
Abstract
Purpose:
This study evaluated the tolerance and therapeutic efficacy of rhenium-188 hydroxyethylidene diphosphonate (188Re-HEDP) in patients with different types of advanced cancer suffering from bone pain caused by osseous metastases.
Methods:
Sixty-four patients received a single injection of escalating doses of 188Re-HEDP with various dosages. Vital signs were observed before and after treatment for 8 weeks; adverse effects and rebound pain were recorded within 8 weeks after injection. Blood counts, biochemical parameters, and electrocardiogram were also measured over a period of 8 weeks. Clinical follow-up studies including the bone pain score and the Karnofsky performance score were performed. Pain response was scored by a four-point pain-rating scale as complete, marked, mild, and no response.
Results:
No adverse effects or clinically significant changes in vital signs, electrocardiograms, and biochemical parameters in patients were observed, and there was no statistical change in alkaline phosphate levels in patients before or after treatment. The overall nadir of thrombopenia was at week 4, leucopoenia at week 3, and anemia at week 8. At week 8, the mean level of platelets and leukocytes returned to baseline levels. The pain score descended from 8.11 to 7.74 on the day of therapy, with a nadir of 4.89 at week 4, and up to 6.67 at week 8 after therapy (p < 0.05). The Karnofsky performance score continually increased from 74.81 before therapy to 82.31 at 8 weeks (p < 0.05). Pain palliation was reported by 73.33% of patients, with a mean duration of 6.85 weeks and a mean start time of 4.05 days. Of the specific tumor types, pain relief was achieved in 84.62% of patients with prostate cancer, 78.57% with breast cancer, 62.50% with lung cancer, and 55.56% with liver cancer.
Conclusions:
188Re-HEDP is a useful radiopharmaceutical agent for improving bone pain in patients with advanced cancer with painful bone metastases.
Introduction
A variety of bone-seeking radiopharmaceuticals, such as phosphorus-32 (P-32), strontium-89 (Sr-89), samarium-153 ethylene diamine tetramethylene phosphonic acid, and rhenium-186 hydroxyethylidene diphosphonate (186Re-HEDP), have been developed for systemic therapy of patients with widespread osseous metastases. Rhenium-188-HEDP (188Re-HEDP) is a new radiopharmaceutical with several major advantages; it is inexpensively available on demand from a W-188/rhenium-188 generator, and a kit is available for easy radiolabeling of the bone-seeking HEDP. 1,2 The most important physical characteristics of 188Re are emission of high-energy beta particles, with a maximal energy of 2.12 MeV, and its relatively short physical half-life of 16.9 hours. Thus, some investigators 3,4 consider 188Re to have potential antitumoral effects, and radioprotection can be more easily achieved for 188Re than for other radionuclides used for therapy, such as 131I.
A few studies of pain palliation of 188Re-HEDP in patients with prostate cancer with osseous metastases who were suffering from bone pain have been reported, and they showed that application of 188Re-HEDP in humans is safe and that pain palliation can be achieved in approximately 70% of patients. 5,6
This clinical trial was designed to evaluate the tolerance for and effectiveness of 188Re-HEDP for the palliation of painful bone metastases in Chinese patients with different types of advanced cancer.
Materials and Methods
Patient criteria
The criteria for admission of patients to the study were painful bone metastases in cancers that had been histologically proved and that were without visceral metastases (confirmed by X-ray and computed tomography); failure of previous conventional therapy; multiple metastases in bone scanning with 99mTc-MDP showing increased uptake; white cell and platelet numbers higher than 3500/mm3 (3.5 × 109/L) and 80,000/mm3 (80 × 109/L), respectively; serum creatinine (Scr) and alanine aminotransferase (ALT) concentrations ≤115 μmol/L (normal range: 44–115 μmol/L) and 75 U/L (normal range: 0–75.0 U/L), respectively; life expectancy >8 week; a minimum 8-week interval from discontinuation of chemotherapy; and external radiotherapy and bisphosphonate.
On the other hand, exclusion criteria were obstructive renal pathology or renal insufficiency, urinary incontinence, psychiatric pathology, evidence of spinal marrow compression, pathological fracture, infiltration of a nerve plexus of peripheral nerves combined with severe heart and cerebral vessels disease, and serious illness and organ dysfunction not related to primary cancer.
In accordance with the Helsinki Declaration, all patients were comprehensively informed about the experimental character of the study and the possible side-effects, and all patients gave written informed consent. Approval was obtained from the local ethics committee.
Patient information
No patients treated with hormone therapy were included in this study. Sixty-four patients with pain associated with bone metastases were included in the study. Four patients were removed from the study, 2 for failure to follow-up and 2 for failure to comply with the protocol (they received antitumoral drugs within 8 weeks after injection of 188Re-HEDP). Sixty patients (men, 38; women, 22; mean age, 58 ± 10 years; range, 36–70 years) belonged to Per-Protocol population. The primary histologically proved malignancy was prostate cancer in 26 patients, breast cancer in 14 patients, lung cancer in 8 patients, liver cancer in 9 patients, and various other types in 3 patients (rectal cancer, oesophageal cancer, and laryngeal cancer).
