
Abstract
Monoclonal antibodies (mAbs) have been approved for therapeutic use in a broad range of medical indications, especially in oncology, and are forming the most rapidly expanding category of pharmaceuticals. Although engineered mAb fragments and nontraditional antibody-like scaffolds are receiving increasingly more attention, most of the mAb candidates evaluated in past and ongoing clinical trials are full-length mAbs. Immuno-positron emission tomography (PET), the tracking and quantification of mAbs with PET in vivo at superior imaging quality, is an exciting novel option for better understanding the in vivo behavior and efficacy of mAbs in individual patients. This review focuses on immuno-PET with full-length mAbs, and the associated use of the long-lived positron emitters zirconium-89 (89Zr) and iodine-124 (124I). Very recently, crucial achievements have been obtained to allow broad-scale application of 89Zr- and 124I-immuno-PET in clinical mAb development and applications. 89Zr and 124I became commercially available worldwide for clinical use. A chelate for facile coupling of 89Zr to mAbs became commercially available, and generic procedures for labeling of mAbs with 89Zr and 124I in a current good manufacturing practice compliant way were established. In this review, critical aspects for the translation of immuno-PET from preclinical investigations to clinical trials will be discussed, as well as the potential clinical applications of immuno-PET. An overview of the results of the first clinical immuno-PET studies will be provided.
Introduction
Recent advances in molecular and cellular biology have facilitated the discovery of novel molecular targets for tumor cells, for example, key molecules involved in proliferation, differentiation, cell death and apoptosis, angiogenesis, immune recognition, invasion, and metastasis or associated with cancer cell stemness. 1 This knowledge has boosted the design of cutting-edge pharmaceuticals, with monoclonal antibodies (mAbs) forming the most rapidly expanding category. Presently, 22 mAbs, of which 19 are intact immunoglobulins, have been approved by the U.S. Food and Drug Administration (FDA) for therapy, most of them for systemic treatment of cancer. 2,3 The yearly sales of mAbs have been estimated at $20 billion in 2006, 4,5 and the market is growing at ∼14% per year. 3 Eight (8) mAbs had a sales of >$1 billion in 2007. The clinical phase for FDA-approved anticancer mAbs took on average 90.8 months. 3 Over 200 new mAb candidates for treatment of cancer and immunological diseases are under clinical development by biotech and pharmaceutical firms worldwide, and also most of them are full-sized humanized and human immunoglobulin G antibodies rather than antibody fragments or antibody-like scaffolds. 6
Despite these commercial successes, it is fair to state that the efficacy of current mAbs remains quite limited, with benefit for just a portion of patients, and also approval of new mAbs directed against novel targets is stagnating. Moreover, the costs of mAb therapy are excessive, and this issue has become a subject of national discussions regarding the rights of cancer care. 7,8 The question is how to improve the efficiency of mAb development and the efficacy of mAb-based therapy and how to identify patients with the highest chance of benefit. In other words, when, how, and for whom should antibody-based therapy be reserved? Stakeholders in this arena are physicians (who want to have patients treated in an optimal way), pharmaceutical companies (who want to have rapid and cheap drug development, and application of mAbs in appropriate patient groups), insurance companies and health care authorities (who want to have optimal efficacy of medicines, at minimum price), and first of all the patients groups (who want to have highest probability for cure, at minimum morbidity). To answer these questions, better insight in the in vivo behavior of therapeutic mAbs and their interaction with critical disease targets in individual patients should be obtained. Immuno-positron emission tomography (PET) is an attractive novel tool for characterizing mAbs in vivo, because it enables quantitative imaging of mAbs at high resolution and sensitivity.
