
Abstract
The overexpression of the epidermal growth factor receptor (EGFR) in head and neck squamous cell carcinoma (HNSCC) is associated with poor prognosis. Targeted nuclear imaging of the EGFR expression could improve the diagnostics in patients with HNSCC. However, the high expression of EGFR in normal organs may conceal the tumor uptake and therefore limit the use. This study assesses the biodistribution of a novel human epidermal growth factor (hEGF) radionuclide conjugate after preinjection with anti-EGFR affibody molecules. hEGF was conjugated with p-SCN-Bn-NOTA and labeled with 67Ga. The biodistribution of [67Ga]Ga-NOTA-Bn-NCS-hEGF in nude mice with EGFR-expressing xenografts was evaluated either alone or 45 minutes after preinjection with one of the anti-EGFR affibody molecules ZEGFR:1907, (ZEGFR:1907)2, or (ZEGFR:955)2. The novel radioimmunoconjugate, [67Ga]Ga-NOTA-Bn-NCS-hEGF, demonstrated high stability in vitro and specific binding to hEGF in vitro and in vivo. Preinjection with anti-EGFR affibody molecules improved the tumor-to-organ ratio in the liver, salivary glands, and colon. Overall, the dimeric high-affinity affibody molecule (ZEGFR:1907)2 exhibited the best results. These findings show that preblocking with an anti-EGFR affibody molecule is a promising tool that could improve the outcome of radionuclide-based imaging of EGFR-expressing tumors.
Introduction
The epidermal growth factor receptor (EGFR, also known as HER1 and ErbB-1) is a transmembrane protein with tyrosine kinase activity that regulates essential cellular functions, such as cell proliferation, motility, survival, and differentiation. Enhanced signaling of EGFR is common in many malignancies including head and neck squamous cell carcinomas (HNSCCs).
The enhanced EGFR signaling in HNSCC is due to overexpression of EGFR, as EGFR mRNA is overexpressed in up to 90% of cancer cells and is also common in metastases originating from HNSCC. 1,2 Mutations of the EGFR kinase in head and neck cancer are rare. 3,4 Detecting overexpression of EGFR, evaluated in tumor biopsies, is a way of predicting the prognosis and choosing specific therapy for a particular HNSCC patient, because a high level of EGFR is associated with a faster tumor progression and early metastases. 5 –8 As an example, EGFR expression of an HNSCC tumor can be used to predict local-regional relapse after radiotherapy 9 and to select patients who might benefit from accelerated radiotherapy. 10,11
When comparing different methods of EGFR detection, targeted radionuclide imaging is probably advantageous over biopsy analyses, as it is a noninvasive, sensitive technique with fewer false-negative results. Such errors are commonly caused by biopsy sampling error or discordance with EGFR expression in primary tumors and metastases. Targeted nuclear imaging of the EGFR family receptors may also improve the diagnostics as shown in a recent human breast cancer study with 68Ga-labeled anti-HER2 affibody molecules. 12
A targeting imaging agent should have certain features for successful imaging: it should find its target rapidly, bind with high specificity, and internalize to a high extent, especially if labeled with metals. The unbound fraction should also be rapidly cleared from the blood and healthy tissue and excreted, to provide high tumor-to-organ uptake ratio and contrast. One important factor is the molecular size of an imaging agent, because it is a factor that influences its extravasation, diffusion in intercellular space, tumor uptake, and distribution rate. One of the natural ligands of EGFR, the human epidermal growth factor (hEGF), with a molecular weight of 6.2 kDa, has been previously evaluated as a targeting agent for imaging of EGFR overexpression and demonstrated to have desirable pharmacokinetics. 13 –15
There are concerns regarding conventional EGFR targeting. EGFR is naturally expressed in normal organs such as the liver, skin, and GI tract and is therefore not limited to tumor cells. Even more crucial and problematic for imaging of head and neck cancers is the physiological uptake in the thyroid, salivary glands, and oral mucosa, because it may mask the signal from the lesions in the head and neck area. It has been previously suggested and demonstrated that the relative uptake in the healthy organs and lesions can be modulated. By variation of the administered ligand amount, the tumor-to-organ ratios can be improved, most probably because of receptor saturation in the healthy organs. 15,16 –18
An earlier work has assessed a method for EGFR targeting with improved tumor selectivity compared with standard EGFR targeting. Preinjection of hEGF or the anti-EGFR affibody molecule (ZEGFR:955)2 in nude mice with EGFR-expressing xenografts reduced the liver uptake of subsequently injected hEGF, compared with hEGF injection without preinjected hEGF or anti-EGFR affibody molecule. Thus, the tumor-to-liver ratio was improved. 19 These data are in agreement with earlier results of Tolmachev and coworkers, who showed a significant decrease of 111In-DTPA-hEGF uptake in the EGFR-expressing organs such as the liver, spleen, pancreas, intestines, and submaxillary salivary glands with preinjection of unlabeled hEGF. 20 Further, Hu and coworkers 18 have shown that decrease of 111In-DTPA-hEGF uptake in the EGFR-expressing organs after preinjection of nonlabeled hEGF is accompanied by increased radioactivity uptake in the EGFR-expressing tumor xenografts.
