
Abstract
Purpose:
The aim of this study was to examine the efficacy of intra-arterial 90Yttrium treatment in the management of unresectable hepatic neuroendocrine tumors (NET) metastases unresponsive to treatment and the role of 111In-octreotide scintigraphy in the evaluation of treatment response.
Methods:
Thirteen (13) patients with a mean age of 53.3 years not eligible for surgical treatment were included. Before the procedure, routine tests for renal/hepatic functions and bilirubin levels as well as 99mTc-macroaggregated albumin test to detect any leakage to the lungs were done. Treatment doses were calculated using body surface area method and all patients received 90Y resin microspheres through hepatic artery catheter. Abdominopelvic computed tomography (CT) and 111In-octreotide scintigraphy were done before and after treatment. Patients were divided into two groups based on their treatment response as assessed by either 111In-octreotide scintigraphy or CT: group 1, responders; group 2, nonresponders.
Results:
For all patients, 1-year survival rate and overall survival was 84.7% and 20 months, respectively. Based on 111In-octreotide scintigraphy findings, 1-year survival rate was 90% and 66.7% for responders and nonresponders, respectively, whereas corresponding overall survival was 21.3 months and 15.3 months. Survival data based on CT findings were as follows: 1-year survival rate, responders, 80%; nonresponders, 100%; overall survival, responders, 20.4 months, nonresponders, 18.5 months.
Conclusions:
Intra-arterial treatment with 90Y has survival benefits in treatment-refractory liver metastases from NETs and it could be used in these patients. Since it is a functional imaging method, 111In-octreotide scintigraphy may be better discriminates patients responding to treatment from patients not responding.
Introduction
Neuroendocrine tumors (NETs), carcinoid tumors in particular, are rare and heterogeneous group of neoplasms. Since they originate from endocrine cells, they are capable of producing biogenic amines and polypeptide hormones. These tumors are slow growing malignancies with extremely variable location and clinical behavior. 1 NETs and carcinoid tumors most frequently originate from midgut and commonly metastasize to the liver. On the other hand, NETs arising from foregut and hindgut commonly metastasize to the bone. Liver metastases from these tumors are responsible for symptoms due to hormone secretion resulting in carcinoid syndrome. These characteristic symptoms include cutaneous flushing, episodic hypertension, and diarrhea. Although the primary therapy is surgery, hepatic resection is not an option for all patients, since only a very small number of patients have limited disease. Somatostatin analogs such as octreotide and lanreotide are used in unresectable NET patients in an attempt to control carcinoid symptoms and symptomatic control can be achieved in 80% of the cases. However, these patients can be refractory to this therapy in due course. Additionally, there is no certain agreement on the use of chemotherapy in NETs and response rate to this treatment modality is around 30%. 2 On the other hand, re-growth and recurrence occurs after hepatic transarterial embolization (TAE) and chemoembolization (TACE), although the control of the disease is possible for a certain time period. Thus, repeated TAE or TACE procedures are required to maintain stable disease (SD).
Selective internal radioembolization with 90Yttrium has been used to treat unresectable liver tumors. 90Y is a pure β emitter with a physical half-life of 64.2 hours and its average tissue penetration is 2.5 mm. Transarterial procedure with 90Y microspheres treats liver tumors with combining the effects of hepatic arterial embolization and high dose radiation. Reduction in tumor size and increase in survival were observed after treatment with selective intra-arterial 90Y radioembolization in hepatocellular carcinoma and colorectal liver metastases.
111In-octreotide scintigraphy is commonly used for the diagnosis and follow-up of NETs and particularly for NETs of gastroenteropancreatic origin (GEP) possessing high density of somatostatin receptors. Various studies reported sensitivity rates between 67% and 91% for 111In-octreotide scintigraphy in the diagnosis of NETs of GEP origin. 3,4
This study aimed to evaluate the effectiveness of intra-arterial treatment with 90Yttrium microspheres in treatment-refractory and unresectable liver metastases of NETs and the value of 111In-octreotide scintigraphy in the evaluation of treatment response.
