
Abstract
Center for Genetic Engineering and Biotechnology (CIGB)-M3 is a trivalent recombinant single-chain Fv antibody fragment specific for carcinoembryonic antigen (CEA). Preclinical studies with radiolabeled CIGB-M3 have showed that the antibody fragment accumulates in human colon tumor xenografts growing in nude mice. A Phase I clinical trial was carried out to determine safety, biodistribution, and pharmacokinetics of the radiolabeled CIGB-M3 in two groups of patients with CEA+ colorectal cancers. Group I (10 patients) received a single intravenous injection of 0.3 mg of 131I-CIGB-M3 (16.7–23.3 mCi/mg). Group II (7 patients) received 1 mg (5–7 mCi/mg). No adverse events related to the injected product were recorded, and no immunology response was detected up to 6 months after the injection. Tumors were detected in 15 of the 17 studied cases. The pharmacokinetic profile showed beta half-times of 14.1 and 6.3 hours for Groups I and II, respectively. Seventy-two (72) hours after the administration of the product, 85% of the total injected activity was excreted in urine in the form of free 131I. The kidneys were identified as the organs that can limit the maximum tolerated dose. The 131I-CIGB-M3 was safe in patients with colorectal cancer. The biodistribution and pharmacokinetic data suggest that the product can be further tested for molecular radiotherapy of CEA+tumors.
Introduction
Radioimmunotherapy, also denominated molecular radiotherapy, uses radiolabeled antibodies to target and selectively irradiate and destroy tumor cells. 1,2 The regulatory approval some years ago of the anti-CD-20 radiolabeled antibodies Bexxar® and Zevalin®3 –5 for the treatment of lymphoma brought forth a renewed interest in this field, but the use of radiolabeled antibodies for solid tumor therapy remains a complex research and clinical task.
The lack of success of molecular radiotherapy in solid tumors seems to be strongly associated with several factors. 6 Both the size of full antibodies and the presence of an Fc domain determine nonoptimal biodistribution and pharmacokinetic properties that make it difficult, if not impossible, to deliver sufficient radiation dose to the tumors without a concomitant toxicity for some normal organs. The chance of effective therapeutic dose delivery in bulky tumors is also limited by antibody penetration due to the size of the targeting agent. Finally, in the case of murine monoclonal antibodies (Mab), the foreign Fc contributes to immunogenicity.
Taking the aforementioned points in mind, it is foreseen that molecular radiotherapy of solid tumors will progress through a change in strategy. First, some authors sustain that the effort should be placed more in controlling minimal residual disease and metastases using this therapeutic approach. 6 Last, pretargeting procedures as well as the use of smaller antibody molecules could provide better ways for increasing tumor damage and avoidance of normal tissue adverse effects.
The development of small genetically engineered antibody fragments with faster clearance, higher tumor-to-background ratio, and low immunogenicity is one of the most promising avenues. Single-chain Fv (scFv) fragments, Fabs, scFv engineered to multivalent forms, and minibodies are at the center of the current efforts to overcome the molecular limitations of radiolabeled full antibodies. 7 –9
Center for Genetic Engineering and Biotechnology (CIGB)-M3 is a bacterial recombinant multivalent antibody fragment derived from the anticarcinoembryonic antigen (CEA) mouse Mab CB/ior-CEA.1. 10 –16 A 99mTc form of CB/ior-CEA.1 has been approved in Cuba and other countries for the scintigraphic follow-up of operated colorectal cancer patients. But, because of its immunogenicity and unfavorable liver accumulation, 17,18 CB/ior-CEA.1 cannot be developed into a molecular radiotherapeutic product. The approach to this problem was to preserve the excellent specificity of the CB/ior-CEA.1 antibody binding site and convert it into a smaller molecule, without Fc, CH1, or Ck mouse constant domains. In the design of the CIGB-M3 scFv, the variable heavy (VH) and light (VL) domains are interspaced by a 5-aa linker that favors the production of tri- and divalent forms (diabodies and triabodies) in the bacterial periplasm, which are later purified and isolated by metal ion affinity and size exclusion chromatographies, respectively. The trivalent form of CIGB-M3 has been used in preclinical studies and shown to have identical specificity when compared with the parental monoclonal antibody. Radiolabeled CIGB-M3 is also selectively accumulated in CEA+human LS174T tumor xenografts growing in nude mice. 10,19,20
The trivalent form of the CIGB-M3 has been produced under GMP conditions and batches submitted to stability, preclinical toxicology, and other tests required by the Cuban regulatory authority for a Phase I clinical trial application permission. This article reports the results of the conducted Phase I clinical trial where untreated colorectal cancer patients with CEA+tumors were intravenously injected with two dose levels of 131I-labeled CIGB-M3, to evaluate safety, biodistribution, pharmacokinetics, and the potential of this antibody fragment for the molecular radiotherapy of these tumors.
Methods
A Phase I, open-label clinical trial was carried out with the participation of the National Institute of Oncology and Radiobiology (radiolabeling, patients, biodistribution, and pharmacokinetic studies) and the “Hermanos Ameijeiras” Hospital (radiolabeling), both in Havana, Cuba. The clinical protocol was approved by the ethics committees of the participating institutions and by the Cuban regulatory authority (State Center for the Control of Medicaments; CECMED). The study complied with the Declaration of Helsinki.
