
Abstract

“It's tough to make predictions … especially about the future!”
Introduction
This editorial was generated during the health care debate and months before its publication. Health care reform may have been adopted in the interim, despite a lack of consensus on what is required. The US health care system needs to be reformed! The status quo is unsustainable! In 2007, the health care industry accounted for more than $2.4 trillion or about 17% of the U.S. gross domestic product. Tens of thousands of dollars per person per year are expended for health insurance. About 50 million people are uninsured.
Legislation to expand coverage, control costs, and modernize the health system has been advanced. These euphemisms obscure the fact that the health care debate is focused on the wrong solutions, once again. Specific proposals range from electronic medical records and reduced reimbursement for specialists to a single-payer national health insurance system; these proposals have proven counterproductive in the past. Although the electronic medical record improves accounting and other recordkeeping, it diverts attention from the patient. Shifting dollars from specialists to providers from primary care disciplines has failed in the past. National health insurance to cover everyone will increase costs. Let's be honest! Somebody pays for expanded coverage of any type!
Yes, we need to tame health care costs and enhance its quality while attempting to cover more uninsured individuals. Surveys show that the people want the government to expand health care while containing costs, controlling excesses, and providing safety nets for the less fortunate. The patient and the patient's primary care-provider (to be distinguished from a provider from a primary care discipline!) must be empowered to improve health care while controlling costs. Using incentive programs, these individuals should be made responsible for cost-effective care. A single-payer system can dictate who is eligible for which services and for what technology but lacks sufficient wisdom to assure that every patient receives quality care. Politicians promise that which they cannot deliver and for which they do not provide payment. Government can influence the marketplace by example and through educational efforts and political pressure. The people do not want band-aids nor do they want big government nor big business. Big has proven bad thus far!
We wish to express opinions on U.S. health care reform that stem from our experiences as providers and as patients in the U.S. health care system and our exposure to national health care systems in other countries.
U.S. health care reform should build around the following: Choice of physician and health care coverage; Personal responsibility for health and health care costs; and An incentive program for each patient's designated primary care provider (i.e., “captain of the ship”) and for the patient.
False Promises
Strong words suggest a weak cause. To quote a syndicated newspaper columnist, “After all, every other advanced country offers universal coverage while spending much less on health care than we do.” The column proceeded to suggest that controlling health care costs and expanding health care access would not raise costs because the uninsured do not require much care. Left unanswered were questions, such as: Why? If we bankrupt the nation? The health care system? U.S. industry?
What is meant by “affordable, portable health insurance for all Americans?” There is a deep divide between those that acknowledge that someone ultimately pays for health care and those that refuse to acknowledge that there are no “free lunches” (except, perhaps, those provided by lobbyists). Health care has become much too expensive and its cost continues to increase at an alarming rate. The cost per individual for health care in the United States is about twice that of other countries. Although everyone desires the best health care, decreasing the cost of health care must be a priority! Quality care at reasonable cost is feasible if the focus is on the patient and not on technology.
Status of U.S. Health Care
People in the United States are no longer the healthiest in the world. U.S. health care is good, but its quality has decreased while its cost has increased. Policy makers can make changes that make Americans healthier but have not done so over the decades. Health care is about care and not about making money. Delivery of care to a patient is a privilege bestowed by a responsible patient on a provider (and system), who share responsibility for health and even life. For too many, it has become a lucrative business. Health care providers need to be reminded that ministering to another human in need is a greater source of gratification than driving “Beemers and Hummers.”
Responsibility of Provider and Patient
Examples of U.S. health care systems when providers and patients shared responsibility and trust, and when otherwise.
Then
More than 50 years ago, one of the authors, as a child, became ill with a high fever. The concerned mother took the child to the family physician, a general practitioner, who diagnosed “fall-itis,” as it was in the fall of the year. No tests, drugs, or antibiotics were involved; only a brief history, examination, reassurance, and supportive care. Two (2) months later, a bill for $7.50 arrived by mail. Before the last installment was paid by the family, a similar illness occurred; the physician diagnosed “spring-itis,” as it was spring, and similar billing events ensued. These unplanned expenses did not noticeably affect the family menu, even though the “patient” and the provider accepted their respective responsibilities.