Radiopharmaceutical
188Re-HEDP was provided by Shanghai Institute of Applied Physics, Chinese Academy of Sciences. It is inexpensively available on demand from a W-188/rhenium-188 generator, and a kit is available for easy radiolabeling of the bone-seeking HEDP. 188Re-HEDP was prepared by adding 1 mL of a 188ReO4 − solution (414 MBq) to a vial containing the lyophilized HEDP kit formulation just described (pH ≈ 1). The solution was heated in a water bath for 10 minutes at 100°C. Sterility and pyrogen tests were performed on each preparation. Radiochemical purity was determined by ascending chromatography with acetone and NaCl 0.9% as mobile phases and Whatman 1 M and 3 M as stationary phases, respectively. Radiochemical purity is ≥95%.
Treatment protocol
Groups of at least 10 patients were treated with escalating doses of 188Re-HEDP, starting with 20 MBq/kg and escalating up to 50 MBq/kg. If no toxicity was observed after the treatment of patients, the next higher dose was given. The toxicity was confirmed by at least 2 patients with the same results. The dose escalation was terminated if any patients demonstrated unacceptable toxicity, which was defined as hematological toxicity (World Health Organization [WHO] grading) grade 3 or 4. In this case, the previous group was considered to have received the maximum tolerated dose. For the assessment of toxicity, the toxicity criteria of the WHO were used. 7 According to this toxicity scale, thrombocyte counts of 76–99 × 109/L, 50–74 × 109/L, 25–49 × 109/L, and below 25 × 109/L, leukocyte counts of 3.0–3.9 × 109/L, 2.0–2.9 × 109/L, 1.0–1.9 × 109/L, and below 1.0 × 109/L, and hemoglobin concentrations of 95–100, 80–94, 65–79, and below 65 g/L correspond to toxicity grades 1, 2, 3, and 4, respectively. The maximum decrease was calculated by comparison of the pre-treatment level of thrombocytes, leukocytes, and hemoglobin (baseline) with the lowest level during the follow-up period.
Except for 4 patients who were removed from the study, 14 patients received 20 MBq/kg188Re-HEDP; 15 received 30 MBq/kg; 15 received 40 MBq/kg; and 16 received 50 MBq/kg.
188Re-HEDP was administered as a bolus injection via a running intravenous saline drip. After the injection, patients were hospitalized for 72 hours in the nuclear medicine ward. Vital signs (heart rate, blood pressure, breath, and temperature), any adverse effects, and rebound pain were recorded.
Blood samples were drawn before and weekly after treatment for the determination of blood counts and clinical chemistry parameters (over a period of 8 weeks). For analysis of hematological toxicity, the thrombocyte and leukocyte counts and hemoglobin concentration were examined during the week before therapy and 1, 2, 3, 4, 6, and 8 weeks after therapy, as shown in Table 1. To analyze liver and renal toxicities, Scr, blood urea nitrogen, and liver enzymes (ALT) were determined during the week before therapy and within 1, 4, and 8 weeks after therapy (Table 1). The level of ALP, which was regarded as an index of bone resorption, was also measured, and electrocardiograms were performed to access cardiac toxicity (Table 1).
B.i., before injection; P.i., postinjection; HR, heart rate; BP, blood pressure; BT, body temperature; Br, breath; AE, adverse effect; EKG, electrocardiogram; BC, blood counts; ALT, alanine aminotransferase; BUN, blood urea nitrogen; ALP or AKP, alkaline phosphates; Scr, serum creatinine; PS, score of bone pain; KPS, Karnofsky performance score.
Pain evaluation
The patients had to complete a pain diary that included information on Karnofsky score during the baseline period and throughout the study. The week before the injection of 188Re-HEDP was considered as the baseline period. During this time, no new analgesics were administered. The pain measurement tool of the Visual Analogue Scale served as a basis for pain documentation. On the scale, zero represents no pain, and 10 represents intolerable pain. 8 Visual Analogue Scale is an approach commonly used to measure pain intensity and is well validated in the cancer population. 9
The time at which the scores of bone pain and Karnofsky performance were evaluated is shown in Table 1.
For the assessment of pain palliation, patients had to document the pain and describe the situation in their pain diaries. Pain response was scored by a four-point pain-rating scale as complete, marked, mild, and no response.
Statistical test
Regression analysis was performed to calculate the relationship between the decrease in thrombocyte and leukocyte counts with the administered activity (p < 0.05 was considered statistically significant). For statistical testing of the average thrombocyte and leukocyte counts and hemoglobin levels, a Student's t-test for dependent variables was used, comparing each week after therapy with the baseline value (again p < 0.05 was taken statistically significant). The changes in pain score and Karnofsky performance score were also tested by Student's t-test.