Patient eligibility
Main inclusion criteria were age beyond 18 years, with histologically and immunohistochemically confirmed CEA+colorectal adenocarcinomas in any clinical stage of the disease, eligible for surgery, and with no previous oncospecific treatment. Patients to be included in the trial should have WHO performance status ≤2, adequate bone marrow function with neutrophils ≥1.5×109/L, hemoglobin ≥9 g/L, platelets ≥100×109/L, adequate clotting with international normalized ratio≤1.3, creatinine clearance >50 mL/min, and adequate hepatic function ≤2×upper limit of the normal value. The uses of contraceptives by women in fertile age were compulsory.
Main exclusion criteria were a history of another neoplastic disease, previous administration of some murine, chimerical or humanized antibody, hypersensitivity to preparations that contain iodine, uncontrolled hypertension, and autoimmune disorders or another noncompensated chronic disease. Written informed consent was mandatory for inclusion in the trial.
Study design
Each included patient would receive a single intravenous (i.v.) dose of the radiolabeled anti-CEA CIGB-M3 antibody fragment, administrated in volumes of 300 μL to 1 mL over a period of 1–2 minutes. Two treatment groups were defined. The first group would receive 0.3 mg of radiolabeled CIGB-M3, and the second group 1 mg of the same product. In both cases, the total radioactivity dose was similar, at 5–7 mCi (185–259 MBq) of 131I.
Because of safety concerns, the second group would not start until 48 hours after the last patient of Group I was injected, in the absence of severe adverse events (AEs). No routine preventive allergic prophylaxis should be offered, but i.v. hydrocortisone 100 mg and chlorpheniramine 10 mg were programmed if clinically needed.
Three (3) days before antibody fragment administration and continuing for 1 week afterward, patients should receive a daily iodine solution (150 mg/day) to prevent uptake of 131I by the thyroid gland. Evacuation enemas should be administered 12 hours prior to the injection to guarantee no fecal elimination of the antibody fragment at least during the first 24 hours after administration.
After a follow-up period of 72 hours for biodistribution and pharmacokinetics studies, patients were free to receive the established conventional treatment (surgery, followed by chemotherapy and/or radiotherapy), exception made of therapeutic antibodies, because the latter could interfere in the determination of anti-CIGB-M3 antibodies.
The vital signs of patients would be taken during the first 24 hours, and any AE (clinical and laboratory alterations) should be recorded during the first month after injection. The presence of anti-CIGB-M3 antibodies in patient's sera samples should be evaluated until 6 months after the first administration.
Plasma CEA levels are used as a control variable, measured only at study entry time.
CIGB-M3 antibody fragment preparation
Human-grade quality (GMP) CIGB-M3 antibody fragment was produced in lyophilized form (0.3 mg/vial) by the Development Unit of CIGB (Havana). Details about the origin of the antibody fragment, and other data related to production, purification, and preclinical studies, have been reported elsewhere. 10,19,20 The CIGB-M3 scFv produced by the recombinant bacteria have been recently characterized by mass spectrometry and X-ray crystallography as a mixture of biologically active tri- and divalent (triabodies and diabodies) (manuscript in preparation). During the GMP production procedure, the mixture is submitted to a size exclusion chromatography polishing step that produces a reproducible preparation with more than 80% triabody forms. This preparation has been used in preclinical studies and in this clinical trial.
CIGB-M3 radioiodination
The lyophilized CIGB-M3 scFv preparation was reconstituted with injection sterile water to attain a concentration of 1–1.5 mg/mL. Chloramine-T (Sigma) was mixed with the antibody fragment to a molar ratio of 50:1, together with 444–592 MBq (12–16 mCi) of 131I-Na (CENTIS, Havana) in 0.05 M PBS. The mixture was vortexed, and after 2 minutes, 100 μL of sodium metabisulfite in 0.05 M PBS was added according to the amount of chloramine-T. Subsequently, the reaction mixture was purified on a preequilibrated 15×50 mm Sephadex G-25 polypropylene column (Amersham Pharmacia Biotech). The radioactivity of each 1 mL fraction was measured in an activimeter (PTW, Curiementor 3) and the fractions containing the radiolabeled product were pooled and filtered through a 0.22-μm cellulose membrane sterile filter (Millipore).
The radiolabeling efficiency was assessed by instant thin-layer chromatography in 1×12 cm strips, using 0.9% saline as mobile phase. The immunoreactivity of the radiolabeled fragment was controlled as described by Wu et al. 15 Briefly, 50 μL (50 μg) of radiolabeled fragment was incubated for 30 minutes at 37°C with 1 μg of CEA (Calbiochem) in 500 μL of 50 mM PBS. This reaction was fractioned by FPLC size exclusion chromatography and samples were counted in a gamma well counter (CAPINTEC, CAPRAC-R). Radioactivity values were plotted and a corresponding radiochromatogram was obtained. Immunoreactivity was estimated from the area under the curve.
Dosimetry estimates and biodistribution analysis
Static planar imaging studies from head, chest, abdomen, and pelvis were performed at 2, 4, 8, 24, 48, and 72 hours after radiolabeled antibody fragment injection using a General Electric 400T gamma camera with a high-energy collimator. Geometric mean count rate of anterior and posterior views were used to evaluate the uptake and retention of radiotracer in normal organs and tumor. For whole-body dosimetry, probe measurements from anterior and posterior counts of patients located at fixed distances were used.
21
The estimation of absorbed dose in normal organ and tumor was performed using the MIRD scheme.
22
The normal organs' S-values for 131I (reference man and woman phantoms) were downloaded from
Activity estimates in tumor surgical samples
The radioactivity associated with tumor samples from several patients who underwent planned surgery at 7–9 days after 131I-CIGB-M3 administration was measured in a gamma well counter (CAPINTEC, CAPRAC-R) and estimated as %ID/g of tissue. Nontumor, adjacent tissue samples taken at surgery were also processed and used for comparison purposes.
