
Abstract
Tc-99m macroaggregated albumin (MAA) hepatic perfusion study and hepatic angiography are routinely performed prior to yttrium-90 (Y-90) microsphere therapy for patients with hepatocellular carcinoma (HCC) or metastatic cancers to the liver. The purpose of this study was to examine the incidence of altered Tc-99m MAA distribution in these patients and to identify factors that are associated with these changes. A total of 176 Tc-99m MAA hepatic perfusion studies in 159 patients performed in preparation for Y-90 microsphere therapy were retrospectively reviewed. Abnormal findings were identified and correlated with diagnosis, infusion site, tumor volume, and tumor uptake by using bivariate statistical analysis. Abnormal Tc-99m MAA distribution on the hepatic perfusion imaging studies include excessive hepatopulmonary shunting with an elevated shunting fraction (>10%; n=23, 13%) and abnormal intra-abdominal visceral deposition in the GI tract, pancreas, spleen, and umbilical vein (n=19; 11%). Patients with a diagnosis of HCC showed higher incidence of abnormal hepatopulmonary shunting compared with other types of tumors (p<0.05). The incidence of abnormal intra-abdominal visceral deposition is higher with infusion into the left hepatic artery or proper hepatic artery/common hepatic artery compared with infusion into right hepatic artery (p<0.001). In 9 of 12 cases with abnormal deposition in the stomach, duodenum, or pancreas, the cause was identified upon reviewing angiography retrospectively and was subsequently corrected. In conclusion, the hepatic perfusion imaging study is an important imaging modality in preparation and guidance of Y-90 microsphere treatment.
Introduction
Primary and metastatic liver tumors are among the most common causes of cancer mortality worldwide. 1,2 Although surgical resection of solitary liver metastases can enhance survival, the vast majority of patients are unresectable at initial diagnosis or recurrence. 2 –4 Radiolabeled micropsheres directly delivered through the hepatic arterial circulation are preferentially localized in the peritumoral or intratumoral arterial vasculature, allowing delivery of a high radiation dose to the tumor and avoiding excessive radiation to the normal hepatic parenchyma. 5,6 Yttrium-90 (Y-90) microsphere therapy has shown promising results for the treatment of patients with hepatocellular carcinoma (HCC) and metastatic tumors in the liver. 7,8
Complications of the therapy can arise from extrahepatic microsphere deposition. Deposition of Y-90 microspheres in the lungs has been reported to be complicated by radiation pneumonitis. 9 Gastrointestinal or pancreatic deposition can cause gastric ulceration, gastroduodenitis, and pancreatitis. 10 Therefore, a Tc-99m macroaggregated albumin (MAA) hepatic perfusion imaging study and a hepatic angiography are routinely performed prior to treatment to assess the vasculature of the tumor and to screen for abnormal distribution of the tracer in the lung and gastrointestinal system.
The present study retrospectively reviews 176 Tc-99m MAA hepatic perfusion imaging studies performed in preparation for Y-90 microsphere therapy. The objective of this study was to examine the frequency of altered Tc-99m MAA distribution and its association with the primary diagnosis, infusion site, and hepatic angiography and to identify the causes of altered tracer distribution.
Patients and Methods
A total of 176 Tc-99m MAA hepatic perfusion studies in 159 patients in preparation for Y-90 microsphere therapy were included and retrospectively reviewed.
Procedure
A catheter was placed either in the proper hepatic artery (PHA) or its left or right branch (left hepatic artery [LHA] or right hepatic artery [RHA]) in the interventional radiology suite. Prophylactive coil embolization of the gastroduodenal artery (GDA) was frequently performed, at the interventional radiologist's discretion, if infusion into the PHA. A hepatic arteriography was obtained to confirm the position of catheter. About 185 MBq of Tc-99m MAA was then injected through the catheter. After the catheter and the sheath were removed and hemostasis at the catheter site was established, the patient was transported to the nuclear medicine suite. Planar images of the whole body and SPECT/CT images of the abdomen were obtained (GE Infinia SPECT/CT scanner). The images were displayed on a computer workstation (Xeleris; General Electric Medical Systems) and interpreted by experienced readers.
Calculation of the fractional shunting to the lungs (ratio of the counts in the lungs to the total counts in the lungs and liver)
Regions of interest (ROIs) were drawn over the lungs and liver and gamma emission counts were obtained on both anterior and posterior planar images. Counts were calculated by multiplying anterior and posterior counts for each ROI and then taking the square root.