Results
Clinical results
Within the follow-up period of 8 weeks, no death and serious side-effects occurred in any patients. At 6 hours after receiving the injection, 1 patient who received a dose of 20 MBq/kg reported “nausea, vomiting, and hidrosis” that lasted 24 hours and resolved without medical intervention.
No clinically significant change in vital signs (heart rate, blood pressure, breath, and temperature) was observed.
Five patients reported a “bone flare” phenomenon.
Hematotoxicity
In the 20 MBq/kg group, 1 patient showed reversible leucopoenia of grade 1 toxicity after treatment. The nadir of leucopoenia (3.2 × 109/L) was at week 4. No significant hematopoietic alterations were observed in other patients.
In the 30 MBq/kg group, 3 patients showed grade 1 reversible leucopoenia, and 1 of them had grade 3 reversible thrombopoenia (this patient had had grade 1 thrombopoenia at baseline). The nadir of leuco- and thrombopoenia was at week 3 and 4 after therapy, respectively.
In the 40 MBq/kg group, grade 1 reversible leucopoenia was found in 2 patients (1 patient had grade 1 combined reversible thrombopoenia), and grade 2 in another 2 patients (1 patient with baseline leukocytes <4 × 109/L and grade 1 combined reversible thrombopoenia). Grade 1 reversible thrombopoenia was found in 1 patient, and grade 2 in another one who had grade 1 thrombopoenia at baseline. The nadir of leuco- and thrombopoenia was at week 4.