Materials and Methods
Thirteen (13) consecutive patients (7 women and 6 men) with unresectable liver metastases from NETs were enrolled in this study. The mean age of the patients was 53.3 years (range, 33–73 years). None of the patients was amenable to curative surgical resection and all patients had progressive disease (PD).
Patient selection and treatment protocol
In all patients, widely accepted parameters regarding liver reserve, bone marrow reserve (granulocytes >1500/μL; platelets >60,000/μL), and hepatic vascularity were used as inclusion and exclusion criteria. Liver reserve was evaluated using bilirubin, aspartate transaminase (AST), alanine transaminase (ALT), and alkaline phosphatase (ALP) levels in blood. A bilirubin level <2 mg/dL and AST/ALT/ALP levels less than five times the upper limit of normal were required for radioembolization. Patients with ascites, portal hypertension, portal venous thrombosis, or an expected survival <3 months were excluded as well as the patients with contraindications for angiography and selective visceral catheterization. To evaluate vascular tree, a therapy-planning angiogram was performed. With this angiogram, branches of hepatic artery to the gastrointestinal tract were coiled to prevent 90Y reflux to the stomach, that is, to gastroduodenal artery and right gastric artery. At the end of this planning angiogram, a 150 MBq dose of 99mTc-labelled macroaggregated albumin was administered through the catheter in an attempt to detect arteriovenous shunts from the hepatic arterial system to the pulmonary system or gastrointestinal tract. After this procedure, imaging was obtained by gamma camera and regions of interest were drawn around the liver and lungs in anterior planar images, and the pulmonary shunt was calculated using the following equation: pulmonary shunt fraction=ROI lung counts/(ROI lung counts+ROI liver counts. Patients with a pulmonary shunt less than 20% were eligible for therapy. The 90Y dose was adjusted according to the following body surface area method: activity (GBq)=(BSA–0.2)+tumor volume/total liver volume. The 90Y resin microspheres (Sirtex Medical) were injected through the hepatic artery catheter under intermittent fluoroscopic visualization. Within 1 to 24 hours after microsphere infusion, Bremsstrahlung images were obtained to confirm that the 90Y deposited only in the liver. All patients were hospitalized overnight and medications like analgesics, antiemetic, and H2 antagonist were administered, if necessary. All patients were closely monitored until acute or late toxicities were resolved.
Follow-up
Pre- and post-treatment imaging studies, including contrast enhanced abdominopelvic multi-slice computed tomography and 111In-octreotide scan, were performed 3 weeks before and 6 weeks after the therapy. Biochemical tests, including liver and kidney function tests, and blood count were repeated every 2 weeks for the first month after the procedure and monthly thereafter.
Planar whole body images were obtained 4 and 24 hours after intravenous administration of 111In-octreotide (222 MBq [6 mCi]). About 500,000 count whole body images and, when necessary, 300,000 counts of spot images were obtained with a wide-angle, medium-energy, double-headed gamma camera (G.E. Millennium MG) equipped with parallel hole collimator at 256×256 matrix and 20% energy window focused to the photon peaks of 111In (172 and 245 keV). For suspected sites, SPECT imaging was done at 24 hours with 128×128 matrix, 30 seconds/step, and 360° of angle. A delayed imaging was performed at 48 hours for indeterminate cases due to intensive gastrointestinal activity, particularly in patients suggestive of an abdominal pathology. All scintigraphy images were reviewed by 2 nuclear medicine specialists, and areas of pathological uptake were recorded.
Treatment response
To evaluate treatment response, a semiquantitative measurement of 111In-octreotide uptake based on tumor/background ratio was done before and after the treatment. Accordingly, SD was defined as the absence of significant change in the tumor/background ratio of the lesions, whereas decreased tumor/background ratio was considered partial response (PR). Disappearance of lesions was complete response (CR), and increased number of lesions and/or tumor/background ratio was defined as PD.