Monoclonal Antibodies
The introduction of the hybridoma technology by Kohler and Milstein 9 in 1975 was the starting point of the antibody revolution. With this technology, an unlimited range of mAbs can be obtained against any particular cellular antigen. However, the first generations of mAbs had limitations for clinical use, because their murine origin made them immunogenic. 10,11 Developments in recombinant DNA technology circumvented this, resulting in the production of chimeric mAb (cmAb), humanized mAb, and complete human mAb. Besides intact mAb molecules (molecular weight: ∼150 kDa), also mAb fragments and engineered variants are used, such as F(ab′)2, F(ab′), Fab, single chain Fv (scFv), and the covalent dimers scFv2, diabodies, and minibodies (molecular weights ranging from 25 to 100 kDa), 12 as well as several types of protein therapeutics based on nontraditional scaffolds, such as domain antibodies, 13 affibodies, 14 nanobodies, 15 and anticalins. 16 Although intact mAbs typically achieve optimal tumor-to-nontumor ratios at 2–4 days after injection, for the smaller fragments this is mostly 1–6 hours after injection. Currently, nine mAbs have been approved by the FDA for cancer therapy, all being intact mAbs (Table 1). Five of the mAbs have been approved for treatment of hematological malignancies: rituximab, gemtuzumab ozogamicin, alemtuzumab, ibritumomab tiuxetan, and tositumomab. Four mAbs have been approved for therapy of solid tumors: trastuzumab is used for treatment of metastatic breast cancer; cetuximab, bevacizumab, and panitumumab have been approved for treatment of metastatic colorectal cancer; and cetuximab and bevacizumab have also been approved for the treatment of head and neck cancer and non-small cell lung cancer, respectively. These “solid tumor mAbs” are most effective when combined with chemo- or radiotherapy. They interfere with signal transduction pathways by targeting growth factors or their receptors, the key drivers of tumor growth and survival. In addition, most of the naked therapeutic mAbs can also act via other effector mechanisms such as antibody-dependent cellular cytotoxicity, complement-depending cytotoxicity, or induction of apoptosis. To enhance its therapeutic potency, gemtuzumab has been armed with the supertoxic drug ozogamicin, whereas ibritumomab tiuxetan (Zevalin™) and tositumomab (Bexxar™) are radiolabeled mAbs containing the β-emitters yttrium-90 (90Y) and iodine-131 (131I), respectively. Because of a “cross-fire” effect, radionuclides are especially attractive as warheads to be used in radioimmunotherapy, as, to be effective, not all tumor cells have to be targeted by radiolabeled mAbs. Next to aforementioned mAbs, one naked mAb and one radioimmunoconjugate have been approved in China. 2 The therapeutic value of aforementioned mAbs has been outlined in several excellent reviews. 17 –19 Clinical successes with aforementioned therapeutic mAbs have boosted research and development on new mAbs directed against validated and novel targets enormously. 20
Conjugated antibodies.
FDA, U.S. Food and Drug Administration; CD, cluster of differentiation; IgG, immunoglobulin G; HER2/neu, human epidermal growth factor receptor 2; 90Y, yttrium-90; 131I, iodine-131; VEGF, vascular endothelial growth factor; EGFR, epidermal growth factor receptor.
In 2007, Reichert and Valge-Archer 2 reported on 206 unique therapeutic mAbs in clinical trials during the time period 1980–2005 by commercial companies worldwide for a variety of cancer indications. The 206 anticancer mAbs were specific for 76 targets. Of these 76, 43 were targets for only one mAb. Remarkably, 91 mAbs were specific for only 10 targets, and for most of these targets approved mAbs have become available in the mean time. These targets of highest interest included epithelial cell adhesion molecule (17 mAbs), epidermal growth factor receptor (EGFR) (12 mAbs), mucin-1 (MUC1/CanAg) (10 mAbs), CD20 (10 mAbs), carcino-embryonic antigen and HER2 (9 mAbs each), and CD20, CD33, Lewis Y, and prostate-specific membrane antigen (6 mAbs each). Taking into account the large number of mAbs directed against novel as well as validated targets under development, this raises the question about how to select the best mAbs in an efficient way.
Antibody Imaging in a Therapeutic Setting
Two different approaches of immuno-PET imaging are mostly followed to guide therapy with intact mAbs. In a first approach, fast kinetic antibody-based PET probes are used for same-day imaging at low radiation burden for patients, to confirm target expression, as recently described by Wu and coworkers. 21,22 This approach is potentially helpful for diagnostic purposes and as a scouting procedure for the selection of patients for therapy with intact mAbs. In a second approach, the therapeutic intact mAbs are radiolabeled themselves and imaged in a pretherapy scouting setting or early during the course of therapy to get a better insight in the in vivo behavior and efficacy of the mAbs in individual patients.
