
Abstract
Interleukin-2 (IL-2) was the preferred treatment for medically fit patients with advanced kidney cancer, but recently, several targeted therapies have been approved for metastatic renal cell carcinoma. We wished to determine the long-term survival rate for patients with kidney cancer treated with IL-2 and whether the use of intense inpatient IL-2 has declined since the introduction of targeted therapies. Patients who received IL-2 were identified from clinical trial enrollment, pharmacy logs, and financial billing records. Survival was determined from the earliest date of IL-2 therapy. There were 79 patients hospitalized for high-dose infusional IL-2 between March 1989 and March 2009. Median age was 58 years, and 27% were older than 65 years at the time of treatment. At the time of this analysis, 72 patients had deceased. Median survival was 9.9 months, but 5-year survival was 19.4%. The average number of patients with IL-2 increased from 2.2 per year during 1989–1992 to 5.6 during 1993–2001 after FDA approval, but dropped to 2.0 during 2002–2009. High-dose IL-2 is associated with a 5-year survival rate that is higher than objective response rates, suggesting a delayed immunotherapy benefit for some patients. The use of intensive IL-2 has declined dramatically in recent years, but unless a long-term survival benefit can be shown for these new targeted products, we feel that inpatient IL-2 remains the preferred initial treatment.
Introduction
Kidney cancer remains a significant medical problem with an estimated 58,240 new diagnoses in 2010 and 13,040 deaths, representing 3.8% of all newly diagnosed cancers and 2.3% of all cancer deaths. 1 Deaths occur because of metastatic disease, which is identified in about 10% of patients at diagnosis, but can appear any time subsequently. Nationally, the relative 5-year survival rate for all patients in whom kidney cancer was diagnosed during 1996–2004 was 67%, but for patients with distant disease, the relative 5-year survival rate was only 10%. 1 The treatment of metastatic kidney cancer continues to be unsatisfactory. Chemotherapy is generally considered to be ineffective in renal cell cancer. 2 Although the chemotherapy drugs 5-fluoruracil and vinblastine were often used in the treatment of metastatic renal cell cancer, there are no data to suggest that these agents increase long-term survival. No chemotherapy agents have been granted regulatory approval for the treatment of kidney cancer during the past two decades.
During 1987–2007, the biotherapy agents interferon-alpha (IFN-α) and interleukin-2 (IL-2) were considered the agents of choice for the treatment of metastatic kidney cancer, especially clear cell renal cell carcinoma, which accounts for about 75% of malignant kidney neoplasms. The strongest evidence for IFN-α came from two European randomized trials in which IFN-α was superior to medroxyprogesterone. 3,4 These trials confirmed a higher response rate and better survival for patients who received IFN-α, but neither report provided 5-year survival rates. Analysis of 463 patients enrolled in six different trials with single-agent IFN-α at Memorial Sloan Kettering revealed a median progression-free survival of 4.7 months and a median overall survival of 13 months. 5 The 5-year survival rate was estimated to be as high as 10%, but the median follow-up was less than 4 years for the 61 survivors.
The immune-stimulating cytokine IL-2 was approved in the United States in 1992 for the treatment of metastatic renal cell cancer based on a compilation of 255 patients enrolled in seven phase II trials that utilized high-dose bolus IL-2 therapy. 6 The report emphasized the long-term progression-free survival and overall survival of patients with a documented objective response, especially those whose disease went into complete remission. Numerous trials were conducted in which IFN-α and IL-2 were combined, but none of these regimens were ever shown to be superior to IL-2 alone. Randomized trials established that high-dose bolus IL-2 is superior to regimens utilizing lower doses administered as intravenous boluses or subcutaneously. 7,8 High-dose continuous infusion IL-2 was adopted as the preferred treatment for renal cell cancer in Europe. 9 In a U.S. randomized trial in which patients received lymphokine activated killer cells in both arms, there was no difference in response rates or survival between high-dose bolus and continuous infusion IL-2. 10 High-dose inpatient regimens of IL-2 were considered the standard treatment of choice for patients with metastatic renal cell cancer who were felt to be suitable medical candidates for such therapy. Unfortunately, both of these intensive IL-2 treatment regimens are associated with life-threatening toxicities; so, careful patient selection is important. Intensive IL-2 therapy is not a realistic treatment option for most patients. 11 Further, such treatment requires close monitoring in the inpatient hospital setting and medical management by physicians and nurses experienced in delivery of the therapy.