Affibody molecules (Affibody AB) are small (monomeric form ∼7 kDa), high-affinity proteins based on a scaffold derived from a mutated form of the B-domain of staphylococcal protein A. 21,22 Both monomeric and dimeric forms of affibody molecules have been successfully used for visualization of EGFR-expressing xenografts in vivo. 23,24
Both hEGF and affibody molecule imaging agents have been labeled with gamma- and positron-emitting metal radionuclides for SPECT and PET imaging. 15,25 Compared with SPECT, PET offers advantages in sensitivity, spatial resolution, and quantification. Among the positron-emitting radionuclides, 68Ga (89% β+) has a half-life (68 minutes) that is in good agreement with the kinetics of elimination from the blood and accumulation in tumors of hEGF. It gives high-quality images and allows for sequential examinations during the same day, e.g., for determination of receptor expression. Also, as it is generator produced (68Ge/68Ga; T 1/2(68Ge)=270.95 days), it is easily available. 26 The hEGF-based reporter molecule used in this work comprised a gamma-emitting radiometal, 67Ga (T 1/2=3.26 days), as a surrogate of 68Ga. A bifunctional chelator, p-SCN-Bn-NOTA, was employed for the conjugation with hEGF and subsequent complexation with 67Ga at room temperature, providing the possibility for a kit type of radiopharmaceutical production under mild reaction condition. 27
Herein, the selective blocking effect of three anti-EGFR affibody molecules of different forms and affinities—(ZEGFR:955)2 (K D: 50 nM), 28 ZEGFR:1907 (K D: 2.8 nM), and (ZEGFR:1907)2 (KD: 1.6 nM) 24 —was evaluated in nude mice with EGFR-expressing, UT-SCC7, xenografts. The studied affibody molecules bind to both human and mouse EGFR. 29 In vitro studies 29 have shown that (ZEGFR:955)2 affibody molecule can inhibit binding of 125I-EGF to EGFR-expressing cell lines, and EGFR can inhibit binding of 125I-(ZEGFR:955)2. This is a strong indication of sufficient overlapping of their binding sites. However, the exact epitopes for each ligand are not known. In a previous study, the biodistribution of ZEGFR:1907 and (ZEGFR:1907)2 was evaluated in EGFR-expressing A431 tumor xenografts. The uptake in both high EGFR-expressing organs such as the liver, spleen, and colon and in low EGFR-expressing organs such as the muscle and bone was higher for (ZEGFR:1907)2. 24 It is therefore hypothesized that (ZEGFR:1907)2 as a preinjected blocker would give lower uptake of subsequently injected [67Ga]Ga-NOTA-Bn-NCS-hEGF in the liver, tongue, and salivary glands and hence better tumor-to-organ ratios than the ZEGFR:1907. The (ZEGFR:955)2 with an equal size to (ZEGFR:1907)2 but lower affinity than both (ZEGFR:1907)2 and ZEGFR:1907 was included to clarify the effect of size and affinity on the biodistribution.
Methods
Labeling materials
Recombinant hEGF was purchased from Millipore (GF144). HEPES (4-(2-Hydroxyethyl) piperazine-1-ethanesulfonic acid), double-distilled hydrochloric acid (Riedel de Haën), sodium hydroxide (semiconductor grade), and gallium chloride (crystalline solid, 254193) were obtained from Sigma-Aldrich. The S-2-(4-isothiocyanatobenzyl)-1,4,7-triazacyclononane-1,4,7-triacetic acid (p-SCN-Bn-NOTA) was purchased from Macrocyclics. 67Ga (50 mCi) was obtained from MDS Nordion, Inc., in 0.1 M HCl solution of 106 μL. Sodium dihydrogen phosphate, disodium hydrogen phosphate, and trifluoroacetic acid (TFA) were obtained from Merck. The purchased chemicals were used without further purification. Deionized water (18.2 MΩ), produced with a Purelab Maxima Elga system, was used in all reactions.
Conjugation of p-SCN-Bn-NOTA to hEGF
hEGF (70 nanomoles) in 800 μL of borate buffer (0.066 M, pH 9.4) was added to dry p-SCN-Bn-NOTA (10–20-fold excess over hEGF) under stirring, and the pH was further adjusted to 9.0 (Fig. 1). The mixture was left at room temperature for 3–4 hours or overnight at 4°C. The conjugate was purified and concentrated using Microcon centrifugal filters (YM-3; Millipore) against deionized water and the purified product was stored at −25°C. The filtration fractions were analyzed by RP-HPLC to control the conjugate breakthrough and recovery. The product was not detected in the filtrate and the recovery was over 95%.

Scheme of p-SCN-Bn-NOTA coupling to EGF. EGF, epidermal growth factor.
Preparation of [67Ga]Ga-NOTA-Bn-NCS-hEGF
A variable amount of 67Ga (7–28 MBq) dependent of the required specific radioactivity was added to the HEPES solution (0.3 M, 200 μL) in 0.1 M HCl. The pH of the solution was adjusted with NaOH to 3.5–4.5 if needed.
Then, 5–15 nanomoles of NOTA-Bn-NCS-hEGF was added and the reaction mixture was incubated either at room temperature for 10 minutes or at 90°C for 5 minutes. The radiochemical purity of [67Ga]Ga-NOTA-Bn-NCS-hEGF was assessed by UV- and radio-HPLC, and the concentration of the conjugate and the tracer was determined from UV-HPLC standard plots. To verify that the binding of 67Ga to hEGF was NOTA mediated, a control experiment was performed. The procedures were the same as described earlier, but nonconjugated hEGF was used. The stability of [67Ga]Ga-NOTA-Bn-NCS-hEGF in buffer was monitored by UV-HPLC for 17 hours.