For the first approach, mAb fragments or small mAb-like molecules can be used. As for immuno-PET the physical half-life (t ½) of the radionuclide should be matched with the biological half-life of the protein to which it is being conjugated, for this application, gallium-68 (68Ga, t ½ = 1.13 hours), fluorine-18 (t ½ = 1.83 hours), copper-64 (64Cu, t ½ = 1.13 hours), 86Y (t ½ = 14.7 hours), and bromine-76 (t ½ = 16.2 hours) are the positron emitters of choice. Procedures for coupling these positron emitters to mAbs and preclinical results with short-lived positron emitters coupled to mAb fragments have been extensively discussed in recent reviews. 21 –29 Although excellent imaging results have been obtained with antibody-based PET probes in tumor-bearing mice, caution is needed when aiming the translation of these results to clinical applications. Although mAb reactivity with human tumors is considered to be similar for xenografted nude mice and cancer patients, cross-reactivity with normal organs can be totally different. This was demonstrated in PET imaging studies with anti-EGFR mAbs in nude mice bearing EGFR (HER1)-positive human cancer xenografts. Most mAbs, cetuximab and panitumumab included, bind only to human EGFR and not to murine EGFR, therefore showing predominantly high and selective tumor uptake. 30 –32 However, Tolmachev et al. 33 evaluated an 8-kDa affibody recognizing human as well as murine EGFR and observed a relatively high liver uptake and low tumor uptake. Liver uptake was particularly high at low affibody dose and could be explained by the abundant EGFR expression in this organ, which is consistent with abundant EGFR expression in human livers. Indeed, initial clinical imaging studies with 111In-labeled anti-EGFR mAb 225 also showed high liver uptake, whereas for imaging of EGFR expression in tumors, relatively high mAb doses were required. 34 Also recent clinical immuno-PET studies with zirconium-89 (89Zr)–trastuzumab demonstrated that a relatively high mAb dose of at least 50 mg is required to allow reliable HER2 imaging in breast cancer patients. At low mAb doses, rapid hepatic clearance of the probe was observed, most probably due to high levels of shed extracellular domain of HER2 in the plasma (Fig. 1). 35 Aforementioned data indicate that tumor imaging with a low dose of fast kinetic mAb fragment will be difficult if not impossible, when there is a high level of target antigen present in well-accessible normal organs (mAb sink).

Zirconium-89–trastuzumab dose-dependent biodistributions with 10 mg trastuzumab (
In the second approach, therapeutic intact mAbs are radiolabeled with long-lived positron emitters such as 89Zr (t ½ = 78.4 hours) or 124I (t ½ = 100.3 hours) and imaged prior or during the course of mAb therapy. For the latter purpose, a small part of the therapeutic dose of intact mAb can be radiolabeled, whereas cold and radiolabeled mAb can be administered simultaneously or immediately after each other. With this approach, the relation between targeting efficiency and therapeutic response can be studied.
In future, the quantitative PET imaging of therapeutic intact mAbs can be of value at several stages of mAb development and application. Preclinical immuno-PET studies in xenograft-bearing nude mice can show the efficiency of tumor targeting with a particular mAb and the regulation of target expression, whereas immuno-PET studies in nonhuman primates can be particularly attractive to assess cross-reactivity with normal tissues in relation to toxicity. From first-in-human clinical trials with new mAbs, it is important to learn about the ideal mAb dosing for optimal tumor targeting (e.g., saturation of receptors), the uptake in critical normal organs to anticipate toxicity, and the interpatient variations in pharmacokinetics and tumor targeting. mAb imaging might provide this information in an efficient and safe way, with fewer patients treated at suboptimal dose. This approach is especially attractive when the mAb of interest is directed against a novel tumor target that has not been validated in clinical trials before. As will be illustrated in a later section, quantitative mAb imaging might also be of value to guide optimal use of FDA-approved mAbs, also when used in combination therapy.