Pharmacokinetic study
Blood samples were drawn at 5 minutes, 15 minutes, 30 minutes, 1 hour, 2 hours, 4 hours, 8 hours, 24 hours, 48 hours, and 72 hours after administration of the radiolabeled antibody fragment. Urine corresponding to the time periods 0–2, 2–8, 8–24, 24–48, and 48–72 hours after administration of the radiolabeled antibody fragment was collected. Patients were also asked for urine samples before each gammagraphic study.
Whole blood, serum, and urine samples were counted in a gamma-well counter (CAPINTEC, CAPRAC-R). To correct for radioactive decay, injection standards were counted simultaneously. Radioactivity of these samples was expressed as the percentage of injected dose per liter (%ID/L).
To calculate the amount of radioactive fraction associated with the protein, 200 μL samples (serum and urine) from each time point were precipitated with 20% of trichloroacetic acid (TCA) and 4% HSA. After 30 minutes incubation and centrifugations, the radioactivity in supernatant and pellet were counted. The pharmacokinetic parameters were estimated using the WinNolin professional version 2.1 (Pharsight Corporation).
Radiolabeled antibody fragment stability in patient's serum
To evaluate the stability of the radiolabeled protein, 100 μL serum samples from each extraction time were analyzed by FPLC size exclusion chromatography using a Superose 12 HR 10/30 column (Amersham Pharmacia Biotech). Fractions taken every 1 minute were collected and the radioactivity was measured in a gamma-well counter (CAPINTEC, CAPRAC-R). The retention times of free 131I-CIGB-M3 and of the immunocomplex formed by mixing 131I-CIGB-M3 and CEA, in this same column, were taken as reference to interpret the results.
Analysis of human anti-fragment antibody response
The human antibody response against CIGB-M3 was assayed in patient's serum samples taken before injection and at 2 weeks and 1, 3, and 6 months after administration, using a quantitative indirect ELISA assay. Briefly, Costar 96-well polyvinyl plates were coated with 25 μg/mL of CIGB-M3 antibody fragment in PBS for 2 hours at 37°C. After blocking the plates with skimmed milk for 1 hour at 37°C, patient's serum samples were diluted from 1:50 to 1:64,000 in PBS–skimmed milk 3% (m/v) and 100 μL of each dilution pipetted into duplicate wells. The plates were incubated for 1 hour at 37°C. After several washes, specific recognition of anti-CIGB-M3 antibodies was done by adding 100 μL/well of protein A-HRPO (1:80,000; Sigma) for 1 hour at 37°C. After several washes, the reactions were developed with 5 mg orthophenilendiamine (Sigma) and 10 μL H2O2 in citrate solution for 15 minutes at 25°C. Sulfuric acid 2 N was the stop solution. Absorbances were read at 492 nm in a LabSystems Multiskan MS. Serial dilutions of purified rabbit polyclonal anti-CIGB-M3 IgG (from 0.45 to 200 ng/mL) were used to generate a standard curve. A patient's serum sample was considered positive if the detected antibody value was>12.5 ng/mL.
Plasma CEA
CEA levels in blood were measured by an immunoradiometric assay using the CIS Bio International ELSA-2-CEA kit.
Statistics
Data were double entered and validated on Microsoft Access and then imported into SPSS version 13.0 for further analysis. Continuous variables were expressed as mean±standard deviation or median±interquartile range and minimum and maximum values (range). With these variables, analyses of normality (Shapiro Wilk's test) and homogeneity of variance (Levene's test) were carried out. Categorical variables were given as absolute values and percentages. Groups (if comparable) were compared using the Fisher's exact or chi-square tests for categorical variables and the Student's t-test (parametrical) or Mann–Whitney's U test (nonparametrical) for continuous variables. The level of significance chosen was 0.05.
Results
Patients
Seventeen patients diagnosed with colorectal cancer were enrolled in the study. The first 10 patients received 0.3 mg of the radiolabeled CIGB-M3 antibody fragment (Group I) and the following 7 received 1.0 mg (Group II). Groups were balanced according to demographic and baseline characteristics (Table 1). Nine patients were male and 14 were of white skin color. The age ranged between 60 and 80 years. As expected, colon cancer (70.6%) prevailed over rectum cancer. Tumor volume was higher in patients from Group II (160±75.8 g vs. 112±139 g). The WHO clinical cancer stage II was the most frequent, with almost half of the included patients. The mean serum CEA values were higher (and variable) in Group II but were not associated with tumor stage in any of the groups.
Data are expressed as mean±standard deviation (range) or absolute value (percentage).
Estimated from morphometric data obtained after surgery or from computed axial tomography images.
Positive value:>4 ng/mL.
CEA, carcinoembryonic antigen; SD, standard deviation.
Radiolabeling
Taking into account that the same amount of 131I (5–7 mCi) was used to label both 0.3 mg (Group I) and 1 mg (Group II) of CIGB-M3, the specific activities were 16.7–23.3 and 5–7 mCi/mg, respectively. The radiolabeled CIGB-M3 fragments were stable at the two produced specific activities. After purification, the radioactivity associated with protein was 98.8%±1.2%, and immunoreactivity was always over 85%. Patients were injected 30–45 minutes after radiolabeling.
