
Abstract
Somatostatin analogs (SSA) are the standard diagnostic and treatment tools in the clinical management of patients with neuroendocrine tumors (NETs) expressing somatostatin receptors (SSTRs). Although symptomatic and biochemical control is obtained with SSA in the majority of functional NETs, antineoplastic effects of SSA are partial and of limited duration. The aim of this study was to quantify expression levels of five SSTR subtypes (SSTR1–SSTR5) and correlate them with the clinical outcomes of patients with NETs who underwent SSA therapy. The expression levels were analyzed using real-time polymerase chain reaction in a series of 22 metastatic NETs with a median time of 10 months on the SSA therapy (range 2–82 months). The median duration of disease stabilization in patients who developed progression (n = 14) was 9 months (range 3–92 months). The median survival period for all patients was 44 months (range 3–175 months). According to RECIST criteria, one (5%) partial objective tumor response was obtained, disease stabilization was achieved in 10 (45%) patients, and progressive disease was observed in 11 (50%). Analysis of mRNA expression of the SSTR subtypes showed that SSTR2 and SSTR5 were expressed in all of the studied NETs; SSTR1 and SSTR4 in all but 3 tumors (86%); and SSTR3 in only 10 NETs (49%). Interestingly, our preliminary data suggest that only the levels of SSTR4, though it has the lowest affinity for SSA of all SSTR subtypes, were significantly associated with the stabilization of disease during SSA therapy (p = 0.0357). These levels correlated with time to progression (p = 0.0015) and overall survival (p = 0.0017) in NET patients.
Introduction
Neuroendocrine tumors (NETs) represent a heterogeneous family of neoplasias that may develop from various endocrine glands (such as pituitary, parathyroid, or neuroendocrine adrenal glands), endocrine islets (within the thyroid or pancreas), as well as from endocrine cells dispersed between exocrine cells throughout the digestive and respiratory tracts. 1 –3 The development of somatostatin analogs (SSA) as important diagnostic and treatment tools has revolutionized the clinical management of patients with NETs expressing somatostatin receptors (SSTRs). 4
Today, SSA are commonly used to obtain symptomatic control in functional NETs. However, inhibition of tumor growth and occasional objective responses have been also reported. These effects occur as a result of inhibition of hormone secretion, antagonism with growth factors, or direct antiproliferative effects on tumor cells mediated by specific SSTRs. 5 –7 To date, five subtypes of SSTR have been cloned and characterized. 8 –10 The molecular mechanisms of SSA antiproliferative action need to be elucidated. The analogs presently available for clinical use (octreotide and lanreotide) bind to SSTR2 and SSTR5 and, at higher doses, also to SSTR3, 11 which has been shown to promote apoptosis. 12 Differential expression of SSTRs, especially SSTR2, seems to be important in predicting the results of SSTR scintigraphy (SRS) and therapeutics, mainly symptomatic response to SSA. 5,13 –18
Relatively few data are available concerning the semiquantitative expression of SSTR subtypes in NETs from studies using densitometry for autoradiography, immunohistochemistry, and real-time polymerase chain reaction (PCR) analysis. 6,8,9,11 A good correlation between real-time PCR and immunohistochemistry has been found in NETs, indicating that the former method may indeed be sufficiently accurate in detecting SSTR subtypes. 5 Till now, only one report focusing on quantification of SSTR gene expression in NETs by use of real-time qPCR exists, but not in regard to SSA therapy response. 19
The purpose of this study was to quantify the expression levels of SSTRs (SSTR1–SSTR5) as possible biomarkers of NETs with real-time qPCR and to evaluate their possible role in the stabilization of disease during standard SSA treatment regimen in NET patients. The relevance of SSTR expression levels in predicting time to progression and overall survival in NET patients were analyzed.