Calculation of the tumor volume as a percentage of perfused liver volume and total liver volume and tumor-to-normal liver uptake ratio (T/N uptake ratio)
Three ROIs were drown on every other slice of the SPECT and CT images, over the liver, perfused liver, and liver with increased perfusion representing tumor perfusion. The percentage of tumor volume to the perfused liver volume was calculated. The percentage of tumor uptake to the total liver uptake was also calculated by dividing the total accounts of the tumor by the total accounts of the liver. The T/N uptake ratio was calculated by dividing the average account rate per pixel of the tumor by the average account rate per pixel of the nontumorous liver. 11 For HCC patients, AFP levels obtained at the same time or within 2 weeks apart from the time of the hepatic perfusion study were used for calculation.
Defining abnormal intra-abdominal Tc-99m MAA distribution
Any detectable deposition of Tc-99m MAA in the spleen, pancreas, or bowel was considered abnormal. Uptake in the stomach more intense than kidneys was considered abnormal.
Statistics
Bivariate analysis was performed using chi-square test and t-test.
Results
Patients
A total of 176 Tc-99m MAA hepatic perfusion studies were performed in 159 patients (27 patients had more than one Tc-99m MAA hepatic perfusion study in which Tc-99m MAA was injected into different branches of the hepatic artery). Characteristics including the age, gender, primary diagnosis, and infusion site are described in Table 1.
HCC, hepatocellular carcinoma; RHA, right hepatic artery; LHA, left hepatic artery; PHA, proper hepatic artery; CHA, common hepatic artery.
Those cases with abnormal Tc-99m MAA distribution that were rejected for the treatment or that required further management alteration including Y-90 dose reduction or altered interventional strategies were identified on the hepatic perfusion imaging studies (n=42; 24%; Table 2).
Hepatopulmonary shunting
The majority of the studies (n=153; 87%) demonstrated low-grade uptake in the lungs with a shunting fraction of <10%. Seventeen studies (n=17) demonstrated moderately increased activity in the lungs (shunting fraction of 10%–20%) and six studies (n=6) demonstrated markedly increased activity in the lungs (shunting fraction of >20%) (Fig. 1).

A 60-year-old woman with hepatocellular carcinoma.
Among three subgroups with different primary diagnosis, the frequency of abnormal hepatopulmonary shunting was particularly higher in the HCC subgroup than the other two subgroups (p<0.05; Table 3). The frequency of abnormal hepatopulmonary shunting among subgroups with different infusion site was not significantly different (p=0.39).
p<0.05.
To determine whether abnormal hepatopulmonary shunting is associated with higher percentage of tumor volume, tumor uptake, or T/N ratio, a bivariate statistical analysis using t-test was performed. The mean of tumor volume (%), tumor uptake (%), T/N ratio, or AFP levels (for HCC patients only) showed no statistical differences between the group with low degree of lung uptake versus that with elevated lung uptake (p=0.54, 0.34, 0.33, and 0.29, respectively; Table 4). No correlation was found between the hepatopulmonary shunting ratio and tumor marker levels (AFP) in HCC patients (p=0.634).
Abnormal intra-abdominal deposition
Abnormal intra-abdominal deposition was identified in 19 cases, including gastrointestinal and/or pancreatic deposition (n=12), umbilical vein deposition (n=5), and splenic deposition (n=2) (Table 2). Using bivariate statistical analysis, it was found that infusion of Tc-99m MAA into the LHA or into the PHA/common hepatic artery (CHA) was associated with a higher frequency of abnormal intra-abdominal deposition of the radiotracer compared with infusion into the RHA (p<0.001; Table 5). The subgroups with different primary diagnosis showed no difference in frequency of abnormal intra-abdominal deposition (p=0.12).
p<0.001.
Twelve (n=12) patients were identified with a high degree of Tc-99m MAA deposition in the stomach, duodenum, or pancreas. These patients were either injected in the LHA (n=5) or in the PHA/CHA (n=7) and none of these patients were injected in the RHA (Table 6). Upon reviewing the hepatic arteriography performed before Tc-99m MAA infusion, the following vessels were found to be responsible for anomalous Tc-99m MAA deposition: GDA (n=4); right gastric artery/branches (n=3); and aberrant left gastric artery/branches (n=2). No definite cause was identified in the rest of the three cases (n=3; Table 6). Those cases with identifiable causes on the hepatic arteriography were further managed with altered interventional strategies by coil embolization of the involved arteries and/or repositioning of the microcatheter more distally to avoid tracer flowing into those vessels (Table 6: cases 1–9; Figs. 2 –4). All 9 cases were successfully treated with Y-90 microsphere therapy without complications. The remaining three cases without identifiable cause on the hepatic arteriography were rejected for Y-90 microsphere therapy.
