
Abstract
The aim of this study was to investigate the underlying mechanisms associated with fluorine-18 fluorodeoxyglucose (F-18 FDG) uptake in an incidentally detected thyroid cancer during nonthyroid cancer evaluation. Among 92 patients (10 men and 82 women; mean age, 56.2 ± 10.9 years; age range, 26–78 years) with focal thyroid FDG uptake during nonthyroid cancer evaluation, 14 patients with cytologically confirmed papillary thyroid cancer were included. For semiquantitative analysis, the maximal standardized uptake value was calculated. Immunohistochemical studies were performed for hypoxia inducible factor 1 alpha (HIF1α), HIF2α, glucose transporter 1 (GLUT1), GLUT3, carbonic anhydrase IX (CA-IX), hexokinase type II (HK II), and vascular endothelial growth factor (VEGF). The significant findings of this study were as follows: (1) a lack of HIF1α and HIF2α expression; (2) low-degree expression of GLUT1 (1 patient), GLUT3 (5 of 14 patients), HK II (3 of 14 patients), and CA-IX (1 patient); and (3) high degree expression of VEGF (all 14 patients). The data presented in this study indicate that F-18 FDG uptake in incidentally detected thyroid cancer was not related to hypoxia-induced upregulation of GLUT1, GLUT3, CA-IX, and HK II. Ki-67 expression was not associated with F-18 FDG uptake. However, all incidentally detected thyroid cancers showed a high degree of expression of VEGF.
Introduction
In the United States, ∼37,340 new cases of thyroid cancers are diagnosed each year and the estimated number of deaths in 2008 was 1590. 1 Fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (F-18 FDG PET/CT) has emerged as a significant molecular imaging technique in clinical oncology and cancer research. 2 –4 Some studies have shown the value of F-18 FDG PET/CT in the follow-up of well-differentiated thyroid cancers, especially in patients with elevated serum thyroglobulin and a negative iodine scan. 5 –7 Apart from the diagnostic capability, F-18 FDG PET has an independent prognostic power in patients with thyroid cancer. 8
It is generally accepted that cancer cells have increased rates of glucose metabolism compared with normal cells. 9 The cellular mechanism underlying the increased F-18 FDG accumulation in cancer cells is due to a higher rate of glucose transport across the cell membrane 10 in addition to a higher rate of phosphorylation coupled with diminished rates of dephosphorylation of intracellular phosphorylated glucose. Although a number of mechanisms have been suggested for the increased glucose utilization in cancer cells, glucose transporter (GLUT) is considered to be one of the most important factors for increased glucose utilization. 11
Hypoxia is also known to be an important regulator of tumor angiogenesis and growth. Tissue hypoxia evokes adaptive responses in the affected cells, largely through the hypoxia inducible factor (HIF). HIF1 can increase the rate of glucose uptake, primarily through the induction of the facilitative GLUTs (GLUT1 and GLUT3). 12,13 Also, hexokinase types I and II (HK I and HK II) can be induced by HIF1, but it appears that HK II is more important for modifying glucose during hypoxic stress. 14 Tissue hypoxia can thus be measured by endogenous hypoxia markers, such as HIF1α, HIF2α, GLUT1, GLUT3, and carbonic anhydrase IX (CA-IX). 15,16
This study hypothesizes that measurement of these endogenous markers of hypoxia could provide a possible mechanism of F-18 FDG uptake in incidentally detected thyroid cancers. Also, there are no studies documenting the mechanisms of F-18 FDG uptake in these cancers. The aim of this study was to define the underlying mechanisms associated with F-18 FDG uptake in incidentally detected thyroid cancers.