In the 50 MBq/kg group, grade 2 reversible leucopoenia was found in 3 patients (2 patients had baseline value of leukocytes <4 × 109/L), and grade 1 in 1 patient. Grade 1 reversible thrombopoenia 1 was found in 3 patients, and grade 2 in 2 patients. The nadir of leuco- and thrombopoenia was at week 3 and 4, respectively.
A statistically significant decrease in the mean thrombocyte count of all patients was found at week 3 (Fig. 1) and week 4, with the nadir during week 4. The decrease in the mean leukocyte count was less marked than that of the thrombocyte count, but a statistically significant decrease was also noted at weeks 2, 3, 4, and 6 (Fig. 2), with the nadir during week 3. At week 8, the mean thrombocyte and leukocyte counts returned to baseline levels again. The continued decrease in hemoglobin concentration was found, and the nadir was at week 8 (Fig. 3).
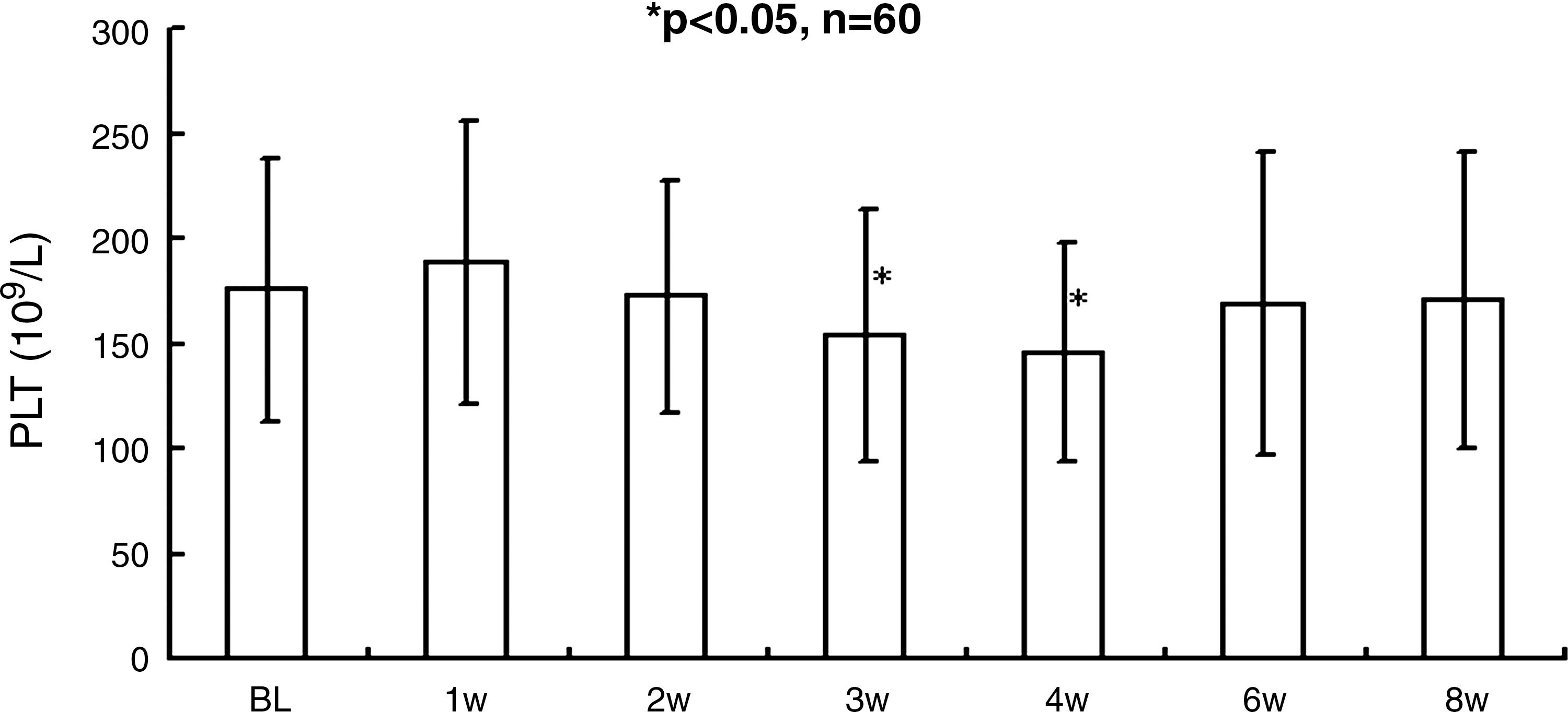
Mean thrombocyte count with standard deviation after injection of rhenium-188 hydroxyethylidene diphosphonate (188Re-HEDP).

Mean leukocyte count with standard deviation after injection of 188Re-HEDP.
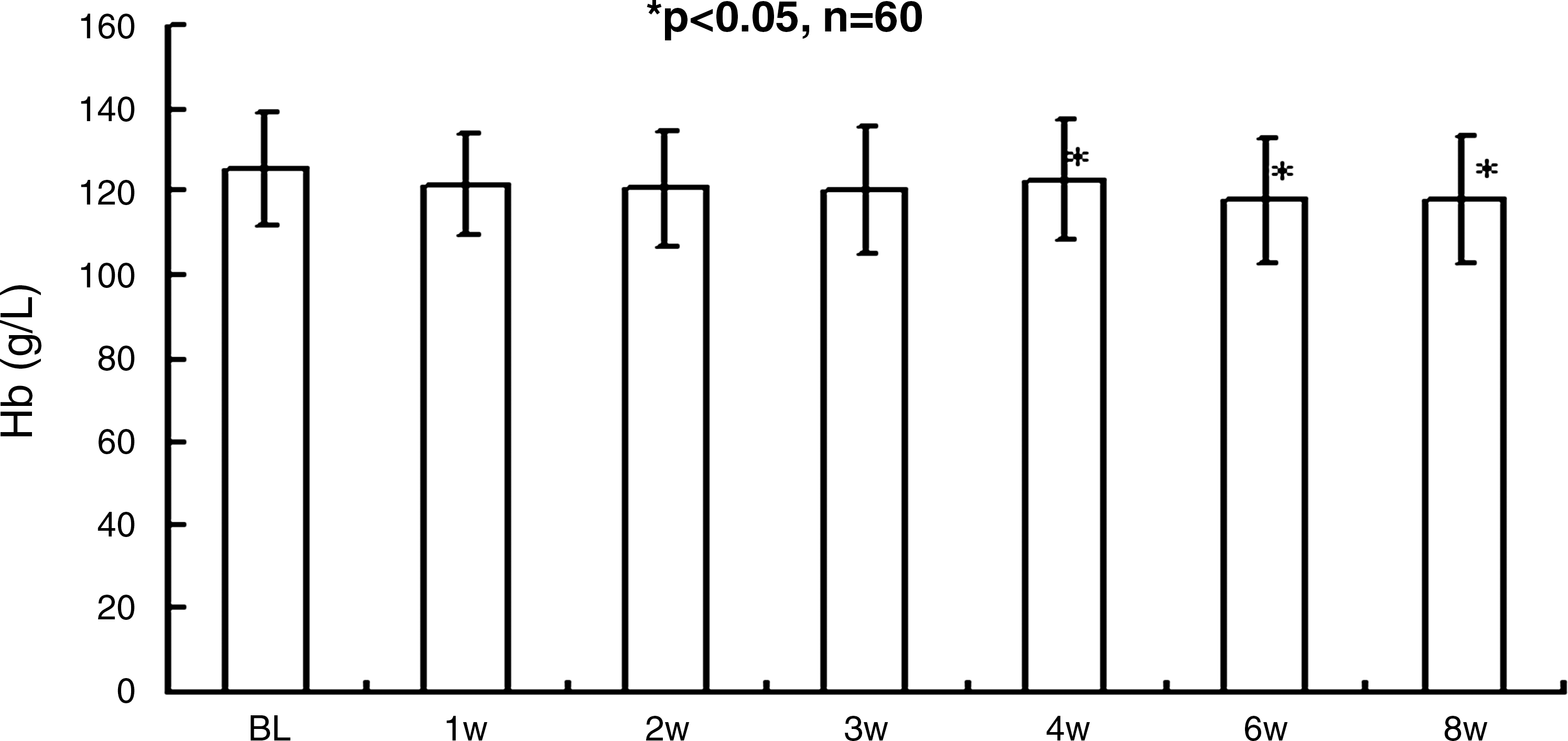
Mean hemoglobin concentration with standard deviation after injection of 188Re-HEDP.