In patients with available abdominopelvic computed tomography (CT) images, response rates were also evaluated using response evaluation criteria in solid tumors (RECIST) as follows: CR, complete disappearance of the mass; PR, at least 30% reduction in the largest diameter; SD, less than 30% reduction but the disease is not progressive; PD, more than 20% increase in tumor diameter.
The average of the responses of each lobe was used when both hepatic lobes received treatment. The initial treatment served as the reference time point for survival estimations.
Patients were divided into two groups for both CT based and 111In-octreotide scintigraphy based treatment response rates. Group 1 included patients with PR and CR, whereas group 2 included patients with PD and SD. Groups were compared for their overall survival according to treatment response based on 111In-octreotide scintigraphy and abdominopelvic CT.
Statistical analysis
Overall survival analysis was performed using Kaplan–Meier method and comparison was done using log rank (Mantel-Cox) test. Nonparametric Mann–Whitney U test was used for the comparisons of the groups with regard to percent changes in tumor/background ratio after treatment.
Results
Patients
Thirteen (13) patients received 16 intra-arterial radionuclide treatments with 90Y between March 2008 and April 2009. The mean age was 53.3 years (range, 33–73 years). Seven (7) patients were female and 6 were male. Primary site of the NET was pancreas in 3 patients, small intestine in 3 patients, rectum in 1 patient, and the origin was unknown in 6 patients. Only 5 patients had other metastatic foci in addition to liver metastasis: 2 patients, in abdominal lymph nodes; 1 patient, in spleen; 1 patient, in the lung; and 1 patient in the lung, spleen and bone. Two (2) of the patients with known primary tumor origin had received surgical treatment for the primary foci (Whipple operation for pancreas and colectomy for rectum). Patients had received the following treatments for their liver metastases before intra-arterial radionuclide treatment: 5 patients, only long acting somatostatin analog (Sandostatin Long Acting Release [Sandostatin LAR®, Novartis]); 4 patients, long acting somatostatin analog plus high dose 111In-octreotide treatment; 1 patient, long acting somatostatin analog plus chemoembolization; 1 patient, hepatic mass excision followed by treatment with somatostatin analog plus chemoembolization; and 1 patient had only hepatic mass excision. The remaining 1 patient received intra-arterial 90Y treatment without any prior surgical intervention or treatment since that patient had idiopathic biliary stenosis (Table 1).
Sand, Sandostatin LAR; Surg, surgery; Chemb, chemoembolization; 111In-oct, high dose 111In-octreotide therapy.
Radiation delivery
Ten (10) patients received treatment for single lobe, whereas 3 patients received treatment for both right and left lobes. The mean treatment dose was estimated as 1.4 and 1.3 GBq for the right and left lobe, respectively. In all patients, the leakage to the lungs was less than 20%. Therefore, neither reduction in the estimated dose nor discontinuation of the treatment was required. Before the treatment, the mean total bilirubin, AST, and ALT levels were 0.5 mg/dL, 90.5 U/L, and 40.6 U/L, respectively; corresponding post-treatment values were 0.5 mg/dL, 29.1 U/L, and 27 U/L.
Toxicity
Technical success of intra-arterial delivery of 90Y microspheres was 100% and none of the patients experienced complication due to angiographic intervention. All patients experienced postradioembolization syndrome characterized by mild abdominal pain, nausea, and subfebrile fever. A combination of a nonopioid analgesic, an antiemetic, and a H2 receptor blocker was given to patients not tolerating these symptoms. Symptoms decreased in intensity within 1 week and completely disappeared in 15 days. Bremsstrahlung imaging done 24 hours after treatment did not show any activity outside the liver. All patients were hospitalized for one night as a preventive measure and prolonged hospitalization was not required in any of the patients.
Response
111In-octreotide scintigraphy was done in all patients, on average 3 weeks before and 6 weeks after the treatment (Fig. 1). Pre- and post-treatment abdominopelvic CT imaging results were available in 10 patients (Fig. 2). Patients were followed for a mean duration of 17.4 months (range, 12–24 months) after the treatment. One-year survival rate, overall survival, and median survival were 84.7%, 20 months, and 18 months, respectively. Kaplan–Meier curve for overall survival is shown in Figure 3.
