
Abstract
Metaiodobenzylguanidine (MIBG) is an enzymatically stable synthetic analog of norepinephrine that when radiolabled with diagnostic (123I) or therapeutic (131I) isotopes has been shown to concentrate highly in sympathetically innervated tissues such as the heart and neuroendocrine tumors that possesses high levels of norepinephrine transporter (NET). As the transport of MIBG by NET is a saturable event, the specific activity of the preparation may have dramatic effects on both the efficacy and safety of the radiodiagnostic/radiotherapeutic. Using a solid labeling approach (Ultratrace), noncarrier-added radiolabeled MIBG can be efficiently produced. In this study, specific activities of >1200 mCi/μmol for 123I and >1600 mCi/μmol for 131I have been achieved. A series of studies were performed to assess the impact of cold carrier MIBG on the tissue distribution of 123/131I-MIBG in the conscious rat and on cardiovascular parameters in the conscious instrumented dog. The present series of studies demonstrated that the carrier-free Ultratrace MIBG radiolabeled with either 123I or 131I exhibited similar tissue distribution to the carrier-added radiolabeled MIBG in all nontarget tissues. In tissues that express NETs, the higher the specific activity of the preparation the greater will be the radiopharmaceutical uptake. This was reflected by greater efficacy in the mouse neuroblastoma SK-N-BE(2c) xenograft model and less appreciable cardiovascular side-effects in dogs when the high-specific-activity radiopharmaceutical was used. The increased uptake and retention of Ultratrace 123/131I-MIBG may translate into a superior diagnostic and therapeutic potential. Lastly, care must be taken when administering therapeutic doses of the current carrier-added 131I-MIBG because of its potential to cause adverse cardiovascular side-effects, nausea, and vomiting.
Introduction
Targeted molecular radiotherapy is the logical extension of molecular diagnostic radionuclide imaging. Treatment success in cancer depends on sufficient upregulation of disease target, the specificity of the target, choice of the radionuclide, and a sufficient concentration delivered to and residence time at the target. 1
Metaiodobenzylguanidine (MIBG) is a synthetic analog of the biogenic amine, norepinephrine, and has been widely used in its radiolabeled forms (usually 131I or 123I) since the early 1980s for the diagnosis and, when labeled with iodine-131, radiotherapy of various neuroendocrine tumors such as neuroblastoma, pheochromocytoma, and carcinoid. Like norepinephrine, MIBG is concentrated in sympathomedullary tissues predominantly by an active uptake mechanism, the norepinephrine transporter (NET). 2 –4 The NET is expressed on the surfaces of highly sympathetically innervated cells of normal tissue, such as the heart and adrenal glands, and is highly expressed in tumors of neural crest origin, such as neuroblastoma and pheochromocytoma. 2 –4 This uptake and prolonged retention of MIBG within the intracellular catecholamine storage vesicles constitute an ideal target/mechanism to exploit for the detection and treatment of neuroendocrine tumors because it ensures an increased concentration and dwell time of the radiodiagnostic/therapeutic in the tumor.
The current commercial methods to produce 123I- and 131I-MIBG utilize the copper-catalyzed isotope exchange reaction. This method requires 1–2 mg of nonradioactive MIBG, which must be present in 2000-fold molar excess to the radioactive sodium iodide (131I or 123I), coupled with heating the mixture to 150°C, to drive the halogen exchange to equilibrium. The radiolabled MIBG is subsequently separated by column chromatography. Although this is a simple synthesis, it precludes the ability to produce MIBG with high specific activity because of the inability to separate nonradiolabeled MIBG by column chromatography. Vaidyanathan and Zalutsky 5 developed two routes to synthesize high-specific-activity MIBG, in which the use of the halogen exchange reaction was avoided by using nonradiolabeled iodine for iodine (123 or 131). However, a time-consuming high-performance liquid chromatography purification is required. Hunter and Zhu 6 have demonstrated a more practical approach in the use of aryl-tin intermediates, where the benzylguanidine precursor is bound to a polystyrene-based resin through a di-butyltin linker. Radiolabeling is performed simply by heating 131I-sodium iodide with an oxidizing agent and filtering off the radiolabeled MIBG. The intrinsic implication of this technique is that very high-specific-activity iodine-labeled radiopharmaceuticals can be rapidly produced with no other components in the solution, except the aqueous vehicle. This process offers a true “carrier-free” or “noncarrier-added” radiopharmaceutical preparation and thus avoids any potential competitive pharmacological effects of the carrier. Molecular Insight Pharmaceuticals, Inc., is developing this true “carrier-free” version of 131I-MIBG as Ultratrace 131I-MIBG.
The present series of studies were performed to compare the tissue distribution and efficacy of the Ultratrace 123/131I-MIBG with the carrier-added 123/131I-MIBG.
Materials and Methods
Radiopharmaceuticals
High-specific-activity 123/131I-MIBG was produced by Molecular Insight Pharmaceuticals via a validated cGMP process, using the Ultratrace solid phase method. It was provided as a sterile frozen solution, with a high specific activity and in radioactive concentration. The Ultratrace process uses a solid polystyrene resin containing the covalently bound stannylbenzylguanidine precursor, which undergoes a 1:1 displacement reaction with iodine at room temperature. Briefly, the solid phase precursor is suspended in a dilute mixture of radioactive 123/131I-sodium iodide, hydrogen peroxide, and acetic acid at 25°C for 60 minutes. The oxidized 123/131I-iodine reacts to disrupt the covalent bond between the tin and benzylguanidine precursor with radioiodine insertion at the meta position of the phenyl ring to form 123/131I-MIBG. As 123/131I-MIBG forms, it is simultaneously cleaved from the solid polymer resin and dissolves into the liquid phase. The labeled 123/131I-MIBG is then separated from the remaining solid resin and any residual reagents by using cation exchange chromatography. The purified 123/131I-MIBG is eluted from the column and collected in a glass vial containing a solution of sodium gentisate and sodium ascorbate acting as radiostabilizers. The formulated final product solution is filtered through two 0.22-μm membrane sterilizing filters and 15 mL aliquots were aseptically filled into 30-mL glass vials, which are then aseptically capped, sealed, and frozen.
The final drug formulation of 123/131I-MIBG was tested and certified to have a radionuclide purity of >99.0%. Carrier-added 123/131I-MIBG was made by fortifying 123/131I-MIBG with the appropriate concentration of cold MIBG to achieve the desired specific activity. CIS-US 131I-MIBG was purchased from CIS-US.
123/131I-MIBG rat tissue distribution studies
A quantitative comparison of the tissue distribution and pharmacokinetics of the carrier-added and the Ultratrace 123I-MIBG or 131I-MIBG was performed in separate groups of male and female Sprague Dawley rats (N = 2 per sex per group per time point). The test samples were diluted in phosphate-buffered saline (pH 7.0) and administered via the tail vein as a bolus of 10 μCi/rat (∼40 μCi/kg) in a constant volume of 0.1 mL. The animals were euthanized by asphyxiation with carbon dioxide at 0.25, 1, 6, 24, 48, and 72 hours postinjection. Tissues (heart, liver, lungs, spleen, large and small intestine [with contents], stomach [with contents], kidneys, thyroid, skeletal muscle, testes or uterus and ovaries, brain, bone marrow, and bone) were dissected, excised, weighed wet, put in plastic tubes, and assayed in an automated γ-counter (LKB model 1282; Wallac Oy). Tissue time–radioactivity levels of 123/131I-MIBG expressed as percent injected dose per gram (%ID/g) were determined. Blood samples were also obtained at the time of sacrifice and weighed, and total radioactivity was determined. Tissue samples were counted along with aliquots of the injected dose to correct for radioactive decay and to calculate %ID contained in each sample. The %ID/g per tissue was calculated by converting the decay-corrected counts per minute to the percent dose or the amount of radioactivity in nCi and then dividing by the weight of the tissue or organ sample.