Toxicity
All the AEs registered up to 1 month after injection are shown in Table 2. These were similar for both groups, appeared at least 72 hours after CIGB-M3 single injection, or were associated with other interventional procedures. None could be related with the administration of the radiolabeled fragment preparation. The most frequent AEs were those related to laboratory alterations, such as anemia (35.3% of the patients), increase of erythrosedimentation rate (35.3%), thrombocytosis (29.4%), and leukocytosis (29.4%), all of them common in cancer. Most of the registered events were mild (80.5%) and just one anemia was categorized as severe in 1 patient (#9) from the first group, which required a transfusion of red cells.
None of these AEs was related to the radiolabeled fragment.
AE, adverse event.
No significant changes were detected in routine hematological and biochemical parameters between baseline and 1 month after injection values for each group.
No human anti-CIGB-M3 antibodies were detected in any patient after the single-dose injection of the antibody fragment, during the 6-month analysis period of all patients.
Radiolabeled CIGB-M3 stability in serum
FPLC
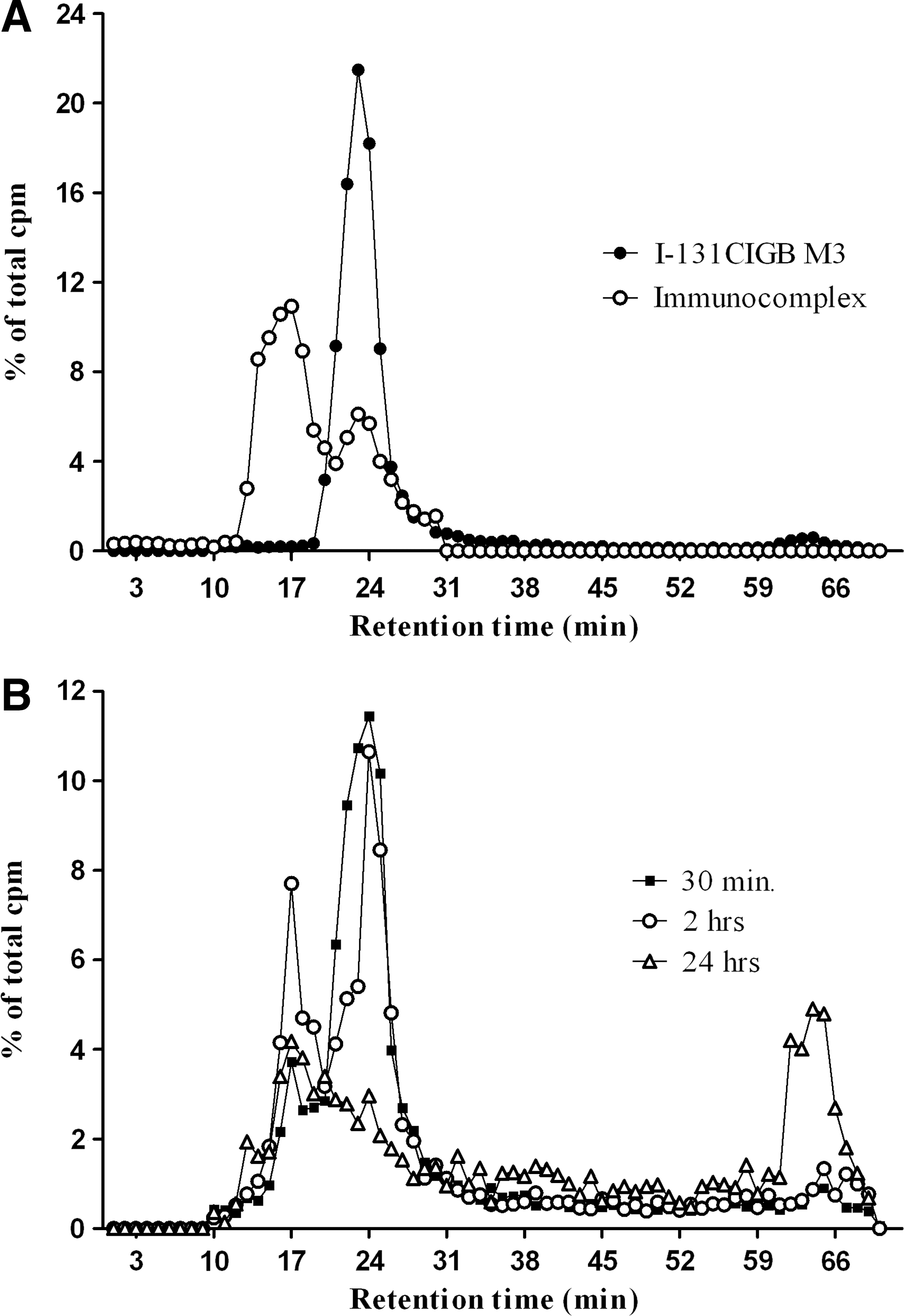
Figure 1A shows the FPLC profiles of free (peak with retention time of ≅24 minutes) and CEA-associated (peak with retention time of ≅17 minutes) radiolabeled CIGB-M3. These two in vitro generated profiles were taken as reference for the analysis of patients' serum radiochromatograms, of which Figure 1B shows a representative behavior (patient no. 9). A proportion of radiolabeled CIGB-M3 seems to rapidly associate with antigen in circulation, and a substantial amount remains as free unassociated fragment for at least 2 hours. At the 24 hours time point, both free and associated radiolabeled fragments are present in circulation, but as a diminished fraction of the total injected radioactivity. In consequence, a peak of free iodine (retention time ≅65 minutes) is apparent. Most of the patients had flat profiles after 48 hours, indicating that either the radiolabeled CIGB-M3 antibody fragment had been sequestered by the tumor or 131I separated from the molecule (see Urine analysis section given later). No correspondence of profiles and circulating CEA blood levels at diagnosis was found.