In the past decade, several new targeted agents have been approved for the treatment of metastatic renal cell cancer, including the antivascular endothelial growth factor monoclonal antibody bevacizumab in combination with IFN-α, 12,13 several tyrosine kinase inhibitors (sorafenib, sunitinib, and pazopanib) that inhibit the signal transduction that results from activation of vascular endothelial growth factor-receptors, 14 –16 and temsirolimus and everolimus, which inhibit the mammalian target of rapamycin kinase. 17,18 Although the long-term survival benefits of these agents have not yet been established, they have been enthusiastically adopted by the medical oncology community because of their high-response rates and a better-tolerated and more easily managed tolerable toxicity profile compared with IL-2. Because of the recent introduction of these agents, we wished to examine the use of inpatient IL-2 over time in a community hospital setting and determine the long-term survival of patients who were thus treated. Our hypothesis was that more than 10% of these patients would survive at least 5 years based on concepts of a delayed immunotherapy benefit that would not necessarily be associated with an objective response.
Materials and Methods
A retrospective analysis was performed to determine the long-term survival of patients with metastatic renal cell carcinoma who were accessioned to the cancer registry of a large community hospital. Patients who had received inpatient IL-2 were identified from clinical trial logs, pharmacy logs, and financial billing codes. The year in which inpatient IL-2 therapy was initiated was noted for each patient. Observed and relative survival were calculated from the date of original diagnosis and from the date of initiation of inpatient IL-2 therapy using data retained in the local cancer registry using computer software designed for registry reporting (Electronic Registry Systems, Inc., Cincinnati, OH).
Results
Seventy-nine patients were identified who were hospitalized for intensive IL-2 infusional therapy between March 1989 and March 2009. There were 54 men and 25 women; 76 were Caucasian, and 3 were Asian. Median age was 55 years at the time of original diagnosis and 58 at the time of IL-2 therapy. Age at the time of IL-2 therapy ranged from 17 to 76 years, with 21 patients 65 years or older. At the time of original diagnosis, 10 had local disease; 11, regional extension; 7, lymph node involvement; 43, distant metastases; and 8, unknown stage. All had distant metastatic disease at the time IL-2 therapy was initiated.
Distribution by year in which IL-2 therapy was initiated is shown in Figure 1. There was a sharp increase in the numbers of patients receiving IL-2 after FDA approval in May 1992, and a dramatic decline in the use of IL-2 as the tyrosine kinase inhibitors sorafenib and sunitinib became available in clinical trials in 2002 and 2003 before their receiving regulatory approval in December 2005 and January 2006. Only 1 patient received inpatient IL-2 during 2008 and 2009. During 1989–1992, 9 patients were treated as part of IL-2 clinical trials, an average of 2.2 per year. After approval of IL-2, 56 patients were treated during 1993–2001, an average of 5.6 per year. After sorafinib and sunitinib had been introduced in 2002 and 2003, only 14 patients were treated during 2003–2009, an average of less than 2.0 per year.