Cardiovascular effects in conscious dogs
Four (4) male and 4 female beagle dogs were surgically implanted with telemetry units to permit the assessment of arterial pressure and heart rate in the conscious free-roaming state. A gel-filled pressure transducer (for blood pressure measurements) was inserted into the left femoral artery and secured appropriately. Two electrocardiogram (ECG) leads (one positive and one negative) were tunneled through the subcutaneous tissue to the left ventrolateral thoracic region (positive lead) and on to the right ventral chest region, cranial to the manubrium of the sternum and to the right of the midline (negative lead). Upon completion of a 3-week postsurgical recovery and acclimation period, each dog was intravenously (i.v.) administered saline followed by MIBG in ascending doses of 0.03, 0.3, 1, and 3 mg/kg, i.v., at 30-minute intervals and the effects on arterial pressure, heart rate, and behavior were continuously monitored. The doses were chosen to encompass the range of total MIBG administered in human-equivalent therapeutic preparations of 131I-MIBG.
131I-MIBG therapy study
Human neuroblastoma xenografts were established in CD/1 nu/nu athymic mice by using the method described by Rutgers et al. 7 A suspension containing 3 × 106 freshly harvested SK-N-BE(2c) cells was delivered by intrasplenic injection. When palpable hepatic and splenic tumors developed, 2–3-mm fragments were placed subcutaneously into the subcostal flank of new nescient mice. When tumors reached an average volume of ∼400 mm3, animals were randomly assigned to one of the treatment groups. Animals were divided into the following 7 groups (N = 8–10 mice per group): saline, carrier-added 131I-MIBG or noncarrier-added Ultratrace 131I-MIBG at 8.1, 24.3, and 81 mCi/m2 (2.7, 8.1, and 27 mCi/kg). Each animal was administered the test sample i.v in a volume of 0.1 mL, using the schedule outlined above, for ∼10 seconds. Tumor dimensions were measured twice weekly with digital calipers and tumor volumes were calculated with the following formula: (width 2 × length)/2. Mice were followed until tumor volumes reached the maximal allowable size per IACUC guidelines of 1500 mm3. Carrier-added 131I-MIBG, manufactured via the halogen exchange method, was purchased from Amersham Biosciences. It had a specific activity of 8.25 mCi/μmol at the time of injection, whereas the Ultratrace 131I-MIBG (ultra) had a specific activity of 1283 mCi/μmol (155-fold increase in specific activity).
Data analysis
All values were decay corrected to the time of injection and are expressed as the mean ± standard deviation or standard error of the mean. To assess differences between the groups, statistical analyses consisting of a one-way analysis of the variance and, where appropriate, Student's unpaired t-test (DF = N − 1; two-tailed probability) were performed. Differences were considered significant when p < 0.05.