Methods
Patients
Ninety-two (92) patients (10 men and 82 women; mean age, 56.2 ± 10.9 years; age range, 26–78 years) with focal thyroid FDG uptake during F-18 FDG PET/CT whole-body scanning for nonthyroid cancer evaluation were included in the study. Among these 92 patients, 14 patients with cytologically confirmed papillary thyroid cancer were included for the immunohistochemical studies. All 14 patients had papillary thyroid cancer and had undergone a total thyroidectomy (mean age, 52.1 ± 10.3 years; age range, 26–70 years; 12 women and 2 men). The primary underlying cancers were breast cancer (7 patients [50%]), cervical cancer (3 patients [21.5%]), colon cancer (2 patients [14.3%]), gastric cancer (1 patient [7.1%]), and thymic cancer (1 patient [7.1%]). At the time of initial presentation, the cancer stages were T1 (n = 3), T3 (n = 9), T4a (n = 2), N0 (n = 9), N1a (n = 3), N1b (n = 2), and M0 (n = 14). The mean thyroid cancer size was 1.31 ± 0.71 cm (range, ∼0.5–3.4 cm). The patient characteristics are summarized in Table 1. Ethical approval for this study was obtained from the Research Ethics Committee of our institute. Written consent was obtained from all the patients.
F-18 FDG PET/CT
An F-18 FDG PET/CT image was obtained with a dedicated PET/CT scanner (Gemini; Philips), consisting of a dedicated germanium oxyorthosilicate full-ring PET scanner and a dual slice helical CT scanner. Standard patient preparation included at least 8 hours of fasting and a serum glucose level lower than 120 mg/dL before F-18 FDG administration. PET/CT imaging was performed at 60 minutes after injection of F-18 FDG. Sixty (60) minutes after administration of F-18 FDG, a low-dose CT (30 mA s, 120 kV) covering the area from the base of the skull to the proximal thighs was performed for the purpose of attenuation correction and precise anatomic localization. Thereafter, an emission scan was conducted in the three-dimensional mode. The mission scan time per bed position was 3 minutes, and nine bed positions were acquired. PET data were obtained using a high-resolution whole-body scanner with an axial field view of 18 cm. The average total PET/CT examination time was 30 minutes. After scatter and decay correction, PET data were reconstructed iteratively with attenuation correction and reoriented in axial, sagittal, and coronal slices. The row action maximum-likelihood algorithm was used for three-dimensional reconstruction.
F-18 FDG PET/CT analysis
The F-18 FDG PET/CT scans were reviewed by experienced nuclear physicians blinded to the results of other imaging modalities and pathology. The medical records of treatment regimens, other medical imaging commodities, and fine-needle aspiration biopsies were reviewed and analyzed. The PET/CT images were independently reviewed by two experienced nuclear physicians and any disagreement was resolved by consensus. To calculate maximal standardized uptake value (SUVmax), manually defined circular regions of interest were drawn on the attenuation-corrected emission images throughout axial planes in which suspicious lesions could be delineated.
Immunohistochemistry
Surgically resected specimens were immediately fixed in 10% buffered formalin (pH 7.0). All sections containing both tumor and surrounding thyroid tissue were embedded in paraffin, and serial sections (4 μm) were cut from a selected, paraffin-embedded tissue block. For pathologic diagnosis, one of these sections was stained with hematoxylin and eosin. The other sections were used for immunohistochemistry. Sections (4 μm) from paraffin blocks were transferred to poly-
After an appropriate antigen retrieval procedure, primary antibodies were applied to the sections. Antibodies against Glut-1 (rabbit polyclonal antibody; Dako), Glut-3 (rabbit polyclonal antibody; Abcam), and Ki-67 (mouse monoclonal antibody; Dako) were incubated with the tissue sections at room temperature for 1 hour. Antibodies against HIF-1α (mouse monoclonal antibody; Novus), HIF-2α (mouse monoclonal antibody; Novus), VEGF (rabbit polyclonal antibody; Santa Cruz Biotechnology), CA-9 (rabbit polyclonal antibody; Novus), and HK II (rabbit polyclonal antibody; Lifespan) were incubated with the sections overnight at 4°C. Immunohistochemical procedures were performed using a Dako Envision plus kit for HIF-1α and HIF-2α and a Biotin-free Catalyzed Amplification System II (K1497; Dako). The reaction products were visualized by exposing sections to 3,3′-diaminobenzidine. Nuclei were lightly counterstained for about 20 seconds with Mayer's hematoxylin. Sections were then mounted in diluted malinol after the application of Universal Mount (Dako). In each staining batch, appropriate positive control specimens were used.
