24 and 72 hours postinjection of radiolabeled peptides. 46
Non Selective Protective Effects
Ionizing radiation induces cell damage in patients undergoing nuclear medicine treatment similar to other medical practices, such as radiotherapy and radiology, but the dose of ionizing radiation is lower in nuclear medicine, compared with radiotherapy. Moreover, a high dose of ionizing radiation induces acute side-effects and damage to critical organs, such as hematopoietic and gastrointestinal organs. Low doses of ionizing radiation cause DNA damage and chromosomal breaks, resulting in chronic diseases, such as cancer. Many reports show that synthetic and natural protective compounds are capable of reducing DNA and cellular damage induced by ionizing radiation. 2 These agents may be suitable for use in patients for nuclear medicine purposes due to cell damage induced by gamma-rays (Fig. 1). Thiol synthetic compounds assessed comprehensively as radioprotective agents reduce acute side-effects, such as mortality, induced by ionizing irradiation. There are several reports indicating that amifostine reduces DNA and chromosome damage from exposure to low doses of gamma-rays in animal and human models. 57 –59 WR-2721 (amifostine) reduced genotoxicity in mouse bone marrow induced by 2 Gy of gamma-rays by 2.85-fold, compared with irradiated control mice. 57 Amifostine reduced DNA damage induced by gamma irradiation in human lymphocytes when treated in vivo or in vitro. 58,60 These results showed that amifostine reduces side-effects and DNA damage from gamma rays when cells are exposed to low doses of γ-rays. Captopril is a thiol-containing drug that is used as an antihypertensive drug. Hosseinimehr et al. has shown that low dose (25 mg/kg) administration of this drug to mice significantly reduced micronuclei induced by gamma irradiation at a dose of 2 Gy by 57%. 61 Although the initial development of radioprotective agents led to the discovery of effective synthetic thiol compounds, the side-effect profile of these agents has necessitated the search for natural compounds that are more effective and less toxic. Several medicinal plants that were evaluated for their radioprotective efficacy have shown protective capabilities against the damaging effects of ionizing radiation. Plant products hold various pharmacologic properties and can be offered as a major strategy for finding new drugs. The proposed radioprotective efficacy of plant extracts is based on the large number of active constituents, such as antioxidants and immunostimulants. 62,63 These plants protect against DNA damage and chromosomal aberrations induced by gamma-rays.
Citrus extract has been shown to mitigate genotoxicity induced by gamma irradiation when administrated 1 hour before gamma irradiation. 64 Hawthorn fruit extract, at a dose of 100 mg/kg, reduced the frequency of micronuclei induced by gamma irradiation (2 Gy) in mouse bone marrow cells. 64 Other herbal medicines have been evaluated for radioprotective effects in animal models, including Hippohae rhamnoides, Abana, Liv 52, Trinospora cardifolia, and Panax ginseng. 62,63,66 One strategy is to find the most powerful radioprotective compound from a natural source. Flavonoids, for example, are a family of polyphenolic compounds found in fruits and vegetables. These compounds exhibit strong antioxidant properties. The radioprotective effects of flavonoids, such as hesperidin, orientin, vicenin, naringin, querectin, and rutin, were investigated in the genotoxicity induced by irradiation in mouse bone marrow cells. These flavonoids significantly protected against genotoxicity induced by gamma irradiation in mouse bone marrow cells. 57,67 –69 Antioxidant activity is the main mechanism proposed for the radioprotective effect of these natural products. Melatonin is a hormone produced by the pineal gland and exhibits antioxidant activity. Several studies have shown that melatonin has radioprotective effects in animal and in human lymphocytes maintained in vitro. 70,71 Administration of a single oral dose of melatonin (300 mg) to healthy human volunteers has been shown to reduce the frequency of chromosomal aberrations induced by irradiation in human cultured lymphocytes. 72 Although many natural compounds have been investigated as radioprotective agents, mostly assessed in animal models, it is necessary to support their potential use in patients or healthy humans for protective effects. These natural compounds have shown lower effets, compared with thiol-synthetic compounds, for radioprotection against mortality induced by gamma irradiation. 2 Nevertheless, these compounds have shown excellent protection at low to medium doses of gamma irradiation. For example, hesperidin and hawthorn extract show similar efficacy, when compared with amifostine in radioprotective effect. 63,64 With respect to the low toxicity and side-effects, these agents will be designated as candidates for potential radioprotective use in patients undergoing nuclear medicine imaging or therapy and the personnel who administer such imaging or therapy. It should be noted that most of these compounds were assessed in normal mice or human lymphocytes; therefore, it is necessary to study the effects of these agents on distribution of radiopharmaceuticals also for imaging purposes or selective protection in normal organs, compared with tumor cells. Amifostine protected normal cells, and not tumor cells, against side-effects induced by gamma irradiation in patients undergoing radiotherapy with external beam. 3,4
Immunomodulators can stimulate growth, differentiation, and proliferation of hematopoietic progenitor and stem cells. In this way, these agents may protect, repair through enhanced production of bone marrow cells, and circulate granulocytes, lymphocytes, and platelets. 2,73,74 These agents may be useful as radiopharmaceuticals in therapies that involve bone marrow impairment and suppression.
Conclusions
Protecting patients and personnel during exposure to ionizing radiation is of extreme importance when using radiopharmaceuticals for imaging and therapeutic purposes in nuclear medicine, because these drugs emit gamma-rays or beta-particles that induce DNA and cell damage. Secondary tumors are the most common side-effects of these treatments, followed by DNA damage induced by at least low or medium doses of ionizing radiation. Because acute syndromes are usually not observed in patients or personnel in nuclear medicine, acute hematopoetic syndrome may occur while using radioiodine and radiopeptide therapy. There are two strategies for potential use of radioprotective agents in patients. First, radioprotective agent use in patients with specific therapy, such as amifostine, reduces mocusitis and salivary gland damage induced by radioisotope in radioiodine therapy in patients. Amino acids and Gelofusine are able to inhibit tubular uptake of filtered peptides and reduce kidney damage induced by radiolabeled peptide therapy. Second, radioprotective agents with antioxidant activity reduce chromosomal aberration induced by gamma- or beta-rays. Antioxidants, such as vitamin E, flavonoids, and herbal medicine, are included in this category. These agents, administered prior to exposure to ionizing radiation, scavenge free radicals produced by ionizing radiation in the biologic system. These agents are highly beneficial for patients and personnel, prior to encounter with radioisotopes or gamma-rays during their treatment or practice. Natural products, in the form of food supplements, are helpful for personnel and patients who are exposed to ionizing radiation. Further research is needed in order to assess the effect of radioprotective agents on the distribution of radiopharmaceuticals in normal and tumor cells to benefit patients undergoing nuclear medicine.
Footnotes
Disclosure Statement
No competing financial interests exist.