The pharmacokinetics of 123/131I-MIBG was analyzed by WinNonlin 4.1 (Pharsight). The blood and tissue concentration–time data were computed by a noncompartment method and PK parameters (C max, AUC, and MRT) were generated. Total organ clearance (CL) was calculated from the following equation: CL = dose/AUC. Steady-state volume of distribution (V ss) was calculated as follows: V ss = MRT × CL.
Results
Comparison of 123I-MIBG manufactured via the Ultratrace or the halogen exchange method
A study was conducted in rats to investigate the impact of cold carrier (carrier added) on the tissue distribution of 123I-MIBG. This was accomplished by comparing the high-specific-activity (1283 mCi/μmol), noncarrier-added 123I-MIBG prepared via the Ultratrace method to the currently used halogen exchange method to produce 123I-MIBG with a specific activity of 8.25 mCi/μmol.
Both preparations were cleared from the blood in a similar manner, and at 72 hours postinjection, blood levels of both preparations were below the limits of detection (Fig. 1). The terminal half-life for the carrier-added preparation and the Ultratrace preparation did not differ (15 and 18 hours, respectively). There was no significant difference in the C max levels when comparing the preparations in individual tissues. Total radioactivity tissue exposure was determined using AUC0-inf. A 1.8 times greater exposure was observed in the heart and lung in the Ultratrace 123I-MIBG-treated animals when compared with the carrier-added preparation. Radioactive exposure in the bone marrow tended to be lower (approximately half ) in the Ultratrace group when compared with the carrier-added preparation (Fig. 2).
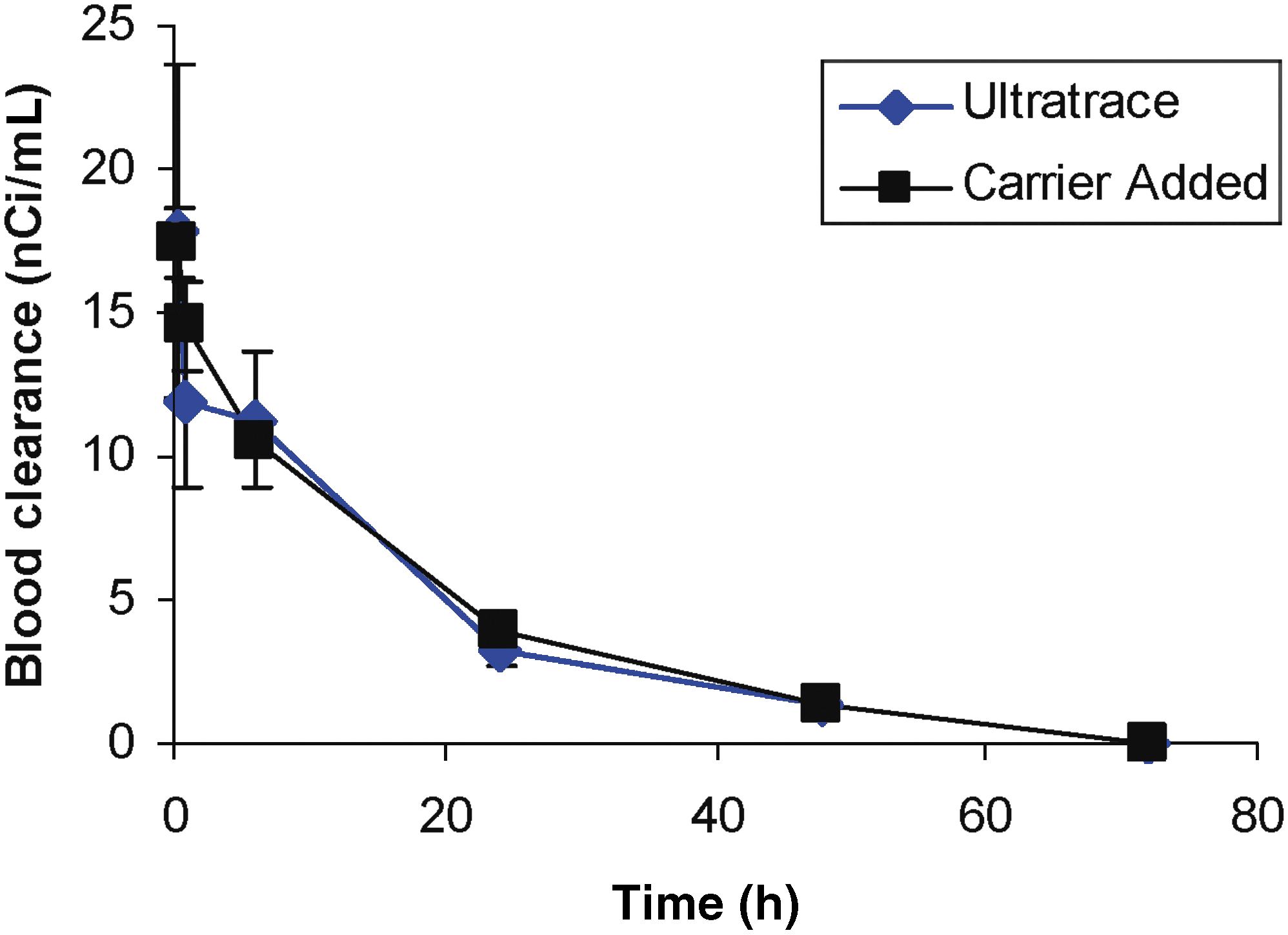
Blood clearance of 123I-MIBG prepared using the Ultratrace or the carrier-added method in the conscious rat administered 40 μCi/kg intravenously. The blood concentrations are expressed as the mean ± standard deviation in nCi/mL decay corrected to the time of injection for 4 rats each per time point. The specific activity of the Ultratrace 123I-MIBG was 1283 mCi/μmol and of the carrier-added 123I-MIBG was 8.25 mCi/μmol, which resulted in MIBG doses of 1.8 and 0.01 μg/kg, respectively. MIBG, metaiodobenzylguanidine.
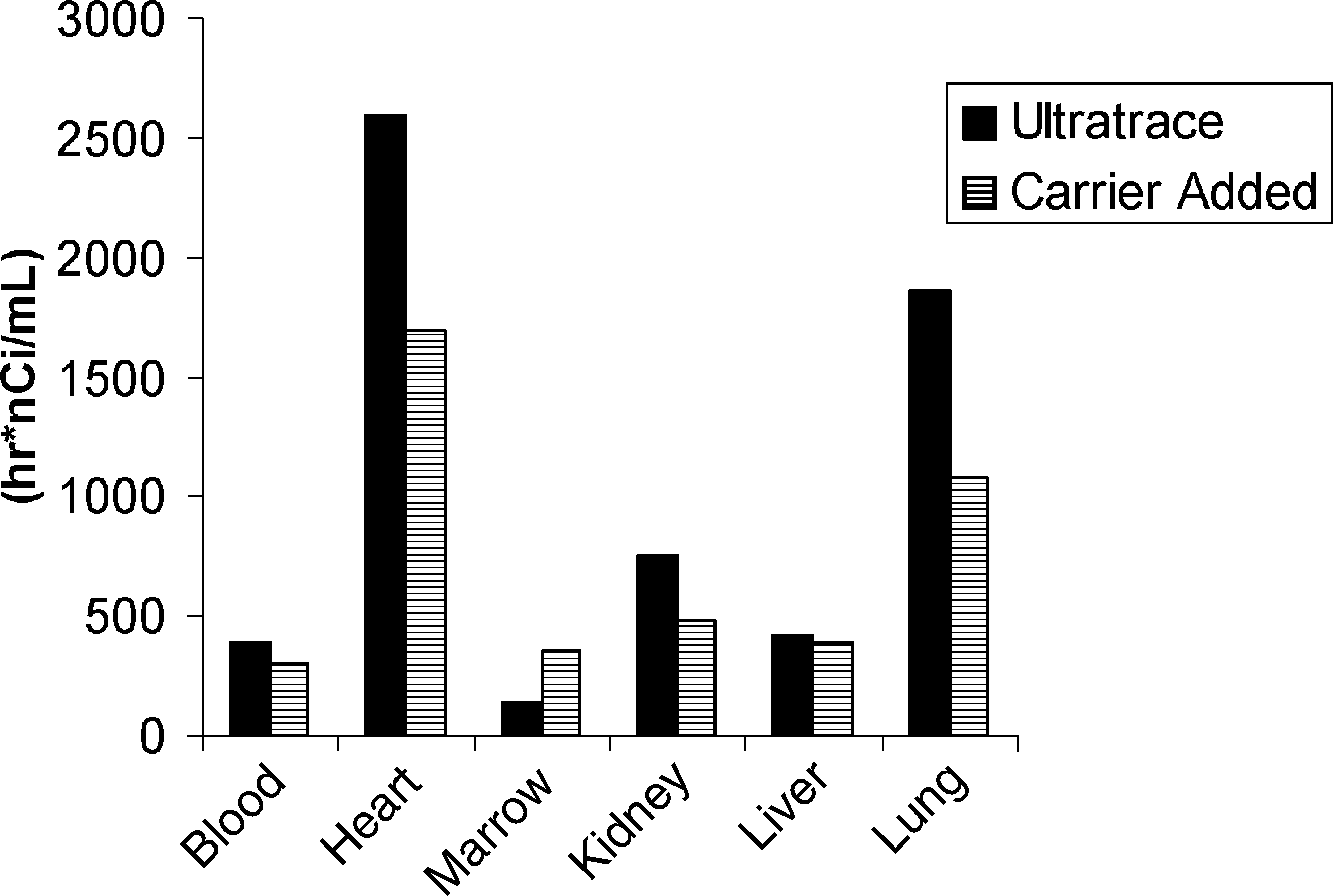
Tissue exposure of 123I-MIBG prepared using the Ultratrace or the carrier-added method in the conscious rat administered 40 μCi/kg intravenously. The AUC0-inf is expressed as the mean tissue exposure in the conscious rat. Each histogram is the mean exposure calculated using six time points with 4 rats per time point. The specific activity of the Ultratrace 123I-MIBG was 1283 mCi/μmol and of the carrier-added 123I-MIBG was 8.25 mCi/μmol, which resulted in MIBG doses of 1.8 and 0.01 μg/kg, respectively. MIBG, metaiodobenzylguanidine.
Figure 3 illustrates the total MIBG content in selected tissues expressed as exposure (AUC). Because of the differences in specific activity, there was a 300–1000 times greater exposure (heart 26 vs. 10,138 [hours·pg]/mL; marrow 1.4 vs. 2145 [hours·pg]/mL for the Ultratrace vs. the carrier-added MIBG, respectively) to tissue of animals administered MIBG prepared by the carrier-added preparation when compared with the Ultratrace method.