Scoring of immunohistochemistry
With light microscopy, all the tissue sections were scored semiquantitatively considering the proportion of the cells showing immunoreactivity among whole tumor cells. In each analysis, the percentages of strongly immunoreactive tumor cells in total tumor cells were visually analyzed in several lower fields (original magnification, 10 × 10) covering the entire specimen, and the average percentage was calculated and scored on four-point scales (negative, <10%: 1+; 10%–25%: 2+; 26%–50%: 3+; and >50%: 4+), with the exception of Ki-67. For Ki-67 antibody, the labeling index was measured as the percentage of nuclear immunoreactive cells among at least 1000 tumor cells.
Statistical analysis
Data were expressed as the mean ± standard deviations. The statistical differences of SUVmax according to the expression of biological variables were assessed using the Mann–Whitney U-test. Pearson's correlation analysis was used to determine the relationships between SUVmax and thyroid cancer size. Spearman's rank correlation analysis was used to determine the relationships between biological variables and SUVmax. Statistical significance was defined as a p-value of <0.05.
Results
Figure 1 illustrates the representative cases of immunohistochemical staining results of this study.
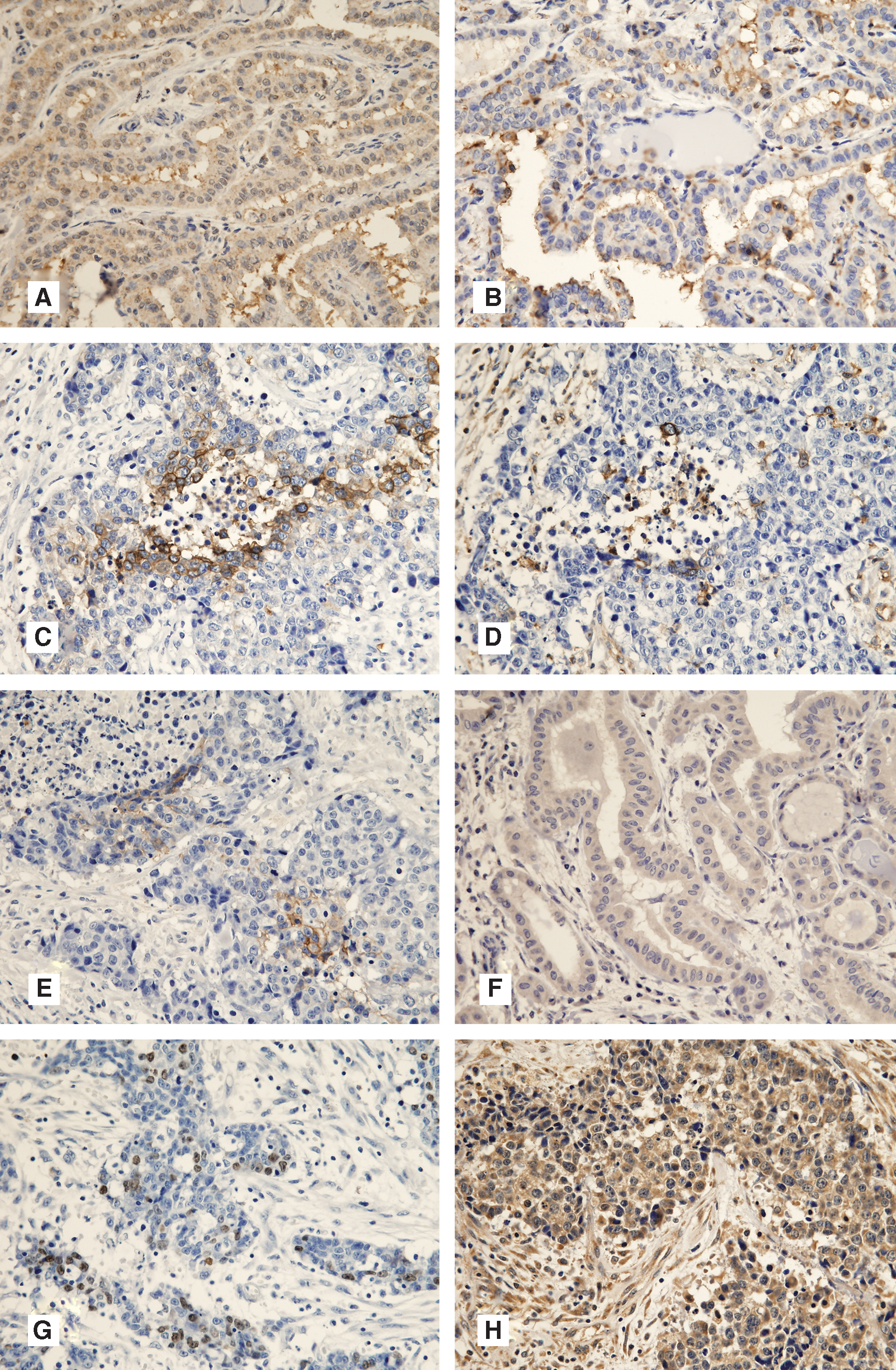
Immunohistochemical staining representing the expression profiles for various molecules. Cytoplasmic expression of HIF1α (
F-18 FDG PET/CT and immunohistochemical results
