
Abstract
As a well-established single-modality approach for early-stage prostate cancer, transperineal interstitial permanent prostate brachytherapy (TIPPB) has gained increasing popularity due to its favorable clinical results. Currently, three isotopes, namely Cs-131, I-125, and Pd-103, are commercially available for TIPPB. This is the first study to systematically explore the dosimetric difference of these three isotopes for TIPPB. In total, 25 patients with T1-T2c prostate cancer previously implanted with I-125 seeds were randomly selected and replanned with Cs-131, I-125, and Pd-103 seeds to the prescription doses of 115, 145, and 125 Gy, respectively. The planning goals attempted were prostate Vp100 ∼ 95%, Dp90 ≥ 100%, and prostatic urethra Du10 ≤ 150%. The dosimetric parameters, as well as the number of seeds and needles required, were analyzed and compared. The mean homogeneity index (HI) was 0.59, 0.56, and 0.46 for Cs-131, I-125, and Pd-103 plans, respectively. The average Du10 was 124.6%, 125.7%, and 129.7%, respectively. The average rectum Vr100 was 0.19, 0.22, and 0.31 cc, respectively. In addition, the average number of seeds was 57.9, 63.0, and 63.7, and the average number of needles required was 31.6, 32.9, and 33.6 for Cs-131, I-125, and Pd-103 seeds, respectively. This study demonstrates that TIPPB, utilizing Cs-131 seeds, allows for better dose homogeneity, while providing comparable prostate coverage and sparing of the urethra and rectum, with a comparable number of, or fewer, seeds and needles required, compared to I-125 or Pd-103 seeds. Further biological and clinical studies associated with Cs-131 are warranted.
Introduction
Transperineal interstitial permanent prostate brachytherapy (TIPPB) has gained increasing popularity and developed rapidly over the past decade due to the advent of the transrectal ultrasound (TRUS) and template-guided technique. TIPPB has become a well-established and most frequently employed approach as a single modality for early-stage prostate cancer 1,2 and has replaced radical prostatectomy in some institutes due to the treatment's apparent high efficacy and low morbidity. It also plays an important role as part of a multimodality program for intermediate- and high-risk patients with prostate cancer.
TIPPB was generally performed with either I-125 or Pd-103 seeds before Cs-131 seeds became available commercially. The use of I-125 for low-Gleason-score tumors and Pd-103 for higher Gleason score tumors has been suggested, based on isotope dose rate and cell-doubling time observed in in vitro studies. 3 Cs-131 has been recently developed and introduced to the market, and approved by the U.S. Food and Drug Administration for TIPPB. Cs-131 is more attractive due to the shorter half-life and higher average energy emitted. It has the half-life of 9.7 days that is considerably shorter than those of the other two radionuclides commonly used in TIPPB, I-125 (59.4 days) and Pd-103 (17.0 days). Recent radiobiologic data suggest that isotopes of shorter half-lives may have more advantages in the treatment of prostate cancer, 4,5 especially for the tumors with a short potential doubling time (T p ). 6 Bostancic et al. reported that I-125 resulted in twice to three times the likelihood of a PSA (prostate-specific antigen) spike, compared with Pd-103, in hormone-naïve patients. 7 In addition, a shorter acting isotope also has advantage in terms of morbidity. Multiple investigators have reported that patients treated with Pd-103 had lower complication rates than those treated with I-125 and more rapid resolution of the urinary toxicity. 8 –11 But, Pd-103 generally involves the use of more seeds and needles, in comparison with I-125, and leads to significant increase in cost, time, and trauma to the patients, as well as more inhomogeneous dose distributions due to its lower average energy emitted. Actually, some primary results of recent studies have shown that the resolution of urinary symptoms occurred more rapidly with Cs-131, as compared with I-125. 12,13
Irrespective of the isotope used for implantation clinically, knowledge of the dosimetry of different isotopes is very important. Efforts to obtain an optimal dose distribution within the prostate and to the surrounding organs at risk are necessary for obtaining the optimal clinical outcomes and establishing appropriate standards of care. To our knowledge, there are few systematic studies on the dosimetric difference of the three isotopes, to date. The aim of this study was to compare the dosimetric differences of TIPPB plans by utilizing Cs-131, I-125, and Pd-103 seeds.