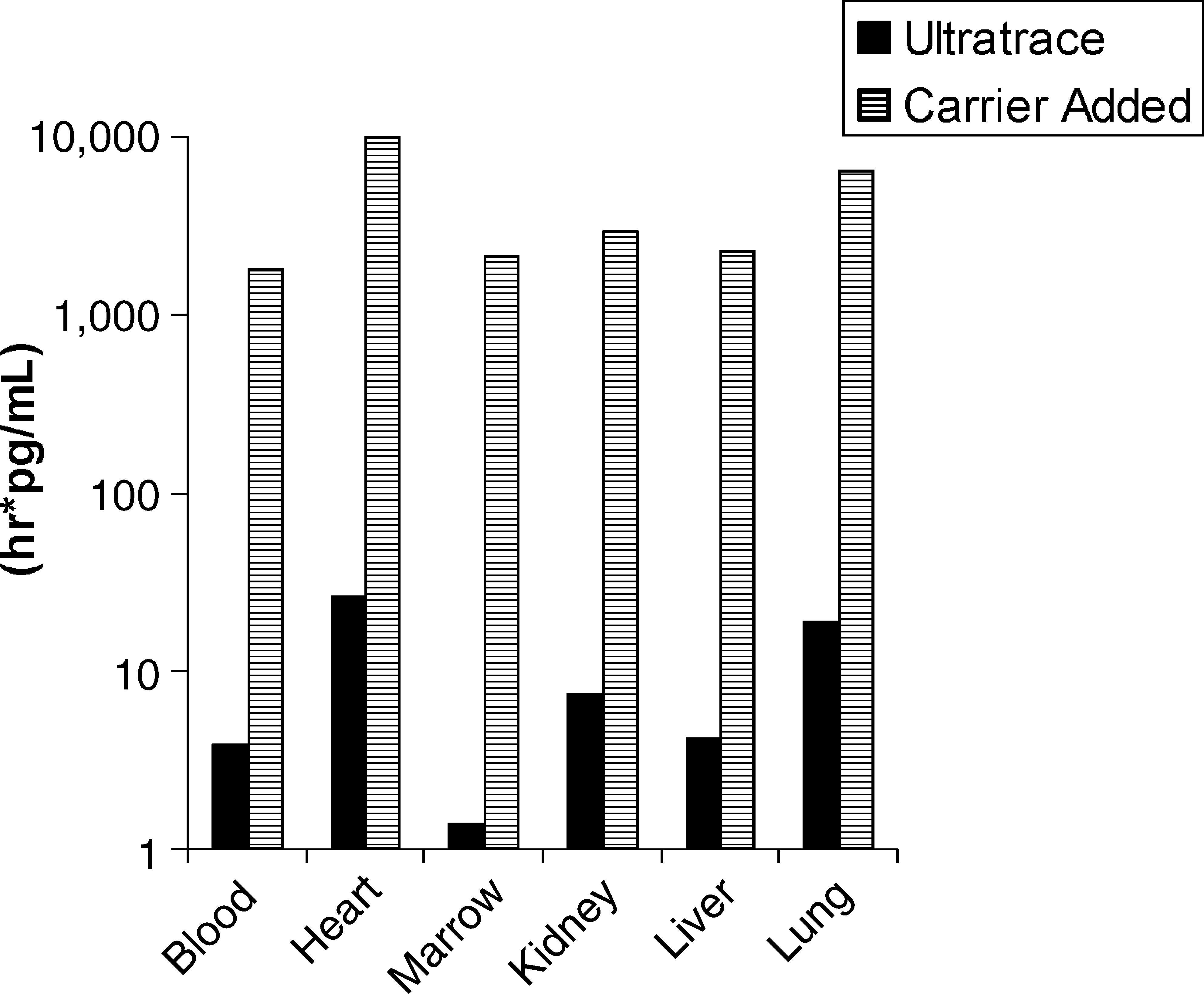
Tissue exposure of total MIBG, prepared using the Ultratrace or the carrier-added method, in the conscious rat administered 40 μCi/kg intravenously. The AUC0-inf is expressed as the mean tissue exposure in the conscious rat. Each histogram is the mean exposure calculated using six time points with 4 rats per time point. The specific activity of the Ultratrace 123I-MIBG was 1283 mCi/μmol and of the carrier-added 123I-MIBG was 8.25 mCi/μmol, which resulted in MIBG doses of 1.8 and 0.01 μg/kg, respectively. MIBG, metaiodobenzylguanidine.
Comparison of 131I-MIBG manufactured via the Ultratrace or the halogen exchange method
The tissue distributions of 131I-MIBG prepared using (1) the Ultratrace method and (2) the iodine exchange, carrier added, method (CIS-US 131I-MIBG) were assessed in separate groups of 4 rats each at six time points through 72 hours postinjection. In the present study, 131I-MIBG was i.v. administered at 40 μCi/kg (specific activity: Ultratrace >1600 mCi/μmol and Cis 1 mCi/μmol). Tables 1 and 2 show the tissue distributions of 131I-MIBG prepared using the Ultratrace method versus the CIS-US product prepared using the halogen exchange method. Both 131I-MIBG preparations were cleared from the blood in a similar manner. After reaching C max (the first time point), blood concentrations readily declined, with similar residence times of 22.2 and 19.3 hours for the Ultratrace 131I-MIBG and the carrier-added 131I-MIBG, respectively. Mean blood clearance values were similar for both preparations (0.1 L/[kg·h]), indicating that 131I-MIBG is slowly cleared in rats. Blood exposure (AUC0-inf) was similar for both the Ultratrace (286 hours·nCi/mL) and the CIS-US (323 [hours·nCi]/mL) preparations. Mean volume of distribution at steady state (V ss) ranged from 3.1 to 2.4 L/kg for the Ultratrace and the CIS-US groups, respectively. Thus, in a 0.3-kg male rat, V ss would be ∼1 L, which is >100% of body weight (assuming that 1 L is equal to 1 kg). This indicates that 131I-MIBG is highly distributed into deep tissue compartments.
All values are expressed as the percent injected dose/g decay corrected to the time of injection mean ± standard deviation for 4 rats per time point.
Sum of paired organs.
MIBG, metaiodobenzylguanidine.
All values are expressed as the percent injected dose/g decay corrected to the time of injection mean ± standard deviation for 4 rats per time point.
Sum of paired organs.
MIBG, metaiodobenzylguanidine.
As anticipated, because of the mechanism of action of MIBG, uptake and exposure were greatest in the heart. 8 After reaching C max at the first time point, heart concentrations declined with mean residence times of 12.1 and 11.7 hours for the Ultratrace 131I-MIBG and the CIS-US 131I-MIBG, respectively. Mean heart clearance values were similar for both preparations (0.2 L/[kg·h]), indicating that 131I-MIBG was slowly cleared from the heart in rats. Heart exposure (AUC0-inf) was similar for both the Ultratrace (2794 [hours·nCi]/mL) and the carrier-added Cis-US (2460 [hours·nCi]/mL) preparations.