Quality Aspects of Clinical Immuno-PET
To translate immuno-PET from preclinical investigations to a phase I clinical trial, it is necessary to create a pharmaceutical quality formulation, manufactured under current good manufacturing practice (cGMP). In most cases, the radionuclides used for radiolabeling are to be considered as active pharmaceutical ingredients (APIs), especially when the final preparation is released for use without further purification. Also, chelates used for binding of radionuclides are to be considered as APIs. Quality aspects that must be documented for radionuclides are identification (e.g., half-life and gamma emission spectrum), (radio)chemical purity, stability data, storage conditions, expiry, batch identification, and impurity profile. During the last years, procedures have been developed for the production of large batches of highly pure 89Zr and 124I in a cGMP compliant way, and both positron emitters are nowadays commercially available. 36 –38
89Zr is coupled via a chelate to the lysine residues of an mAb, whereas 124I can be coupled directly via tyrosine residues. With respect to the latter, procedures have been established for efficient coupling of no-carrier-added 124I,38 and also many preclinical proof-of-concept 124I-immuno-PET studies have been performed as described in some recent reviews. 22,23 For stable coupling of 89Zr to mAbs, a multistep procedure has been developed by Verel et al. 36 using a succinylated derivative of desferrioxamine B (N-sucDf ) as bifunctional chelate. The choice of desferrioxamine B is attractive because it is used clinically in a safe way for many years. In addition, several preclinical immuno-PET studies have been performed with 89Zr-N-sucDf-mAb conjugates as a prelude to clinical trials, for example, with cmAb U36, 36 DN30 (anti-cMet), 39 G250 (anti-carbonic anhydrase IX), 40,41 cetuximab, 30,32 ibritumomab tiuxetan, 42 rituximab, 43 bevacizumab, 44 and trastuzumab. 45
A shortcoming of the N-sucDf-based labeling procedure, however, is that it is relatively time consuming and complicated, and therefore, it is challenging with respect to cGMP compliancy. Recently, the newly developed p-isothiocyanatobenzyl derivative of desferrioxamine B (Df-Bz-NCS) was introduced, which provides an efficient and rapid preparation of 89Zr-mAbs. 46,47 Biodistribution and imaging experiments showed high, selective, and similar accumulation of 89Zr-Df-Bz-NCS-conjugates and 89Zr-N-sucDf-conjugates in tumor-bearing mice (Fig. 2). These results were confirmed by the Genentech, Inc. group, who also developed new desferrioxamine B derivatives for site-specific coupling of 89Zr to engineered thiol groups of so-called thio-antibodies. 48,49
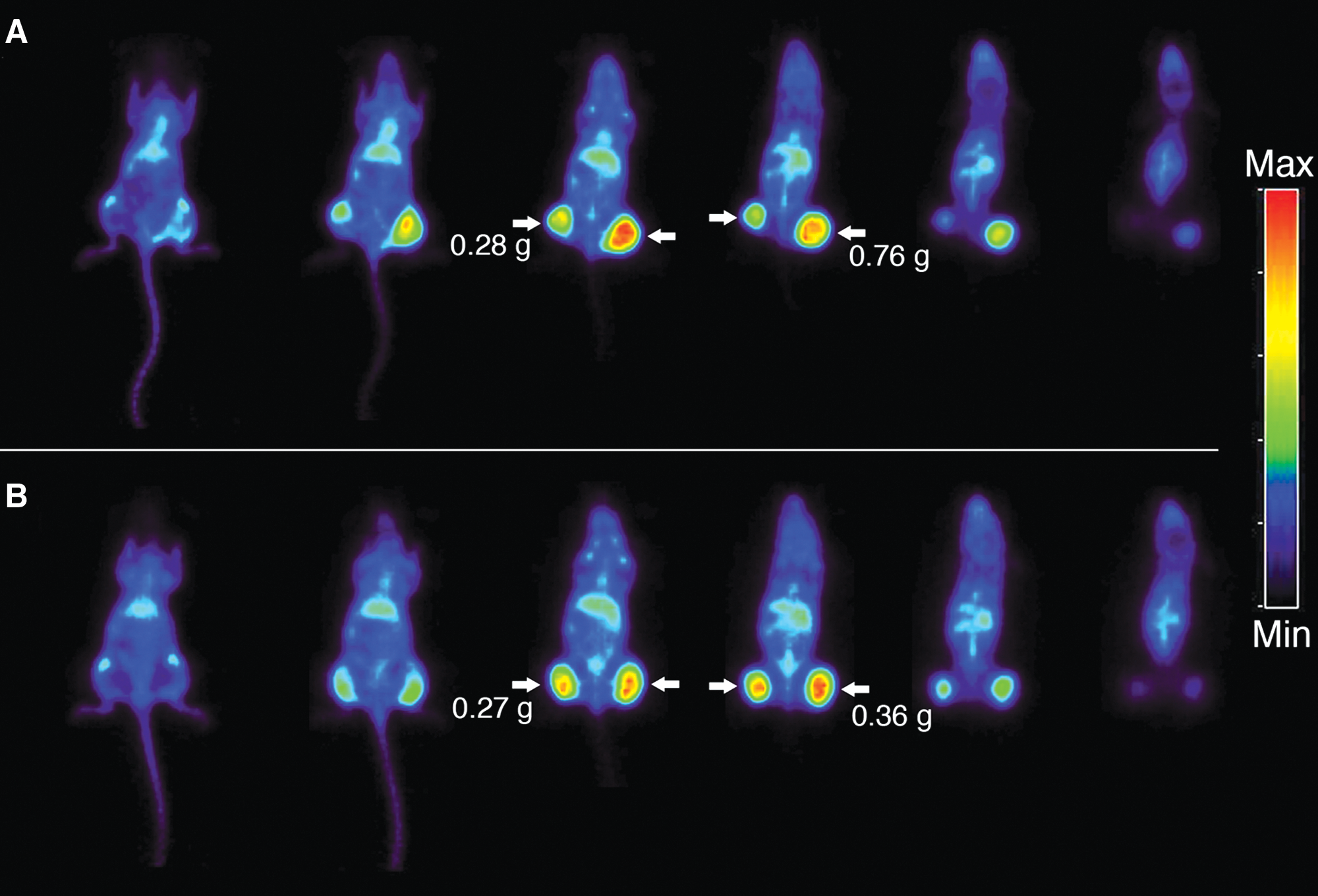
Positron emission tomography images (coronal slices) of 2 different FaDu xenograft-bearing nude mice at 72 hours after injection with 89Zr-Df-Bz-NCS-cmAb U36 (
