
Abstract
Purpose:
Neurotensin subtype 1 receptor overexpression is found in a variety of human tumors. The aim of this pilot/phase I study was to assess the safety profile, pharmacokinetics, and imaging characteristics of 99mTc-Demotensin VI in tumor patients.
Methods:
Scintigraphy with 99mTc-Demotensin VI was performed in 14 patients (2 female and 12 male) with advanced tumor stages. The diagnoses were pancreatic adenocarcinoma (n=4), small cell lung cancer (SCLC) (n=4), non-small cell lung cancer (NSCLC) (n=4), and colon carcinoma (n=2). Patients were injected with 500–550 MBq 99mTc-Demotensin VI. Blood samples were taken at various time points and urine was also collected up to 24 hours post-injection (p.i.) Planar images were acquired at 15–30 minutes, 1–2 hours, 4 hours, and 24 hours p.i. with additional SPECT imaging at 4 hours.
Results:
Radiochemical purity always exceeded 95% up to 4 hours. Urinary and blood excretion was rapid with 5.05% ID (mean: n=5) in plasma after 4 hours. No side effects were observed after injection of 99mTc-Demotensin VI. Focal tracer accumulation was observed in 3 patients with brain metastases due to NSCLC, although specificity of this uptake could not be proven. Further, no tumor-related findings were observed. Although stability tests in human plasma revealed that 99mTc-Demotensin VI remained intact up to 2 hours incubation, ex vivo urine analysis indicated rapid metabolism.
Conclusion:
99mTc-Demotensin VI was well tolerated by patients and showed favorable pharmacokinetics; however, tumor targeting was limited to brain metastases. Further studies on stability issues and receptor characterization in tumors are warranted to introduce neurotensin receptors (NTSR) imaging into the clinic.
Introduction
Today the use of radiolabeled peptides in cancer diagnosis and therapy is well established. 1,2 Especially, radiolabeled somatostatin analogs have found a wide application mainly for the detection, staging, and follow-up of neuroendocrine tumors 3 and, recently, for somatostatin receptor targeted radiotherapy as well. 4 However, in a number of frequently occurring tumors, such as in colorectal or exocrine pancreatic cancer, somatostatin receptor scintigraphy fails because of the lack of receptor expression.
An interesting alternative to somatostatin are neurotensin analogs. Neurotensin (NT) is a 13-amino acid peptide first detected in bovine hypothalamus and acts both as a neurotransmitter/neuroregulator in the central nervous system and as a hormone in the periphery. 5,6 To date, three NT-receptor (NT-R) subtypes have been identified and cloned (NTS1, NTS2, and NTS3) with NTS1-R, showing the highest affinity for NT. 7
NT-Rs are expressed in high density by several cell lines of colonic, pulmonary, pancreatic and astrocytic origin, 7 while tumor growth in animals inoculated with colon carcinoma cell lines could be restrained by the use of NT receptor antagonists. 8 Additionally, in vitro studies showed high ectopic NT receptor expression in ductal exocrine pancreatic carcinomas, Ewing's sarcomas, meningiomas, 9 and lung tumors. 10
Buchegger et al. 11 published first results of a novel technetium labeled NT-tracer (99mTc-NT-XI) evaluating ductal pancreatic adenocarcinoma patients. However, results were inconclusive in the small group of patients included in this study.