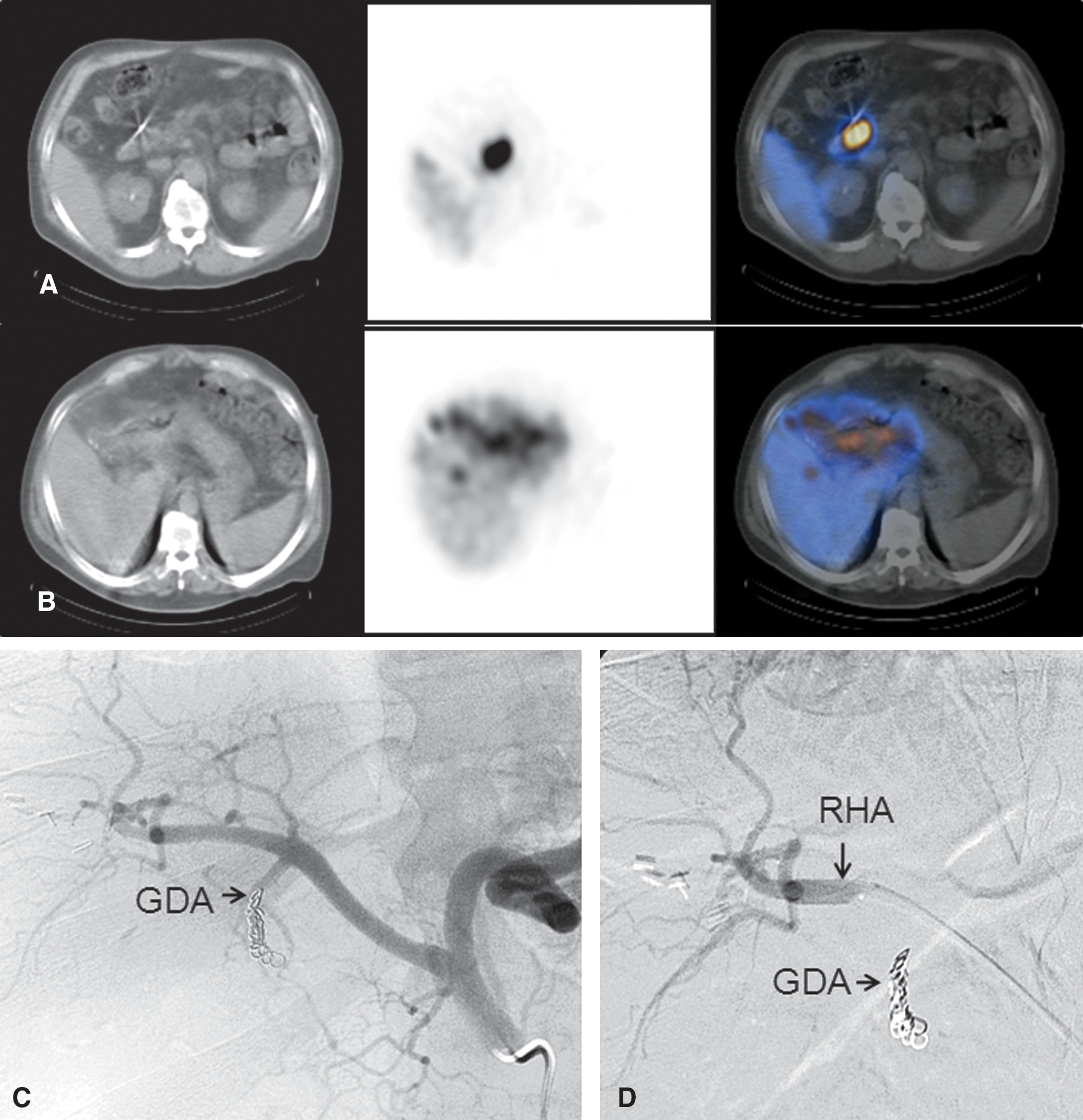
A 56-year-old man with neuroendocrine tumor metastatic to the liver.