Synthesis of NatGa-NOTA-Bn-NCS-hEGF
NatGa of natural isotope composition was complexed with NOTA-Bn-NCS-hEGF. Twenty (20) millimolar aqueous solution of NatGaCl3 (5 μL) was added to the HEPES solution (0.3 M) of 0.1 M HCl (200 μL) and the pH was adjusted with NaOH to 3.5–4.5. Then, 10 nanomoles of NOTA-Bn-NCS-hEGF was added and the reaction mixture was incubated at room temperature for 10 minutes or at 90°C for 5 minutes. NatGa-NOTA-Bn-NCS-hEGF was used as an authentic reference for the confirmation of the UV-HPLC chromatogram signals.
HPLC analysis
Analytical liquid chromatography was performed using an HPLC system from Beckman consisting of a 126 pump, a 166 UV detector, and a flow count radiation detector (Bioscan, Inc.) coupled in series. Data acquisition and handling were performed using the Beckman System Gold Nouveau Chromatography Software Package. Separation was conducted using a Vydac RP 300 Å HPLC column (150 mm, 4.6 mm, 5 μm particle size; Vydac). The applied gradient elution had the following parameters: A=10 mM TFA, B=70% acetonitrile (MeCN), 30% H2O, 10 mM TFA with UV detection at 280 nm (flow rate was 1.0 mL/min) for 0–2 minutes isocratic 20% B, 20%–90% B linear gradient 8 minutes, and 90%–20% B linear gradient 2 minutes. The recovery of the radioactivity from the HPLC column associated with [67Ga]Ga-NOTA-Bn-NCS-hEGF and radioactive impurities were controlled. Retention times for the UV- and radio-signals of the tracer were 7.94±0.04 and 8.13±0.05 minutes, respectively.
Instant thin-layer chromatography
For additional determination of purity and stability of the 67Ga-labeled EGF, instant thin-layer chromatography (ITLC) was performed 24 hours after the labeling procedure. One (1) drop (approximately 10 μL) of the conjugate solution was placed on a chromatography strip (Biodex) and developed in 0.2 M Na-acetate (pH 5.5), followed by analysis with a phosphor imager (Cyclone Storage Phosphor System) and analyzed using the OptiQuant image analysis software.
Tumor cells
The EGFR-expressing head and neck squamous cell line UT-SCC7 was used (kindly provided by Dr. R. Grenman, Turku University Central Hospital, Finland). The mean density of EGFRs (±standard error of the mean) has been determined to be 0.5×106±0.02×106 per cell in a previous study.
19
UTSCC-7 cells were grown in a humidified incubator with 5% CO2 at 37°C in DMEM medium (Biocrom Kg), complemented with 10% fetal bovine serum (Sigma Aldrich), 1%
Specificity and antigen presence
UTSCC-7 cells were seeded in plates with 48 wells and were allowed to grow until 80% confluence under optimal growth conditions. To verify the specificity of binding, a blocking solution with 100 times higher concentration of nonlabeled human EGF (Millipore) was added together with 50 ng/ml [67Ga]Ga-NOTA-Bn-NCS-hEGF in complete cell medium to saturate the receptors. The wells were divided into two groups: in the first group of wells, the blocking solution of nonlabeled human EGF was added at the same time as [67Ga]Ga-NOTA-Bn-NCS-hEGF. The second group of wells received nonlabeled human EGF both 15 minutes before and at the same time as the [67Ga]Ga-NOTA-Bn-NCS-hEGF. The wells were incubated for 1 hour at 37°C in humidified conditions. The medium was removed and UTSCC-7 cells were washed six times with serum-free medium and then trypsinized with trypsin–EDTA solution (Biocrom Kg). The cells were counted with a cell counter and the radioactivity of the media and the cells was measured with a gamma counter. The fraction of cell-bound radioactivity was then calculated.
Biodistribution in tumor-bearing mice
Xenografts were formed by subcutaneous inoculation of 12×106 UTSCC-7 cells in 300 μL medium in the right posterior leg in 20 nude balb/c (nu/nu) female mice. The tumors were allowed to grow for 19 days. The mice were housed in a controlled environment and fed ad libitum.
At the time of the biodistribution experiment, the average mouse size was 18.3 g (standard deviation [SD]: 1.2) and the average tumor size was 0.3 g (SD: 0.22). Tumor uptake was 100%. There was no difference in mouse or tumor weight between the groups.
The mice were divided into four groups with five animals in each. Group 1 (control) received intravenous injection (i.v.) via the tail vein with 1 μg (1.6 nM) [67Ga]Ga-NOTA-Bn-NCS-hEGF in 100 μL phosphate-buffered saline (PBS) (53 kBq). The other three groups initially received anti-EGFR affibody molecules of equimolar amount subcutaneously at the back, between the forelegs. Forty-five (45) minutes later they received i.v. injection of 1 μg (1.6 nM) [67Ga]Ga-NOTA-Bn-NCS-hEGF in 100 μL PBS.
Group 2: 25 μg (ZEGFR:1907)2–1 μg (1.6 nM) [67Ga]Ga-NOTA-Bn-NCS-hEGF (52 kBq).
Group 3: 50 μg (ZEGFR:1907)2–1 μg (1.6 nM) [67Ga]Ga-NOTA-Bn-NCS-hEGF (56 kBq).
Group 4: 50 μg (ZEGFR:955)2–1 μg (1.6 nM) [67Ga]Ga-NOTA-Bn-NCS-hEGF (52 kBq).