The authors of the present study were involved in the development of a novel NT analog functionalized at the N-terminal with a tetra-amine chelator, Demotensin VI (N4-(β)Ala-Arg-Dab-Pro-Tyr-Tle-Leu-OH), for stable binding of 99mTc. 12 This compound can be labeled with 99mTc at high specific activities and shows a high mouse plasma stability and a high binding affinity for the NTS1-R on WiDr cells (0.08 nM). It is rapidly internalized in NTS1-R-expressing WiDr cells, and in a WiDr tumor model in mice, 99mTc-Demotensin VI exhibits high and specific uptake in the tumor (up to 4.30%±0.45% ID/g at 1 hour p.i. and 2.31%±0.28% ID/g vs. 0.31%±0.02% ID/g block at 4 hours p.i.) and a fast body clearance via the kidneys into the urine. These qualities were attributed to strategic modifications of the peptide NT(7–13) lead structure to enhance the resistance of easily biodegradable peptide bonds to proteolytic enzymes and modification of the more specifically involved Arg 9 -substitution by Dab 9 and additional replacement of Ile 12 by Tle 12 to stabilize the second proteolysis-susceptible Tyr 11 -Ile 12 bond in the motif. 12
The present article reports on an initial patient study to investigate the safety, pharmacokinetics, and imaging properties of 99mTc-Demotensin VI in patients with colorectal, lung, and exocrine pancreatic tumors. Several reports indicate, as assessed by in vitro evaluation, selective and high expression of NTS1-R in these tumors. Reubi et al., 13 for instance, showed positive NT receptor expression in the majority of 24 ductal pancreatic adenocarcinomas, whereas endocrine pancreatic cancers did not show receptor expression, as assessed by receptor autoradiography. In a further preclinical study, receptor overexpression was also found in most of 26 cases with pancreatic adenocarcinomas. 14 Co-expression of NT and NT receptors was also documented at the molecular level in lung cancer using reverse transcriptase–polymerase chain reaction (RT-PCR). 15 Further, Allen et al. 16 showed that radiolabeled NT binds with high affinity to small-cell lung cancer cells in vitro. Regulatory peptides, including also NT, and their receptors were also found in many human colon cancer cell lines, as assessed by receptor binding studies, immunohistochemistry, and RT-PCR. 17 –19 These preclinical findings were considered a good basis to assume high probability of NT receptor expression in adequate densities and to select suitable tumor patients for inclusion in the present study.
Methods
Patients
Scintigraphy with 99mTc-Demotensin VI was performed in 14 patients (2 female and 12 men) with a mean age of 60.1 years, SD±10.3 years, ranging from 47 to 79 years, (for details, see Table 1). The major inclusion criterion was a histologically confirmed malignancy derived from the lung, exocrine pancreas, or colon, with tumor types selected on the basis of sufficient NTS1-R expression level previously reported. 13 –19 Eight patients suffered from lung cancer (4 patients with SCLC and 4 patients with NSCLC), 4 patients suffered from adenocarcinoma of the pancreas, and 2 patients suffered from colonic adenocarcinoma. All patients were in advanced stage of disease with the presence of distant metastases or enlarged inoperable solitary tumors. This clinical study was approved by the local ethical committee. Application of 99mTc-Demotensin VI was approved by the “Arzneimittelbeirat” of the Austrian Ministry of Health, and all patients gave their informed consent prior to inclusion.
SCLS, small cell lung cancer; LN, lymph node; FDG, fluorodeoxyglucose; CT, computed tomography; MRI, magnetic resonance imaging
Radiopharmaceuticals
[99mTc-N4 0]-(β)Ala-Arg-Dab-Pro-Tyr-Tle-Leu-OH (99mTc-Demotensin VI) was prepared as recently described. 12 Briefly, 20 μg Demotensin VI was incubated with 25 μg SnCl2, 0.001 M Na3-citrate, and 1 GBq 99mTc-pertechnetate in 0.5 mL of 0.1 M phosphate buffer (pH 12.3) at room temperature. After 30 minutes, the labeling solution was neutralized with 1 M NaH2PO4 and then diluted to a final volume of 5 mL with 0.9% NaCl. This solution (pH 6–8) was finally sterilized by filtration through a Millex-GV filter (Millipore) and 500–600 MBq (∼10 μg) of the radiolabeled peptide was injected as a (10 mL) bolus to each patient enrolled in this study. The radiochemical purity was tested by reverse-phase HPLC (Gynkotek M480 low pressure gradient pump with Shimadzu SP6V variable UV detector and radiometric detection) using a Discovery RP Amide C16 column (5 μm, 150×4.6 mm; Supelco) and a aqueous 0.1% TFA and MeCN solvent system. The amount of 99mTc-colloid was tested using ITLC-SG (Gelman, Science) with 1 M ammonium acetate/MeOH 1:1 as solvent system.