There was a correlation between dose escalation and the reduction in thrombocyte and leukocyte counts, but there was no statistical significance between them.
Among 16 patients with baseline thrombocyte counts below 200 × 109/L, thrombopoenia was observed in 7 (43.75%); by contrast, only 4 of 44 patients with higher thrombocyte counts (>200 × 109/L) showed thrombopoenia (9.09%), assessed by reference to WHO criteria (Table 2). Of 6 patients with baseline leukocyte counts below 4 × 109/L, 3 patients (50%) had grade 2 leucopoenia, whereas 2 patients of 54 patients with baseline leukocyte counts ≥4 × 109/L had grade 2 leucopoenia (3.70%) (Table 2). Nine of 11 patients with hemoglobin ≤120 g/L (81.81%) were anemic after therapy, but only 2 of 49 patients with hemoglobin >120 g/L (12.50%) were anemic (Table 2).
Plasma ALT concentrations are a marker of liver injury. Of 60 patients, only 1 patient showed a clinically significant elevation in ALT, from a baseline value of 19 U/L to a value of 119 U/L at week 8.
Plasma Scr and blood urea nitrogen concentrations, which reflect renal function, were within the normal range before and after treatment in all patients.
There was a rise in ALP after treatment at weeks 4 and 8, but no statistically significant change was found between pre-treatment and posttreatment time points.