Patients and Methods
Study population
Twenty-two (22) tumor specimens obtained from patients with metastatic NETs (11 men and 11 women, age 62 ± 22 years) were formalin-fixed after resection or biopsies. All tumors were functional in terms of the presence of symptoms caused by hormonal overproduction. Symptomatic control was achieved with octreotide only (n = 16), lanreotide only (n = 2), or both sequentially (n = 4). The tumor markers plasma chromogranin-A (p-CgA) and 24-hour urinary 5-hydroxy-indolylacetic acid (u-5-IHAA) were measured in all the patients before treatment and then every 4 weeks during treatment. Treatment activity was evaluated after 6 months of therapy by objective response according to RECIST criteria using computed tomography scans. General clinical and pathological characteristics of the patients are summarized in Table 1. Informed consent approved by the local ethical board was obtained from each patient. Clinical data were retrieved from the Masaryk Memorial Cancer Institute's (Brno, Czech Republic) patient records.
According to the WHO 2000 classification, classic structural criteria are combined with Ki-67 score and mitotic rate.
ECOG, Eastern Cooperative Oncology Group; WHO, World Health Organization; IFN, interferon.
Tissue sample preparation and RNA isolation
Formalin-fixed paraffin-embedded specimens of NETs (containing >90% tumor tissue) were dissected and placed in nuclease-free microcentrifuge tubes under the supervision of an experienced pathologist. One milliliter (1 mL) of xylene was added for deparaffinization with vortexing for 5 minutes at room temperature. The samples were left at 60°C for 3 minutes and then centrifuged at 14,000 rpm for 7 minutes at room temperature. Supernatants were removed, and 1 mL of 100% ethanol was added with vortexing for 7 minutes. This ethanol washing step was repeated twice. Samples were then air dried, and 360 μL of digestion buffer containing 30 mM Tris-HCl, 20 mM ethylenediaminetetraacetic acid, 1% sodium dodecyl sulfate (all from Sigma), and nuclease-free water were added to the tubes. Samples were homogenized and, after adding 40 μL of Proteinase K (Qiagen) solution, incubated at 56°C until the tissue was completely digested (>3 hours). Total RNA was isolated with the RNeasy Mini Kit (Qiagen) according to the manufacturer's instructions. RNA concentration and purity were controlled by ultraviolet spectrophotometry (A260:A280 > 2.0; A260:A230 > 1.8) using Nanodrop ND-1000 (Thermo Scientific).
Reverse transcription and real-time qPCR
cDNA was obtained by reverse transcription (Thermocycler Tgradient; Biometra). For this, the reaction mixture containing 1 μg of total RNA, random hexamers (Qiagen), and ribonuclease-free water was incubated at 65°C for 5 minutes, then cooled quickly on ice, and the following components added to 20 uL final volume: 5 × Reaction Buffer, Ribonuclease Inhibitor, dNTP mix, Revert Aid™ M-MuLV H-Reverse Transcriptase (all from Fermentas), and ribonuclease-free water. The mixture was incubated for 120 minutes at 42°C, and the reaction was stopped by heating the mixture at 95°C for 5 minutes and chilled on ice.
The real-time PCR was performed using Applied Biosystems 7000 Sequence Detection System according to the manufacturer's recommendations. The PCR mixture, with a total volume of 25 μL, included 4 μL of the reverse transcription product, 1 × TaqMan Universal PCR Master Mix, and 1.25 μL of primers and probe mix of the TaqMan Expression Assays for SSTR1–SSTR5 (SSTR1, Hs00265617_s1; SSTR2, Hs00990356_m1; SSTR3, Hs00990356_m1; SSTR4, Hs01566620_s1; SSTR5, Hs00265647_s1; Applied Biosystems). The mixture was incubated in 96-well optical plates at 95°C for 10 minutes, followed by 40 cycles of 95°C for 15 seconds and 60°C for 10 minutes. The Ct data were determined with default threshold settings. All reactions were run in triplicates, and average Ct and standard deviation values were calculated.
Statistical analysis
Expression data were normalized according to the expression of the housekeeping gene GAPDH (Assay No. 402869; Applied Biosystems). Statistical differences between clinicopathologic parameters and mRNA levels were evaluated using the Mann–Whitney U-test between two independent groups. The long-rank test was used to measure the differences in Kaplan–Meier curves. p-Values lower than 0.05 were considered to be significant. All calculations were performed with the software Statistica (StatSoft Inc., version 6.0).