Table 2 summarizes the immunohistochemical results of 14 incidental thyroid cancers together with SUVmax. Notable findings of this study were as follows: (1) a lack of HIF1α and HIF2α expression; (2) a low degree expression of GLUT1 (1 patient), GLUT3 (5 of 14 patients), HK II (3 of 14 patients), and CA-IX (1 patient); and (3) a high degree expression of VEGF (all 14 patients).
SUVmax, maximal standardized uptake value; HIF1α, hypoxia inducible factor 1 alpha; HIF2α, hypoxia inducible factor 2 alpha; GLUT1, glucose transporter 1; GLUT3, glucose transporter 3; HK II, hexokinase type II; CA-IX, carbonic anhydrase-IX; VEGF, vascular endothelial growth factor.
Table 3 shows the statistical differences between SUVmax and biological variables. SUVmax did not show any statistical difference according to the expressions of the biological variables.
SUVmax, maximal standardized uptake value; HIF1α, hypoxia inducible factor 1 alpha; HIF2α, hypoxia inducible factor 2 alpha; GLUT1, glucose transporter 1; GLUT3, glucose transporter 3; HK II, hexokinase type II; CA-IX, carbonic anhydrase-IX; VEGF, vascular endothelial growth factor; NA, not accessible.
Table 4 demonstrates the correlations between SUVmax and different biological markers. The biological markers did not show any statistically significant correlation with the SUVmax of incidentally detected thyroid cancers. Only the size of the cancer had a statistically significant correlation with SUVmax (r = 0.6343, p = 0.0148; Fig. 2).
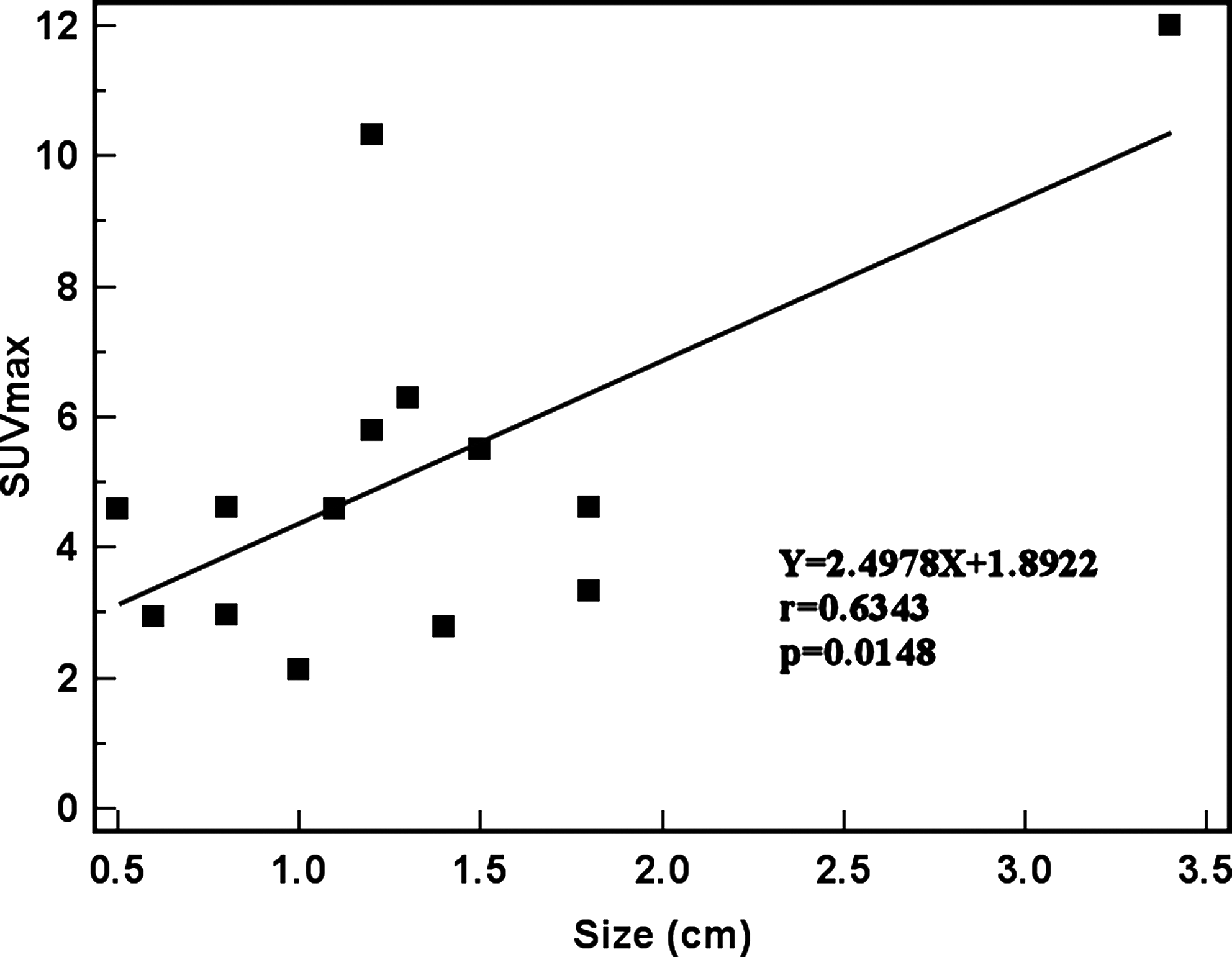
Correlation between cancer size and fluorine-18 fluorodeoxyglucose uptake. SUVmax, maximal standardized uptake value.