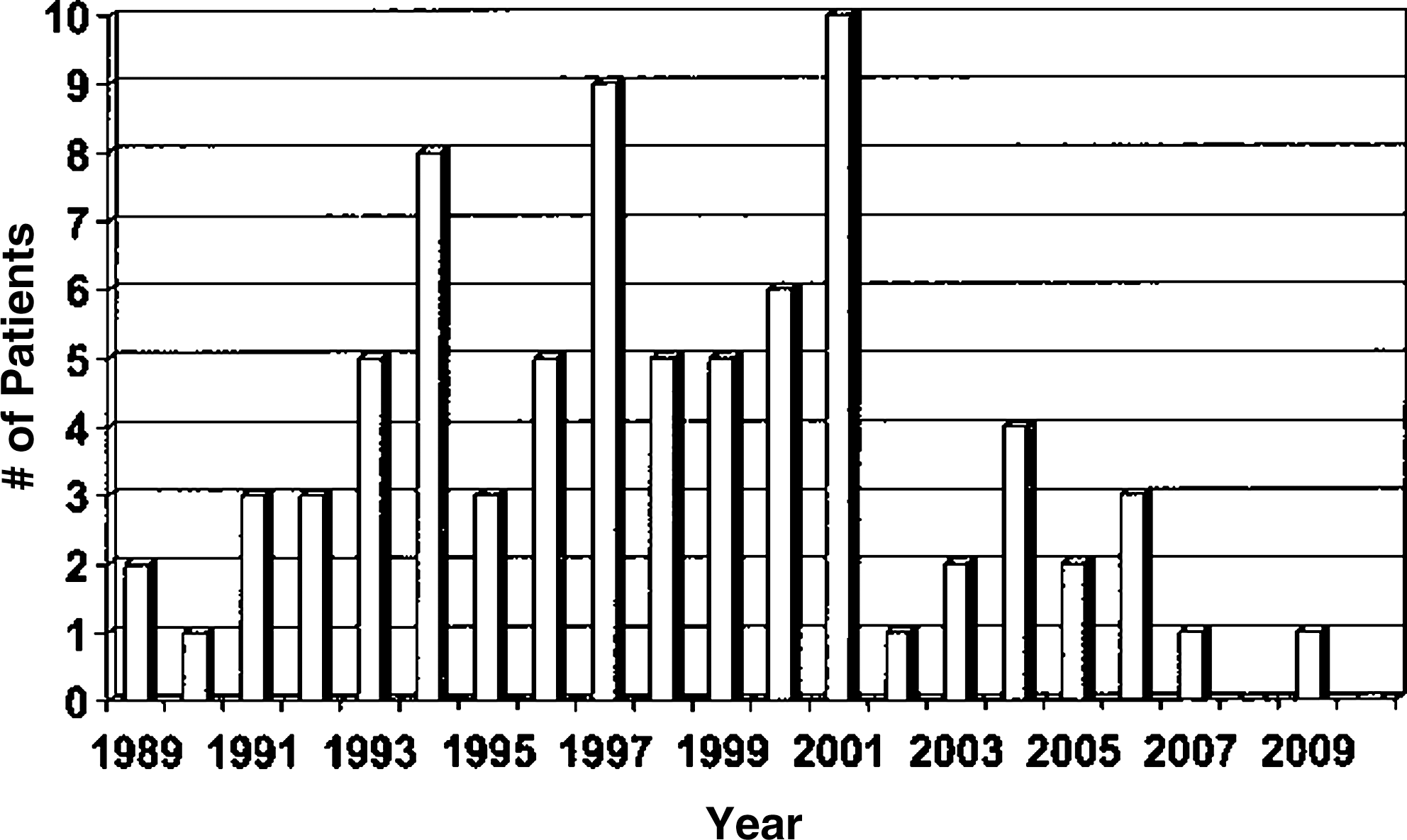
Distribution of patients with metastatic renal cell cancer treated with inpatient, i.v. IL-2.year. IL, interleukin; i.v., intravenous.
The survival curve from the date of initiating intravenous IL-2-based therapy is shown in Figure 2. Follow-up was excellent with no patients lost to follow-up, and only 2 patients censored because of short follow-up after treatment. There were 72 patients who were deceased, and 7 were censored alive 2, 4, 6, 9, 14, 15, and 16 years after initiating IL-2 therapy. From the date of IL-2 therapy, the median survival for all 79 patients was 9.9 months, but the 5-year survival was 19%. Since this was not a prospective study, there were no reliable response rate data to correlate with survival and limited prognostic information for individual patients. However, 26 of these patients did participate in national IL-2-based clinical trials of the Cancer Biotherapy Research Group, in which only 19/225 (8.4%) had an objective response to high-dose infusional IL-2. 19 –21 From the date of original diagnosis, median survival for all patients collectively was almost 3 years, and the 5-year survival rate was 37%. Fifteen patients survived more than 5 years after a diagnosis of metastatic disease. For the 43 patients who had distant disease at diagnosis, the median survival was 16 months, and the 5-year survival rate was 22%.