Results
Response to treatment and follow-up
Twenty-two (22) patients with progressive metastatic NETs participated in the study. Patient characteristics are shown in Table 1. Thirteen (13) patients had elevated tumor markers (p-CgA in 6, u-5-IHAA in 4, and both markers in 3 patients), 4 patients did not present with elevation of tumor markers, and for 5 patients p-CgA and u-5-IHAA levels were not available. Octreotide scintigraphy (octreoscan) was positive in all 22 patients (see Fig. 1). According to RECIST criteria, one (5%) partial objective tumor response was obtained, disease stabilization was achieved in 10 (45%) patients, and progressive disease was observed in 11 (55%) patients (2 patients died of some nononcological cause). Among the 20 patients evaluable for symptomatic response, the overall response rate was 95%, while 2 (10%) patients showed complete response (asymptomatic). Seventeen (17) (85%) patients indicated improvement in the symptoms. Of the 13 patients who were assessable for biochemical response, 2 (15%) achieved stabilization of both markers (p-CgA and u-5-IHAA), 8 (62%) experienced decrease in one of the analyzed markers, and 3 (23%) showed no effect on the marker levels. The median time on SSA therapy was 10 months (range 2–82 months). There were no serious drug-related adverse events. The median duration of disease stabilization in patients who developed progression (n = 14) was 9 months (range 3–92 months). The median survival period for all patients was 44 months (range 3–175 months).
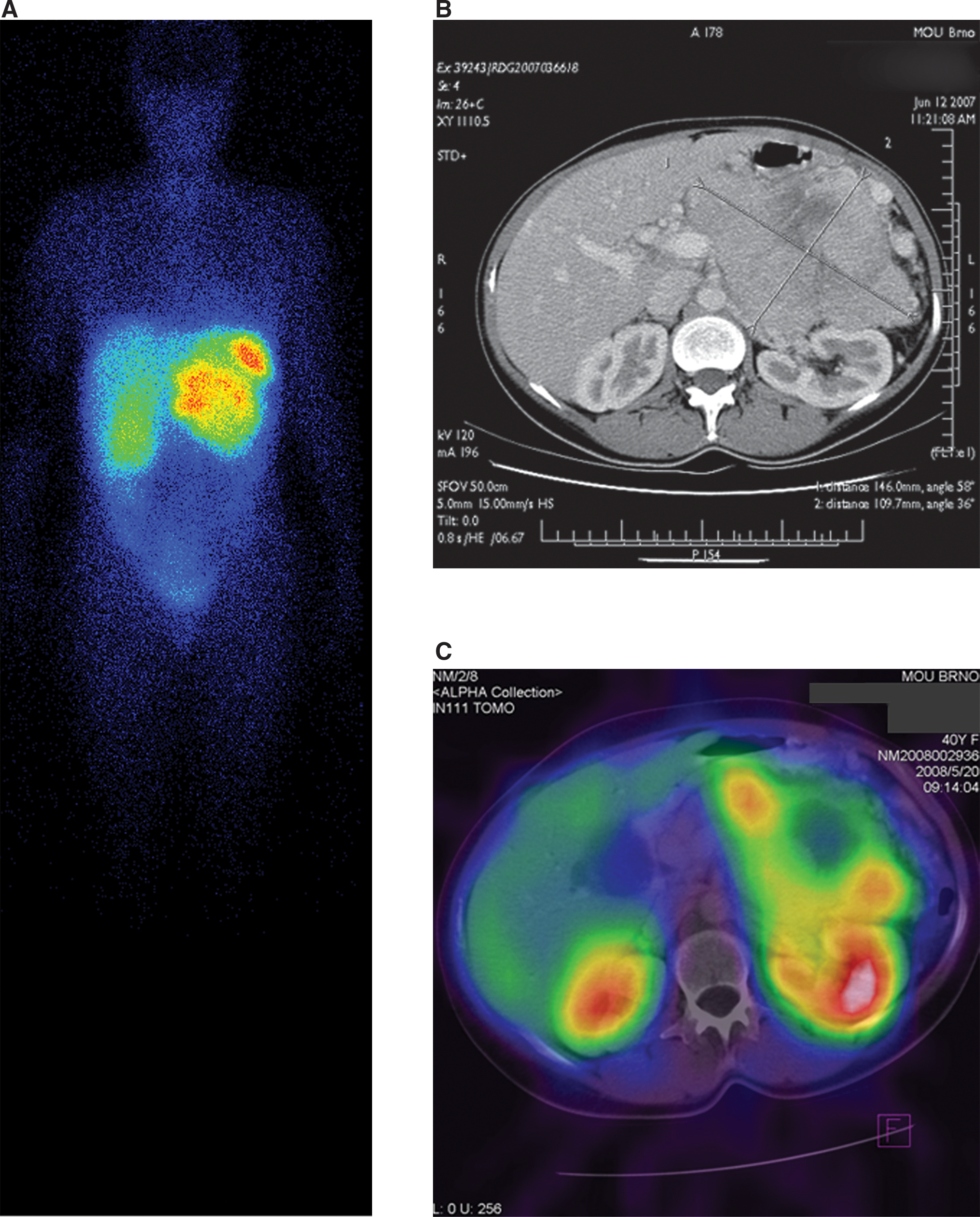
111In-pentetreotide (octreotide) whole-body SPECT scintigraphy and SPECT/C image fusion in a 40-year-old woman with an enormous abdominal mass of neuroendocrine tumor. (
Comparison of SSTR expression levels with clinicopathological features and outcome of NET patients
The expression levels of SSTR1–SSTR5 in the group of patients with stable disease were compared with their levels in the group of patients with progressive disease to evaluate the potential significance of SSTRs in the prediction of outcome. Patients with stabilized disease during SSA therapy tended to have lower expression levels of SSTR4 than those with progressive disease. SSTR4 was significantly decreased (p = 0.0357) in the NETs of patients who responded to therapy (see Table 2 and Fig. 2). However, no association was found between stabilization of disease and treatment response with regard to SSTR1, SSTR2, SSTR3, and SSTR5 (see Table 2). Lower levels of SSTR4 were also associated with significant