Materials and Methods
Patient selection and source modeling
We randomly selected 25 patients with T1-T2c (2002 American Joint Committee on Cancer clinical staging system) prostate cancer, previously implanted with I-125 seeds in our hospital, and replanned these patients with Cs-131 (model CS-1), I-125 (model 6711), and Pd-103 (model Pd-200) seeds, using the Prowess Brachytherapy 3.0 treatment planning system. Before the study, the treatment-planning system was commissioned for each source model. The dose-rate constant of 1.06 cGyh−1U−1 and half-life of 9.7 days were used for Cs-131 seeds. 14,15 The data of radial dose function and anisotropy function were taken from the results of Murphy et al.'s study. 16 The data of I-125 (model 6711) and Pd-103 (model Pd-200) were configured according to the revised American Association of Physicists in Medicine (AAPM) protocol in 2004 (AAPM TG43 U1). 17 The data of radial dose function and anisotropy function were taken from Tables 2, 3, 5, and 10 from Murphy et al. 16 for I-125 and Pd-103, respectively. The dose-rate constant was set to 0.965 cGyh−1U−1 and 0.686 cGyh−1U−1 for I-125 (model 6711) and Pd-103 (model Pd-200) respectively.
Structure contouring and treatment planning
The prostate, prostatic urethra, and anterior wall of the rectum were contoured on each axial transrectal ultrasound image obtained at 5-mm slices for intraoperative dosimetry, with no margin applied for planning target volume (PTV). For each case, three optimized treatment plans were generated by automatic peripheral loading with identical contours of structures by the same medical physicist. Based on the latest recommendation of the American Brachytherapy Society, 18 the consensus report from the Cesium Advisory Group, 15 and results of biologic modeling, 19 the prescribed doses were set to 115, 145, and 125 Gy for Cs-131, I-125, and Pd-103 seeds respectively. The seed strengths employed were 1.8, 0.5, and 1.8 U for Cs-131, I-125, and Pd-103 seeds, respectively. Planning criteria included the following dose-volume histogram (DVH) quality indices: Vp100 ∼95%, Dp90 ≥ 100%, and prostatic urethra Du10 ≤ 150%, where Vp100 is the percentage volume of the prostate that receives at least 100% of the prescribed doses, Dp90 is the minimum percentage dose received by 90% of the volume of the prostate, and prostatic urethra Du10 is the minimum percentage dose received by 10% of the contoured urethra volume that received the most doses. To minimize the bias due to planning variability, the geometric arrangement and number of seeds used were carefully tuned to achieve the required planning criteria for the DVH quality indices for all three isotopes.
DVH calculation
For the purpose of plan comparison, the following DVH quality indices were recorded: Vp100, Vp150, Vp200, Dp90, prostatic urethra Du30, Du10, Vu120, and Vr100, where Vu120 is defined as the percentage volume of the contoured urethra that receives at least 120% of the prescribed doses, and Vr100 is defined as the volume of contoured rectum that receives at least 100% of the prescribed doses. Vp100 and Dp90 were analyzed for the description of the prostate-dose coverage, Vp150, Vp200, and homogeneity index (HI) for dose homogeneity, Du30, Du10, and Vu120 for dose to urethra, and Vr100 for dose to rectum. HI was calculated as: [(Vp100-Vp150)/Vp100] (20).
Number of seeds and needles analysis
In addition to the DVH quality indices, the number of seeds and needles required for each plan were also recorded for the consideration of the treatment cost, implant time, and trauma to the patient. The differences in the mean number of seeds/cc and the mean number of needles for the 25 patients obtained from using different isotopes were analyzed.
Statistical analysis
A self-control analysis was performed to assess any difference among the three isotopes. To compare the three groups of plans, the results of Cs-131 plans were designed as the baseline and compared with those of the other two groups. A direct comparison of the dosimetric parameters between I-125 and Pd-103 plans was also performed. A paired two-tailed Student's t-test was used for data analysis. The threshold for statistical significance was p < 0.05. All data were analyzed by using Statistical Package for Social Science, version 13.0, software (SPSS, Inc., Chicago, IL).
Results
DVH calculation
The mean size of prostates was 33.3 cc (range, 13.0–66.1) for the 25 patients. Table 1 summarizes the effect of isotope selection on prostate DVH quality indices. Differences in Dp90 and Vp100 were small and insignificant for all the three isotopes, with the average Dp90 of 108.0%, 107.8%, and 108.9% and Vp100 of 95.5%, 95.3%, and 95.4% for Cs-131, I-125, and Pd-103 seeds, respectively.
HI, homogeneity index.
Differences in Vp150 and Vp200 were statistically significant, with Pd-103 showing the greatest increase in both values. As compared to I-125 and Pd-103, Cs-131 improved the dose homogeneity of the prostate. The average Vp150 decreased from 51.9% (Pd-103) and 42.1% (I-125) to 39.4% (Cs-131), and the average Vp200 decreased from 28.7% and 20.9% to 19.6%. The mean HI was 0.59, 0.56, and 0.46 for Cs-131, I-125, and Pd-103 plans, respectively.
Table 2 shows the effect of isotope selection on prostatic urethra and rectum DVH quality indices. For Du30, Du10, Vu120, and Vr100, there are no statistically significant differences for the three isotopes. However, Cs-131 showed the lowest values for all of them. The average Du10 was 116.6 (Cs-131), 117.4 (I-125), and 117.9 (Pd-103). The average Vu120 was 23.8%, 29.5%, and 26.9%, respectively. The average rectum Vr100 was 0.19, 0.22, and 0.31 cc for Cs-131, I-125, and Pd-103 plans, respectively.