Imaging
Whole-body imaging was performed with a double-headed gamma-camera (Elscint HELIX). All patients were imaged at 15 minutes, 1–2 hours, 4 hours, and 24 hours after bolus injection of 99mTc-Demotensin VI. The camera was equipped with a low-energy all-purpose parallel hole collimator, with a window setting at 140 keV and a window width of 10%. SPECT imaging of regions of interest (ROIs) was performed at 4 hours p.i. and, in some patients, additionally at 1 hours p.i. Acquisition parameters were 60 projections, 25 seconds/projection, matrix 64×64, and zoom 1.
Image analysis
All data were analyzed on the HERMES work station (Nuclear Diagnostics). The ROI technique was used for semiquantitative analysis of main organ and tumor uptake. ROIs were drawn over the whole body, tumor sites, testes, intestine, spleen, kidneys, liver, bladder, thyroid gland, heart wall, and a right thigh area (as an ROI for muscle) on conjugated views of the whole-body images. For evaluation of kidney uptake, the left kidney was selected to avoid interference from liver superimposition.
Absolute organ or lesion uptake was calculated from total counts in organs (decay corrected for the 15 minutes image) as a percentage of whole-body uptake from early images at 15 minutes before voiding, using the conjugated views from anterior and posterior images. For the subsequent imaging, patients had to void before. Preliminary dosimetry was performed using OLINDA/EXM. 20 The central dosimetry analysis used patient-specific organ masses estimated from computed tomography (CT) scan–determined organ volume.
Repeated CT evaluation and other imaging modalities, for example, 18 F-fluorodeoxyglucose ( 18 F-FDG) and magnetic resonance imaging (MRI), were used as the reference standard.
Pharmacokinetics
In 4 patients, heparinized blood samples were taken at 1, 2, 5, 10, and 30 minutes and at 1, 2, 4, and 20–24 hours p.i. and radioactivity was determined in a gamma counter. Urine was collected over 24 hours, samples were measured in a gamma counter, and the cumulated excretion was calculated. Excreted urine was analyzed by high-performance liquid chromatography (HPLC) in 3 patients at early time points (1–4 hours) after injection of 99mTc-Demotensin VI.
Metabolic stability
Fresh plasma from human blood was obtained and 99mTc-Demotensin VI was incubated at 37°C. Aliquots at 0, 5, 15, 30, 60, and 120 minutes were analyzed by HPLC to reveal forming metabolites. Urine was collected over 24 hours and samples were analyzed by HPLC in 4 patients at early time points (1–4 hours) after injection of 99mTc-Demotensin VI.
Safety
Acute toxicity of 99mTc-Demotensin VI was tested in male and female mice (RCC Study No. 845940). No sign of toxicity was found up to 33 μg peptide/kg body weight. This amount corresponds to >2000 μg in a 70 kg patient, which is >100 times the dose actually injected to patients.
Patients were monitored during the course of the study (blood pressure and pulse) and routine blood parameters were determined at 24 hours prior to and 1 month after the study.
Results
None of the patients showed any sign of adverse reactions. In general, the injection of 99mTc-Demotensin VI was well tolerated, with no objective changes observed in clinical or laboratory parameters.
Whole-body images of patient No. 3 at different time intervals after injection are shown in Figure 1. Slight physiological uptake was found in the mediastinum and the intestine early after application, which disappeared almost completely after 2 hours p.i. Within just a few minutes after tracer administration, some soft tissue uptake and blood pool activity were observed. This pattern remained stable over the whole scanning period. Although all included patients had elevated tumor load, no specific radiotracer uptake was observed in any of the known tumor lesions in the trunk of any of the 4 pancreatic adenocarcinoma patients, the 2 colorectal patients, or the 8 pulmonary cancer patients. Whole-body retention, as calculated from conjugated views, and residence times are shown in Figure 2. Moderate nonspecific tracer uptake was also found in the breast in 1 female and in 1 male patient who presented with gynecomastia, but without tumor-related disease in this organ.
