
Abstract
Twenty-nine (29) patients with recurrent head and neck carcinomas underwent 125I seed permanent implantation under ultrasonography guidance and the feasibility and efficacy of 125I seed implantation were assessed. The postplan evaluation showed that the actuarial D90 of 125I seeds ranged from 90 to 160 Gy (median, 130 Gy). The activity of each 125I seed ranged from 0.35 to 0.8 mCi (median, 0.6 mCi). The total number of sources implanted ranged from 3 to 61 (median, 22). The follow-up ranged from 3 to 40 months (median, 8 months). The 1-, 2-, and 3-year local control rates were 53.1%, 34.8%, and 17.4%, respectively, with a median local control of 16 months (95% confidence interval, 5.8–26.1). The 1-, 2-, and 3- year survival rates were 54.1%, 27.5%, and 27.5%, respectively (median, 13 months; 95% confidence interval, 6.0–19.9). Of the 25 patients, 5 (17.2%) died of local recurrence and 7 (24.1%) died of metastases; 2 patients showed recurrences at 3 and 8 months after seed implantation and subsequently died of pneumonia. One (1) patient died of heart disease. One (1) developed ulceration with tumor progression. Blood vessel damage and neuropathy were not observed. Percutaneous ultrasound-guided 125I seed implantation is a feasible, safe salvage for patients with recurrent carcinomas of the head and neck.
Introduction
It is difficult to manage local recurrences of the head and neck cancers with resurgery and external beam radiotherapy (EBRT). 1 –4 Salvage surgery is associated with a high rate of morbidity and mortality. Clinical outcome for recurrent head and neck carcinomas remains poor, with the major causes being local and regional failure. 5 –8
Intraoperative high-dose-rate (HDR) brachytherapy was used for the treatment of recurrent solid carcinomas. However, the use of this isotope has several disadvantages: (1) personnel are significantly exposed to radiation, (2) the shielding requirements are high, (3) limited dosimetry; it is necessary to administer the isotope in combination with surgery. 9
Interstitial permanent implantation of radioactive seeds into the tumor has the following major advantages: (1) high dose to the tumor target; (2) continuous radiation increases the probability of damaging malignant cells during a sensitivity phase of the cell cycle. 10 –14 The application of ultrasound-guided interstitial brachytherapy technique for prostate carcinoma treatment was first reported by Holm in 1983. 15 In 1988, Ragde et al. brought the method to the United States and it became a standard treatment option for low-risk prostate cancer. 16
This study investigates the efficacy and feasibility of 125I seed implantation under ultrasonography guidance for recurrent head and neck carcinomas and analyzes the local control rates, survival rates, and complications.
Materials and Methods
Patient information and selection
A retrospective analysis of 29 patients (median age, 56 years; range, 26–94 years) with recurrent head and neck carcinomas who underwent 125I seed implantation guided by ultrasonography (Color Doppler Ultrasound with probe and guiding stabilization devices, Aloka 550-5000) at the Peking University Third Hospital between June 2002 and November 2009 was performed.
The eligibility criteria were as follows: histologically proven recurrent head and neck carcinomas after surgery combined with EBRT or EBRT alone with no evidence of distant metastasis, Karnofski performance status of 60 or higher, and no major dysfunction of the kidney, liver, or bone marrow. Patient characteristics are shown in Table 1. All the patients had ever received EBRT, with total does from 20 to 150 Gy (median, 70 Gy). Eight (8) patients had received chemotherapy one to six cycles (median, 4). All the patients were considered unsuitable for salvage surgery, and the others refused to undergo EBRT or surgery.
Treatment planning before seed implantation
At 1–2 weeks before seed implantation, the tumor volumes were measured using computed tomography (CT) scans at 5 mm intervals. The clinical target volume included the gross tumor volume (GTV) and an extended margin of 0.5 cm. These tracings were digitized onto a computer treatment planning system (TPS) (3D treatment planning system; Beijing Fei Tian Industries, Inc.) and used to calculate the D90 (the doses delivered to 90% of the target volume defined by CT using dose–volume histograms) of irradiation. The preplan of seed implantation showed that D90 was 120–160 Gy (median, 144 Gy), The total number of seeds implanted ranged from 5 to 96 (median, 23).
Seed implantation technique
Under adequate local anesthesia, interstitial needles (18-gauge) attached to ultrasound probe stabilization devices were inserted into the tumor according to the guidelines on ultrasonography screen; the needles extended 0.5 cm of GTV and kept each other in a parallel array of 1 cm apart. Precautions were taken to avoid puncture of large blood vessels by placing the needles at a distance of 1 cm. After all needles were inserted into the tumor, 125I seeds (Beijing Atom and High Technique Industries, Inc., Model 6711, T 1/2: 59.4 days, energy level: 27.4–31.4 keV) were implanted using a Mick applicator and kept with 1.0 cm interval in the GTV and then all the needles were removed. All the patients received perioperative prophylactic antibiotics. The median number of 125I seeds implanted was 22 (range, 3–61). The specific activity of 125I seeds ranged from 0.35 to 0.80 mCi per seed (median, 0.60 mCi). The total amount of isotopes implanted ranged from 1.75 to 37.05 mCi.