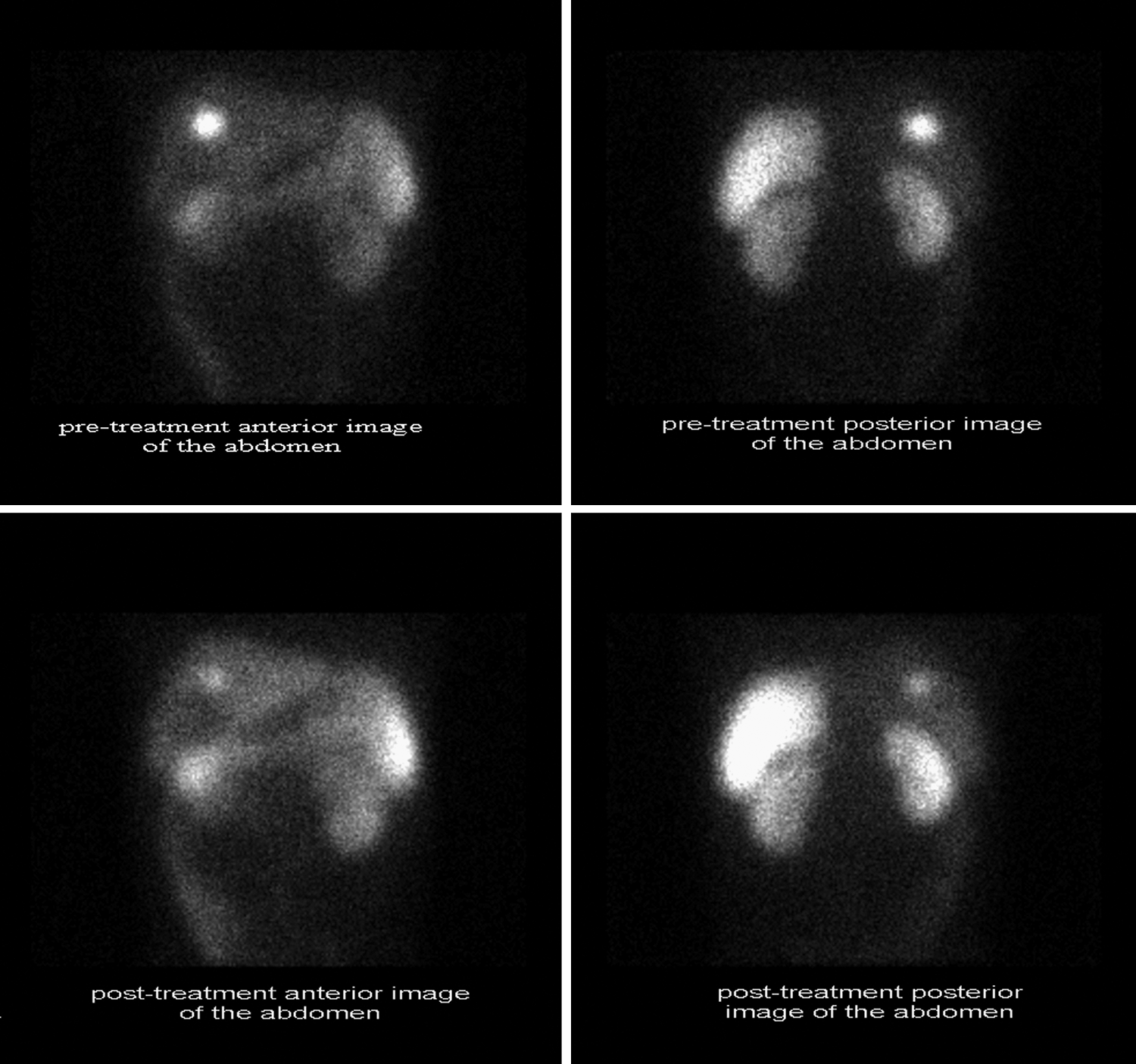
Forty-two (42)-year-old man with liver NET, pre- and post-treatment 111In-octreotide scintigraphy images. NET, neuroendocrine tumor.