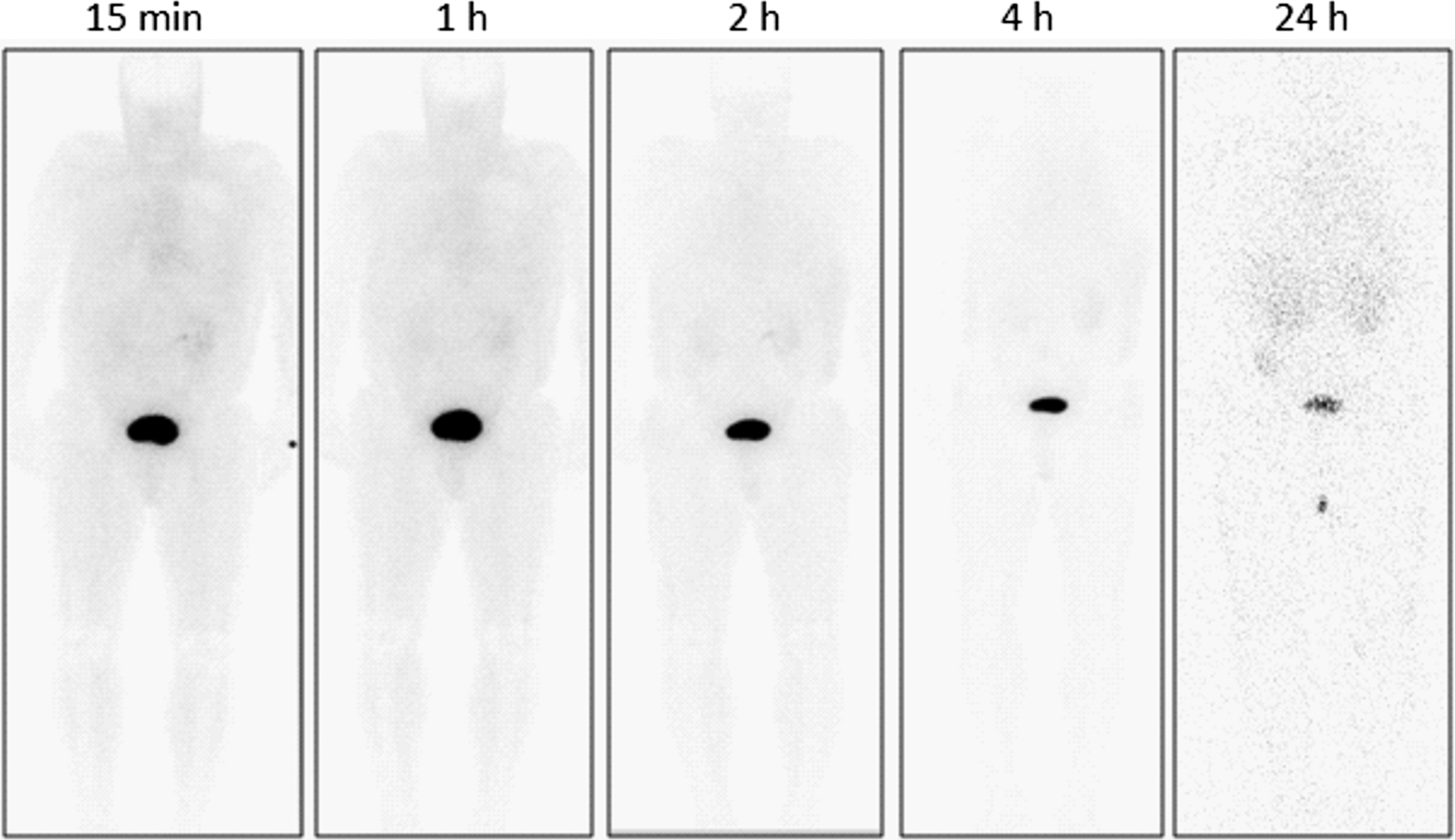
Planar whole-body anterior images at 15 minutes, 1 hour, 2 hours, 4 hours, and 24 hours post-injection (p.i.) of patient 3. In this patient with small cell lung cancer (SCLC) and widespread metastases, no specific tumor uptake was found.

The fraction of administered activity in whole body as a function of time after administration of the radiotracer; all time points are included.