One (1) hour after the [67Ga]Ga-NOTA-Bn-NCS-hEGF injection, the mice were euthanized with an overdose of a mixture of ketamine and xylazine given by intraperitoneal injection followed by exsanguination via heart puncture. The tumor, blood, liver, spleen, kidneys, submaxillary salivary glands, tongue, femur bone (including bone marrow), skin, and a small portion of colon (without feces) were excised and weighed. The radioactivity content was measured in a gamma counter (1480 WIZARD, Wallace Oy). The remaining GI tract with content, tail, and the carcass radioactivity was also measured. In the carcass, the urinary bladder was emptied of urine before measurements. Note that the uptake in colon should represent radioactivity accumulation in intestine walls, and uptake in the rest of GI tract with content should represent radioactivity accumulated in the intestines wall and radioactivity excreted via the bile.
For each group of animals, three injection standards of 100 μL [67Ga]Ga-NOTA-Bn-NCS-hEGF (volume of injection) were measured for radioactivity and a mean injected dose was calculated. The injected activity of [67Ga]Ga-NOTA-Bn-NCS-hEGF for each mouse was calculated using the following formula: Injection standard−Residual activity in the syringe−Activity in tail. Radioactivity uptake in the organs was calculated as percentage of injected activity per gram of tissue (%ID/g). For the GI tract and carcass, the uptake was calculated as percentage of injected activity per organ. The tumor-to-organ ratio was calculated as activity/gtumor divided by activity/gorgan.
The experiments complied with current Swedish law and were performed with permission granted by the Uppsala Committee of Animal Research Ethics.
Statistical analysis
Statistical analyses were performed using GraphPad Prism Version 5.02 for Windows (Graphpad Software; Tumor Biol, Inc.;
In the biodistribution studies, data are presented as the mean±SD. The significance of differences between groups was tested with one-way analysis of variance with Tukey's multiple comparison test. Difference were considered statistically significant if p<0.05.
Results
Synthesis of [67Ga]Ga-NOTA-Bn-NCS-hEGF
The synthesis of [67Ga]Ga-NOTA-Bn-NCS-hEGF was a two-step procedure, in which hEGF was first conjugated to a bifunctional chelator, p-SCN-Bn-NOTA, resulting in nearly quantitative bioconjugate formation via an isothiourea bond (Fig 1). The efficiency of the subsequent labeling of NOTA-Bn-NCS-hEGF with 67Ga at room temperature was concentration dependent, increasing from 94% to >99% when using 5 and 10–15 nanomoles, respectively, of the bioconjugate. Purification of the resulting [67Ga]Ga-NOTA-Bn-NCS-hEGF was not required, because the radioactivity incorporation was over 95% and the reaction buffer (HEPES) was compatible with biological systems.
The amount of 67Ga used in the labeling reactions was defined by the product-specific radioactivity determined by the biological experiment design. It was well below (3–10 picomoles) the amount (200 picomoles) when the concentration of the other metal impurities start interfering and deteriorating the labeling complexation reaction. 30 The specific radioactivity was 0.33±0.01 and 5.5±0.01 MBq/nmol, respectively, for animal and cell studies.