HIF1α, hypoxia inducible factor 1 alpha; HIF2α, hypoxia inducible factor 2 alpha; GLUT1, glucose transporter 1; GLUT3, glucose transporter 3; CA-IX, carbonic anhydrase-IX; HK II, hexokinase type II; VEGF, vascular endothelial growth factor; SUVmax, maximal standardized uptake value; NA, not accessible.
Discussion
The major findings of this study can be summarized as follows: thyroid cancers detected incidentally during F-18 FDG PET/CT evaluation for nonthyroid cancer patients showed, using immunohistochemical techniques, a lack of HIF1α and HIF2α expression, a low degree of expression of GLUT1, GLUT3, HK II, and CA-IX, and a high degree of expression of VEGF.
Few studies are available on the relationship between endogenous hypoxia markers and F-18 FDG uptake in cancer. A recent study showed that the uptake of F-18 FDG, as measured by the SUVmax, was associated with the expression of HIF1α and GLUT1, both of which were upregulated under hypoxic conditions. 17 Indeed, this study provided evidence that not only is hypoxia related to F-18 FDG uptake in vitro, but also in vivo it is associated with an increase in F-18 FDG uptake in nonsmall cell lung cancer. 17 However, the present study was unable to demonstrate any HIF1α and HIF2α expression and found very low-level expression of CA-IX in incidentally detected thyroid cancers. These findings suggest that incidentally detected thyroid cancer is not associated with hypoxic conditions and F-18 FDG uptake in these cancers may not be related to tumor hypoxia.
