
Abstract
Metaiodobenzylguanidine (MIBG), radioiodinated with 131I, has been available for 25 years. Its role in the United States is limited to diagnostic imaging, whereas its therapeutic application in patients with neuroendocrine tumors for whom surgical treatment would not lead to a cure, has been approved in Europe. 131I-MIBG treatments can be a valuable addition to the current gamut of treatment options for patients with metastatic neuroendocrine tumors, especially given the limited role for other systemic treatments, such as chemotherapy. There are basically two treatment strategies: one or two high-dose treatments or continuous low-dose treatments. 131I-MIBG could induce symptomatic relief in the vast majority of patients treated, both following high-dose treatment and low-dose maintenance treatment. Biochemical responses can be observed in about half of the patients, whereas radiographic responses are described in roughly one third of the patients. Several articles suggested a survival benefit to patients treated with 131I-MIBG. Side-effects of the treatment mainly consist of myelotoxicity, nausea, and hypothyroidism. Future developments are focused on the use of high-specific-activity 131I-MIBG in high doses. The role of 131I-MIBG in relation to other treatments remains to be established, although treatment 131I-MIBG seems to be at least as effective as other systemic treatments, with limited side-effects.
Introduction
Metaiodobenzylguanidine (MIBG) is a norepinephrine analog that, labeled with either 123I or 131I, has been used for the imaging of neuroendocrine tumors. In 1984, the therapeutic use of 131I-MIBG was first described in patients with pheochromocytoma. 1 In the same period, the first reports appeared on the use of this radiopharmaceutical in patients with neuroblastoma 2 and carcinoid. 3 During this 25-year period, many patients have been treated with 131I-MIBG, but it did not lead to a major breakthrough in the treatment of patients with metastatic neuroendocrine tumors. 131I-MIBG still has not been approved for therapeutic use in the United States and Canada, although it is available for treatment in Canada. In Europe, it has been approved for therapeutic use and is widely available for clinical use. Recently, the European Association of Nuclear Medicine (EANM) updated the guidelines for the therapeutic use of 131I-MIBG. 4 However, even in Europe, the role of 131I-MIBG for the management of metastatic neuroendocrine tumors is rather limited. In this article, we summarize the indications for use, other treatment options, dosing of the radiopharmaceutical, and side-effects.
Neuroendocrine Tumors in Adults
The majority of neuroendocrine tumors in adults consist of pheochromocytoma and paraganglioma, carcinoid, and medullary thyroid carcinoma. Pheochromocytoma and paraganglioma are tumors derived from secretory cells characterized by amine and amine precursor uptake and decarboxylation, either in the adrenal medulla (pheochromocytoma) or the paraganglia (paraganglioma). Both tumor types secrete catecholamines. Carcinoid tumors are derived from neoplastic proliferation of cells of the diffuse neuroendocrine system. These cells are ubiquitous throughout the gastrointestinal tract, urogenital tract, and bronchial epithelium. Most carcinoid tumors arise in the gastrointestinal tract, but about 30% occur in the bronchi. Medullary thyroid carcinoma is a tumor derived from C-cells in the thyroid gland. Like other cells of neuroectodermal origin, C-cells have an amine precursor uptake decarboxylase system. They produce calcitonin.
The primary management of neuroendocrine tumors is surgical, either curative in the case of limited disease, or debulking when metastatic disease is present. Possibilities for surgery should always be considered in the patient's management, given the lack of alternatives that are capable of inducing a cure. Patients with metastatic neuroendocrine tumors suffer most from effects caused by the tumor's hormones and metabolites, thus requiring a different approach for treating these tumors and a different way of evaluating the effect of treatment. The effect of systemic treatment in inducing an objective response, as assessed by radiologic techniques of measuring a reduction in tumor sizes, is limited. Therefore, focus is less on reduction of tumor volume, but more on reduction of symptoms, as evaluated by quality-of-life questionnaires or diaries, and reduction of the tumor's hormonal productivity, as evaluated by serial measurement of serum chromogranin A, urinary 5-hydroxyindoleacetic acid (5-HIAA) (in carcinoid), catecholamines (pheochromocytoma), or carcinoembryonic antigen (CEA) and calcitonin (medullary thyroid cancer).