The binding of 67Ga to hEGF was proven to be NOTA mediated by performing a control experiment in which the original hEGF was used instead of NOTA-Bn-NCS-hEGF. The reaction mixture content was monitored by UV-Radio-HPLC, and no radioproduct co-eluting with the references such as hEGF, NOTA-Bn-NCS-hEGF, or NatGa-NOTA-Bn-NCS-hEGF could be detected, thus confirming that the hEGF itself does not bind 67Ga. [67Ga]Ga-NOTA-Bn-NCS-hEGF demonstrated high stability in buffer for at least 17 hours with constant radiochemical purity (>95%) as determined by Radio-HPLC (Fig. 2). The outcome was also confirmed with ITLC at 24 hours after labeling (data not shown). Previously, the stability of Ga-NOTA complex against the trans-chelation of the radiometal to plasma proteins was tested in human plasma and it was found stable for at least 4.5 hours at 37°C. 27
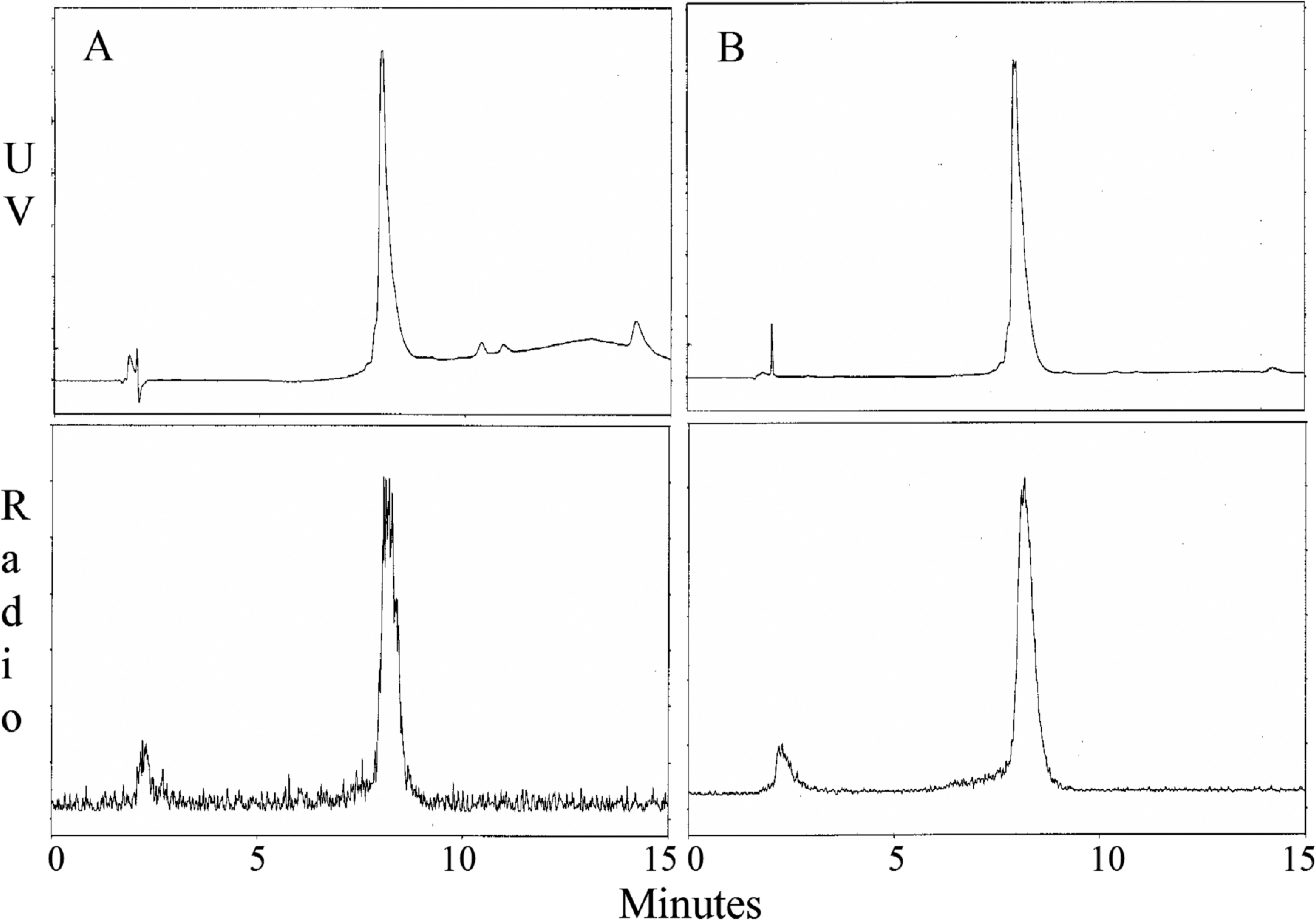
UV-Radio-HPLC analysis chromatograms of [67Ga]Ga-NOTA-Bn-NCS-hEGF immediately after the synthesis
Specificity and antigen presence
The results from the cellular binding study are displayed in Figure 3. A specific binding of [67Ga]Ga-NOTA-Bn-NCS-hEGF to UTSCC-7 cells was clearly demonstrated, as unlabeled hEGF blocked the binding of radiolabeled hEGF. By also adding the blocking solution 15 minutes before [67Ga]Ga-NOTA-Bn-NCS-hEGF, the binding of radiolabeled hEGF was further reduced.

Cellular binding assay of [67Ga]Ga-NOTA-Bn-NCS-hEGF on UTSCC-7 cells. The blocking solution of nonlabeled human EGF (Millipore) was added 15 minutes before and at the same time (3+3 μg block), or at the same time (3 μg block) as 30 ng [67Ga]Ga-NOTA-Bn-NCS-hEGF to saturate the receptors. CPM=counts per minute. Error bars represent the standard deviation. Control, n=6; 3+3 μg block, n=3; 3 μg block, n=3.
Biodistribution in tumor-bearing mice
The biodistribution data of [67Ga]Ga-NOTA-Bn-NCS-hEGF uptake and the result of the statistical analysis are presented in Figure 4. Generally, all three affibody molecules were able to reduce the [67Ga]Ga-NOTA-Bn-NCS-hEGF uptake in EGFR-expressing organs without reducing the hEGF tumor uptake.

Biodistribution of [67Ga]Ga-NOTA-Bn-NCS-hEGF in tumors and organs of UTSCC-7 xenograft-bearing nude mice. [67Ga]Ga-NOTA-Bn-NCS-hEGF was injected i.v. either alone (Control) or 45 minutes after s.c. injection of indicated affibody molecules. Data are expressed as percentages of injected activity per gram of tissue (ID/g%), except for the GI tract, which is expressed as percentages of injected activity per organ. Asterisk (*) indicate significant difference compared with the control group. Error bars represent the standard deviation. N=5. i.v., intravenously; s.c., subcutaneously.
The hEGF uptake in the liver and salivary glands was lower in all the blocking groups. In the liver, (ZEGFR:1907)2 gave the lowest hEGF uptake. In the salivary glands the monomeric and dimeric forms of ZEGFR:1907 showed a trend, although not significant, toward higher blocking capacity than (ZEGFR:955)2. The uptake in the GI tract was lower in all blocking groups, whereas in the colon only ZEGFR:1907 resulted in a lower uptake. Tongue uptake, however, showed no difference from control, although there was a trend toward a lower uptake with all three blocking affibody molecules.
The uptake of [67Ga]Ga-NOTA-Bn-NCS-hEGF in blood and tumor did not differ between the control group and the affibody molecule blocking groups. A trend toward higher [67Ga]Ga-NOTA-Bn-NCS-hEGF uptake in tumor compared with control could also be observed for all three blocking groups; however, it was not statistically significant.
In the kidneys, (ZEGFR:1907)2 gave a higher hEGF uptake compared with both control and ZEGFR:1907. In the bone, ZEGFR:1907 and (ZEGFR:955)2 resulted in lower uptake of [67Ga]Ga-NOTA-Bn-NCS-hEGF. For the spleen and skin, there were no differences between the groups.