Postimplant dosimetry evaluation
Postoperative dosimetry was routinely performed for all patients immediately or after 24 hours using a three-dimensional seed identification technique and 5-mm-thick CT scans. The contoured images and sources were entered into TPS software (Prowness–3D; SSGI). Isodose curves for each slice (Fig. 1) and dose–volume histograms of the target (Fig. 2) were generated. The postplan evaluation showed that the actuarial D90 was 90–160 Gy (median, 130 Gy).

The isodose curve distribution after seed implantation from computed tomography scan. The inner red curve represents GTV; curves are isodose lines of 160, 140, 120, and 90 Gy from inside, respectively. GTV, gross tumor volume.

The dose–volume histograms of GTV and spinal cord after seed implantation. DVH, dose volume histogram; DLV, dose limited volume; D–X, dose–D100, D90, D80; V–X, volume–V150, V100, V90; Cord, spinal cord.
Follow-up
Tumor response was evaluated at 4 weeks for the first time and thereafter every 2–3 months for the first 2 years and then every 6 months thereafter. The follow-up time was measured from the date of seed implantation. The median follow-up period was 8 months (range, 3–40 months). Complications were scored using the Radiation Therapy Oncology Group/European Organization for Research and Treatment of Cancer Late Radiation Morbidity Score. 17
Statistical analysis
Tumor responses were documented according to the World Health Organization criteria. 18 Overall survival curves and local control were generated using the Kaplan–Meier method and the Statistical Package for Social Sciences (SPSS) 10.0 software.
Results
Local control
The 1-, 2-, and 3-year local control rates were 53.1%, 34.8%, and 17.4%, respectively, with a median local control of 16 months (95% confidence interval, 5.9–26.1). Five (5) (17.2%) died of local recurrence. One (1) developed ulceration with tumor progression. Two (2) patients relapsed at 3 and 8 months after seed implantation, respectively, and subsequently died of pneumonia. One (1) showed partial response and died of cardiovascular event at 3 months after seed implantation (Fig. 3).
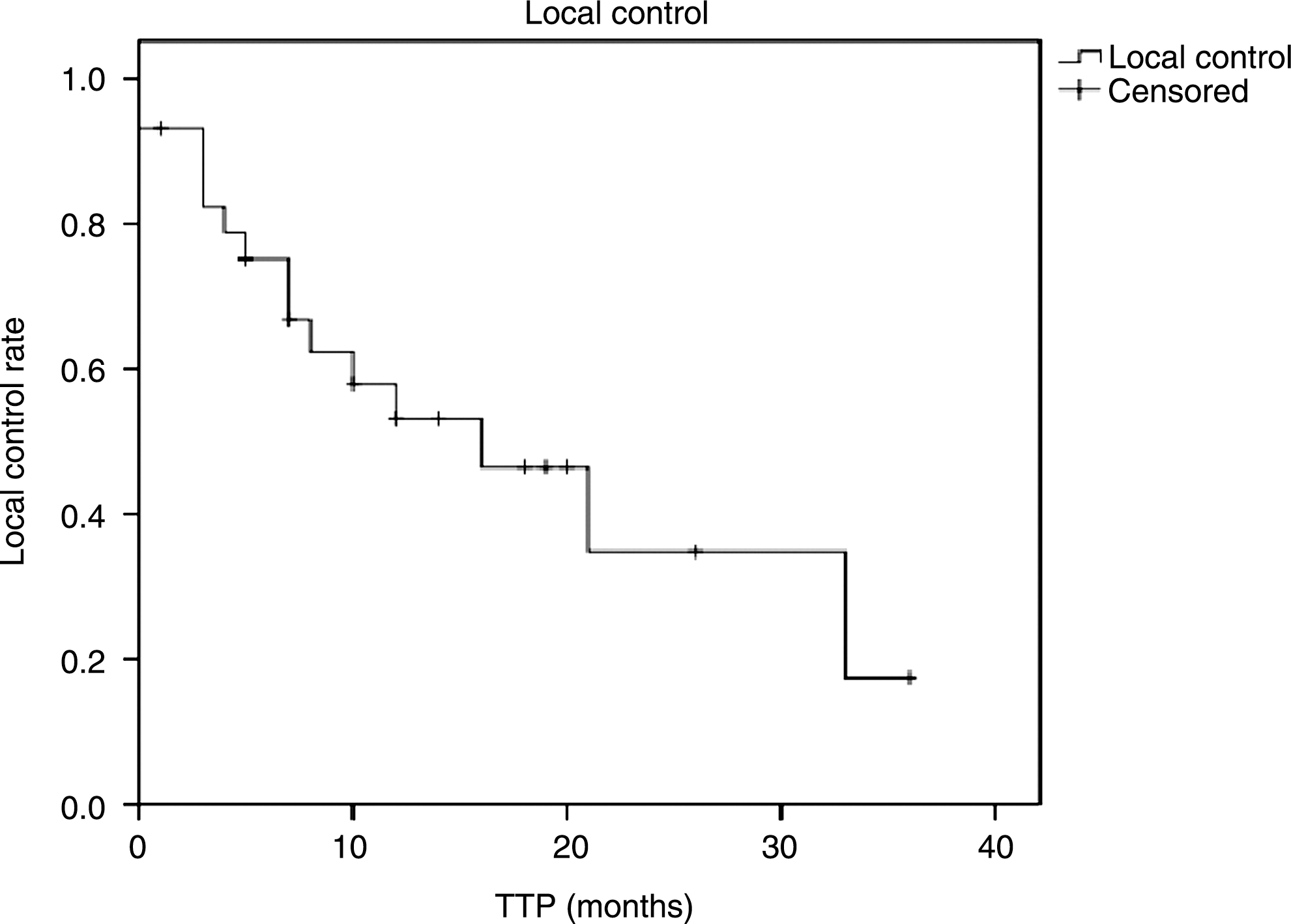
Kaplan–Meier estimates showing local control for 29 patients after 125I seed implantation. TTP, time to progression.