Given the indolent nature of most neuroendocrine tumors, chemotherapy hardly plays a role. In classical midgut carcinoids, chemotherapeutic regimens generate short-lasting responses in less than 10% of cases. 5 Only in patients with more aggressive tumor types, such as endocrine pancreatic tumors and lung carcinoids, streptozotocin-based combinations, including 5-flourouracil and doxorubicin, or a combination of cisplatinum and etoposide, have generated objective responses. 5 In the case of rapidly progressive metastatic pheochromocytoma, combination chemotherapy with cyclophosphamide, vincristine, and dacarbazine could induce a partial remission in one third of patients, although of short duration. 6
In the case of expression of somatostatin receptors by the tumor, treatment with somatostatin analogs, such as octreotide or lanreotide, is currently considered the standard of care. These analogs are considered to reduce symptoms in the majority of cases and to inhibit tumor growth. 7 A recent study showed that long-acting sandostatin prolongs progression-free survival, when compared to placebo. 8 Somatostatin analogs can also be labeled with either 111In, 90Y, or 177Lu, in order to be used for the treatment of neuroendocrine tumors. A recent overview of the results of clinical studies using radiolabeled somatostatin analogs reported objective responses in 10%–30% of patients treated. 9
Interferon-alpha has been used for the treatment of metastatic carcinoid tumours since 1982. Its use can lead to a reduction of symptoms in about 70% of cases and a reduction of biochemical markers in approximately 40% of cases. 7 A reduction in tumor size is only observed in a small minority (10%–20%) of patients treated. 7
The newest development in the systemic treatment of neuroendocrine tumors is the evaluation of the use of tyrosine kinase inhibitors. The use of sunitinib in a group of 107 patients with carcinoid and pancreatic endocrine tumor led to an objective response in 17% of patients. 10 No mention was made of symptomatology or hormonal responses. In another study evaluating the use of imatinib in a heterogeneous group of 15 neuroendocrine patients, no objective responses were observed. 11
Therapeutic Use of 131I-MIBG
Not only catecholamine producing tumors take up MIBG, but carcinoid and medullary thyroid carcinoma can be MIBG-avid, too, in approximately 70% of cases. In order to assess the possibility of treatment with 131I-MIBG, diagnostic imaging with either 123I-MIBG or 131I-MIBG scintigraphy is warranted. In the case of MIBG-avidity, treatment with 131I-MIBG can be considered (Fig. 1).
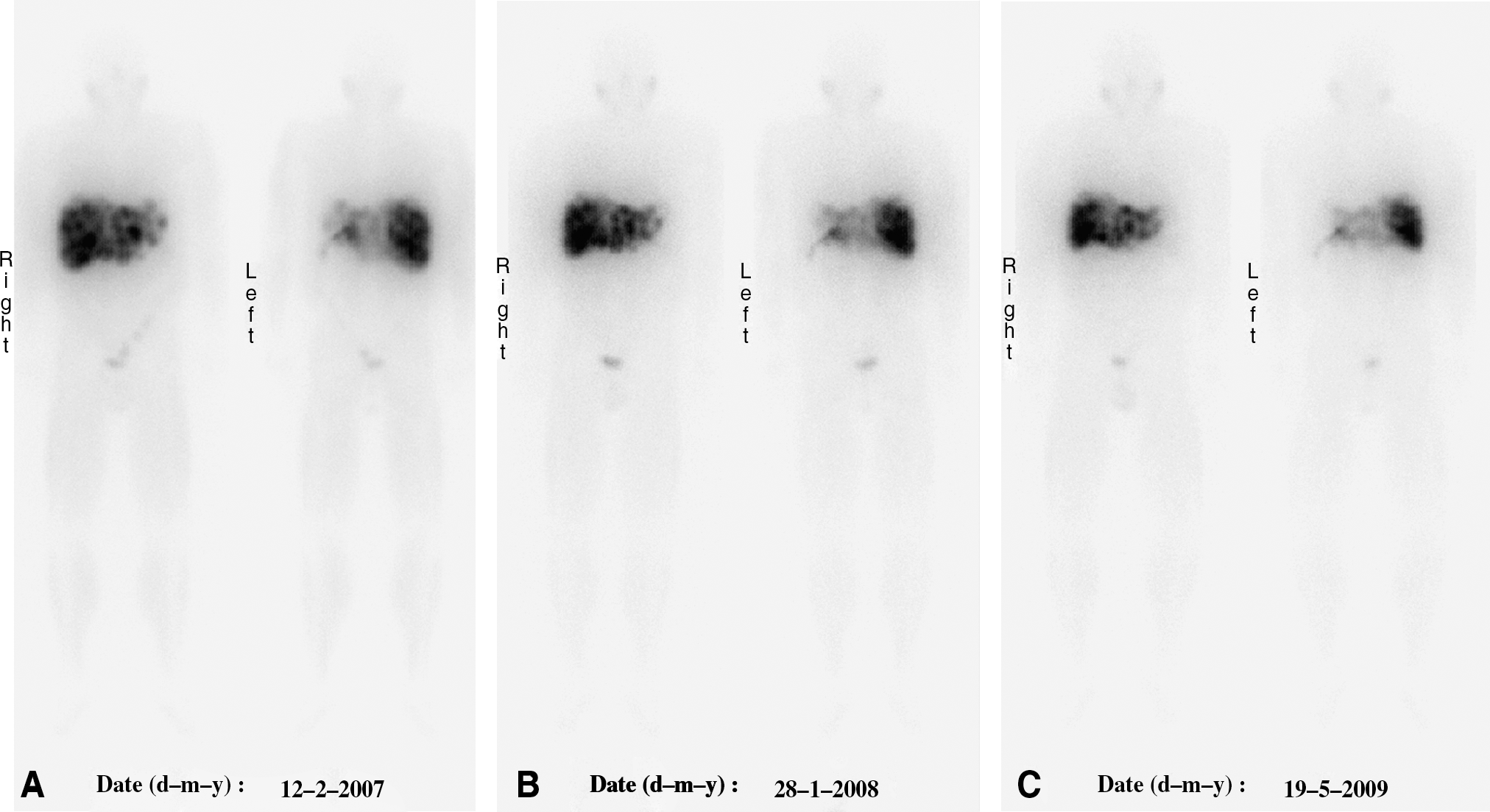
A 67-year-old man who presented in 2002 with a left adrenal mass and liver metastases, which appeared to be metastatic pheochromocytoma. He underwent a left adrenalectomy in 2002. In 2006, he was treated with a high dose of 18.5 GBq of 131I-MIBG. He required 4 platelet infusions and Neupogen® (Amgen Inc., Thousand Oaks, CA) injections following this treatment. He subsequently started 131I-MIBG maintenance treatment in February 2007. He received 7 low-dose treatments with 131I-MIBG (average dose, 3.7 GBq) between February 2007 and May 2009. The post-therapy images after treatment #2 (