Focal tracer accumulation with high intensity was found in the cerebrum of 3 patients with brain metastases. Each of them suffered from an adenocarcinoma of the lung. Figure 3 shows the pathological tracer uptake in the brain in one of these patients. This patient received no local treatment concerning the cerebral metastasis. The 2 other patients (No. 7 and No. 8) with brain metastases had been treated before scanning with 99mTc-Demotensin VI. In patient No. 7, the brain lesion was resected, and patient No. 8 received external beam radiation. However, all 3 patients showed comparable tracer uptake in terms of the abnormal finding in the cerebrum. Despite the abnormal findings in the brain in 3 patients, tumor-related uptake could not be delineated in the trunk in whole-body images and in SPECT. Radiation-absorbed dose in organs was also calculated based on the residence time of 99mTc-Demotensin VI in 1 patient. Data are included in Table 2.
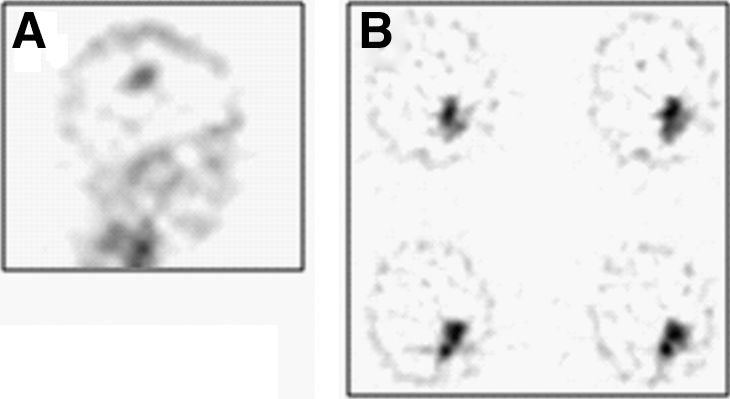
99mTc-Demotensin VI shows intense uptake in the brain metastases of lung cancer in patient 6; SPECT images: sagittal projection