Now
Despite choosing primary care physicians known to value a thorough history and examination, referrals often get into “procedure bins.” By way of example, one of the authors, with a long-standing skin lesion, found himself in a white gown left to approve an operative procedure, rather than meeting with the consulting dermatologist, as anticipated. Had not the physician been upset by the providers' “counter” signs, an expensive “hole in the face” could have ensued. Evaluation by the skin specialist led to the recognition of, and (liquid nitrogen) treatment for, a benign lesion, rather than the primary care provider's diagnosis of a basal-cell cancer. The difference in costs was thousands of dollars.
Even though billing hundreds and, often, thousands of U.S. dollars, health system “counters” demand more. Signs declare that fees and copays are required at the time of service. Credit cards are accepted! While accepting that cost sharing by the patient has been shown to contribute to better health and lower costs, it seems incongruous that the patient entrusts health, and even life, to the health care system and cannot be trusted to pay for services! Should not both the provider and the patient be responsible and trustworthy? Why has there been a change? Health care became a big business. Patients have been led to expect “free lunches.”
Primary Care Provider: “Captain of the Ship”
The economics of health care encourage procedures, rather than care. Compensating health care organizations and providers on the basis of quantity of services must be stopped! Primary care providers should be motivated to provide care, rather than services. Physicians need to be encouraged to be “healers” and not “bean counters.” The current system spurs a relentless drive to increase services with little reward for counseling the patient and family and for coordinating the patient's care.
The health care team needs to be coordinated by a primary care provider (whether physician, specialist, or other provider), the “captain of the ship,” who requires compensation for counseling and for coordinating care (Fig. 1). Each patient should designate his or her most significant health care provider, the captain of the ship, annually. It could be a family practitioner one year, a cardiologist or oncologist another year, and a pain specialist another year, depending on the patient's health issues. Although the traits that characterize a good captain-of-the-ship primary provider can be selected for, and reinforced by, educational programs, many programs focus on traits more characteristic of “technocrats,” including educational programs that are identified with the primary-care disciplines. Patients and providers should be educated and empowered to question “procedural medicine.” The patient and the captain of the ship must be rewarded for efforts that decrease the volume of “care” and, therefore, its cost.