Since the early days of radionuclide therapy, the goal of most treatments has been to deliver high doses of radioactivity to the tumor, with acceptable absorbed doses to other tissues. In most cases, the bone marrow appeared to be the dose-limiting organ. Some studies advocate the use of high doses of 131I-MIBG for the treatment of neuroendocrine tumors in order to achieve tumor-size reduction. However, given the indolent nature of the tumor and a still significant life expectancy of patients with metastatic disease, several centers have adopted an approach in giving patients multiple treatments over a prolonged period of time. In recent years, several centers have published the results of their respective ongoing treatment regimens. Table 1 summarizes the results of the most recent studies.
NE, neuroendocrine.
Most treatment regimens described the use of 131I-MIBG doses ranging from 5 to 11 GBq per treatment, allowing at least 12 weeks between each consecutive treatment. Patients are being followed for a considerable period of time, allowing not only an analysis of the response to treatment, but also providing survival data. All studies report symptomatic improvement in the vast majority of patients treated. Further, most studies report a significant improvement of the biochemical parameters. Anatomic response to treatment is observed in the minority of patients.
Most groups analyzed the effect of multiple low doses of 131I-MIBG on survival. Table 2 summarizes 5-year survival rates and median progression-free survival, as reported by the most recent studies. Our group not only analyzed the survival following multiple doses of 131I-MIBG, but also compared those data to survival data from another center in the same Canadian province that—at the time of the study—did not have access to 131I-MIBG treatment. 18 The patient groups were matched with respect to age, gender, tumor site, metastases, as well as concomitant treatment. The 5-year survival in our center was 63% in the 58 patients analyzed, whereas the 5-year survival rate in the 59 patients at the other center was 47% (p = 0.10).
Median dose per treatment.
NE, neuroendocrine; PFS, progression free survival.
A few studies have been published recently describing the results of high-dose 131I-MIBG treatment. Safford et al. describe the results of a series of 98 patients with metastatic carcinoid tumor. 19 The majority of patients received a single dose of 131I-MIBG, although 22 patients received two, and 4 patients three treatments. The median initial dose of 131I-MIBG was 11.3 GBq (306 mCi), whereas the median cumulative dose was 14.8 GBq (401 mCi). This treatment protocol led to a significant overall reduction of 5-HIAA levels (28%). In 37% of patients for whom 5-HIAA levels were available, a reduction of >50% was achieved. A radiographic response was induced in only 15% of patients, but radiographic response was not associated with longer survival. Interestingly, during the course of this protocol, the initial dose of treatment was raised. Analysis of the data revealed that patients treated with a higher initial dose (>14.8 GBq [400 mCi]) survived longer than patients who received less than 14.8 GBq (400 mCi) as the initial dose (4.7 versus 1.9 years).