Electrocardiogram results remained consistent before and after therapy in most patients. In 2 patients who received 40 MBq/kg, electrocardiograms that showed abnormal conduction before therapy documented normal results after therapy, whereas in 3 patients who received 20 MBq/kg, electrocardiograms that revealed normal patterns before therapy graphed abnormal electrocardiograms after therapy.
Pain score
A tendency of the pain score to decrease from baseline levels of 8.11 to 7.74 during day of therapy was noted, and this decrease continued to the nadir of 4.89 at week 4 after therapy. After the nadir, the pain score began rising and reached 6.67 at week 8 after therapy (p < 0.05, by the paired t-test between scores before and after therapy) (Fig. 4 and Table 3). A statistically significant increase in the Karnofsky performance score from 74.81% ± 10.51% before therapy to 78.89% ± 11.55% at 1 week was observed, and the score continued to increase up to 82.31% ± 13.94% at 8 weeks after a single injection (p < 0.05, by the paired t-test between scores before and after therapy) (Fig. 5 and Table 3).
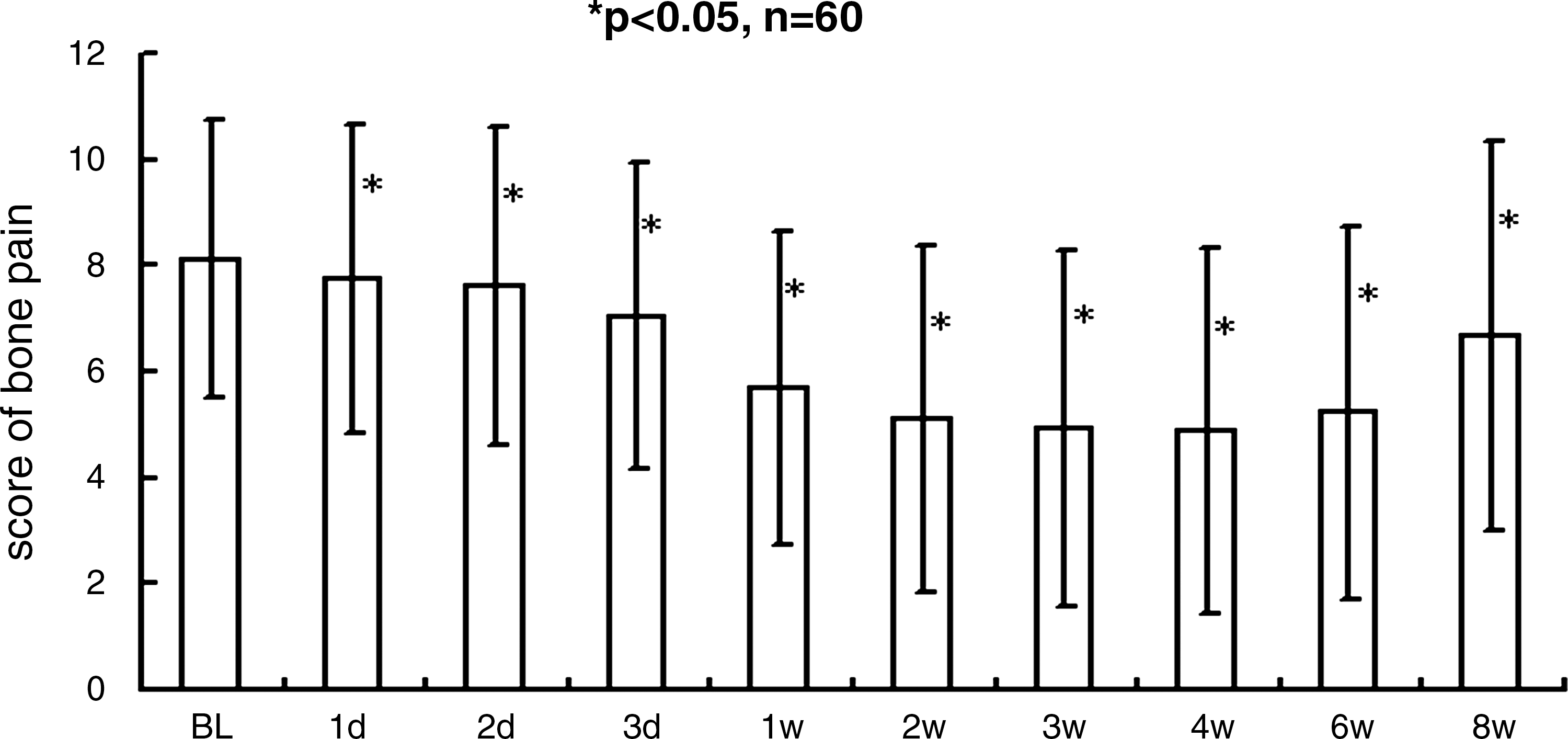
Mean score of bone pain with standard deviation after injection of 188Re-HEDP.
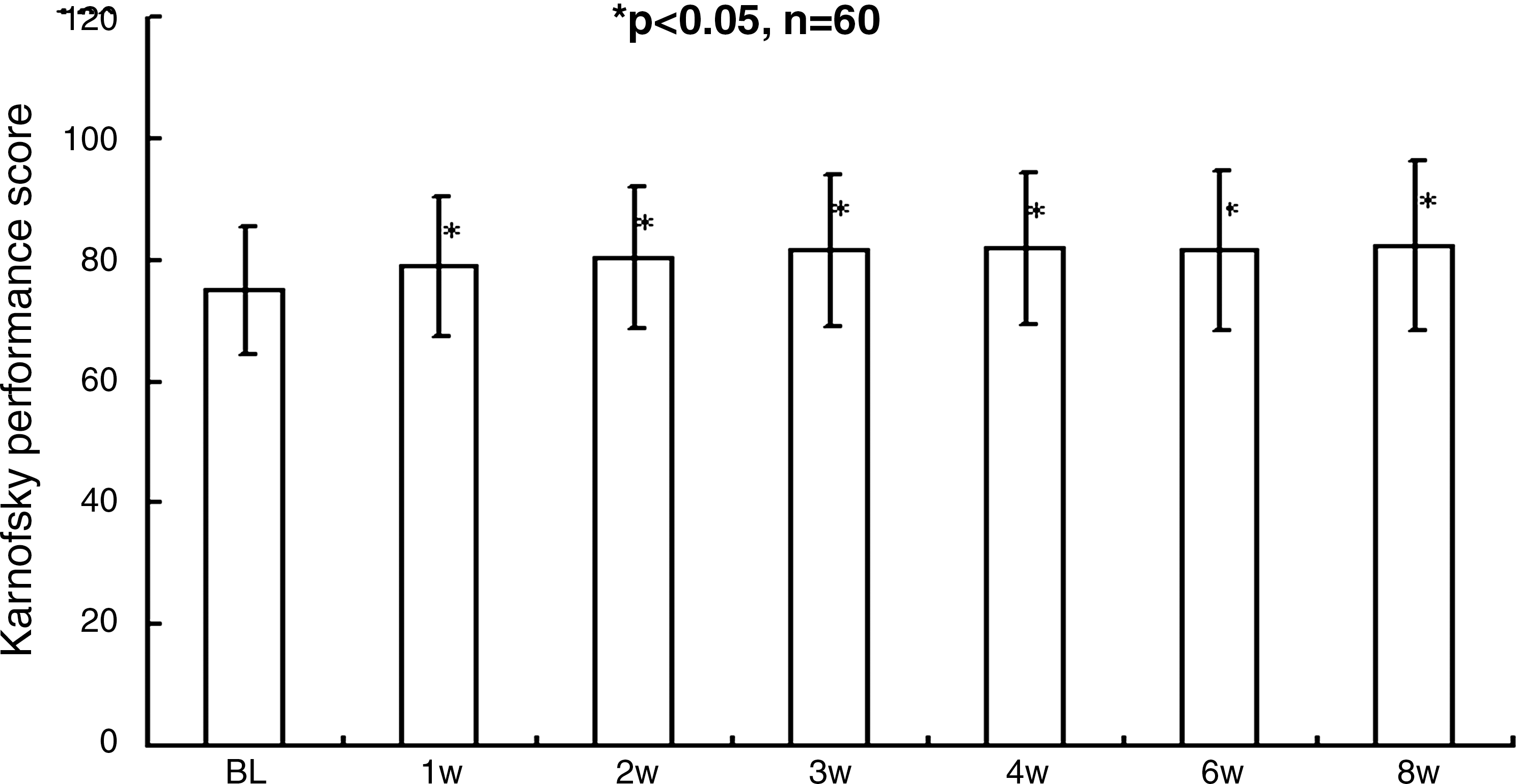
Mean Karnofsky performance score with standard deviation after injection of 188Re-HEDP.