The tumor-to-organ ratios and the results of the statistical analysis are presented in Figure 5. In the salivary glands, there were higher ratios for all affibody molecule blocking groups compared with control. The highest tumor-to-organ ratio was obtained by (ZEGFR:1907)2 (tumor-to-organ ratio: 1.00; SD:±0.12), followed by ZEGFR:1907 (0.81±0.27), (ZEGFR:955)2 (0.67±0.18), and control (0.32±0.06). In the liver, the dimeric forms of affibody molecules, (ZEGFR:1907)2 (0.27±0.07) and (ZEGFR:955)2 (0.17±0.05), gave higher tumor-to-organ ratio compared with control (0.06±0.01). The monomeric ZEGFR:1907 ratio (0.12±0.07) was not significantly different from control. For the colon, the ZEGFR:1907 (0.93±0.26) and (ZEGFR:1907)2 (0.84±0.10) showed higher ratio compared with control (0.50±0.08). In the skin, only ZEGFR:1907 showed higher ratio (1.16±0.42) compared with control (0.67±0.18). The tumor-to-blood ratio was equal in all groups. In the tongue, kidneys, spleen, and bone, the tumor-to-organ ratio was also equal between all blocking groups and control.
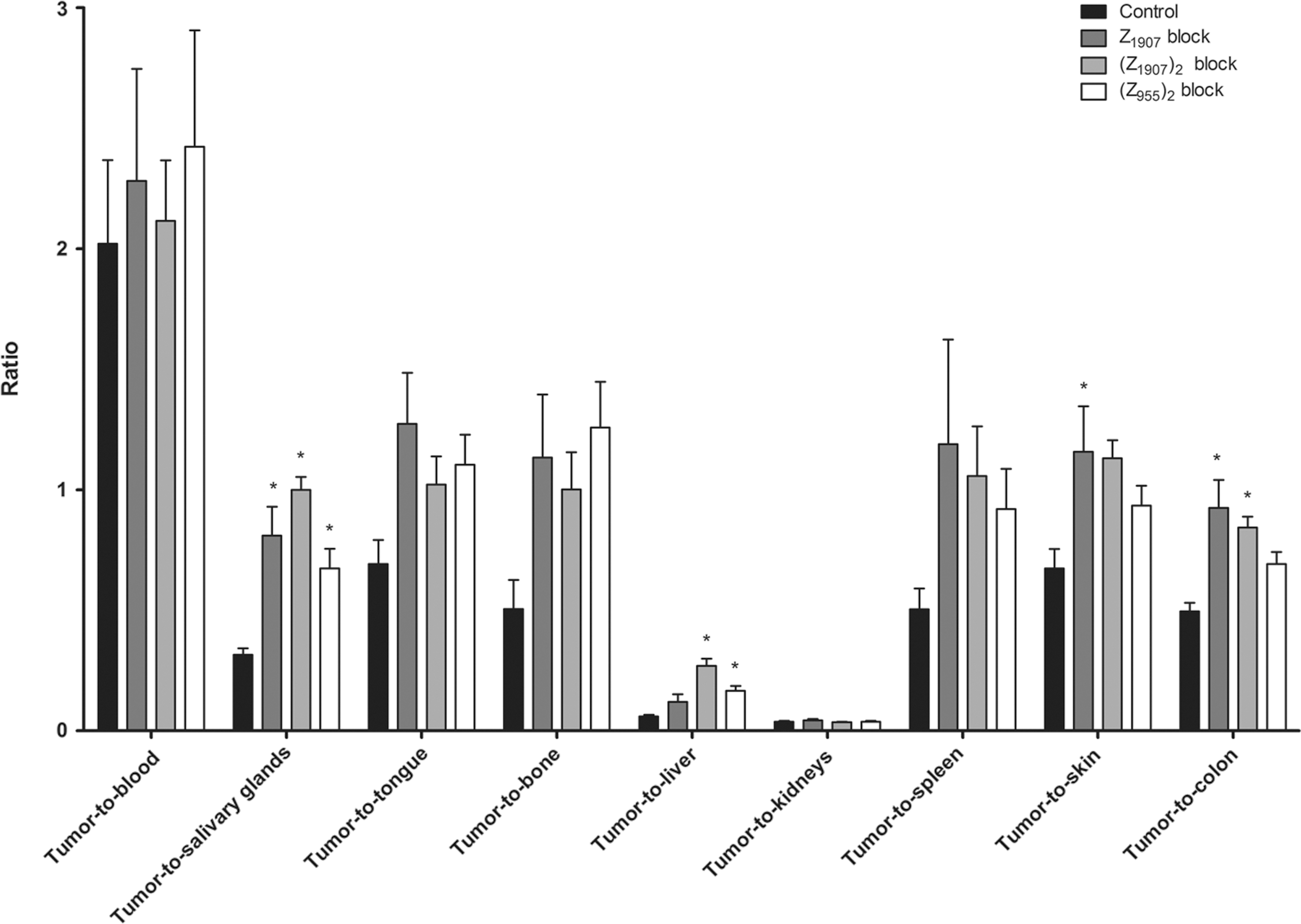
The tumor-to-organ ratio of [67Ga]Ga-NOTA-Bn-NCS-hEGF in tumors and organs of UTSCC-7 xenograft-bearing nude mice. [67Ga]Ga-NOTA-Bn-NCS-hEGF was injected i.v. either alone (Control) or 45 minutes after s.c. injection of indicated affibody molecule. The tumor-to-organ ratio is expressed as activity/gtumor divided by activity/gorgan. Asterisk (*) indicates significant difference compared with the control group. Error bars represent the standard deviation. N=5.