The aforementioned achievements indicate that all reagents and procedures are in place to allow broad-scale clinical application of immuno-PET with 89Zr- and 124I-labeled intact mAbs. Although 89Zr is particularly suitable for PET imaging of internalizing mAbs, 124I is the radionuclide of choice in combination with noninternalizing mAbs. In contrast to directly labeled 124I, 89Zr is trapped inside the cell after internalization of the mAb (residualization). 30,50 Residualization also occurs to some extent in organs of mAb catabolism, such as liver, kidney, and spleen.
Quality analyses to be performed after radiolabeling include tests to assess the chelate-to-mAb substitution ratio, radiochemical purity, mAb integrity and immunoreactivity, and apyrogenicity. When labeled according to aforementioned procedures, 124I-mAbs can also be used as PET surrogates for scouting the biodistribution of therapeutic 131I-mAb conjugates, whereas 89Zr-mAbs can be used for scouting therapeutic 90Y- and 177Lu-mAb conjugates. 30,38,42,50 –52
Potential of 89Zr-Trastuzumab PET: An Example
In current practice, pathological analyses are often performed to confirm target expression and to select patients for mAb therapy. For example, patients with metastatic breast cancer are only eligible for therapy with the anti-HER2 mAb trastuzumab, when protein overexpression and gene amplification have been confirmed on a biopsy of the tumor by immunohistochemistry or fluorescence in situ hybridization (in 20%–30% of patients). It is questionable, however, whether a representative overview of in vivo HER2 expression status can be obtained by analysis of just a single biopsy. It is possible that HER2 expression in primary tumor and metastatic lesions is not the same, or it does not remain stable during the course of the disease, for example, upon chemotherapy and/or hormonal therapy. 53 –56
Taking multiple or repeated biopsies is not a solution, especially because lesions are often heterogeneous (resulting in nonrepresentative biopsies) and difficultly accessible. It is of note that HER2 has also a functional role in normal tissues such as the heart. This is probably the explanation for the cardiotoxicity induced by trastuzumab, especially when combined with anthracyclines. Interestingly, shortly after completion of anthracycline treatment, myocardial HER2 overexpression has been demonstrated in 50% of the patients. 57 Therefore, it seems worthwhile to evaluate the value of trastuzumab imaging for prediction of cardiotoxicity, especially when next-generation anti-HER2 therapeutics such as trastuzumab-DM1 (trastuzumab coupled to the supertoxic drug mertansine) are considered for therapy. 57 –59 Cross-reactivity of such supertoxic conjugates with normal tissues might result in unacceptable toxicity, as was recently demonstrated for the anti-CD44v6 conjugate bivatuzumab-DM1. 60
Antibody imaging might have added value for patient selection, because it can be used to assess target expression and mAb accumulation in all tumor lesions and normal tissues, noninvasively, quantitatively, and even over time (4-dimensional). This information might be particularly relevant when mAb therapy is combined with other treatment modalities, such as chemo- and radiotherapy, to find routes to maximum synergism. Ideally, topographic information on tumor extension is obtained to enable assessment of homogeneity of mAb tumor accumulation.