Two other high-dose studies were conducted in pheochromocytoma and paraganglioma patients. The same group of Safford et al. also described the results of the high-dose treatment of 33 pheochromocytoma and paraganglioma patients. 20 The mean dose for the (initial) treatment was 14.5 GBq (391 mCi). Most patients only received one treatment. Again, the group found a survival benefit for patients treated with a high dose (>18.5 GBq [500 mCi]), when compated to those treated with an initial dose (<18.5 GBq [500 mCi]; 3.8 versus 2.6 years). Thirty-eight percent (38%) of patients showed a radiographic response; however, this was not associated with prolonged survival. Symptomatic response was observed in 86% of patients. The group of Fitzgerald et al. administered even higher doses of 131I-MIBG, following the harvest of stem cells. 21 They described the results of treatment of 30 patients in an ongoing phase II trial with a mean dose of 30.8 GBq (833 mCi) of 131I-MIBG. Only 4 patients required a reinfusion of their stem cells because of severe myelotoxicity. This treatment regimen led to an objective response in the majority of patients: 4 sustained complete remissions (CRs) and 15 sustained partial remissions (PRs). The 5-year survival was 75%.
Side-Effects
Side-effects of multiple treatments with 131I-MIBG are rather limited. The radiopharmaceutical should be infused slowly. Nausea following the administration of the radiopharmaceutical is quite common and tends to be significantly worse in the case of large hepatic tumor burden. Ondansetron is the antiemetic of first choice, as per the EANM guidelines. 4 Rarely, in adults with pheochromocytoma or paraganglioma, a significant rise in blood pressure can be observed during the administration of the radiopharmaceutical. Monitoring of the blood pressure during the infusion is, therefore, advised. Phentolamine, an alpha-adrenergic blocking agent, should be present in the administration room. Further, a carcinoid crisis could be induced in patients with carcinoid. Therefore, octreotide ampules should be part of the emergency medication set, too.
Hematologic toxicity is usually mild, even following multiple treatments or following high-dose regimens. At our center, 180 patients with metastatic carcinoid have been treated with an average of four treatments per patient at a mean dose of 5.0 GBq per treatment. Grade 3 or 4 hematologic toxicity only occurred in 17 of 180 patients. 22 Hypothyroidism is a long-term side-effect that is quite common, despite the use of adequate thyroid blockage with potassium iodide. Unlike treatments with radiolabeled somatostatin analogs, renal toxicity is uncommon following multiple infusions of 131I-MIBG. 22
Interactions with Other Medication
Multiple drugs that interfere with 131I-MIBG have been identified. The EANM guidelines currently provide the most comprehensive overview of cardiovascular, sympathomimetic, and neurologic drugs that interfere, including advice on how long the drugs should be discontinued before 131I-MIBG can be administered. 4 Given the possibility of multiple treatments with 131I-MIBG, it could be considered to replace drugs that are known to interfere by drugs that do not.
Concomitant Treatment
Treatment with 131I-MIBG could be combined with external-beam radiation. For instance, in patients with a pending fracture or a specific site of intense pain, palliative external-beam radiation can be beneficial to the patient. It can safely be combined with 131I-MIBG, since normally only a limited field is being irradiated. Further, treatment with long-acting octreotide in patients with metastatic carcinoid does not have to be discontinued during 131I-MIBG treatment, since they do not interfere.
A combination of 131I-MIBG and chemotherapy was described by Sisson et al. 23 Treatment consisted of three cycles of 131I-MIBG treatment, followed by chemotherapy 3–4 months after completion of the 131I-MIBG treatments. The addition of chemotherapy had a moderate additional effect in the 2 patients who completed the 9 months of chemotherapy. A simultaneous infusion of 131I-MIBG and chemotherapy was not described and would probably lead to significantly enhanced cytopenias due to the combination of these two myelotoxic modalities.
Finally, we would advocate against the simultaneous use of interferon-alpha and 131I-MIBG, since the patients who were treated with a combination of both at our center showed significantly more myelotoxicity than other patients.
Proposed Treatment Algorithm
Clinical experience obtained over a 25-year period, summarized in multiple publications, suggests that the use of 131I-MIBG in adults with metastatic neuroendocrine tumors is advantageous with respect to symptom reduction and hormone-level reduction in the majority of patients treated, and it could lead to objective anatomic responses. Since there seems to be a survival benefit when 131I-MIBG is added to the spectrum of treatments offered to neuroendocrine patients, the algorithm, as suggested by Sywak, remains valid (Table 3). 18 It is routinely used in our clinic.