improvement in time to progression (p = 0.0015) and overall survival (p = 0.0017) of NET patients (Figs. 3 and 4). There was no association between any of SSTR gene expression and Ki-67 score and mitotic rate.

Association of normalized SSTR4 expression levels with objective response to somatostatin analog therapy evaluated after 6 months of treatment (Mann–Whitney U-test, p = 0.0357). SSTR, somatostatin receptor.

Kaplan–Meier curves showing time to progression of disease in groups of patients with different expression levels of SSTR4 gene (long-rank p = 0.0015). SSTR, somatostatin receptor.
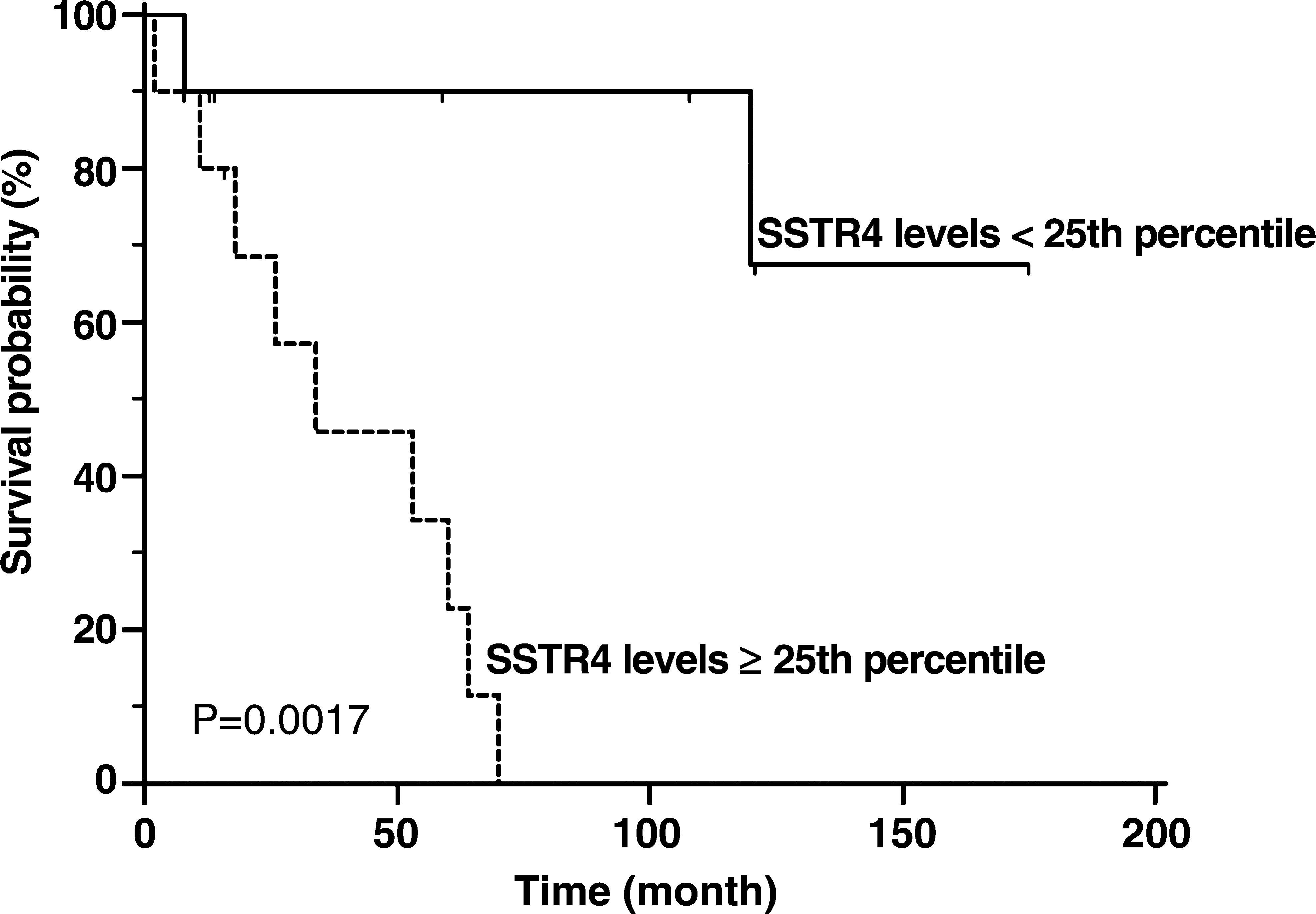
Kaplan–Meier curves showing overall survival of patients based on different expression levels of SSTR4 gene (long-rank p = 0.0017; 2 patients in the SSTR4 low-level group died of non-oncological cause). SSTR, somatostatin receptor.
Medians of expression are related to glyceraldehyde-3-phosphate dehydrogenase (GAPDH) levels, with the 25th–75th percentile in parenthesis. The percentages of tumors expressing a receptor subtype are indicated below medians data.
p-Value according to Mann–Whitney U-test between two groups (significant differences are bolded).
NET, neuroendocrine tumors; SSA, somatostatin analogs; SSTR, somatostatin receptor.