Survival
The 1-, 2-, and 3-year actuarial overall survival rates were 54.1%, 27.5%, and 27.5%, respectively, with a median survival of 13 months (95% confidence interval, 6.0–16.9). Seven (7) (24.1%) died of distant metastases and 14 patients are still surviving (Fig. 4).

Kaplan–Meier estimates showing overall survival for 29 patients after 125I seed implantation.
Complications
None of the patients showed bone or soft tissue necrosis and carotid rupture.
Discussion
The present modality for local recurrent head and neck carcinomas is salvage surgery or surgery combined with intraoperative HDR brachytherapy. Salvage surgery offers technical feasibility, but the curative potential is low; in such cases, local failure is at least 40% or more. 6 Surgery combined with intraoperative HDR brachytherapy has been used for recurrent head and neck carcinomas, with a local control rate and 5-year survival rate of 40%–60% and 14%, respectively. 19 –23 Pulsed-dose-rate brachytherapy can offer an alternative option for reirradiation. 24 Unfortunately, the size and location of most recurrences do not allow the optimal use of intraoperative HDR barchytherapy.
Radium-226 and iridium-192 HDR brachytherapy have been used for T1 and T2 patients with oral cavity and oropharynx carcinomas; the local tumor control was very high and good function was obtained. 25 –28 Vikram et al. treated 124 patients with advanced recurrent head and neck cancers using 125I seed implants. The completed regression was 71% and the rate of serious complications was 5.5%. 29 Goffinet et al. reported 125I seed implantation as a surgical adjuvant for advanced recurrent head and neck cancers; local control rate was 70%. 30 Park et al. analyzed 35 patients with advanced recurrent squamous cell cancers of the head and neck treated with surgery followed by 125I seed implantation. The 5-year disease-free survival was 41%. 31 Ashamalla et al. reported 94 patients treated with gold grain implants; complete local control was 33%. 32
Although concomitant intraoperative HDR brachytherapy has been demonstrated to enhance actuarial survival and local tumor control, the complication has been reported to vary from 11% to 56%. 30 –32 Martinez et al. have reported a complication rate of 11%. 33 Goffinet et al. reported that approximately half of their patients developed complications. The main complications of HDR brachytherapy are skin ulceration and wound breakdown. Occasionally, patients show carotid rupture. 30 Krempien et al. reported the feasibility of image-guided interstitial implantation with locally recurrent head and neck cancers. The 1- and 2-year local control rates were 78% and 57%, respectively, and the actuarial 1- and 2-year survival rates were 83% and 64%, respectively. 34
The present study attempted to improve the local control and sequelae of seed implantation by using ultrasound guidance. Ultrasound guidance allows virtual planning and navigated implantation of needles, thus optimizing needle distribution and keeping them at a safe distance from the organ at risk. The 1-, 2-, and 3-year local tumor control rates were 53.1%, 34.8%, and 17.4%, respectively. The 1-, 2-, and 3-year survival rates were 54.1%, 27.5%, and 27.5%, respectively, with a median survival of 13 months. Five (5) (17.2%) died of local recurrence and 7 (24.1%) died of metastases. In the present study, none of the patients showed bone or soft tissue necrosis and carotid rupture.
Conclusions
Percutaneous ultrasonography-guided interstitial implantation of 125I seeds is a feasible and promising salvage modality for patients with recurrent head and neck carcinomas. The present study included limited number of patients and had a short follow-up time; therefore, it is necessary to perform further studies with a large number of patients, and a long-term result of this procedure is still under investigation.
Footnotes
Acknowledgments
The authors thank Dr. Wei-Juan Jiang for manuscript assistance and Dr. Jin-Na Li and Su-Qing Tian for their help in figure preparation. This study was supported by the Foundation of Capital Medical Development and Research (Item No. 2009–2024).
Disclosure Statement
The authors declare that they have no conflict of interest.