Figure 4 summarizes further pharmacokinetic parameters of 99mTc-Demotensin VI. The plasma time–activity curve (see Fig. 4A) shows a rapid biphasic elimination of 99mTc-Demotensin VI from circulation, with <10% of the injected dose remaining in plasma at 2 hours p.i. Mean cumulative urinary excretion (±SD) was 20.78% (±12.29%) after 2 hours, 18.12% (±6.99%) between 2 and 4 hours, and 53.8% (±38.46%) between 4 and 24 hours (Fig. 4B).
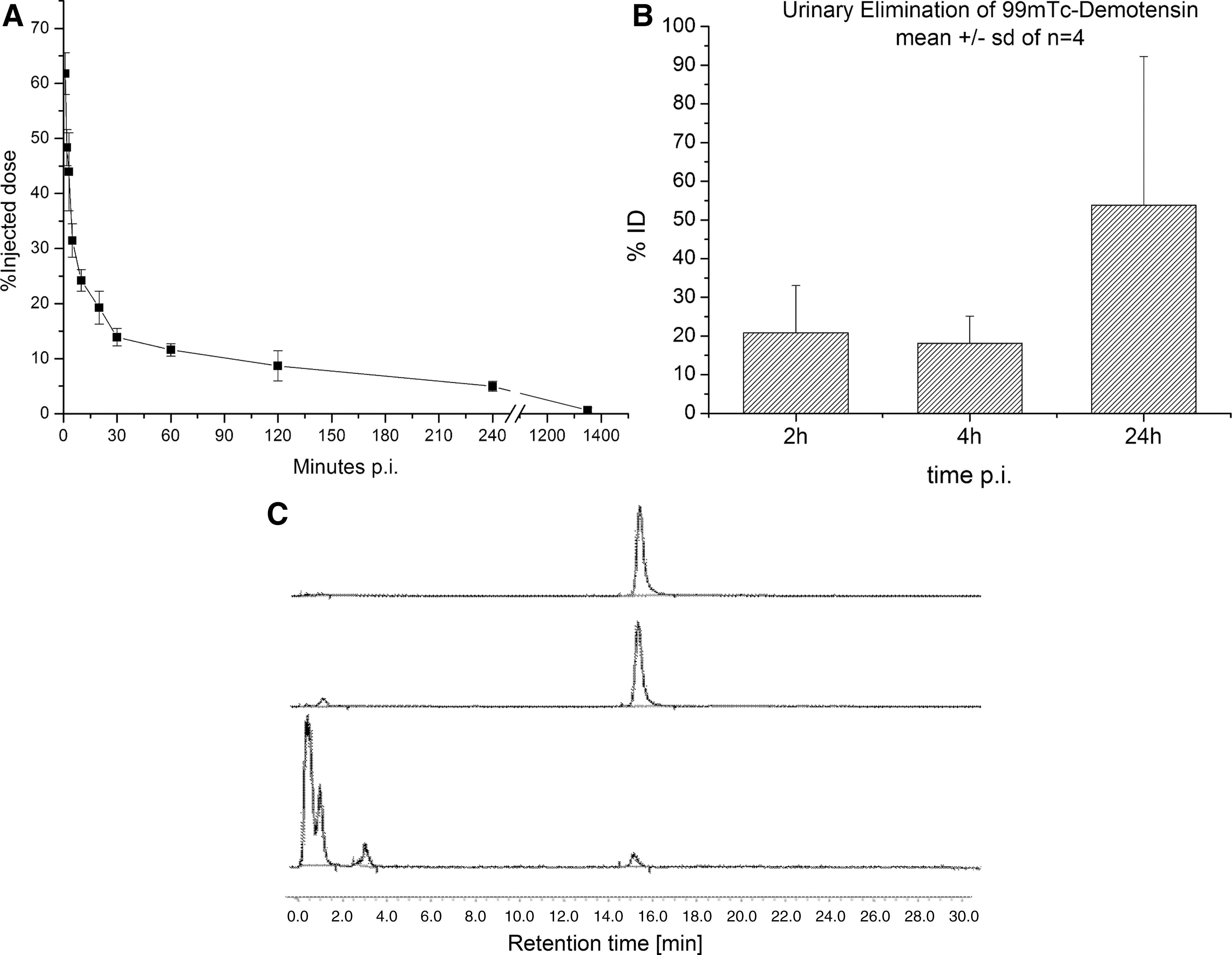
Radiolabeling of Demotensin VI with 99mTc leads to 99mTc-Demotensin VI, with a yield of >95% up to 4 hours. In all cases, <2% free pertechnetate, 99mTc-colloid, or 99mTc-citrate and minimal amounts of peptide-related impurities were detected by HPLC in the quality control analysis before injection (Fig. 4C). Therefore, no purification of the preparation was required and 99mTc-Demotensin VI could be injected after simple sterile filtration. The radiotracer remained 90% intact up to 2 hours of incubation in fresh human plasma at 37°C, as revealed by HPLC analysis (Fig. 4C) and in agreement with previously reported comparable findings in mouse plasma incubates. 12 However, mainly peptide degradation products and only traces (2.0%–11.4%) of intact peptide were detected upon HPLC analysis of collected urine in all samples up to 4 hours p.i. (an example is shown in Fig. 4C). This is in agreement with previously reported findings in mouse urine 12 ; also, HPLC profiles of urine samples in mice and man were very comparable.