Preclinical proof-of-concept studies have been performed using 89Zr-trastuzumab as the PET imaging probe. 89Zr-trastuzumab immuno-PET appeared capable for observation of HER2-positive xenografts, primary tumors, as well as small metastatic lesions, but HER2-negative lesions present in the same animals were not detected (Fig. 3). 45 Using the same 89Zr-trastuzumab probe, downregulation of HER2 expression was observed and quantified upon treatment of tumors with HSP90 inhibitors. 61,62 As also EGFR and vascular endothelial growth factor (VEGF) expression are downregulated by these HSP90 inhibitors, similar results can be obtained by imaging with radiolabeled cetuximab or bevacizumab. 63,64 These studies showed that immuno-PET probes such as 89Zr-trastuzumab have the potential to be used to measure the efficacy of treatment with HSP90 inhibitors, and that because of the longer half-life of 89Zr, this probe is better qualified for HER2 expression imaging than the previously described 68Ga- and 64Cu-trastuzumab probes. 61,65 –67

Examples of noninvasive small-animal positron emission tomography images (dorsal presentation). Zirconium-89–trastuzumab uptake in human SKOV-3 xenografts in 3 mice at 6 hours (
Experience with Clinical Immuno-PET
124I-labeled mAbs have been used for clinical immuno-PET about 15 years ago, but the number of patients included in these studies was small. 68,69 Diagnostic results were far from optimal, among others because of the poor quality of the murine mAbs used, which were lacking the specificity of nowadays mAbs. 70 Currently, interest in 124I-labeled mAbs has been renewed, partly because of the improved methods for production of 124I and its coupling to mAbs. Two clinical applications attracted attention: Jayson et al. 71 used various doses of 124I-HuMV833, an mAb binding to VEGF121 and VEGF165, to perform PET-imaging studies in 12 patients with various progressive solid tumors. Antibody distribution and clearance were markedly heterogeneous between and within patients and between and within individual tumors. These differences may represent the variation in available targets for the mAb, which could have implications for anti-VEGF therapy. Also, similar studies have been started using 89Zr-bevacizumab as the imaging probe. 44,64
In the other clinical application, 124I-immuno-PET was used for in vivo profiling of renal cancer. Divgi et al. 72 used 124I-cmAb G250 to predict the presence of clear-cell renal carcinomas in 25 patients scheduled for surgical tumor resection. G250 is directed against carbonic anhydrase-IX and overexpressed in clear-cell renal carcinoma. It might be informative to know those renal cancer patients who have this aggressive tumor type because of treatment decisions, although opinions on this point deviate. 73 Fifteen (15) of 16 clear-cell carcinomas were identified accurately by immuno-PET, and all 9 non-clear-cell renal masses were negative for the tracer. This study illustrates how molecular imaging with specific probes can contribute to personalized medicine. Also, 89Zr-G250 conjugates are under development as alternative immuno-PET probes. 40,41