Protein precipitation
The percentage of 131I radioactivity associated with serum proteins at different times after administration of the labeled antibody fragment was studied using serum TCA precipitation. Figure 2A and B shows the behavior of individual patients in Groups I and II, respectively. Highest values were obtained for the 30-minute and 2-hour time periods, in correspondence with what was found by FPLC. The percentage of 131I radioactivity associated with serum protein had already decreased at the 24 hours time point. At 48 and 72 hours, minor increments of radioactivity values were found, with widespread variation among patients.
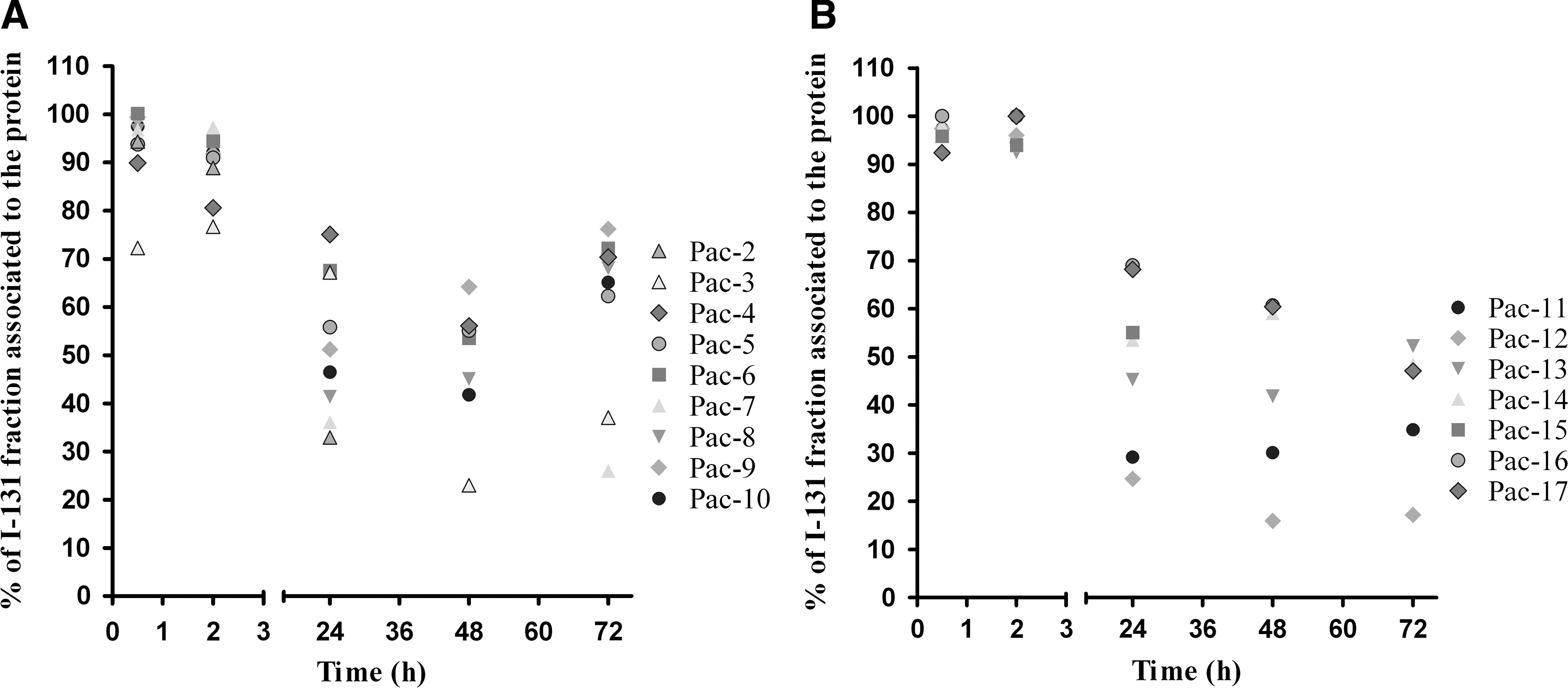
Percentage of 131I radioactivity associated with serum protein (trichloroacetic acid precipitation) at different times after administration of 131I-CIGB-M3.
Urine analysis
Between 30% and 36% of the total injected radioactivity dose was found in urine samples collected during the 8–24-hour time period. By 24 hours, around 50% of the injected dose had been eliminated from the body. This number rose to 80%–85% after 72 hours. The highest urinary excretion rates were found between 2 and 8 hours, with mean values of 0.14 and 0.17 mCi/h for Groups I and II, respectively. The radioactivity in urine associated with protein was under 2% for the whole evaluation period.
Pharmacokinetic analysis
Blood clearance of 131I-labeled CIGB-M3 was better fixed to a biexponential model for i.v. bolus, using the following equation: C(t)=A*e −α*t +B*e −β*t . The general equation includes the macro constants of the initial and terminal slopes that allowed estimating the pharmacokinetic parameters observed in Table 3. The equations were Cp=36.1×e −0.32 t +3.4×e −0.04 t and Cp=20.9×e −2.06 t +24.6×e −0.16 t for Groups I and II, respectively. Concentration values used were those obtained after TCA protein precipitation.
Data are expressed as mean±standard deviation.