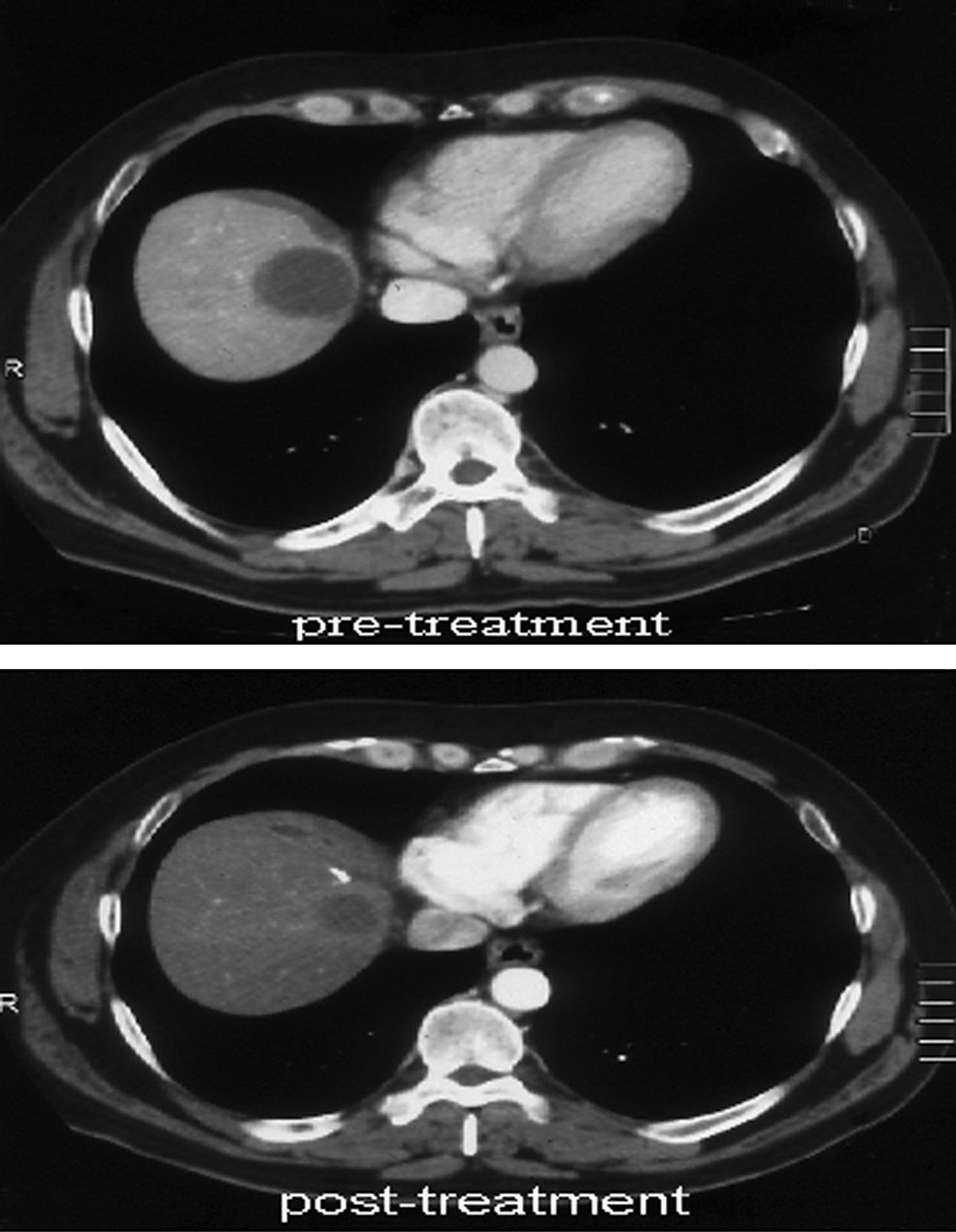
Forty-seven (47)-year-old man with liver NET, pre- and post-treatment CT images. CT, computed tomography.