The published literature indicates that the bone marrow is the dose-limiting organ for the carrier-added 131I-MIBG. 9,10 After reaching C max, at the first time point (18 and 21 nCi/g for the Ultratrace and the CIS, respectively), marrow concentrations declined, with similar mean residence times of 12.3 and 9.8 hours for the Ultratrace 131I-MIBG and the CIS-US 131I-MIBG, respectively. Mean marrow clearance values were similar for both preparations (0.2–0.1 L/[kg·h]), indicating that 131I-MIBG is slowly cleared from the marrow in rats. Marrow exposure (AUC0-inf) was similar for both the Ultratrace (202 [hours·nCi]/mL) and the CIS-US (332 [hours·nCi]/mL) preparations. There was no difference between the preparations observed in the kidney and liver (Table 3). Thus the bone marrow remains the dose-limiting organ for the Ultratrace labeling method.
Analysis was performed using the mean ± standard deviation for 4 rats at six time points. CIS-US (specific activity: 1 mCi/μmol) and Ultratrace 131I-MIBG (specific activity: >1600 mCi/μmol) at 40 μCi/kg were studied in separate groups of 4 rats per time point with six time points through 72 hours postinjection.
MIBG, metaiodobenzylguanidine.
Comparison of blood pharmacokinetics and tissue distribution of the Ultratrace 131I-MIBG and the cold carrier MIBG in the conscious rat
To study the implications of the cold carrier MIBG when therapeutic doses of 131I-MIBG are administered, a tissue distribution study was conducted in conscious rats, wherein the specific activity of the test preparations was adjusted to mimic the amount of cold carrier that would be present at therapeutic doses in the range of 5–10 mCi/kg by using the specific activity of the current commercially available Izotop and the previously available Michigan 131I-MIBG products. In the present study, rats were administered 40 μCi/kg (240 μCi/m2) Ultratrace fortified with cold MIBG to mimic doses of 185 and 370 mCi/m2 (5 and 10 mCi/kg) in man. In the noncarrier-added Ultratrace group, because of the high specific activity, the total amount of MIBG administered was below the limits of quantification. The fortified Ultratrace 131I-MIBG showed comparable blood pharmacokinetics when compared with the Ultratrace 131I-MIBG (Fig. 4). The radiolabel was detected at varying levels in all tissues examined, which decreased readily over time. No difference in tissue distribution was noted with the exception of the heart between 46.5 and 93 mg/mCi (5 and 10 mCi cold carrier mimic) carrier 131I-MIBG. Increasing amounts of the cold carrier MIBG resulted in decreased uptake of 131I-MIBG in the heart (Fig. 4). Notably, when compared with the noncarrier-added Ultratrace 131I-MIBG, both preparations demonstrated a significant (p < 0.005) reduction in exposure (AUC) to 131I-MIBG in the heart. At 6 hours postinjection, concentrations of 115.05 ± 33.71, 28.40 ± 3.67, and 22.34 ± 4.00 nCi/g were determined for the Ultratrace 131I-MIBG, the Ultratrace 131I-MIBG plus 46.5 mg/mCi, and the Ultratrace 131I-MIBG plus 93 mg/mCi, respectively.

Determination of the impact of cold carrier MIBG on blood, heart, and bone marrow clearance in conscious rats. The mean ± SD tissue clearance over time for rats administered the Ultratrace 131I-MIBG (40 μCi/kg), the commercial CIS-US 131I-MIBG (40 μCi/kg), and the Ultratrace 131I-MIBG (40 μCi/kg) fortified with cold carrier MIBG at therapeutic doses of 185 mCi/m2 (cold 46.5 mg/mCi) and 370 mCi/m2 (cold 93 mg/mCi) is depicted. Each point is the mean ± SD for 4 rats per time point. MIBG, metaiodobenzylguanidine; SD, standard deviation.
The decrease in uptake in the heart with low specific activity was anticipated because the heart is a highly innervated tissue with high expression of the norepinephrine uptake-1 transporter. Interestingly, a tendency toward a dose-related increase in 131I-MIBG uptake in the presence of increasing amounts of the cold carrier MIBG was observed in the bone marrow (Figs. 4 and 5).
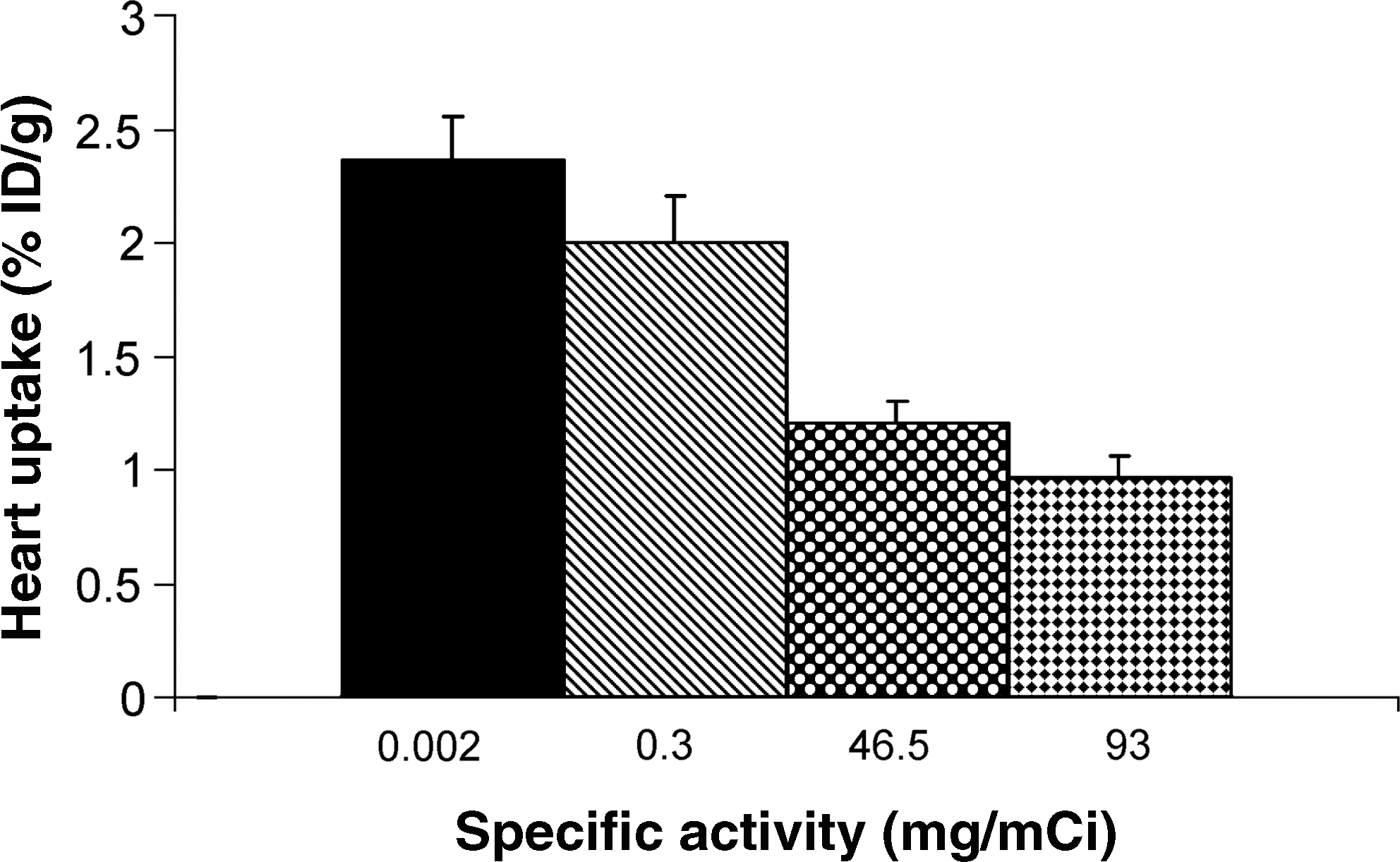
Influence of the MIBG specific activity on heart uptake in the conscious rat at 1 hour postinjection. The mean heart exposure for rats administered 131I-MIBG (40 μCi/kg) at a specific activity of 0.002 mg/mCi for the Ultratrace and 0.3 mg/mCi for the Cis-US, at therapeutic doses of 185 mCi/m2 (43 mg/mCi) and 370 mCi/m2 (93 mg/mCi), is depicted. Each histogram is the mean ± standard error of the mean for 4 rats. MIBG, metaiodobenzylguanidine; %ID/g, percent injected dose per gram.