A recent study found that GLUT1 and GLUT3 are the most important GLUTs in thyroid tumor cells. 18 In particular, GLUT1 is more prevalent in less-differentiated cells, whereas GLUT3 expression is higher in well-differentiated cells. 18 They also reported a similar pattern of expression for GLUT1, but not GLUT3, in human thyroid tumors. 18 The present study found GLUT1 expression in 1 patient (7.1%) and GLUT3 expression in 5 patients (35.7%). However, there was no correlation between F-18 FDG uptake and GLUT expression. Also, GLUT expression appeared to be independent of the endogenous markers of hypoxia (HIF1α, HIF2α, and CA-IX). Similarly, another study investigated GLUT1 expression immunohistochemically in 86 thyroid cancer patients. 19 The authors concluded that GLUT1, p63, and p53 were not expressed in well-differentiated thyroid carcinomas, whereas GLUT1, p63, and p53 were usually expressed late in the course of thyroid tumor progression. These data strongly suggest that in anaplastic carcinomas, disruption of p53-mediated repression results in increased GLUT1 and p63 expression, and that this probably reflects the differential regulation of hypoxia-responsive pathways and basal/stem cell regulatory pathways. 19 Taken in conjunction with these results, the observations in the present study suggest that F-18 FDG uptake in incidentally detected thyroid cancers may not be related to GLUT, especially GLUT1 and GLUT3.
Very few studies have focused on the possible role of HK activity on F-18 FDG uptake in thyroid cancer. In a study conducted on 19 patients with suspected recurrent thyroid cancer, 13 patients were found positive on PET, and F-18 FDG uptake was associated with the expression of HK I. 20 In the present study, HK II activity was noted in 21.4% of the patients (3 of 14 patients); however, HK II expression and SUVmax did not have any correlation. Also, HIF1α and HIF2α activities did not exhibit any relationship with quantitative indices of F-18 FDG PET. These findings suggest that in incidentally detected thyroid cancer, there was no hypoxia-induced upregulation of HK II activity and that HK II activity did not contribute to the F-18 FDG uptake for this type of cancer.
Recently, several studies have documented the expression of VEGF in malignant thyroid cancers. 21,22 Another study showed that increased VEGF expression promotes thyroid cancer cell growth, lymph node metastasis, local invasion, and enhanced distant metastasis, whereas the inhibition of VEGF signaling results in suppression of tumor growth. 23 In the present study, strong expression of VEGF was noted in all incidentally detected thyroid cancers. However, the relationship between the expression of VEGF and markers of hypoxia (HIF1α and HIF2α) could not be defined. The association between GLUTs and VEGF in two human small-cell lung cancer lines has been investigated in an earlier study, 24 wherein co-upregulation of GLUT1, GLUT3, and VEGF was demonstrated, suggesting a modification of glucose kinetics by angiogenesis-related genes. However, in incidentally detected thyroid cancer, and contrary to the results presented in the earlier study, 24 the results indicate that F-18 FDG uptake may not be dependent on hypoxia-induced angiogenesis and that angiogenesis itself is an underlying mechanism of F-18 FDG uptake.
In the present study, SUVmax showed a significant correlation with cancer size. However, in smaller tumors (<1 cm in diameter), the F-18 FDG uptake was underestimated. This could be attributed to the partial volume effect, which is limited by scanner resolution. A recent report suggested that small-sized thyroid carcinomas may have lower SUVs, possibly due to partial volume effect. 25
Conclusion
The data presented in this study indicate that F-18 FDG uptake in incidentally detected thyroid cancer may not be related to hypoxia-induced upregulation of GLUT1, GLUT3, CA-IX, and HK II. Also, Ki-67 expression was not associated with F-18 FDG uptake. However, all incidentally detected thyroid cancers showed a high degree of expression of VEGF.
Footnotes
Acknowledgment
This work was supported for 2 years by a research grant from the Pusan National University.
Disclosure Statement
None of the authors of this study had any conflict of interest.