Kaplan–Meier curve for overall survival after radioembolization with 90Y microspheres.
111In octreotide scintigraphy findings
Based on pre- and post-treatment 111In-octreotide scintigraphy findings of 13 patients, 10 patients achieved PR (77%), 2 had SD (15%), and 1 had disease progression (8%).
Four (4) patients died during follow-up (30.7%) (patients 2, 8, 11, and 12). For these patients, mean post-treatment disease-free survival was 7.25 months and mean survival was 13 months. 111In-octreotide scintigraphy identified two PRs, 1 SD, and 1 PD, among patients who died. The patient with PD was different from the rest of the patient population being the only patient with lung and bone metastasis (patient no. 11). One of the nonsurvived patients with PR died due to abundant amount of VIP secretion (patient no. 2).
111In-octreotide scintigraphy identified PR in 8 out of 9 remaining patients (88.8%) and SD was found in only 1 patient (11.1%) (Table 2).
After intra-arterial treatment.
R, right lobe of the liver; L, left lobe of the liver; PR, partial response; SD, stable disease; PD, progressive disease; CR, complete response.
In 111In-octreotide scintigraphy, decrease in tumor/background ratio after treatment was 30.5%, 8.7%, and 40.2% among all patients, nonsurviving patients, and survivors, respectively (Fig. 4).

Percent decrease in tumor/background ratio on 111In-octreotide scintigraphy after treatment (positive values indicate a decrease in ratio).
Abdominopelvic CT examination findings
Among 10 patients with available abdominopelvic CT results, 1 patient had CR (10%, patient no. 1), 4 had PR (40%), 4 had SD (40%), and 1 had PD (10%), based on the pre- and post-treatment findings of CT images. The results of CT and 111In-octreotide scintigraphy were consistent in 5 out of 10 patients (50%). In 1 of the patients with inconsistent findings (patient no. 1), 111In-octreotide scintigraphy indicated PR, whereas CT findings were in favor of CR, thus CT did not display the lesion. However, the lesion was still active on 111In-octreotide scintigraphy, but lesion/background ratio decreased to 2.08 from 9.36. In 3 patients with inconsistent CT and scintigraphy results, 111In-scintigraphy indicated PR, whereas according to CT findings these patients had SD. The remaining 1 patient had SD on scintigraphy and PD on CT (Table 2).
Comparison of the groups
Percent changes in tumor/background ratio on 111In-octreotide scintigraphy were significantly different between the two groups (p=0.007). On 111In-octreotide scintigraphy, 1-year survival rates were 90% and 66.7%, and overall survivals were 21.3 and 15.3 months, for group 1 (PR and CR) and group 2 (PD and SD), respectively. Based on CT findings, corresponding figures were 80% and 100% for 1-year survival rate and 20.4 and 18.5 months for overall survival. Kaplan–Meier curves are shown in Figure 5a and b and overall survivals of the groups are shown in Figure 6. The two groups did not differ with regard to mean survival regardless of the evaluation method, either scintigraphy or CT (p=0.102). This lack of any statistical difference may be explained by the low number of deaths in both groups. The difference with regard to the duration of survival was 6 months and 1.9 months between the two groups based on scintigraphy and CT assessments, respectively. Thus, demonstration of clinical response was possible with higher accuracy using 111In-octreotide scintigraphy performed 6 weeks after the treatment.