Future Therapeutic Use
Future trials will establish the role of high doses of high-specific-activity 131I-MIBG in the management of patients with metastatic pheochromocytoma and paraganglioma. Currently, high-specific-activity 131I-MIBG (Azedra™; Molecular Insight Pharmaceuticals, Cambridge, MA) is being investigated in a phase II trial. The producer's hypothesis is that unlabeled MIBG does not provide therapeutic benefits, and that it may provide unwanted side-effects and compete with therapeutic 131I-MIBG for binding on target-receptor sites, thereby potentially affecting efficacy. 24 This hypothesis is different from the opinion of the Amsterdam group, who published research on both the therapeutic application of unlabeled MIBG and the combination of unlabeled MIBG and 131I-MIBG to improve tumor targeting. 25 High-specific-activity 131I-MIBG has been used in a phase I dose-finding study. 24 Currently, a phase II study in patients with pheochromocytoma and paraganglioma is being conducted. Patients will receive two doses of 18.5 GBq (500 mCi) or 296 MBq/kg (8 mCi/kg) of high-specific-activity [131]I-MIBG 3 months apart. 26
Further, the adjuvant role of 131I-MIBG following potentially curative surgery with minimal residual disease needs to be established. New developments in the treatment of neuroendocrine patients include trials using tyrosine kinase inhibitors. The role of these in the management of neuroendocrine tumors and their role in relation to the use of 131I-MIBG treatment remain to be established. Finally, when radiolabeled somatostatin analogs may make it to the market, the role for these radiopharmaceuticals in relation to the use of 131I-MIBG needs to be discussed, too.
Conclusions
131I-MIBG is an effective and safe treatment modality for neuroendocrine tumors. Treatment with multiple doses is well-tolerated and generally leads to symptomatic relief. Biochemical responses are noted in approximately half of the patients treated, anatomical responses are seen in about a third of the patients. Use of 131I-MIBG should be considered in patients with MIBG-avid disease with residual disease following optimal surgical treatment, or in those for whom surgery was not possible.
Footnotes
Disclosure Statement
No competing financial interests exist.
About the authors
Ernst J. Postema studied medicine at the Erasmus University Rotterdam, the Netherlands, from 1989 to 1996. He was accepted for the Nuclear Medicine Training Program at the University Medical Centre St. Radboud, Nijmegen, the Netherlands, by Professor Corstens in September 1997. He combined his clinical training with research in therapeutic nuclear medicine. His research focus was treating patients with non-Hodgkin's lymphoma and head and neck cancer with radioactive antibodies. This resulted in a PhD thesis called “Radioimmunotherapy using 186Relabeled humanized monoclonal antibodies,” which he defended at the Radboud University Nijmegen on March 23, 2004.
Since 2003, Dr. Postema has worked as a Nuclear Medicine Specialist. He is currently working at the Cross Cancer Institute, Edmonton, Alberta, Canada. His primary focus is therapeutic nuclear medicine. He also has an academic appointment as an assistant professor at the Department of Oncology, University of Alberta, Edmonton, since September 2005.
Sandy McEwan is a Nuclear Medicine physician and Director of Oncologic Imaging at the Cross Cancer Institute, and Associate Director of Research of the Cross Cancer Institute. He also is Professor and Chair of the Department of Oncology at the University of Alberta in Edmonton, Alberta, Canada. He attended Middlesex Hospital Medical School, University of London, England, graduating in 1975. He obtained his M.Sc. in Nuclear Medicine also from the University of London in 1981 and FRCPC in Nuclear Medicine in 1986. After serving as a Medical Officer in the Royal Navy and as Registrar in Oncology in Auckland, New Zealand, and senior registrar in Nuclear Medicine at Southampton General Hospital, UK, he emigrated to Canada in 1986. He was Professor and Chair of the Department of Radiology and Diagnostic Imaging at the University from 1992 to 1999.
In addition to his leadership duties and administrative, teaching, and clinical activities, Dr. McEwan is Past President of the Society of Nuclear Medicine and is active on many committees with this organization. He was instrumental in establishing the Society's Clinical Trials Network and is a leader of the Canadian Molecular Imaging Network. His research interests include radioisotope therapy and very low-dose-rate radiation effects, clinical trial development of novel molecular imaging agents and imaging biomarkers, and the translation of imaging biomarkers into clinical practice. Dr. McEwan has been instrumental in the development of the Positron Emission Tomography (PET) Program at the Cross Cancer Institute, raising grant funding and donations of approximately $18 million for this project. He has over 100 publications and is frequently invited to speak at international meetings.