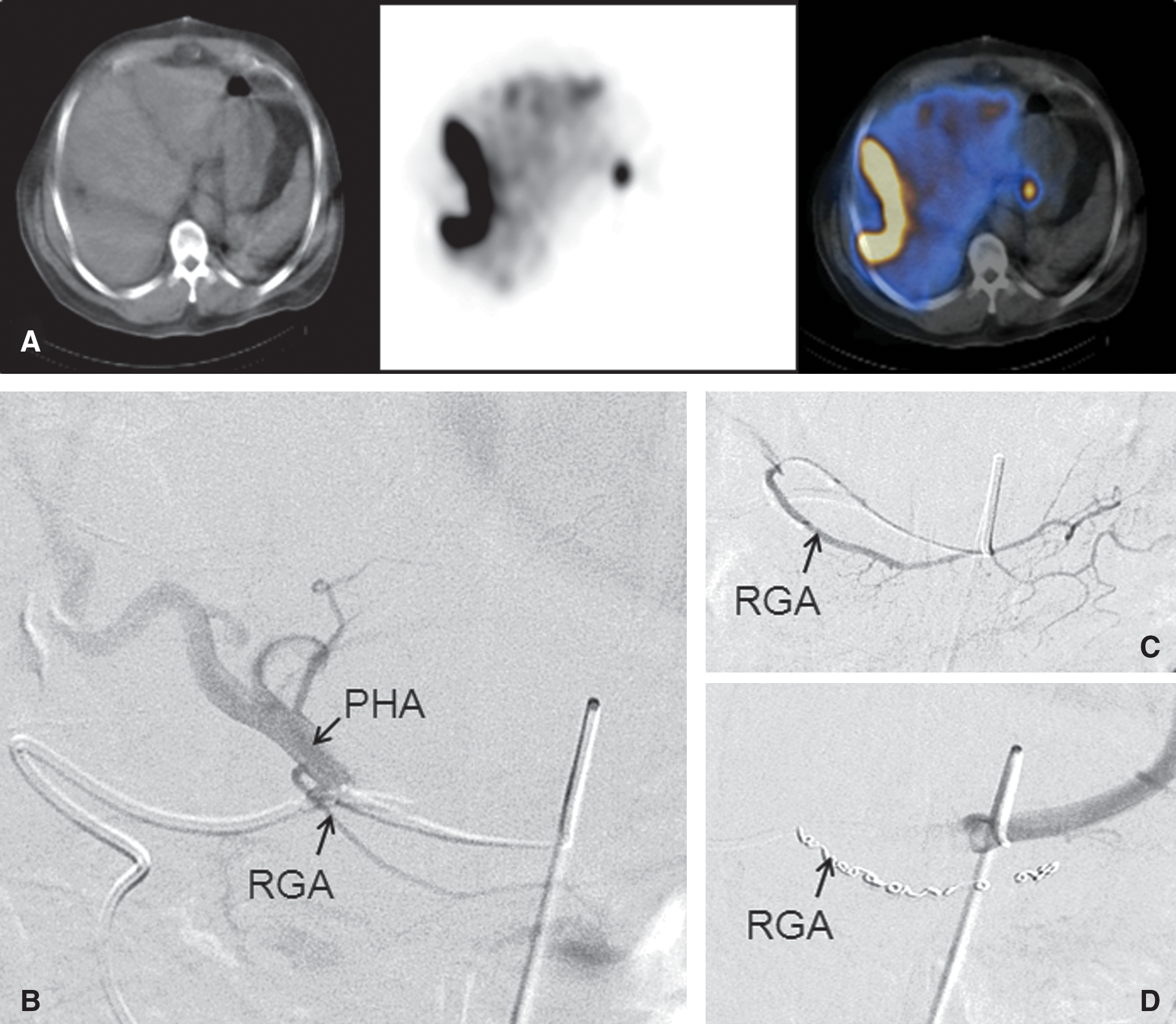
A 62-year-old man with colon cancer metastatic to the liver.