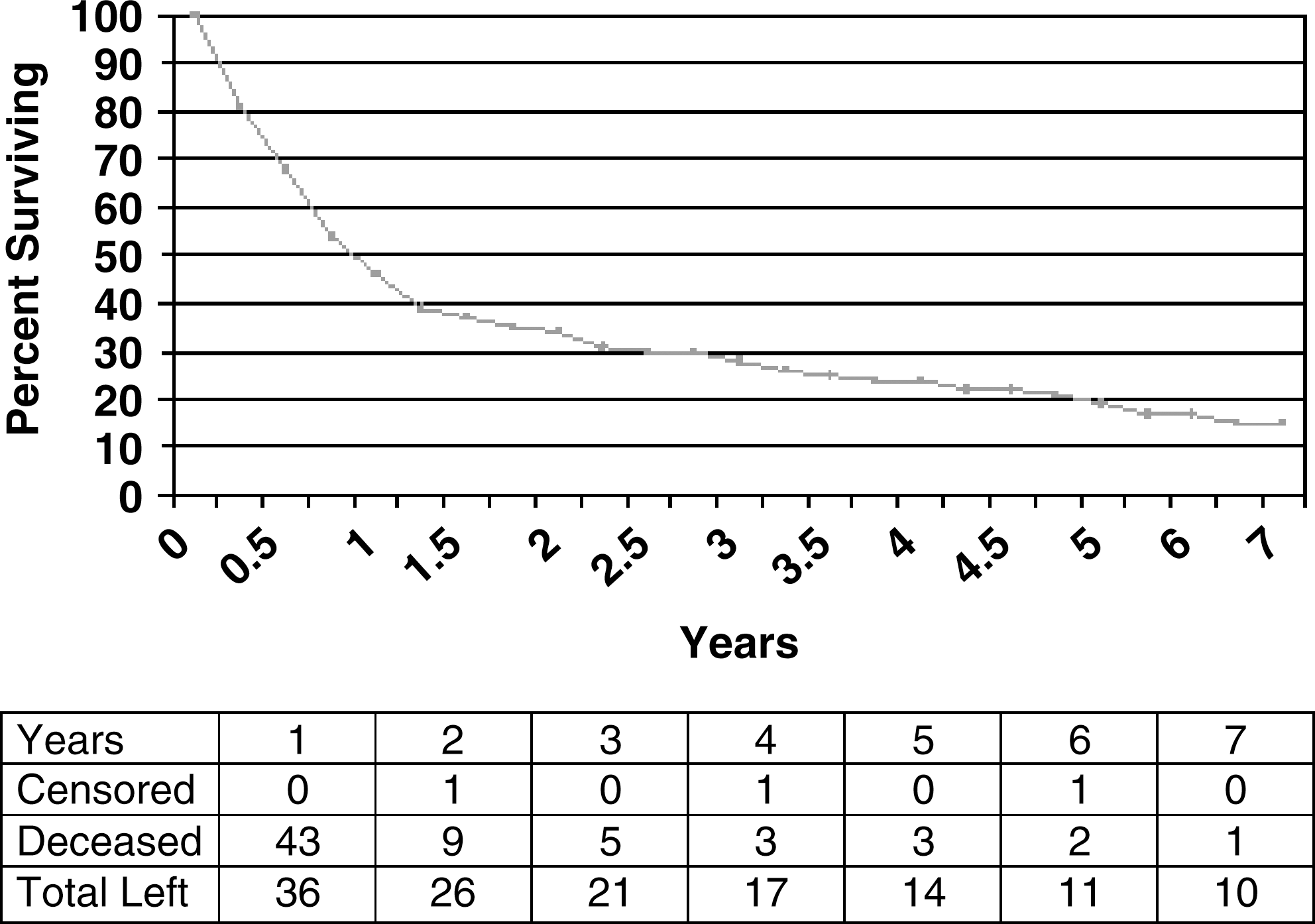
Survival of patients with metastatic renal cell cancer from initiation of intravenous IL-2-based therapy.
Discussion
In this article, we describe the marked decline in the use of inpatient IL-2 therapy for kidney cancer after the introduction of sorafinib and sunitinib and report a 5-year survival rate of about 20% for patients with metastatic kidney cancer who were treated with high-dose infusions of IL-2. As shown in Figure 1, the numbers of patients who had been treated with intensive IL-2 in this community hospital setting increased dramatically after the regulatory approval of IL-2 in 1992, but decreased markedly after the introduction of sorafinib and sunitinib. Due to the toxicity and cost of inpatient IL-2 therapy, there was intensive investigation of various lower dose regimens that could be administered in an outpatient setting. For this reason, even in the years after regulatory approval, many patients with kidney cancer received lower doses of IL-2 as part of outpatient biochemotherapy regimens with 5-FU. 22 Otherwise, the numbers of patients receiving intensive IL-2 during 1993–2002 would have been even greater.