Discussion
Enhanced signaling of EGFR is a common feature of many malignancies. In HNSCCs, enhanced signaling has been shown to be mainly due to overexpression of EGFR. 3,4 This overexpression, evaluated in tumor biopsies, is associated with tumor progression and prognosis, 6 –8 local-regional relapse after radiotherapy, 9 and response to continuous hyperfractioned radiotherapy. 10,11 Quantification of EGFR levels in primary HNSCCs may be useful in identifying subgroups of patients at high risk of tumor recurrence and in selecting the appropriate treatment to improve the long-term survival rates.
In vivo targeted nuclear imaging is advantageous over biopsies because of less false-negative results caused by sampling error and discordance with EGFR expression in primary tumor and its corresponding metastases. Moreover, targeted radionuclide imaging could improve diagnostics.
12
In head and neck cancer patients, PET, using nonspecific tracers as fluoro-2-deoxy-
However, when targeting EGFR in vivo, the natural high expression in many organs, such as the liver, GI tract, and salivary glands, is a problem with regard to tumor versus normal tissue uptake. Modulating the amount of administered ligand can somewhat overcome the problem of an increased background. 16,17 Another method shown to improve tumor-to-normal tissue contrast is preinjection of hEGF or anti-EGFR affibody molecules. 19,20
Herein, it has been demonstrated that lower uptake of a novel radionuclide conjugate, [67Ga]Ga-NOTA-Bn-NCS-hEGF, in EGFR-expressing organs could indeed be achieved by preinjection of the anti-EGFR affibody molecules ZEGFR:1907, (ZEGFR:1907)2, or (ZEGFR:955)2 without compromising the tumor uptake of the radiotracer (Fig. 4). The studied affibody molecules' ability to bind to both mouse and human EGFR and block EGF uptake is of course crucial for the proposed effect. 29,31 In the salivary glands, the best blocking result, in terms of tumor-to-organ ratio, was achieved with (ZEGFR:1907)2 as hypothesized (Fig. 5). In the liver, the pattern of [67Ga]Ga-NOTA-Bn-NCS-hEGF uptake was comparable to that in salivary glands, although the monomeric ZEGFR:1907 did not show any statistically significant difference compared with control. Although the uptake in the liver was reduced with preinjected affibody molecule, the uptake was several times higher compared with tumor tissue. An HNSCC metastasis could probably not be delineated with this technology in the vicinity of the liver. However, when targeting HNSCC, the liver uptake is of less concern for imaging, because hepatic metastases are very uncommon. The dimeric (ZEGFR:1907)2 showed higher tumor-to-liver ratio compared with both the monomeric ZEGFR:1907 and the dimeric (ZEGFR:955)2. In the colon, the tumor-to-organ ratio was higher with the monomeric and dimeric ZEGFR:1907. In addition, the GI tract showed lower uptake values with all preinjected affibody molecules. Actually, there was a slightly, although not significant, lower uptake of [67Ga]Ga-NOTA-Bn-NCS-hEGF and a better tumor-to-organ ratio with preinjection of affibody molecule block in the other organs as well. In line with the hypothesis in the present study, the organs expressing EGFR to a great extent showed a decrease in uptake of [67Ga]Ga-NOTA-Bn-NCS-hEGF with preinjection of blocking anti-EGFR affibody molecules. Although the uptake in the tongue was not significantly lower with preinjected affibody molecule, a trend toward lower uptake could be seen. The tongue is composed of both muscle with low EGFR expression and mucosa with high expression, which may explain the results. In the kidneys, (ZEGFR:1907)2 gave a higher hEGF uptake compared with both control and ZEGFR:1907. Similar effect (significantly increased kidney uptake after partial saturation of EGFR in liver by excess of nonlabeled ligand) has been observed earlier in a number of studies concerning radiolabeled EGF 16,18,20 or anti-EGFR affibody molecules. 24 Most likely, a fraction of a ligand, which would be trapped by interaction with EGFR in liver at low dose of injected ligand, can reach kidney and undergo glomerular filtration and, further, tubular reabsorption in kidneys. This supports a hypothesis that partial blocking of EGFR in liver should increase bioavailablity of the radiolabeled ligand. There were no significant differences in the uptake of [67Ga]Ga-NOTA-Bn-NCS-hEGF in the tumor tissue between the control and blocking groups, although there was a trend toward higher uptake with (ZEGFR:1907)2. The tumor-to-blood ratio did not increase with blocking affibody molecule, most probably because of relatively high blood levels. The animals were sacrificed at 1 hour postinjection of [67Ga]Ga-NOTA-Bn-NCS-hEGF. Higher tumor-to-blood ratio might be achieved if the animals are sacrificed at a later time point to allow further elimination from the bloodstream. However, the majority of radiolabeled hEGF is probably distributed to EGFR-expressing organs within the first 10 minutes followed by a much slower elimination phase in plasma. 15 The biodistribution result is in good agreement with a previous study with preinjection of (ZEGFR:955)2, before 111In-CHX-hEGF, although the tumor-to-liver ratio in the present study is slightly lower for (ZEGFR:955)2. 19
To achieve better tumor-to-organ contrast, it was aimed for a high uptake of blocker in the liver and thereby to increase blood concentrations of targeting hEGF. To increase the tumor-to-organ ratios, the blocker should also saturate EGFR in other organs such as the salivary glands and tongue. The ideal blocker should have high affinity for EGFR and slow off rate to efficaciously bind and saturate the EGFR in normal tissue. The size should be large enough to prevent an efficient extravasation in less well-vascularized tissue as in large tumors. As a preblocking agent of EGFR, the affibody molecules are in favor of unlabeled EGF because of longer circulating time, lower degree of internalization, and less EGFR activation. 32,33 In the present study, preinjection of the dimeric (ZEGFR:1907)2 with higher affinity (K D: 1.6 nM), larger size, and slower off rate in vitro, compared with the monomeric ZEGFR:1907 (K D: 2.8 nM), 24 achieved the highest tumor-to-organ ratios in the liver and salivary glands. The dimeric (ZEGFR:955)2 with much lower affinity (K D: 50 nM) 28 achieved the poorest results.