Impact of MIBG on the cardiovascular system in the conscious dog
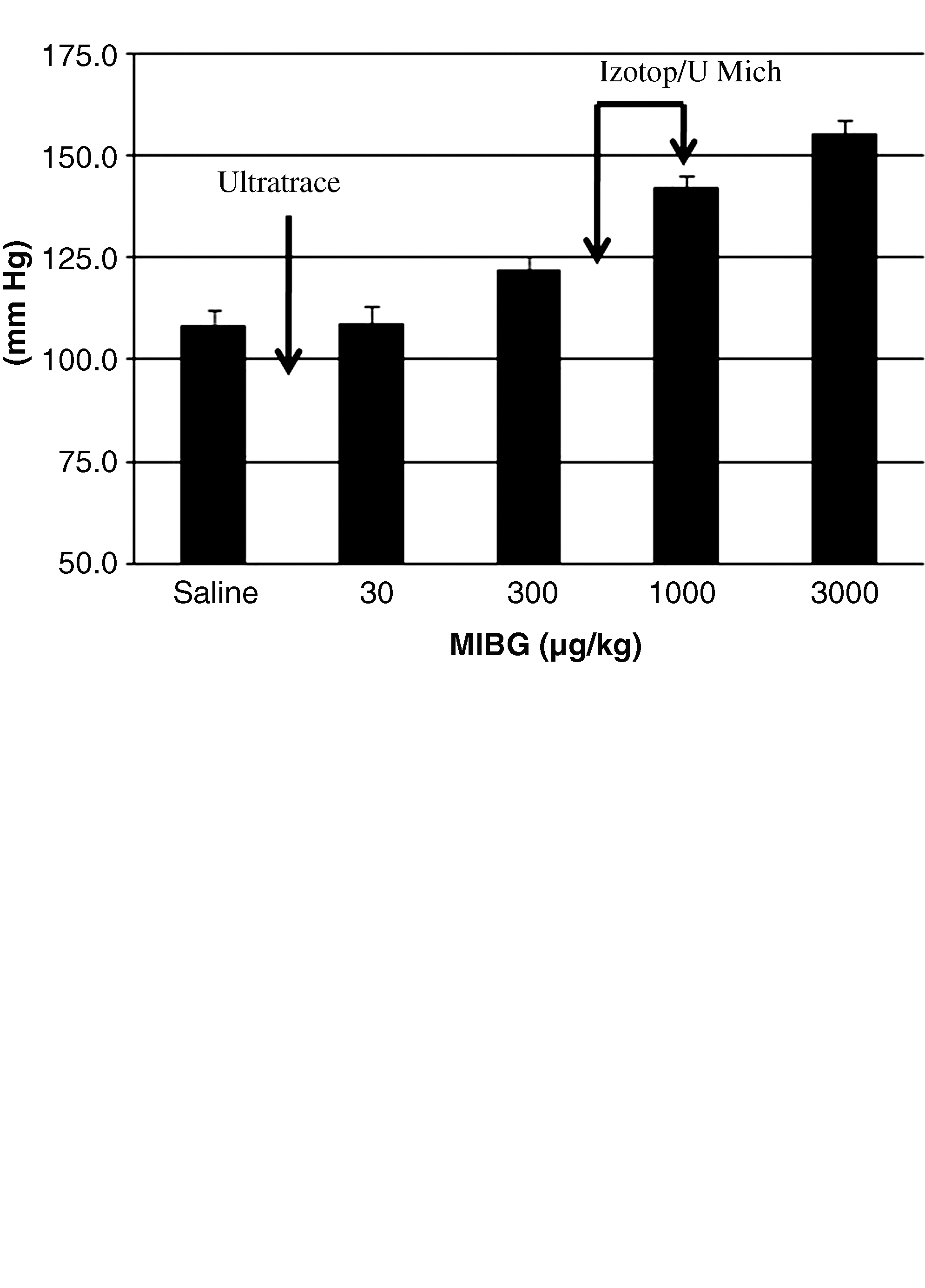
A study was performed to assess the impact of the cold carrier MIBG on the cardiovascular system (arterial pressure, heart rate, and ECG) in conscious telemeterized dogs. The doses were chosen to determine the amount of cold carrier commonly observed in the current commercially available 131I-MIBG therapeutic products. At a dose of 370 mCi/m2, the resultant amount of MIBG delivered by using the Ultratrace 131I-MIBG was 3 μg/kg, whereas by using the Izotop and University of Michigan products ∼600–1000 μg/kg was delivered.
Treatment with MIBG at doses up to 3000 μg/kg had no adverse effect on mortality, clinical, cageside, or postinjection observations, body weights, body weight changes, body temperature, or QT values.
A dose-dependant increase in arterial pressure concomitant with a reflex bradycardia was observed in all animals, with the reflex bradycardia maximized at 1 mg/kg, i.v. At 3 mg/kg, i.v., the duration of action was >20 minutes. MIBG at 30, 300, 1000, and 3000 μg/kg, i.v., elicited dose-related increases in mean arterial pressure of 0%, 13%, 32%, and 45%, respectively, from the baseline value of 108 ± 4 mmHg. A reflex bradycardia was observed, wherein heart rate decreased by 8%, 39%, 50%, and 43%, respectively, from the baseline value of 111 ± 4 bpm (Fig. 6).
Effects of intravenously administered MIBG on mean arterial pressure (
All ECGs were within normal limits following bolus intravenous administration of MIBG at doses of 30 and 3000 μg/kg.