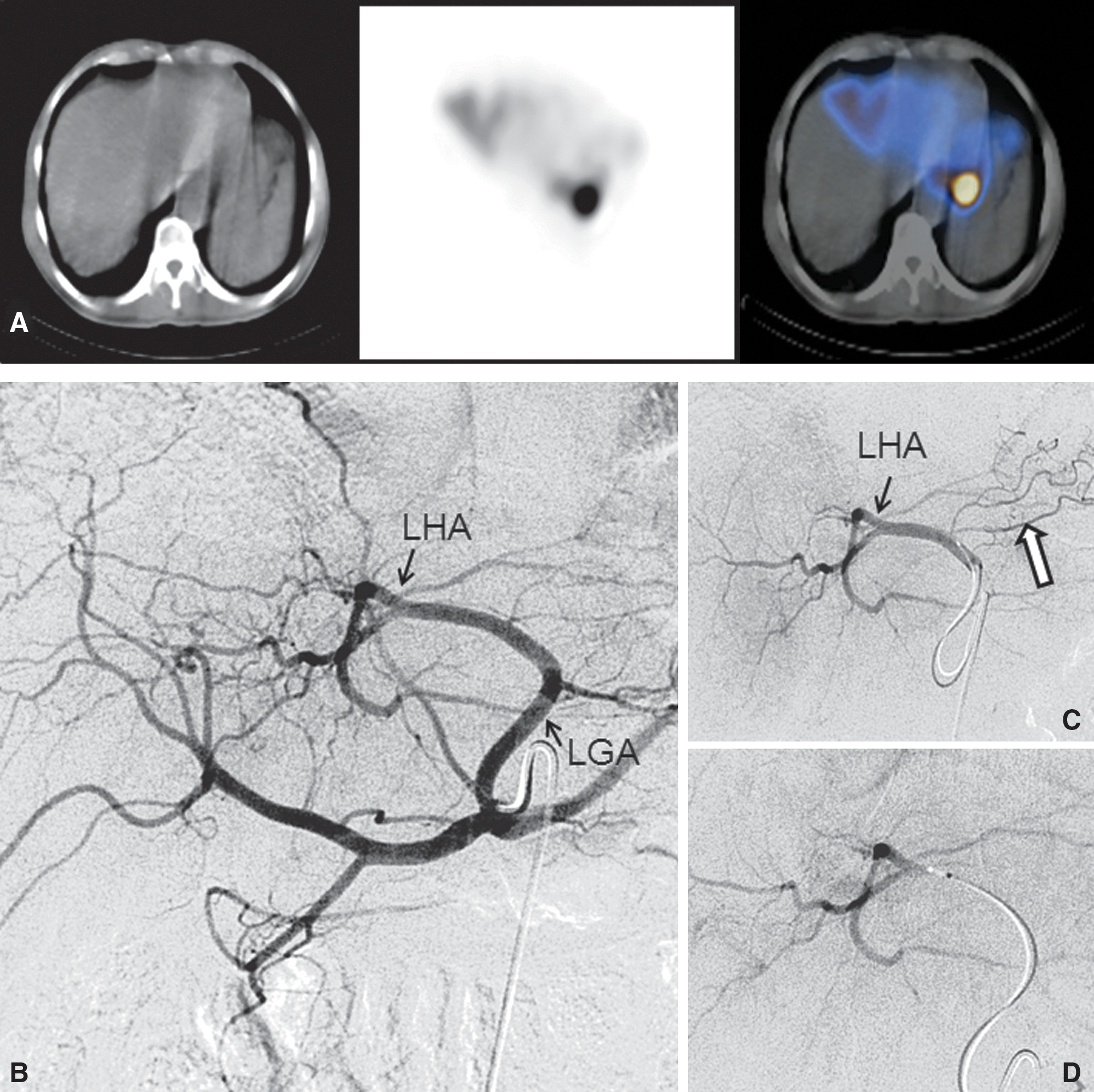
A 66-year-old man with hepatocellular carcinoma.
GDA, gastroduodenal artery; RGA, right gastric artery; Y-90, yttrium-90; NET, neuroendocrine tumor; HCC, hepatocellular cancer; COL, cholangiocarcinoma.
Abnormal radiotracer deposition in the umbilical vein was identified in 5 cases (n=5). Three of these patients (n=3) were injected in the LHA, and 2 (n=2) were injected in the PHA/CHA but none had been injected in the RHA. Three patients were rejected for Y-90 microsphere therapy and the other 2 patients were successfully treated with Y-90 microsphere therapy after changing the injection site, one from the PHA to RHA and the other from LHA to RHA. However, no abnormal angiographic findings were identified on the hepatic arteriography for any of the 5 cases.
Tc-99m MAA deposition in the spleen was identified in 2 cases (n=2). In 1 case, angiogram of the celiac and superior mesenteric arteries demonstrated a stenosis in the hepatic artery. This patient was rejected for Y-90 microsphere therapy based on these findings. In the other case, retrograde flow from the hepatic artery to the splenic artery was evident on hepatic arteriography. This patient was successfully managed by changing the position of the catheter for injection more distally in the RHA.