Figure 1 shows the typical distribution of seeds and dose in a transversal slice, in which several isodose lines for three isotopes are shown in the same prostate midaxial plane. The three plans are all very conformal, and the isodose lines of the 100% prescribed dose provide good target coverage and minimal overlap with the rectum, with good sparing of the urethra. Compared with I-125 and Pd-103, Cs-131 resulted in smaller area with dose higher than 150% and 200% of the prescribed dose.
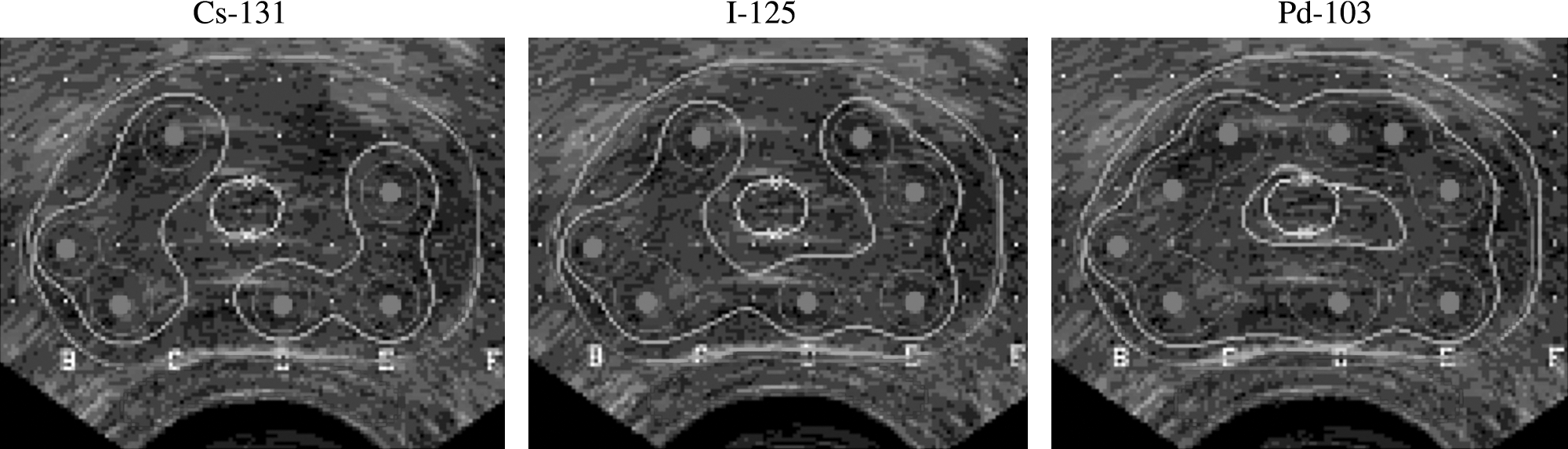
A typical central transverse slice showing the distributions of the seeds and dose for the three seed models studied. The isodose lines shown are 100%, 150%, and 200% of the prescription dose. Prostate, urethra, and anterior walls of the rectum are also shown. The radioactive seeds are marked with dots.
Number of seeds and needles analysis
In terms of the number of seeds and needles required, Cs-131 showed the lowest values for both of them. The differences between I-125 and Pd-103 were small and insignificant. The average number of seeds required decreased from 63.0 (I-125) and 63.7 (Pd-103) to 57.9 (Cs-131), and the average number of needles required decreased from 32.9 and 33.6 to 31.6, respectively. In general, an increase or decrease in the number of seeds/cc results in an increase or decrease in the number of needles required.
Discussion
This study demonstrates that Cs-131 improved the dose homogeneity of the prostate, and also the sparing of the urethra and rectum, but some differences are not statistically significant, while providing a comparable prostate coverage with a comparable number, or fewer, seeds and needles required, compared to I-125 or Pd-103 seeds. The differences were more significant between the Cs-131 and Pd-103 groups than those of the Cs-131 and I-125 groups.