Comparison of the antitumor effects of the Ultratrace 131I-MIBG and the carrier-added 131I-MIBG
A study was performed in the human neuroblastoma SK-N-BE(2c) mouse xenograft model to compare the therapeutic efficacy of the high-specific-activity Ultratrace 131I-MIBG with the low-specific-activity 131I-MIBG purchased from Amersham Biosciences. When the tumors reached a starting volume of 391 ± 8 mm3, animals were randomly assigned to one of the 7 treatment groups. There were no significant differences in the average starting tumor volume in any of the treatment groups. Saline treatment resulted in a linear growth rate over 15 days at which point the animals were euthanized because of tumor size of >1500 mm3. During this time the tumor size increased fourfold, resulting in a tumor doubling time of ∼6 days. The intravenous administration of a single dose of 8.1, 24.3 and 81 mCi/m2 131I-MIBG (2.7, 8.1, and 27 mCi/kg) elicited a dose-related suppression in growth rate when compared with saline. In all cases the decrease in tumor growth rate was approximately twofold greater in the Ultratrace 131I-MIBG groups when compared with the carrier-added 131I-MIBG groups (Table 4 and Fig. 7). At 45 days after the administration of 81 mCi/m2 (27 mCi/kg) Ultratrace 131I-MIBG, the tumor size increased fourfold above baseline when compared with the same administered radioactive dose of the carrier-added 131I-MIBG, wherein a fourfold increase in growth rate was observed at 28 days post-treatment.
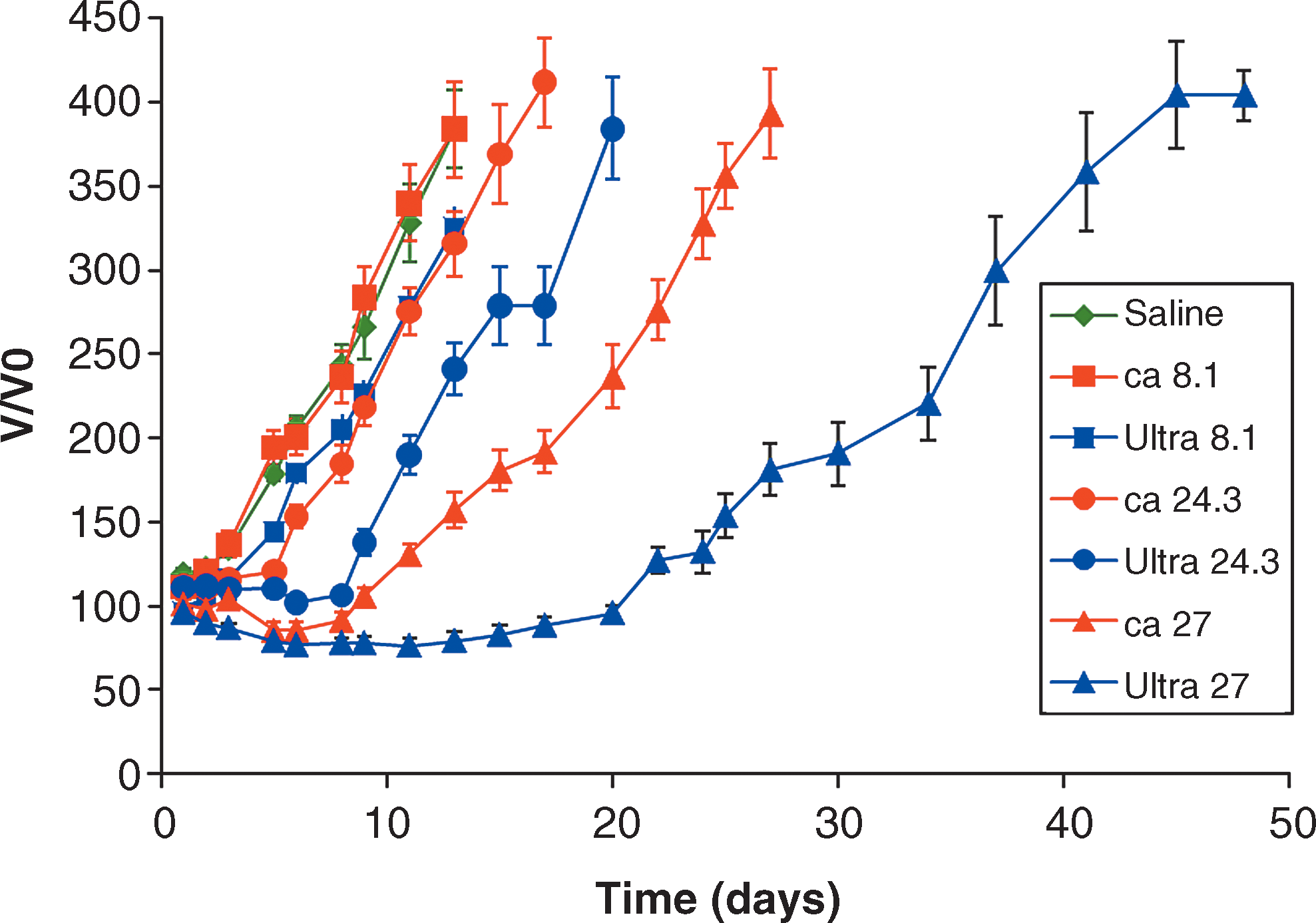
Effects of intravenously administered Ultratrace 131I-MIBG (Ultra) and carrier-added 131I-MIBG (ca) (manufactured by Amersham Biosciences) on tumor growth rate in the human neuroblastoma SK-N-BE(2c) mouse xenograft model. 131I-MIBG was administered as a single intravenous dose of 8.1, 24.3, and 81 mCi/m2 (2.7, 8.1, and 27 mCi/kg) and the effect on tumor growth rate was studied. The change in tumor volume is expressed as the mean ± standard error of the mean normalized to a pretreatment volume for separate groups of 8–10 mice each. MIBG, metaiodobenzylguanidine.
All values are expressed as the mean ± standard error of the mean.
MIBG, metaiodobenzylguanidine.
Discussion
Treatment success of radiopharmaceuticals depends on sufficient upregulation of the receptor or enzyme in the disease, the specificity of the target, choice of the radionuclide, and a sufficient concentration delivered to and retained at the target. 1 The selective targeted delivery of beta emitters to the tumor results in the formation of oxygen-derived free radicals, which interact among themselves to produce additional free radicals. The production of oxygen-derived free radicals is the primary mechanism by which beta radiation induces biological damage at lower radiation absorbed doses to the tumor. 11,12 Because of their rapid metabolic rate, tumor cells have developed several defense and repair mechanisms to deal with the generation of free radicals, the antioxidants being the primary mechanism. When an appropriate dose of beta radiation is administered, this primary defense mechanism can be overcome, resulting in the degradation of the damaged target proteins that culminates with apoptosis of the irreversibly damaged cells. 13,14 Iodine-131 is a desirable isotope for radiotherapy because it possesses both gamma energy for the detection of avid lesions and beta energy to induce tumor cell apoptosis. The targeting moiety described in this article, MIBG coupled with iodine-131, was chosen for the treatment of neuroendocrine tumors because MIBG is an enzymatically stable analog of norepinephrine that has been shown to concentrate in highly sympathetically innervated tissues such as the heart and neuroendocrine tumors. 15 As the NET and presynaptic storage granules, as well as chromaffin granules, are saturable, the specific activity of the preparation may have dramatic effects on both the safety and efficacy of the radiodiagnostic/radiotherapeutic. Using the Ultratrace method, which removes virtually all of the nonradiolabeled MIBG, we were able to achieve specific activities of >1200 mCi/μmol for 123I-MIBG and 1600 mCi/μmol for 131I-MIBG. Andreview, a commercially available preparation of 123I-MIBG, has a specific activity of ∼1 mCi/μmol, whereas radiotherapeutic preparations of 131I-MIBG have specific activities between 1 and 10 mCi/μmol.