Discussion
At present, somatostatin receptor scintigraphy has gained widespread acceptance as a peptide-related tool for tumor diagnosis of neuroendocrine malignancies. 3 The localization mechanism relies on the enhanced somatostatin receptor expression on the cell surface of cancer cells, justifying the use of radiolabeled somatostatin analogs for imaging and radionuclide therapy. 21
Although the overexpression of regulatory peptide receptors has been reported in numerous human cancers, 22 there is little evidence that this approach can be clinically successful for radionuclide imaging and therapy exploiting other molecular targets in addition to somatostatin receptors. Therefore, the present study aimed to provide data on the scintigraphic detection capability of 99mTc-Demotensin VI for NTS1 receptors in selected tumor patients. From the clinical point of view, it might be disappointing that only few tumor sites, especially in the cerebrum, could be delineated, although preclinical data showed that 99mTc-Demotensin VI interacted with a single class of high-affinity binding sites in WiDr cell membranes in a dose-dependent manner. 12 As all included patients showed elevated tumor load with numerous large lesions, limitations of the detection capabilities due to physical properties can be excluded. Although no biopsy of tumor lesions was obtained to provide unequivocal evidence on the receptor expression profile on histopathological level because of ethical concerns, the presence of NTS-1 receptors in these tumors was deduced from several reports in literature. 13 –19 However, it can be assumed that low receptor density and/or cellularity of the type of cancer could in part explain the weakness of the in vivo signal. 22
111In-labeled compounds also showed promising preclinical results for imaging of NTS-1 receptor–positive tumors. 23 Although an 111In-based radiotracer would allow imaging at later time points, thereby favoring delineation of tumors with lower receptor density or employing a lower affinity tracer, the first results with 111In-MP2530 in patients were equally disappointing. 24 In 7 patients with pancreatic adenocarcinoma, no pathological uptake was seen in scintigraphy using this 111In-labeled NT analog. This negative finding was attributed to suboptimal expression level of NT receptors in the lesions as well as to the rapid degradation of the radiopharmaceutical in the blood stream.
Although 99mTc-Demotensin VI was excreted almost completely degraded in the urine of 4 patients even at very early time points after injection as revealed by HPLC analysis of ex vivo urine, it survived incubation in human plasma for up to 2 hours. These results are in accordance with preclinical studies in which only traces of intact peptide were detected as early as 30 minutes after injection in urine after injection of 99mTc-Demotensin VI in mice. 12 Further, in the preclinical study the compound showed to be similarly stable in mouse plasma, but it was rapidly degraded in kidney homogenates. Therefore, the kidneys cannot be ruled out as a major catabolism site of 99mTc-Demotensin VI in vivo for both mice and men, forming metabolic products eventually forwarded into urine to be detected by HPLC. Also, plasma clearance was comparable to the present patient study, considering the overall slower kinetics in man, with 0.55% ID/g in mouse blood corresponding to a total of about 3.3% of ID in total blood at 1 hour p.i. compared with 11.6% ID in patients. In this preclinical study, also specific uptake of 99mTc-Demotensin VI was observed in mouse intestines. 12 However, this finding could not be confirmed in the present evaluation and may be attributed to the different levels of NTS1-R expression between mouse and man.
Nevertheless, in 3 patients, clear tracer uptake was observed in brain lesions. Interestingly, in the present study, there was no difference in the uptake when comparing patients with and without interventions, either by surgery or external beam radiation. Consequently, it could be argued that the tracer localization in brain lesions was caused by direct receptor binding of the radioligand to the receptors in the very brain tissue that have become accessible via the blood–brain barrier leaks caused by tumor growth. Since there is no evidence of receptor-mediated brain uptake, nonspecific accumulation in analogy to uptake of 99mTc-DTPA or 99mTc-pertechnetate in high-grade malignant brain tumors 25 due to passive diffusion indication blood–brain barrier disruption could not be ruled out.
Overall, this study did not reveal final proof of specific tracer uptake in NTS1 receptor–positive tissue in patients, possibly related to both low in vivo stability of this peptide and also low receptor expression in the tumors. Both problems could be addressed in further investigations, on the one hand, to better understand the in vivo metabolic course of 99mTc-Demotensin VI and toward developing more stable analogs and, on the other hand, toward applications in other tumors with potentially higher NTS1 receptor density reported for other tumors, such as Ewing's sarcomas. 9
Conclusions
99mTc-Demotensin VI was well tolerated and showed suitable body clearance, such as rapid renal excretion and minimal abdominal uptake. However, detection capacity was poor in the tumors investigated, especially in pancreatic tumors, most probably because of suboptimal NTS1-R levels in these lesions. These findings are in accordance with results from other groups using different 99mTc- or 111In-labeled NT-analogs. 11,24 The present data further suggest that NT-analogs might not be suitable for imaging pancreatic, colorectal, and lung tumors. However, further investigations seem warranted to evaluate the potential role of NTS1 receptor imaging in oncology.
Footnotes
Disclosure Statement
No competing financial interests exist.