Pain palliation
A palliative effect was obtained in 44 of the 60 patients, resulting in an overall response rate of 73.33%. The mean duration of response was 6.85 weeks, with a range of 4–8 weeks, and the mean beginning time of response was 4.05 days, with a range of 1–7 days (Tables 4 and 5). Response rates included a complete response rate of 10%, a marked response rate of 25%, and a mild response rate of 38.33%.
In the 20, 30, 40, and 50 MBq/kg groups, the response rates were 61.11%, 64.29%, 85.71%, and 85.71%, respectively (Table 5). Of the specific tumor types, pain relief was achieved in 84.62% of patients with prostate cancer, in 78.57% with breast cancer, in 62.50% with lung cancer, and in 55.56% with liver cancer (Table 6).
Discussion
Pain is among the most common and distressing symptoms encountered by patients with advanced cancer. The challenge of pain palliation is to achieve effective relief with minimal side-effects and to deliver this service to all patients in need of these interventions.
Bone pain consequent to metastatic cancer requires a multidisciplinary approach and close cross-specialty liaisons, and its alleviation is crucial to improving the patient's quality of life. 10 In the case of wide bone metastatic disease, nuclear medicine-based, bone-targeted radionuclide therapy has proved to be an efficacious and cost-effective regimen, without many of the side-effects attributable to, or the costs associated with, the other therapeutic modalities. 11,12
188Re-HEDP is a promising palliation agent labeled with 188Re for palliative therapy of bone metastases. One of the major advantages of using 188Re is its on-demand availability from an 188W/188Re generator. 2 Thus, as far as availability and convenience are concerned, it is superior to reactor-produced radionuclides, such as 32P, 89Sr, 153Sm, and 186Re, which are not readily available in certain areas. HEDP can be readily radiolabeled with 188Re (as it can with 186Re), and gamma camera imaging is possible for dosimetry estimates.
After the report of Maxon et al. 13 about the results of an initial feasibility study on the use of 188Re-HEDP in animals and humans, which showed that about 50% of the patients reported pain relief at maximum doses of 1.8 GBq, a few studies concerned with the therapeutic effects of 188Re-HEDP in patients with prostate cancer with osseous metastases, who suffer from bone pain, have been published by Palmedo et al.
In their study 5 of dose escalation of 188Re-HEDP from 1.3, 2.6, 3.3 to 4.4 GBq, 1 patient who received a dose of 4.4 GBq died 6 weeks after the injection due to acute renal failure. Out of the 8 patients in the 4.4 GBq group, three reported a short period of nausea and vomiting some days after the injection. However, a higher dose of 50 MBq/kg was not better than 40 MBq/kg in our study. The possible reason of this difference may be different tumors and patients' condition. In a study by Maxon, 2 out of 8 patients experienced mild renal toxicity with Scr concentrations greater than 133 μmol/L, which returned to normal by 8 week postinjection.
In our study with 188Re-HEDP from 20 to 50 MBq/kg, no renal toxicity was found at weeks 4 and 8 after therapy. Transit mild nausea, vomiting, and perspiration were observed in 1 patient who received 20 MBq/kg of 188Re-HEDP; an increase in ALT at week 8 was noted in one patient with liver cancer who received 30 MBq/kg of 188Re-HEDP, but this may have been a result of the primary liver cancer rather than the treatment. In 5 patients, clinically significant changes in electrocardiogram results after therapy were documented, but no regular pattern was observed in these changes. In 3 patients, electrocardiograms changed from normal to abnormal, and in another two, from normal to abnormal. It is obvious that these changes in electrocardiogram cannot be interpreted as an overall pattern of cardiac toxicity as a result of treatment with 188Re-HEDP. On the whole, there were no severe clinical side-effects that could have been directly correlated to the application of 188Re-HEDP. In particular, no neurological side-effects were observed, which have previously been reported as a rare complication of 186Re-HEDP treatment. 14 Therefore, it may be inferred from the above mentioned data that 188Re-HEDP is relatively safe to use in humans.