The working hypothesis of the present study is that the Ultratrace MIBG will have a similar tissue distribution to the commercially available preparations in tissues with low sympathetic innervation but have superior uptake and retention in those that are highly innervated. To test this hypothesis, the tissue distributions of the Ultratrace 123/131I-MIBG and the carrier-added 123/131I-MIBG were studied.
In the present study, the Ultratrace 123I-MIBG and the carrier-added 123I-MIBG showed similar tissue distribution and pharmacokinetics of radiolabeled compound in most tissues. For the amount of carrier examined here, in the carrier-added preparation there was a 300–1000-fold increase in the transporter exposure to MIBG total mass when compared with the Ultratrace preparation, resulting in, as anticipated, 50% less agonist exposure to the heart compared with the carrier-added preparation (Figs. 2 and 3). These results are in agreement with those of Verberne et al., 8 who demonstrated that decreasing the specific activity from 5.4 to 1.1 mCi/μmol resulted in a decrease of ∼20% in cardiac radioactive uptake. In addition, the present study assessed the impact of MIBG on the cardiovascular system and demonstrated that i.v. administered MIBG elicited a dose-related increase in arterial pressure concomitant with a reflex bradycardia in the normal canine. These results clearly show that the amount of cold carrier administered not only will have an impact on ability to accurately study the sympathetic innervation of the diseased heart but also may have cardiovascular safety implications for increase in blood pressure. Further, these data are consistent with the hypothesis that MIBG tissue uptake is an active process and that the cold carrier MIBG competes with 123I-MIBG for target binding.
The impact of the cold carrier MIBG, administered at therapeutic levels, on tissue distribution was studied in normal rats. In the present study, the Ultratrace 131I-MIBG was fortified with unlabeled MIBG to mimic the total amount of the cold carrier MIBG in doses of 5 or 10 mCi/kg products currently administered to patients. The amount of MIBG present at these levels using the Ultratrace 131I-MIBG was ∼0.06 μg/kg (5.7 ng/mCi). Similar to what we observed with the Ultratrace 123I-MIBG, no differences in tissue distributions in low sympathetic innervated tissues were noted between 46.5–93 mg/mCi carrier-added 131I-MIBG and Cis-US 131I-MIBG when compared with the noncarrier-added Ultratrace 131I-MIBG. In the heart, however, when compared with the Ultratrace 131I-MIBG, a dose-related reduction in retention of and exposure to 131I-MIBG was observed because of its high innervation. Similar results were observed by Mairs et al., 16 who demonstrated, in the mouse, no changes in tissue distribution of the carrier-added and the noncarrier-added 131I-MIBG in tissues with low sympathetic innervation, but a marked reduction in cardiac exposure was also observed. Interestingly, a trend toward higher levels of uptake of 131I-MIBG in the bone marrow was noted, with increasing amounts of the cold carrier MIBG. Similar observations were made by Boyd et al., 17 who found a lack of myelosuppression in mouse xenograft studies using the Ultratrace 131I-MIBG. The reason for these findings is poorly understood. Additional studies to further evaluate this finding are planned. The results of the cardiovascular assessment in dogs clearly show that care must be taken when administering the carrier-added 131I-MIBG because at therapeutic doses of between 5 and 10 mCi/kg the total amount of MIBG administered will be between 300 and 1000 μg/kg, whereas in the case of the Ultratrace noncarrier-added 131I-MIBG it will be 0.06 μg/kg. As observed in the canine cardiovascular assessment, MIBG at 0.06 μg/kg will have no effect, whereas higher doses of 300 and 1000 μg/kg will result in a marked increase in arterial pressure concomitant with a reflex bradycardia.
On the basis of the working hypothesis and the results discussed in the present study, the utilization of the Ultratrace 131I-MIBG as a therapeutic agent suggested the possibility of improved tumor kill and increase in the therapeutic index. To assess this hypothesis, the effects of the Ultratrace 131I-MIBG (specific activity 1283 mCi/μmol) and the commercially available carrier-added 131I-MIBG (Amersham Health specific activity = 8.25 mCi/μmol) in the human neuroblastoma SK-N-BE(2c) mouse xenograft model were studied. Previously, in this model, Mairs et al. 16,18 compared the uptake and retention of the carrier-added and the noncarrier-added 131I-MIBG at 4.5 mCi/kg in the SK-N-BE(2c) mouse xenograft model. In their study, they observed greater uptake in the tumor by using the noncarrier-added 131I-MIBG, which resulted in a tumor radiation absorbed dose that was 2.3 times greater for the noncarrier-added 131I-MIBG than for the carrier-added 131I-MIBG. In the present study, at each comparable administered dose, the Ultratrace 131I-MIBG elicited a greater and more durable reduction in tumor growth when compared with the identical administered dose of the carrier-added 131I-MIBG. These results are in agreement with the work of Boyd et al., 17 who studied the effects of the Ultratrace 131I-MIBG (SA ≥780 mCi/μmol) and the commercially available carrier-added 131I-MIBG (Amersham Biosciences; SA = 8.3 mCi/μmol) on tumor uptake and efficacy in vivo by using the UVW/NET mouse xenograft model. In the present study, comparative imaging of mice administered the commercially available or the Ultratrace 131I-MIBG preparation clearly demonstrated superior in vivo uptake with the Ultratrace 131I-MIBG when compared with the carrier-added preparation. In the therapeutic study, a single dose of either the carrier-added or the Ultratrace 131I-MIBG showed a dose-related inhibition of tumor growth with both preparations. In all cases, the Ultratrace 131I-MIBG was superior to the same dose of commercially available 131I-MIBG. Notably, a single dose of 20 mCi/kg (60 mCi/m2) Ultratrace 131I-MIBG resulted in no tumor growth for >47 days.
Conclusions
In summary, the carrier-free Ultratrace MIBG radiolabeled with either 123I or 131I exhibited similar tissue distribution to the carrier-added radiolabeled MIBG in all tissues that do not have high sympathetic innervation. In highly sympathetically innervated tissues such as the heart and neuroendocrine tumors, it was observed that the higher the specific activity of the preparation the greater will be the radiopharmaceutical uptake, which, in the case of a tumor, translated into a greater and more durable reduction in tumor growth. The targeted increased uptake and retention of the Ultratrace 123/131I-MIBG as well as reduction in MIBG mass per dose may translate into a superior diagnostic and therapeutic activity. These data are consistent with the hypothesis that MIBG tissue uptake is an active process and that the cold carrier MIBG competes with 123/131I-MIBG for target binding. Lastly, care must be taken when administering therapeutic doses of the current carrier-added 131I-MIBG products because of their potential to cause adverse cardiovascular side-effects.
Footnotes
Disclosure Statement
R.J. Mairs serves in the Research Advisory Board of Molecular Insight Pharmaceuticals, Inc. J.A. Barrett, J.L. Joyal, S.M. Hillier, K.P. Maresca, F.J. Femia, J.F. Kronauge, and J.W. Babich are employees of Molecular Insight Pharmaceuticals, Inc.