AUC, area under the curve (total); t 1/2 α, half-life of the distribution phase; t 1/2 β, half-life of the elimination phase; K 12 and K 21, intercompartmental rate constants; C max, maximum serum concentration; %ID/L, percentage of injected dose per liter; MRT, mean blood residence time; V ss, volume of distribution at steady-state; CL, clearance.
Whole blood and serum radioactivity levels showed an initial rapid decline phase followed by a second slower phase with similar curve profile. The radioactivity concentration in serum moved from 50%ID/L at 5 minutes after injection to less than 0.1%ID/L at 72 hours. Patient 15 (dose: 1.0 mg) showed a higher radioactivity value in serum, with 54.4%ID/L. In this patient, the amount of radioactivity associated with serum proteins was very low at the 48 hours time point.
The labeled CIGB-M3 fragment was distributed with a half-life of 1–2 hours after injection. The half-life of the elimination phase (t 1/2 β) was 14.4±4.6 hours for the 0.3 mg dose group and 6.0±3.6 hours for the 1 mg dose group.
Mean blood residence times (MRTs) were 10.1±1.8 and 6.5±2.7 hours for Groups I and II, respectively. Intercompartmental rate constants demonstrated an exchange equilibrium between compartments in the first group and a virtually irreversible exchange toward the central compartment in the second group. The area under the curve and maximum serum concentration were similar in both groups. No correlation between serum CEA and pharmacokinetic parameters was observed in this study (data not shown).
Biodistribution and dosimetry analysis
The analysis of the immunoscintigraphic images concluded that specific tumor radioactivity was present in 9 of the 10 patients (90%) of Group I and 6 of the 7 patients (85.7%) of Group II. An example of a positive gammagraphy in a patient belonging to Group II is shown in Figure 3.
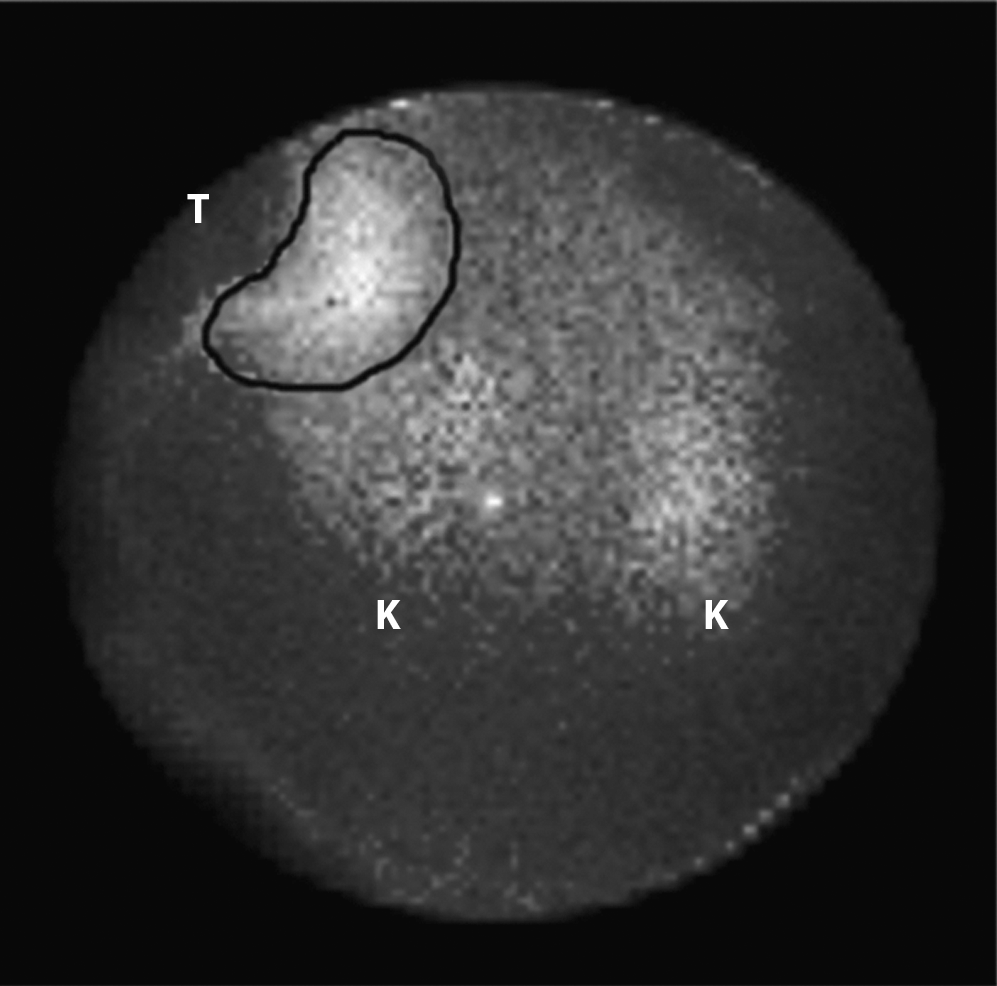
Gammagraphic image from a patient with a cecum well-differentiated adenocarcinoma (tumor mass is 203.7 g by computed axial tomography) at 2 hours after the administration of the radiolabeled CIGB-M3. Specific accumulation (lighter delimited area, labeled as T) is seen in the front abdominal iliac right tumor region that corresponds with colonoscopy data (pseudo kidney form). Kidney accumulation of 131I is seen in areas labeled as K. Serum CEA level=4.1 ng/mL.