As compared with I-125 and Pd-103, Cs-131 maintains the advantages of I-125 and Pd-103 seeds, in terms of radiation safety and rapid dose fall-off, because of its relatively low energy (29.4–34.4 keV). However, Cs-131 is slightly more penetrating due to the higher average energy emitted—30.4 keV versus 27.4 keV for I-125 (model 6711) and 20.8 keV for Pd-103. 21 Therefore, Cs-131 seeds can be geometrically distributed further from each other, and from the urethra and rectum, and sufficient margins may be obtained while limiting source placement to the capsule or close to the capsule. Sahgal et al. also found that Cs-131 resulted in a significantly lower prostate urethra D30, compared with I-125, although a slightly different seed activity, dose constraints, and planning method were used in their study. 22 No surprisingly, Cs-131 produces more homogeneous dose distributions and a somewhat better sparing of organs at risk. The same results were found in Sahgal et al.'s study in terms of Vp150, Vp200, and homogeneity index. 22 For the same reason, Cs-131 also required fewer seeds and needles to achieve the prescribed dose coverage. In this study, patients planned with Pd-103 had a higher dose to the urethra and rectum, because more seeds are needed adjacent to the urethra and rectum due to the limited penetration ability of Pd-103, whereas the disadvantage of less rapid dose fall-off of I-125 and Cs-131 can be overcome partially with judicious treatment planning. Pd-103 decays via electron capture to excited states of Rh-103, and emits photons with energies of 20.1 (82%) and 23.0 keV (18%) in the process of de-excitation via gamma emission and internal conversion. 17 The mean photon energy emitted by Pd-103 seeds would be approximately 21 keV, which is much lower than that of I-125 and Cs-131 photons.
Since the Vr100 of all the 25 patients were below the recommended 1.0 cc of developing rectum bleeding, 9 or even the Cesium Advisory Group recommended value of 0.5 cc, 15 the clinical significance needs to be further defined. A comparison of treatment plans revealed that Cs-131 plans required fewer needles and seeds for comparable seed strength. Similar results were found in previous studies, 3,6 when comparing the plans between I-125 and Pd-103.
Although the dose distribution is purely a function of the mean emission energy, the dosimetric advantage of Cs-131, as shown by this study, is also attributed to its short half-life. The prescription dose for Cs-131 is the lowest of the three in the attempt to create a biologically equivalent dose. Because the energy of Cs-131 and I-125 are similar, the main contributing factor to the difference between Cs-131 and I-125 is the prescription dose. The radiobiologic parameters governing the radiotherapy of prostate cancer are highly uncertain. However, most of the studies pointed to low α/β ratios for prostate cancer. 23,24 If a lower α/β ratio of 1.5 to 3.1 is used, the prescription dose for Cs-131 to give a true equivalent biological dose is likely to be lower, leading to greater dosimetric advantages than that revealed by this study.
It is also observed that given the 100% prescription dose covering the gross tumor volume, the volume of 150% of the prescription dose inside the prostate is the largest for Pd-103 and smallest for Cs-131. Merrick et al. also found Pd-103 implants had higher Vp150 and Vp200, although the clinical significance is not well defined as yet. 25 This fact raises another question on what a biologically equivalent dose is. Dose inhomogeneity in the prostate may not necessarily be a detriment. The larger “hot” volumes associated with Pd-103 may be one of the key reasons besides shorter half-life behind the observed better efficacies than I-125 for hormone-naïve patients. 7 Therefore, the dosimetric advantage of Cs-131 seeds revealed in this study may not translate to clinical advantage. Of course, considering of the factors of geometric uncertainties and prostate shrinkage after implant, the Cesium Advisory Group recommended that the prostate Vp150 should be ≤ 45% for Cs-131 seeds.
Last, the dose comparisons conducted by this study were based on static images. It is well known that during the first few weeks postimplantation, trauma-induced edema will cause the actual dose to deviate from the calculated doses before the implantation. 26 The effect of postimplant edema should be the most significant for Cs-131 seeds among the three sources, because most of the doses delivered by the Cs-131 seeds are during the period when the prostate is swollen. The half-life of Cs-131 seeds (approximately 9.7 days) is directly comparable to the average edema-resolution half-life (approximately 10 days) observed previously by Waterman et al. for I-125 implants. 27 It was found that conventional preimplant dosimetry error for Cs-131 implants was found to be similar to that of Pd-103 implants for typical edema characteristics (magnitude, < 100%; half-life, < 25 days), both of which are worse, compared to 125I implants. 28
Conclusions
In summary, from a standpoint of dosimetry, permanent prostate brachytherapy, utilizing Cs-131 seeds, allows for better dose homogeneity, while providing comparable prostate coverage and sparing of the urethra and rectum, with a comparable number of, or fewer, seeds and needles, compared to I-125 or Pd-103 seeds. The differences are more significant between Cs-131 and Pd-103 groups than those of Cs-131 and I-125 groups. Further biologic and clinical studies associated with Cs-131 are warranted to assess efficacy and morbidity.
Footnotes
Acknowledgments
The authors would like to thank Professor Cedric Yu, Ph.D. for his critical review and thoughtful suggestions of the manuscript for this article and we also would like to thank the prostate brachytherapy team at Peking University Third Hospital for their contributions to this work, in particular, Weiqiang Ran, from the Department of Ultrasound, and Yi Huang, from the Department of Urology.
Disclosure Statement
No competing financial interests exist.