Despite the popularity of several new agents that have been added to the therapeutic armamentarium against renal cell cancer, it is unclear whether treatment with these products is associated with long-term survival benefit. In contrast, treatment with high-dose IL-2 has been shown to be associated with long-term survival and apparent cure in some patients. Earlier reports established that patients with metastatic renal cell cancer who experienced an objective response while enrolled in clinical trials, especially a complete response, had a better survival than patients who did not. 6,23 However, the benefit for patients who did not exhibit an objective response is less clear. In a European study of 281 patients treated with IL-2 alone, median survival was 10 months and only 8% survived 5 years. 24 The objective response rate was 15%; the 5-year survival rates were 60% for complete responders and 18% for partial responders. Longer follow-up of the 255 patients who were the basis of the FDA approval of IL-2 suggested a median survival of 16.3 months and a 5-year survival rate of about 18%. 25
A recent update from the NCI surgical branch again emphasized the association between an objective tumor response and long-term survival in patients with kidney cancer who received high-dose bolus IL-2. 26 Among 259 patients, there were 23 complete responders (9%) and 30 partial responders (12%). Survival was clearly better for the complete responders for whom median survival had still not been reached with median follow-up of more than 10 years. For patients with a partial response, the median survival was 3.3 years, compared with only 1.3 years for nonresponders. The last group included patients classified as having stable disease, and those who had progressive disease at the time of response assessment, but there were no specific data provided for each of these subsets. The median survival for all 259 patients was 19 months, but the 5-year survival rate for all patients was not provided. The median survival of the nonresponders in the NCI series was more than a year, but their 5-year survival was only about 5%. In our cohort of 79 patients, the median survival was only 9.9 months, which is similar to the large European experience. 24
It is increasingly apparent that immunotherapy initially can be associated with stable disease or even some disease progression, but followed by delayed tumor response and survival benefit. This was a major issue in the delayed approval for the anticytotoxic T-lymphocyte antigen-4 monoclonal antibody ipilumumab for melanoma, 27 and the immune cell therapy sipileucel T for prostate cancer. 28 With both of these products, response rates and progression-free survival were unimpressive, but long-term survival benefit was clearly documented in randomized prospective trials. This has led to formulation of newly proposed criteria for determining the efficacy of such products, as benefit is not limited to objective responders. 29
Most reports of IL-2 therapy have emphasized the association between objective response rate and long-term survival and suggested that there was no benefit for nonresponders. It is clear for both high-dose bolus IL-2 and high-dose continuous infusion IL-2 that patients who achieve a complete response do better than those who achieve a partial response, who, in turn, do better than patients who do not have an objective response, which includes patients who are considered to have stable disease, or progressive disease. 23 –25 However, it was previously noted that more than 20% of patients with metastatic renal cell cancer treated on IL-2-based clinical trials survived more than 3 years after initiation of treatment, despite low objective response rates, and of those 14 survivors, 10 had stable disease as their best response to IL-2. 23 The present retrospective study, which includes patients enrolled in clinical trials and patients treated outside of the clinical trial setting after regulatory approval of IL-2, demonstrates that 19% of such patients survive more than 5 years.
Conclusions
Should high-dose IL-2 still be the preferred treatment for patients with metastatic renal cell cancer? Based on the above, we feel that clinicians should continue to consider IL-2 as the initial therapy in any patients with metastatic clear cell renal cell cancer who are medically fit for such therapy. The limitation to this histology is based on analyses suggesting that nonclear cell and papillary kidney cancer do not benefit from IL-2 therapy. 30 If other therapies are used first, patients who were potential candidates for IL-2 may deteriorate because of progressive disease or complications of these other therapies and may no longer be suitable for IL-2. For example, cardiac toxicity is a known risk of antiangiogenesis therapy, 31 and there is at least one report which suggests that patients who receive high-dose bolus IL-2 after previous treatment with sorafinib, sunitinib, or bevacizumab may have an unacceptably high rate of cardiac complications during subsequent IL-2 treatment. 32
Footnotes
Acknowledgments
We wish to thank Stacy Wilton, Michelle Hoffpauer, Carol DePriest, and Pete Vanderplas for their assistance in identifying all patients who had received inpatient IL-2.
Disclosure Statement
The authors declare that they have no proprietary, financial, professional, or other personal interest in any product, service, and/or company that could be construed as influencing the position presented in this article.