Discussion
Y-90 microsphere therapy has been increasingly employed to treat primary or metastatic liver malignancies. However, there is limited information regarding the cause of the aberrant Tc-99m MAA distribution correlation with clinical data and hepatic arteriography.
Based on the results of Tc-99m MAA studies, abnormal findings can be classified into two categories: abnormal lung uptake due to hepatopulmonary shunting and abnormal intra-abdominal visceral deposition.
Prior studies suggested that an abnormal neoplastic vasculature (including increased capillary diameter and length, formation of arterial-venous fistulas, and loss of the typical vascular hierarchy of the capillary vessels) allows passage of the MAA particles to the venous system and contributes to the hepatopulmonary shunting in liver tumors. 11 –14 A prior study demonstrated that hepatopulmonary shunting was influenced by the type, size, and vasculature of the hepatic tumor. 13 It was also shown that HCC was associated with a higher incidence of hepatic artery to portal/venous shunting and a decrease in mean T/N uptake ratio when compared with other types of tumors metastatic to the liver. 11,13 This is in agreement with the present findings and explains the association between the elevated hepatopulmonary shunting and the primary diagnosis of HCC. The group with low uptake in the lungs and the group with elevated lung uptake did not show differences in the percentage of tumor volume, tumor uptake, as well as T/N uptake ratio. For HCC patients, tumor marker levels (AFP) were not correlated with elevated hepatopulmonary shunting in the present study. These findings suggest that type of tumor, rather than its size, or amount of uptake plays an important role in development of abnormal hepatopulmonary shunting.
There was direct evidence of abnormal hepatic arterial to portal shunting in a few patients on hepatic arteriography (Fig. 1). However, in the majority of the patients, hepatopulmonary shunting was only evident on the Tc-99m MAA hepatic perfusion imaging in the absence of any significant arteriographic abnormalities.
Faint or mild activity was seen in the stomach in nearly all patients along with uptake in the salivary, thyroid glands, kidneys, and urinary bladder because of free Tc-99m pertechnetate produced secondary to dissociation of Tc-99m MAA after injection. Quality control studies on all injected Tc-99m MAA showed no significant free TC-99m pertechnetate prior to injection. When the uptake in the stomach exceeded that in the kidneys, it was considered abnormal. This places a lower limit on the detectable amount of shunting to the stomach because of inability to distinguish a small degree of gastrointestinal shunting from tracer breakdown.
The present study found that aberrant deposition in the stomach, intestine, and pancreas as well as in the umbilical vein exclusively occurred when Tc-99m MAA was injected in the LHA or PHA/CHA, whereas none occurred when MAA was injected into the RHA. Only 1 patient showed abnormal uptake in the spleen when injected in the proximal RHA. These findings indicate that Tc-99m MAA deposition in the gastrointestinal tract, pancreas, and umbilical vein is largely dependent on the anatomy of the celiac axis and the position of the microcatheter for injection. Upon reviewing the hepatic arteriography retrospectively, the cause of abnormal intra-abdominal deposition can be identified and further corrected. The GDA, right gastric artery/branches, and aberrant left gastric artery/branches were the common causes for abnormal GI or pancreatic deposition. These arteries are in closer proximity to the PHA and LHA compared with the RHA. This explains why the RHA offers a safer site for infusion.
In the majority of cases, abnormal flow through the GDA or gastric braches was not evident on angiography. In contrast, using SPECT-CT, hepatic perfusion imaging is a sensitive tool to detect intra-abdominal visceral deposition, even in a very small amount. 15 In the present study, most of the cases with abnormal visceral deposition were either managed by coil embolization of the involved vessels or distal positioning of the microcatheter in the hepatic branches further downstream (distally).
In summary, Tc-99m MAA hepatic perfusion imaging can detect abnormal distribution and provide guidance for Y-90 microsphere therapy. Patients with HCC are associated with a higher frequency of abnormal hepatopulmonary shunting. Infusion into the RHA delivers much less abnormal intra-abdominal visceral deposition and therefore offers a safer infusion site. In conjunction with angiography, many potential complications including radiation pneumonitis, gastroduodenal ulceration, and pancreatitis can be avoided.
Footnotes
Disclosure Statement
No competing financial interests exist.