Anti-EGFR affibody molecules have not been yet used in humans. Anti-HER2 affibody molecules have been used in a microdosing setting, and no adverse events have been found. 12 Preclinical toxicity data in rats suggest that there was no observable toxicity of affibody molecules (unpublished data).
In the settings of this study, the small actual difference in size between monomer and dimer seems to be of subordinate importance compared with affinity and off rate. The most promising format of affibody molecule for blocking of normal tissues uptake before the administration of [67Ga]Ga-NOTA-Bn-NCS-hEGF was the dimeric high-affinity (ZEGFR:1907)2. This is probably due to the slower off rate and, hence, higher affinity of (ZEGFR:1907)2. Dimeric forms have an increased concentration of binding sites in close proximity to the target protein, which reduce dissociation rates. The results are in line with a study comparing 111In-labeled ZEGFR:1907 with 111In-labeled (ZEGFR:1907)2 in EGFR-expressing A431 cells. The dimeric (ZEGFR:1907)2 showed a higher uptake in both high EGFR-expressing organs, such as the liver and colon, and low EGFR-expressing organs, such as the muscle and bone in vivo. In contrast, the tumor uptake and tumor-to-organ contrast was superior to the monomeric ZEGFR:1907. 24
When looking at the results from the present study one should take into account that human EGF has high affinity to murine EGFR and vice versa. The Affibody molecules have been selected to bind human EGFR. Previous studies have demonstrated that uptake of radiolabeled ZEGFR:1907, (ZEGFR:1907)2, and (ZEGFR:955)2 was significantly higher in murine tissues expressing EGFR (liver and colon) than uptake of non–EGFR-specific control affibody molecules. 23,24 Further, the uptake in these tissues was significantly reduced when a large excess of nonlabeled tracer was injected. 23,24 These are strong indications of cross-reactivity of anti-EGFR affibody molecules with murine EGFR. However, the development was not aimed to an exact match of affinity of these affibody molecules to murine and human EGFR. Thus, detailed optimization of blocking affibody molecule dose in mice might have a limited relevance in a clinical situation wherein human EGFR would be expressed in both tumors and normal tissues. The fact that such positive results were produced in these settings is very promising, and an even more effective blocking might occur in a clinical setting. Consequently, further development of this approach should be performed in clinics.
When selecting a tracer for radionuclide-targeted imaging, generally small targeting proteins have better tumor penetration and the unbound fraction is more rapidly excreted, leading to higher tumor-to-organ ratios and therefore better contrast. Also, the affinity of the ligand and its internalization are important properties in targeted imaging. hEGF meets these requirements with small size, high affinity, and high internalization of the receptor–ligand complex. 33
The novel hEGF radionuclide conjugate [67Ga]Ga-NOTA-Bn-NCS-hEGF was prepared at room temperature just within 10 minutes. It demonstrated high stability in vitro, as determined by both radio-HPLC and ITLC. This will be an important advantage when transitioning the labeling from 67Ga to 68Ga, which has only a 68 minutes half-life.
The cellular binding study clearly demonstrated a specific binding to hEGFR, as pre and simultaneous administration of unlabeled hEGF reduced the cell-bound radioactivity significantly. Previously, hEGF was conjugated to DOTA moiety and labeled with 68Ga under elevated temperature required by the complex reaction with DOTA. Either conventional heating or microwave mode was used, and in both cases, the bioconjugate demonstrated high stability and maintenance of the biological activity and successful localization of tumor xenografts with micro-PET. 15 In this study, NOTA complexing moiety was used, which offers advantages such as higher stability of the resulting complex and the possibility to perform the labeling synthesis at room temperature. 27 The latter provides mild labeling conditions for fragile, temperature-sensitive macromolecules as well as a simple kit-type tracer production procedure. The combination of the easy access to 68Ga from a generator system and a kit-type labeling at room temperature is of great interest to clinical PET centers. The reason for using gamma-emitting 67Ga as a surrogate for 68Ga in this study was to take advantage of the longer half-life of the former, providing sufficient time for the handling of large group of animals.
In conclusion, the preadministration of anti-EGFR affibody molecules reduced the uptake and improved the tumor-to-organ ratio in the liver, salivary glands, and colon of the subsequently injected radiolabeled EGF. The best results were obtained with the dimeric (ZEGFR:1907)2, which possesses the highest EGFR affinity of the studied affibody molecules. Further, this targeting was performed using a novel radionuclide conjugate [67Ga]Ga-NOTA-Bn-NCS-hEGF, which showed promising results for further 68Ga studies using PET. These findings demonstrate that preblocking with an anti-EGFR affibody molecule, especially (ZEGFR:1907)2, is a promising method that could enhance the outcome of radionuclide-based EGFR-expressing tumor diagnostics and imaging.
Footnotes
Disclosure Statement
No financial conflicts of interest exist for any of the authors.
Acknowledgments
The authors thank Affibody AB for providing the affibody molecules, Dr. R. Grenman, Turku University Central Hospital, Finland, for providing the UTSCC-7 cells, and the Chemical Engineer Veronika Asplund for technical support.