The total incorporated radioactivity fraction in tumor was 6.3% in Group I and 6.6% in Group II. The maximum uptake (without weight correction) was 2.7% and 4.7% for Groups I and II, respectively, with an incorporation half-life of 3.1 hours and 1 hour, respectively. The elimination half-lives (Te) were 20.6 and 19.5 hours for Groups I and II, respectively. The mean absorbed radiation dose in tumor was 2.6 mGy/MBq (range from 0.1 to 6.4) for Group I and 1.1 mGy/MBq (range from 0.3 to 1.9) for Group II (Table 4).
Data are expressed as mean±standard deviation.
ID, injected dose per g of tumor tissue; IAF, incorporated activity fraction (×100%); MU, maximum uptake; TMU, time to reach maximum uptake; T i, incorporation half-life; T e, elimination half-life; D, accumulated absorbed dose.
Kidneys, blood, stomach wall, and thyroid could be considered as source organs. The average doses in mGy/MBq are shown in Table 5. Kidney uptake was observed in all the patients enrolled in the study. Stomach wall radioactivity was detected in 40% of the cases of Group I and 57.1% of Group II. Thyroid radioactivity was seen in 3 patients from Group I and in 1 patient from Group II.
The percentages of injected activity per gram of tissue for the source organs and tumor are shown in Figure 4. The mean values of radioactivity in Group I tumors were close to 0.05% during the first 24 hours, with a value over 0.01% (range from 0.0002% to 0.04%) up to 72 hours. Radioactivity accumulation in tumors was higher throughout the study, compared with blood, thyroid, stomach wall, and kidneys. Tumor maximum uptake was registered at 4 hours with 0.06% (range from 0.003% to 0.13%).

Percentage of the injected dose of radioactivity per gram of tissue (%ID/g; mean and standard deviations) in source organs and tumor after 2, 4, 8, 24, 48, and 72 hours of the administration of the radiolabeled CIGB-M3 fragment.
The radioactivity uptake levels in Group II tumors started with 0.04% (range from 0.01% to 0.07%) at 2 hours and then declined gradually to 0.01% (range from 0.003% to 0.02%) at 24 hours and 0.002% (range from 0.0005% to 0.004%) at 72 hours. Tumor values were lower than those for kidneys but higher when compared with thyroid, stomach wall, and blood.
Maximum kidney uptake was 0.04% (range from 0.001% to 0.08%) after 2 hours in Group I and 0.06% (range from 0.03% to 0.08%) after 2–4 hours in Group II. Blood levels registered less than 0.02%, with very low values of 0.0003%±0.0002%ID/g after 72 hours. Patients 1 and 6 of Group I showed the maximum %ID/g values in tumor, with 0.12% and 0.13%, respectively. These patients had small tumors weighing 6.2 and 31.1 g, respectively.
In kidneys, the absorbed dose was higher in Group II, with a mean of 2.0 mGy/MBq, whereas in bone marrow, the overall range was 0.05–0.13 mGy/MBq. The absorbed dose in liver was not measurable.
Radioactivity in surgical samples
Tumor tissue surgical samples obtained 7 or 9 days after 131I-CIGB-M3 administration in 5 colon cancer patients were studied for radioactivity. The %ID/g radioactivity value obtained in the tumor samples was always higher than that for the normal adjacent tissue. The mean %ID/g in tumor tissue for these 5 patients was 0.046%. Patient 17 showed a %ID/g 66 times higher in the tumor than in the adjacent tissue and 3000 times higher than in the peripheral blood. The tumor sample from Patient 13, negative in the scintigraphy analysis, had a %ID/g in tumor tissue three times higher than that in the adjacent normal tissue sample. This patient was a 66-year-old woman with a moderately differentiated adenocarcinoma of the ascending colon. The tumor mass was estimated to be 22.45 g by CAT.
Discussion
The amounts of recombinant antibody fragment and total radioactivity to be administered to the patients in this study were originally selected on the basis of previous clinical trial experience with the intact parental monoclonal antibody and information disclosed in published reports wherein other similar molecules had been used. 17,18,23 –26
In the present study, it was found that the radioconjugate was excellently well tolerated during the trial, with reported AEs only related to the natural course of the disease. Also, no anti-antibody fragment antibodies were detected in the patient's sera up to 6 months after the antibody fragment administration. The absence of Fc, CH1, and Ck domains in the antibody fragment were most probably the basis for this improved behavior, over that of the parental full antibody, which induced HAMA responses in all injected patients with a single 1 mg dose. 25
Because the total 131I dose to be delivered in this study was the same for the two groups of patients, the specific activity was higher (∼20 mCi/mg) in the group receiving 0.3 mg of radiolabeled fragment. This was meant to be an early test on whether higher specific activities, foreseen for future therapeutic purposes, had some influence on biodistribution and pharmacokinetics of the radiolabeled antibody fragment.
Despite some reports indicating that antibodies can suffer significant damage after labeling, 27 –29 no evidence of this was found in the present study. In preparing the patient's materials for this clinical trial, radiolabeling was conducted between 30 minutes and 1 hour before administration of the antibody fragment to patients, and no significant loss of immunoreactivity was registered. This is in correspondence with previous findings in the sense that a significant loss (30%) of 131I was found only after 48 hours of in vitro incubation in human serum of the CIGB-M3 antibody fragment labeled at high specific activity, at 37°C. 20
The stability of the antibody fragment was confirmed in vivo in this clinical trial. Radioactivity associated with precipitated serum protein, or with FPLC retention times indicative of free or CEA-bound antibody fragment, was detected in both dose groups up to 24 hours after administration. At 48 hours and thereafter, radioactivity in serum was mainly found in the form of free 131I.