Since the introduction of 89Zr-immuno-PET technology, several clinical trials have been started, for example, using 89Zr-labeled trastuzumab, bevacizumab, cetuximab, rituximab, or ibritumumab tiuxetan as the PET probe, and a few have been reported in literature. A first-in-human 89Zr-immuno-PET trial has been conducted with 89Zr-cmAb U36, to see whether this imaging probe is safe and capable for imaging of CD44v6-positive tumors. 74,75 The aim was to determine the diagnostic value of immuno-PET with 89Zr-cmAb U36 in patients with head and neck squamous cell carcinoma (HNSCC), who were at high risk of having neck lymph node metastases. Twenty (20) HNSCC patients, scheduled to undergo resection of the primary tumor and uni- or bilateral neck dissection, underwent computed tomography (CT) and/or magnetic resonance imaging (MRI) and 89Zr-cmAb U36 immuno-PET prior to surgery. Immuno-PET detected all primary tumors (n = 17) as well as lymph node metastases in 18 of 25 positive neck levels. Missed lymph nodes were relatively small and contained just a small proportion of tumor tissue. Representative images are shown in Figure 4. It was concluded that immuno-PET with 89Zr-cmAb U36 performs at least as good for detection of HNSCC lymph node metastases (and probably distant metastases) as CT/MRI, and that use of PET-CT might further support image interpretation. In these studies also, radiation dose estimates were made, and the potential for 89Zr-cmAb U36 quantification was assessed. 76 PET quantification of blood activity in the left ventricle of the heart showed good agreement with sampled blood activity (difference equals 0.2% ± 16.9%), except for heavy-weight patients (>100 kg). A good agreement was also found for assessment of mAb uptake in primary tumors (mean deviation: −8.4% ± 34.5%), indicating the potential of 89Zr-immuno-PET for accurate noninvasive quantification of mAb biodistribution. The mean radiation doses for patients receiving 74 MBq 89Zr in this study was about 40 mSv, which is high and will limit repeated application of 89Zr-immuno-PET. However, the introduction of the new-generation PET/CT scanners will allow better-quality immuno-PET images to be obtained with a lower 89Zr activity dose. Indeed, recent PET/CT studies, in which 37 MBq of 89Zr-trastuzumab was used, showed excellent quality images at an effective dose of about 20 mSv. 35
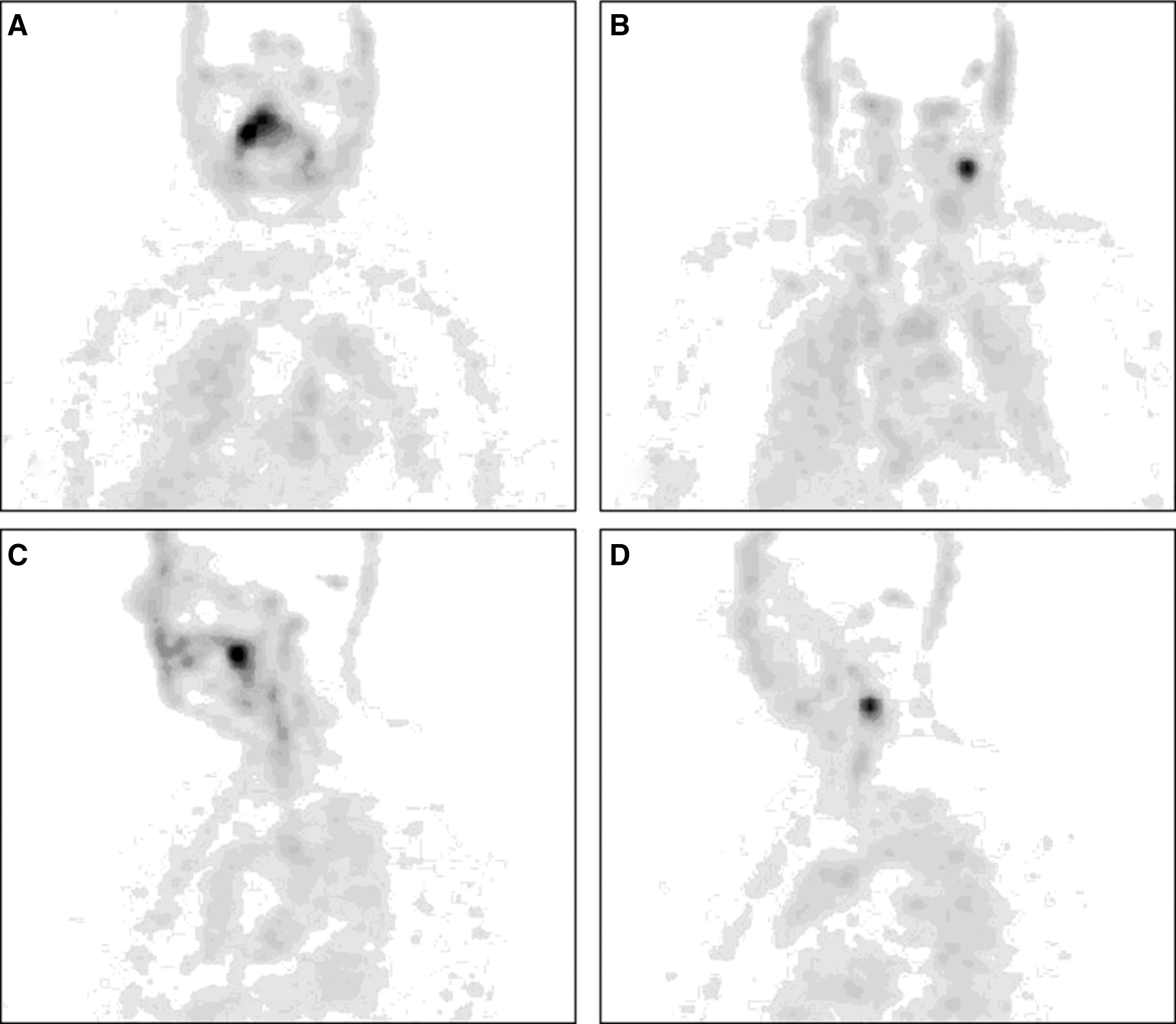
Immuno-positron emission tomography images of 89Zr-cmAb U36 uptake in a head and neck cancer patient with a tumor on the right side of the soft palate and a lymph node metastasis at the left side of the neck (level III). Images were obtained at 72 hours postinjection. (