Discussion
Studies examining the antiproliferative role of SSA in NETs are difficult to interpret because of heterogeneity of tumor types, use of various formulations and doses, and possible lack of objective tumor progression prior to treatment with SSA. Eriksson and Oberg, 20,21 however, collected data from 62 published studies or mini-series pertaining to treatment with octreotide. In those studies, tumor shrinkage was reported in only 10%–20% of patients, but stabilization of tumor growth for 8–16 months could have been achieved in about half of the patients. 20,21 These data are in accordance with the observations in the present study, where partial tumor regression was achieved in 1 (5%) patient and disease stabilization in 10 (45%), with the median duration of disease stabilization being 9 months. Symptomatic and biochemical response rates were comparable with published observations as well. 20,21
The aim of our study was to identify expression levels of SSTR genes by standardized real-time PCR and evaluate their potential value in predicting the time to progression, overall survival, and stabilization of disease during SSA treatment in NET patients. Analysis of mRNA expression of SSTR subtypes in a series of 22 NETs with different sites of origin by real-time qPCR showed that SSTR2 and SSTR5 were expressed in the totality of the studied NETs, SSTR1 and SSTR4 in all but 3 tumors (86%), and SSTR3 in only 10 NETs (49%). These data confirm the frequent and heterogeneous expression of most mRNA subtypes in NETs. Similar results concerning SSTR2, SSTR3, and SSTR5 were also previously observed in 38 patients with NETs (mostly pancreatic) using semiquantitative PCR, although SSTR1 was less frequently observed (66%) and SSTR4 expression was positive in 100% of the NETs analyzed. 8 O'Toole et al. 19 identified analogous expression of SSTR1 (100%), SSTR2 (100%), SSTR3 (63%), and SSTR5 (100%) in 35 NETs by using real-time qPCR. In that study, SSTR4 expression was not quantified. SSTR1–SSTR3 mRNAs were detected at a frequency similar to that reported in previous studies by Kubota et al. 6 and Jais et al. 8 In the present study, SSTR5 mRNA was detected in the majority of tumors analyzed, which is consistent with the findings of Jais et al. 8 Interestingly, Kubota et al. 6 did not detect SSTR5 in any of the seven tumors studied. These discrepancies may be attributed to technological differences and the small number of patients involved in these studies because of low incidence of NETs. The sequence homologies of SSTR subtypes could also account for these conflicting results because different primer sets might be used in evaluating the mRNA expression of SSTR subtypes. In the present study, primer sets and probes paired to the most nonhomologous sites of SSTR isoforms as possible were selected, to circumvent any misinterpretation of the data.
SRS is performed not only for tumor localization but also for predicting the efficacy of SSAs or of modified radiopharmaceutical analogs. 22 –25 However, in some case, SRS results do not correlate with treatment results. 26 –28 Actual SRS using 111In-pentetreotide recognizes mostly the SSTR2 subtype. Pentetreotide shows a 10-fold higher affinity for SSTR2 than for SSTR5 or SSTR3. 4 Previously, semiquantitative real-time PCR revealed most prominently SSTR2 expression in scintigraphic positive tumors. 21 Under the conditions in the present study, there were differences in the objective responses to SSA therapy (according to RECIST criteria), time to progression, and overall survival, although totality of the studied NETs were SSTR2 positive. Thus, SSTR2 levels indicate no predictive capability, even when quantified. Interestingly, SSTR4, though it has the lowest affinity for SSA of all SSTR subtypes, was significantly associated with the stabilization of disease during SSA therapy (p = 0.0357) and strongly correlated with time to progression (p = 0.0015) and overall survival (p = 0.0017) in NET patients. The possible molecular mechanism through which SSTR4 participates in the SSA therapy antineoplastic effects may be based on the dimerization of SSTRs, as observed for SSTR2–SSTR3 and SSTR1–SSTR5. 29 Although SSTR2–SSTR4 heterodimerization has not been observed till now, recent studies suggest the existence of functional interactions between these two subtypes. 30
Conclusions
In conclusion, to our knowledge, this is the first study to demonstrate an association between the gene expression of SSTR subtypes and variables related to the response to SSAs treatment. The negative correlation between SSTR4 expression, stabilization of disease, time to progression, and overall survival suggests that SSTR4 may play an important role in the molecular mechanism of SSA-induced antineoplastic effects in NETs. Further studies and validations are needed, however, to prove our preliminary observations, because only a small, heterogenous group of patients was studied here. If validated, it would pave the way for better treatment decisions and, ultimately, an improvement in the quality of life and survival rate of patients with NET.
Footnotes
Acknowledgments
This work was supported by the Project MZ0MOU2005 of the Czech Ministry of Health.
Disclosure Statement
The authors have no financial conflict of interest.