Urine radioactivity excretion was similar for both groups, with a very high amount of the total injected dose being eliminated from the body after 72 hours. The fact that radioactivity associated with protein in urine was low during the whole period of evaluation indicates that free 131I was measured and that the antibody fragment was not filtered through the kidneys. The latter is consistent with the molecular size of the trivalent fragment, estimated to be 75–90 kDa.
The elimination half-lives of the radiolabeled CIGB-M3 antibody fragments were different between the higher and lower specific activity radiolabeled preparations. The fastest fragment clearance observed for Group II could be due to the existence of patients with bulky tumors in this group, including the patient with liver metastases. Most of the patients in Group I had colon tumors located in the sigmoid region. Patients in Group II had larger tumors of the cecum, hepatic flexure, and ascending colon region, and one of these patients showed liver metastasis with a tumor mass of 104.8 g.
The t 1/2 β values of 14.4 and 6 hours, respectively, are lower than the ones found for the parental mouse monoclonal antibody labeled with 99mTc, which was calculated by Pimentel et al. to be 22 hours in a separate study. 17 Within the comparison limitations imposed by the facts that different radioisotopes were used and the studies were not concomitant, the faster elimination half-life values of the radiolabeled trivalent fragments can be advantageous in a potential therapeutic scenario. With adequate valence and no Fc (hence, no liver recycling), payload delivery to the tumor may be adequate, while attaining less potential damage to normal critical tissues and organs.
Tumor specific uptake was similar among the two dose groups (9 of the 10 patients of Group I and 6 of the 7 patients of Group II), but the %ID/g of tumor tissue value was higher for the former. It can be speculated that the random inclusion of patients with smaller tumors in this group, with probable better accessibility to the radioconjugate, 30,31 favored these results. However, this matter should be studied further if a Phase I/II therapeutic clinical trial is planned, as it could be a more specific consequence of the smaller amount of antibody fragment and higher specific activity administered to this group.
Radioactivity accumulation in tumors over time was higher compared with blood, thyroid, stomach wall, liver, and kidneys. Tumor maximum %ID/g was registered at 4 and 2 hours (Groups I and II, respectively). In previous preclinical experiments using nude mice bearing LS-174 T human colorectal tumor cells, the 131I-labeled CIGB-M3 showed no significant accumulation in the different normal organs, and the highest %ID/g in tumors was found at 24 hours, 20 a difference from the evidence obtained in the present human study that can be attributed to the amount of administered antibody fragments as well as to the already-known important differences in the behavior of animal models, with respect to cancer patients.
The finding of radioactivity in the thyroid of 4 patients was most probably due to an insufficient blockade of the gland. Uptake in stomach wall reported for roughly half of the patients is produced by free iodine capture by the natrium-iodide symporter molecule present in this tissue.
The results of the tracer uptake study in surgical specimens in 5 patients were provocative. Performed 7–9 days after the administration of the radioconjugated antibody fragments, the %ID/g of tissue values were in all cases much higher in the tumor specimen than in the normal adjacent colon tissue obtained during surgery. Patient 13, who was negative by imaging, showed a higher radioactivity value in the removed tumor with respect to the sample of nontumor tissue. The mean value of 0.046%ID/g of tissue for the samples taken from the 5 patients was significantly higher than others reported in the literature, which range between 0.001% and 0.01% of the injected dose. 32
Internal dosimetry showed no significant energy absorption in liver tissue and was very low in bone marrow. The kidneys were identified as the organs that can limit the maximum tolerated dose (MTD), which is understandable as these are the excretion route for free iodine. Considering the absorption in the kidneys, one can make a dosimetry projection for therapy with radioactive maximum loads of the radiolabeled fragment 40 times (11,100 MBq, 300 mCi), the amount that was used in the present clinical trial. Assuming an MTD of 23 Gy for the kidneys, the bone marrow and whole-body doses would be only 0.81 and 0.92 Gy, respectively.
With respect to other similar anti-CEA antibody-related molecules reported in the literature, the CIGB-M3 MRT at the 1 mg dose was faster (13.1 hours) than the mean 29.8 hours documented for the 123I-cT84.66 anti-CEA minibody fragment, 33 of similar molecular size (taking as a reference the triabody form of the present study's scFv preparation). At this dose, CIGB-M3 and the cT84.66 anti-CEA minibody fragment exhibit very similar image sensitivity and positive predictive value (88.2% and 87.5%, respectively). In comparison with another anti-CEA targeting molecule, the 131I-A5B7 F(ab′)2 fragment, 34 urine excretion of free iodine was higher in the present case. A faster clearance can reduce the labeled antibody retention time in tumor but at the same time provide improved therapeutic ratios and less damage to the hematopoietic tissue.
Conclusions
No HAMA response, very low liver accumulation, and a smaller elimination half-life are all important improvements of CIGB-M3 over the parental ior/CB-CEA.1 antibody within a therapeutic scenario. Based on its radioconjugation performance, safety profile, tumor identification, biodistribution, and pharmacokinetic behavior, the CIGB-M3 trivalent scFv antibody fragment should be studied for its possible application in the molecular radiotherapy of human tumors that produce CEA.
Footnotes
Acknowledgments
The authors acknowledge the collaboration of the Development and Quality Control Departments of the CIGB and its Clinical Control Division. The authors also thank the work of hospital staff and technicians at the Nuclear Medicine Departments of the National Institute of Oncology and Radiobiology and the University General Hospital “Hermanos Ameijeiras” of Havana. Finally, the authors value the voluntary decision of all patients included in the study that made possible this clinical investigation protocol.
Disclosure Statement
No competing financial interests exist.