In this study, the number of patients who showed hematotoxicity and the degree of hematotoxicity seemed to increase with the increasing doses. There was a correlation between dose and the decrease in thrombocytes and leukocytes.
Doses of 20 MBq/kg up to 50 MBq/kg are tolerated; hematotoxicity of grade 1 to 2 may occur, but no more than 3. For patients with compromised blood counts, the dose of 50 MBq/kg is still tolerated.
Besides dose, the toxicity is certainly influenced by the baseline blood counts; this is in agreement with Palmdo et al. In our study with 44 patients with thrombocyte counts over 200 × 109/L, no grade 3 or 4 thrombopoenia was observed, thrombopoenia of grade 1 occurred in 2 patients, and grade 2 in another 2 patients. The general incidence of thrombopoenia was 9%. By contrast, in 16 patients with thrombocyte counts ≤200 × 109/L, thrombopoenia of grade 1, 2, and 3 was noted in 5, 1, and 1 patients, respectively, and the general incidence of thrombopoenia was 43.75%, nearly half the patients (Table 2). In 6 patients with leukocyte counts ≥3.5 and <4 × 109/L, that is, leucopoenia of grade 1, the incidence of leucopoenia of grade 2 achieved 50%, whereas in fifty-four patients with leukocyte counts ≥4 × 109/L, leucopoenia of grade 2 was found in 2 patients (incidence of 4%), and the general incidence of leucopoenia was 11%.
The incidence of toxicity-based on hemoglobin concentrations was 82% in 11 patients with hemoglobin concentrations ≤120 g/L and 8% in 49 patients with hemoglobin concentrations >120 g/L. However, the hemoglobin concentration may be influenced by disease progression and by the treatment.
The overall response rate in this study was 73.33%, the average period of response was 6.85 weeks, and the mean start time of response was 4.05 days. The response rate is lower than the study by Savio, 3 with an overall response rate of 78% and earlier response and longer duration in the higher dose group, and is higher than found by Palmedo, 5 with an overall response rate of 64% and an average period of response of 7.5 weeks. These response rates are also similar to those reported for the treatment of bone metastases with 186Re-HEDP 15 –17 ; however, the duration of pain relief of 188Re-HEDP (7.5 weeks in Palmedo's study and 6.85 weeks in ours) seems to be longer than that of 186Re-HEDP, which had an overall response rate of 60% and a duration of response averaging 5.5 weeks. 17 Additionally, the start time of 4.05 days in our study is markedly lower than the 12.5 days found by Palmedo. Further study is needed to investigate the reasons for these differences.
When the response rate of 188Re-HEDP is correlated to the applied dose, it seems that the dose that will achieve an optimal effective pain palliation is 40 MBq/kg. In this study, the response rate could be improved from 61% to 86% with increasing doses. Higher administered activities will induce more frequent responses.
Also, it should be noted that four types of primary cancer, each with ≥8 cases, were included in our study, and all of these cancers showed a satisfactory response rate from 56% to 85%. In painful osseous metastases from four types of patients with cancer, it was found that 188Re-HEDP was especially effective in prostate cancer (85%) and breast cancer (79%). In this study, the 63% pain relief in patients with lung cancer was comparable to that reported by Zhang et al., 18 who found a response rate of 79% for patients with lung cancer with a single dose of 1.15 GBq. In addition, so far the research of pain relief in liver cancer has not been studied. Nine patients with painful bone metastases from liver cancer were included in our study, and the treatment showed a heartening outcome, with a response rate of 56%.
Liepe and co-workers focused on the impact of 188Re-HEDP therapy on the general patient status, and a statistically significant increase in the Karnofsky performance score from 74% ± 7% before therapy to 85% ± 9% at 12 weeks after a single injection was observed. 19 These results are consistent with ours: 74.81% ± 10.51% before therapy, 78.89% ± 11.55% at 1 week, and 82.31% ± 13.94% at 8 week after a single injection. Also, a statistically significant increase in the Karnofsky performance score was found. Thus, it is obvious that 188Re-HEDP may improve the general status of the patients.
Conclusions
188Re-HEDP is a useful radiopharmaceutical agent for improving bone pain and the general status of patients with advanced cancer with painful bone metastases from various tumor types. It can be expected that 188Re-HEDP may be the optimistic choice for patients with clinical cancer with osseous metastases, for it can be easily prepared with a 188W/188Re generator and has attractive nuclear properties for radionuclide therapy of bone pain.
Footnotes
Disclosure Statement
No competing financial interests exist.