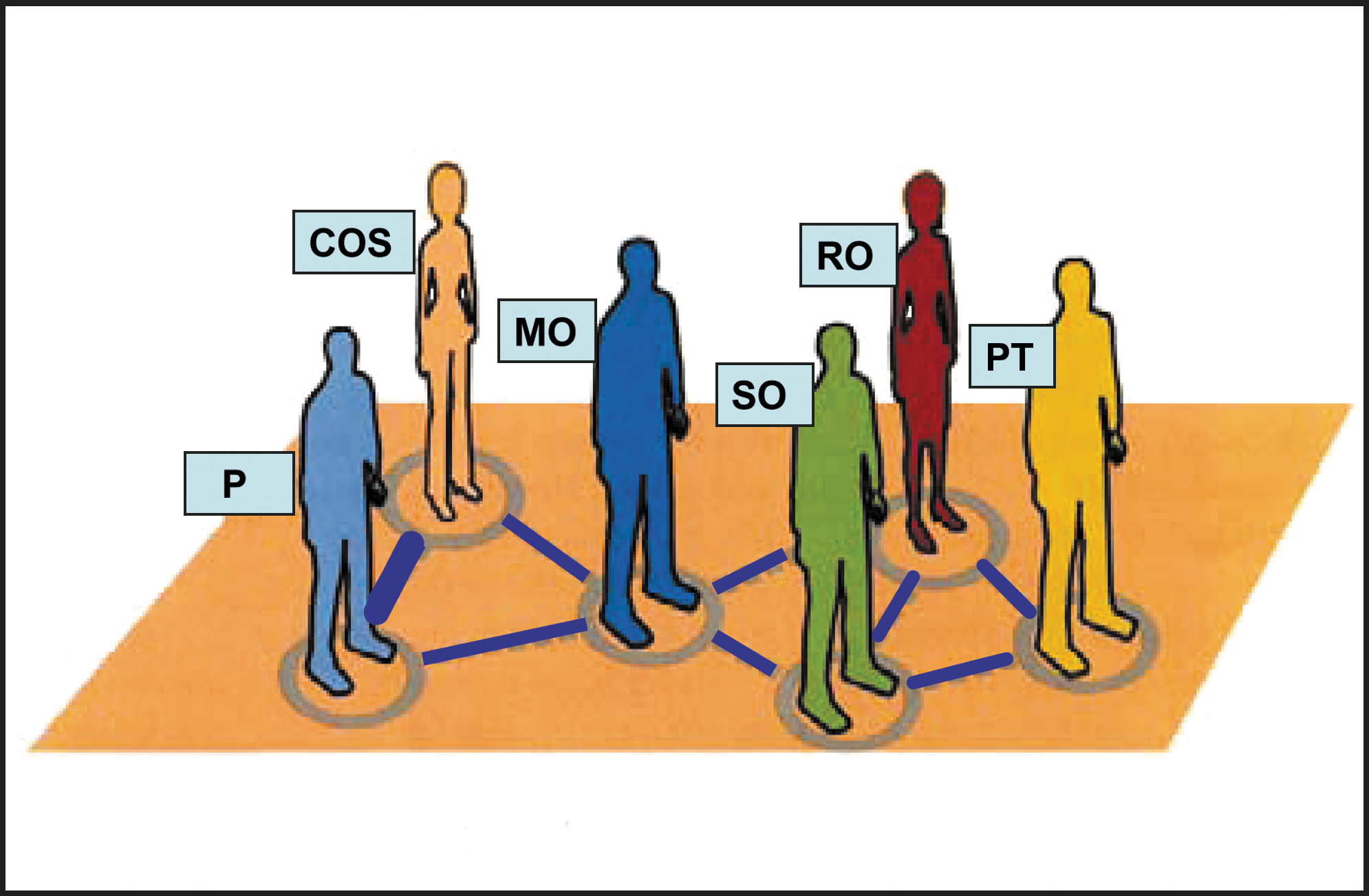
Example of a patient (P) and the “captain of the ship” (COS) provider coordinating the patient's cancer care, along with the health care team (medical oncologist, MO; radiation oncologist, RO; surgical oncologist, SO; and physical therapist, PT, in this instance).
As importantly, nonprofit organizations should be penalized for using taxpayer dollars to develop competing facilities on each corner, a “gas station” mentality.
Personal Responsibility
To assure quality care for those that need it, while controlling its cost, some form of “rationing” seems inevitable. What can each of us do? Each of us can, and must, accept responsibility for our health and the cost of health care. This means a personal responsibility to avoid self-abusive behaviors, such as excessive consumption of food, nicotine, alcohol, drugs, and so forth. Each individual has responsibility for self and to others. What can each of us get? A better health care system, one that is cost effective and does not lead to job loss. A health system that is viable over time.
Summary
Yes, the U.S. health care system needs to be reformed! The growth of costs is unsustainable and will bankrupt the U.S. economy. The system can be fixed, despite the political implications. We must be honest, and we must learn from the mistakes of the past. The goals include lowering costs, improving quality, retaining freedom of choice, and covering more Americans. There must be a balance between the “right” to health care and the right to avoid undue financial burden. Expanded coverage may be humane and appropriate; it will cost someone!
A healthier America depends on a return to individual responsibility and a movement away from a “bigger is better” mentality. There must be acceptance of the principle that it is a trust and a privilege to care for a responsible patient. The patient's primary care provider, the captain of the ship, not some large organization, must be compensated for patient counseling and for coordinating care and reducing dependence on procedures.
Letters to the Editors on this editorial and other topics, related or otherwise, are welcomed.