Kaplan–Meier curves for responders (CR or PR) and nonresponders (SD or PD). Treatment–response status was evaluated using 111In-octreotide scintigraphy findings in the upper survival curve
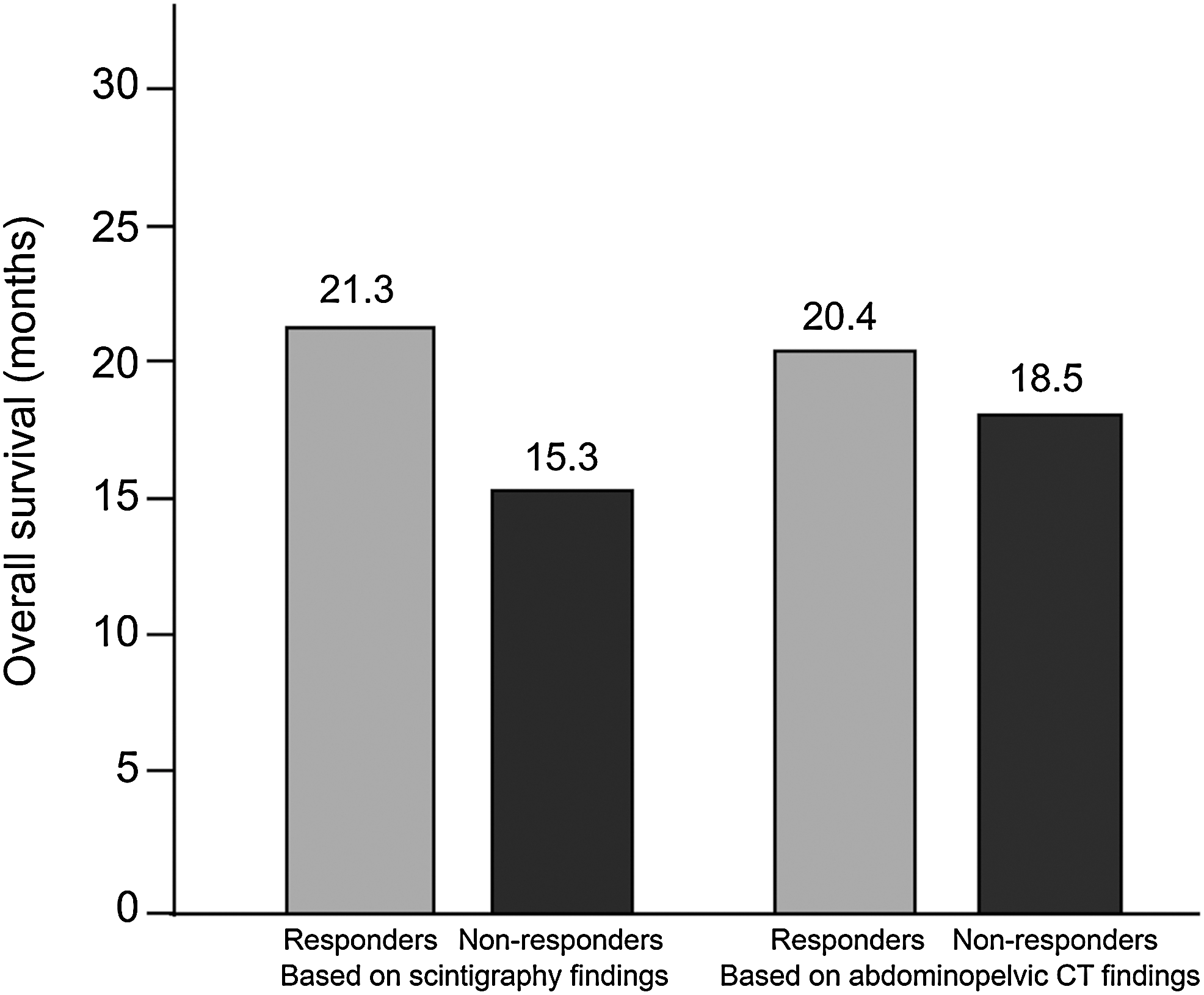
Overall survival data for responders (CR or PR) and nonresponders (SD or PD). Treatment–response status was evaluated either using 111In-octreotide scintigraphy findings or abdominopelvic CT findings, before and after treatment.