The Groningen group determined the best conditions for PET imaging of HER2 expression with 89Zr-trastuzumab. 35 For this purpose, HER2-positive metastatic breast cancer patients received 37 MBq 89Zr-trastuzumab at 3 trastuzumab protein doses, 10 or 50 mg or 10 mg while patients were on trastuzumab treatment. Fourteen (14) patients were included. Several conclusions were drawn from these studies: at least 50 mg trastuzumab is needed to allow reliable observation of mAb uptake in HER2-positive lesions; the best moment to assess 89Zr-trastuzumab tumor uptake is 4–5 days postinjection; PET images showed a high spatial resolution and a good signal-to-noise ratio, which resulted in an image quality unapproachable by previous 111In-trastuzumab SPECT scans 77 ; excellent tumor uptake and observation of metastatic liver, lung, bone, and even brain HER2-positive lesions were obtained (Fig. 5); 89Zr-trastuzumab PET allowed quantification of conjugate uptake in HER2-positive lesions, and it became clear that for some patients with extensive tumor load, no HER2 saturation occurred during trastuzumab therapy. 78 This latter observation indicates that some breast cancer patients might be underdosed with current trastuzumab therapy regimens, and it therefore could be considered to use HER2-PET for applying a more patient-tailored trastuzumab dosing schedule.

Examples of zirconium-89–trastuzumab uptake at 5 days postinjection in a patient with liver and bone metastases (
Conclusions
mAbs are forming the most rapidly expanding category of targeted therapies; however, the efficacy of current mAbs remains quite limited, with benefit for just a portion of patients. Immuno-PET is attractive for studying the in vivo behavior of therapeutic mAbs and their interaction with critical disease targets, because it enables quantitative imaging of mAbs at high resolution and sensitivity. As most therapeutic mAbs are intact mAbs, this update focuses on the progress of immuno-PET with full-length mAbs, and the associated use of the long-lived positron emitters 89Zr and 124I. Crucial achievements have been obtained to allow broad-scale clinical application of 89Zr- and 124I-immuno-PET in clinical mAb development and applications. 89Zr and 124I became commercially available worldwide for clinical use. A chelate for facile coupling of 89Zr to mAbs became commercially available, and also protocols for labeling mAbs with 89Zr and 124I in a cGMP compliant way have been established. In addition, preclinical and clinical proof-of-concept studies have been performed showing the safety, the superior image quality, as well as the potential for accurate quantification of immuno-PET. Review of the literature on the first clinical trials shows that 89Zr- and 124I-immuno-PET might form an attractive tool to allow better understanding of mAb therapy efficacy, more efficient mAb development, and more patient-tailored therapy.
Footnotes
Acknowledgments
Funding support was provided by the Dutch Technology Foundation (STW, grants VBC.6120 and 10074); CTMM, the Center for Translational Molecular Medicine (
Disclosure Statement
No competing financial interests exist.
About the Authors