Discussion
Liver metastasis is frequent in NETs, particularly in those originating from the midgut. Peptides secreted from the liver metastases may result in carcinoid syndrome. The aim of the treatment is to control clinical symptoms of carcinoid syndrome as well as to decrease tumor size or prevent its progression. Although surgery definitely represents the ideal treatment modality, it is possible in only 10% of the cases. On the other hand, systemic chemotherapy provides limited benefit in carcinoid syndrome. 5 Hormone levels and symptoms can be safely controlled when Sandostatin LAR is used in addition to surgery in an attempt to manage carcinoid syndrome symptoms and tumor progression. 2 The use of other local palliative treatment modalities is considered when these efforts fail to prevent tumor progression. In such cases, specific treatment is planned according to the needs of individual patient and may aim to decrease tumor burden, hormonal palliation, or to render the tumor resectable. Depending on these clinical needs, TAE, TACE, or intra-arterial radionuclide treatment may be used. Radiofrequency ablation represents another local treatment option and, similar to surgery, can be used for oligonodular metastases (≤3 lesions) and small-sized lesions (diameter<3–5 cm), whereas transarterial treatments such as TAE, TACE, and radioactive microspheres are suitable for multinodular disease. 6,7
Previous studies reported post-treatment median survival rates ranging between 24 and 32 months with TAE and TACE treatments but in most of the patients the treatment was associated with postembolization syndrome or tumor lysis syndrome requiring prolonged hospitalization or resulting treatment-related death. 8,9 In this study, postembolization syndrome was tolerable not requiring prolonged hospitalization and no treatment-related death was observed. On the other hand, median survival was 18 months and shorter than those observed in previous studies. However, our patient groups were rather heterogeneous with regard to previous treatments, including patients not benefited from TACE previously. In another study examining the results of intra-arterial treatment with 90Y among 8 patients that had progressed following TAE treatment, 1 patient achieved PR, 4 had SD, and 3 had disease progression. 10 In the present study, although the sample size was small, among 3 patients that had received TAE or TACE, 2 achieved PR and 1 had SD, with no death or PD.
In the review by Madoff et al., meta-analysis of the treatment response rates for carcinoids tumors after TACE and TAE as evaluated by CT in a number of studies yielded complete and PR rates of 32% and 55%, respectively. 5 Similar to the results of that meta-analysis, our PR rate as evaluated by CT was 40%; however, this rate was 77% based on 111In-octreotide scintigraphy findings.
In this study, when all patients are considered, 1-year survival rate was 84.7% and overall survival was 20 months. Based on the findings of 111In-octreotide scintigraphy, 1-year survival rate and overall survival were as follows in the two groups: responders, 90% and 21.3 months; nonresponders, 66.7% and 15.3 months. Corresponding figures for CT assessments were as follows: responders, 80% and 20.4 months; nonresponders, 100% and 18.5 months. Although patients with SD and PD were included in nonresponders for both imaging methods, a 1-year survival rate of 100% was obtained according to CT findings, a finding that is not clinically relevant. Based on these results, overall survival difference between the two groups was 6 months with 111In-octreotide scintigraphy and 1.9 months with CT, suggesting that 111In 111-octreotide scintigraphy better differentiates responders than nonresponders. Previous studies have used dynamic and/or spiral CT, magnetic resonance imaging (MRI), or 111In-octreotide scintigraphy to evaluate treatment response and results obtained with radiological methods (e.g., CT or MRI) according to RECIST criteria are in line with our findings; however, the results of functional imaging methods were not separately analyzed in those studies. 11 –14 To the best of our knowledge, no study so far compared these methods in evaluating treatment response and this study is the first comparing CT and 111In-octreotide scintigraphy in the evaluation of treatment response to intra-arterial radionuclide treatment with 90Y. When compared with CT, 111In-octreotide scintigraphy provided accurate results in evaluating clinical response of the patients and it better discriminates patients responding to treatment from unresponsive patients.
This study has several limitations. First is the small sample size. Second, results of the tumor markers were not included since they had been examined in different centers. Finally, radiological imaging was done in different centers and some were only dynamic CT examinations.
In conclusion, intra-arterial treatment with 90Y has survival benefits in NET metastases to liver that are refractory to treatment and it could be used in these patients. Since it is a functional imaging method, 111In-octreotide scintigraphy may better discriminate patients responding to treatment from patients not responding.
Footnotes
Disclosure Statement
There is no conflict of interest.