
Abstract
Photodynamic therapy (PDT) is a noninvasive optical treatment method in which the topical or systemic delivery of photosensitizing drugs is followed by irradiation with broadband red light. Coupling photosensitizers with a specific antibody may allow this approach to target specific cancers. This study determines the antitumor efficacy of coupling verteporfin (Visudyne®), a hydrophobic polyporphryin oligomer, with an antiepidermal growth factor receptor (anti-EGFR) antibody. Poly[2-methacryloyloxyethyl phosphorylcholine-co-n-butyl methacrylate-co-p-nitrophenylcarbonyloxyethyl methacrylate] (PMBN) was conjugated with an anti-EGFR antibody and mixed with verteporfin (verteporfin–PMBN–antibody complex). Tumor-bearing mice were intravenously injected with the verteporfin–PMBN–antibody complex or verteporfin plus PMBN without the antibody. Irradiation was conducted at 640 nm with a dose of 75 J/cm2. The fluorescence intensity in A431 cells in vitro was threefold higher after exposure to verteporfin–PMBN–antibody complex than after exposure to verteporfin–PMBN. In A431 tumor-bearing mice, the intratumor concentration of verteporfin was 9.4 times higher than that of the skin, following administration of the verteporfin–PMBN–antibody complex. Tumor size significantly decreased within 8 days in mice treated with verteporfin–PMBN–antibody complex compared with those treated with verteporfin–PMBN. PDT using a PMBN–verteporfin–antibody complex offers a promising anticancer therapy.
Introduction
Photodynamic therapy (PDT) involves the systemic or local administration of a photosensitizer followed by its subsequent activation by red light. In the presence of oxygen, the activated photosensitizer can generate reactive oxygen species that then produce peroxidative reactions that cause cell damage and, ultimately, cell death. PDT is already widely used for the treatment of many cancers including lung cancer, head and neck cancers, liver metastases, cholangiocarcinoma, and prostate cancer. 1 Several photosensitizers, including Photofrin® and Levulan®, have been approved for cancer therapy. Verteporfin (Visudyne®) is a hydrophobic polyporphyrin oligomer with two structural isomers (Fig. 1), a short photosensitivity period, 2 and maximum absorption at 689 nm. Verteporfin has been approved for PDT of abnormal blood vessels in the eye, including the wet form of macular degeneration, and is usually intravenously administered within 15 minutes before laser irradiation. In terms of antitumor applications, verteporfin has been shown to be effective against various cancers affecting the eye in several clinical studies. 3 –8 Although several studies have evaluated its potential use in other cancers, most of these studies have been performed in vitro using cell lines, and photosensitizers often show poor specificity for tumor tissue, limiting their application in PDT.

Structure of verteporfin isomers.
One approach for improving tumor specificity is to incorporate the photosensitizer using drug delivery systems such as liposomes, 9 –11 epidermal growth factor antibody, 12 water-soluble polymer carriers, 13 –20 and monoclonal antibodies. 21 –25 So far, hydrophobic substances have been successfully delivered in vitro and in vivo using poly[2-methacryloyloxyethyl phosphorylcholine (MPC)-co-n-butyl methacrylate (BMA)-co-p-nitrophenylcarbonyloxyethyl methacrylate (MEONP)] (PMBN) conjugates with proteins, such as EGF, hepatitis B virus surface antigen, and IL-2. 26 –29 PMBN shows good cytocompatibility and can solubilize poorly soluble drugs, such as verteporfin, because of its amphiphilic properties. In addition, the MEONP unit in the PMBN chain is an active ester unit that can immobilize proteins, including antibodies.
Epidermal growth factor receptor (EGFR) is a widely expressed receptor; however, its expression is often greatly increased in some types of cancer, including squamous cell carcinoma. 30 Overexpression of EGFR is also associated with advanced disease, poor prognosis, and resistance to conventional chemotherapy. 31 –33 Therefore, EGFR has become a promising anticancer therapeutic target, and several drugs, including gefitinib, erlotinib, and cetuximab, are directed against it. It has been reported that anti-EGFR monoclonal antibodies (B4G7) can be chemically conjugated to gelonin and a human pancreatic ribonuclease1-EGF fusion protein. 34 Therefore, this study hypothesizes that a complex consisting of verteporfin, PMBN, and an anti-EGFR antibody (verteporfin–PMBN–Ab+complex) would show greater antitumor efficacy compared with verteporfin and PMBN in the absence of the anti-EGFR antibody (verteporfin–PMBN complex). To test this hypothesis, the antitumor effects of these complexes against cancers overexpressing EGFR were compared in vitro and in vivo using tumor-bearing mice.
Materials and Methods
Cell lines
A431 epidermoid carcinoma cells (American Tissue Type Culture Collection [ATCC] No. CRL-1555) and H69 small-cell lung cancer cells (ATCC No. HTB-119) were obtained from the ATCC. A431 cells were maintained in Dulbecco's modified Eagle's medium, and H69 cells in Roswell Park Memorial Institute (RPMI) 1640 medium supplemented with 10% heat-inactivated fetal bovine serum (Gibco) in a 5% CO2 humidified incubator at 37°C.
Animals
All animal experiments were conducted according to Keio University's institutional guidelines for the care and use of laboratory animals in research. Female BALB/cA nude mice were purchased from Oriental Yeast Co., Ltd. They were maintained under specific pathogen-free conditions at Keio University Experimental Animal Center and fed sterile food and water. In each experiment, 8–9 mice aged 6 weeks were used.
Mouse monoclonal antibody against human EGFR
Hybridoma 528 (ATCC No. HB-8509) cells, which produce a murine IgG2a mouse monoclonal antibody against human EGFR receptors, were obtained from the ATCC. The cells were cultured in RPMI 1640 medium supplemented with 10% fetal calf serum in a humidified atmosphere consisting of 5% CO2 in air at 37°C. Ascitic fluid was produced by intraperitoneal inoculation of BALB/c mice with 5×106 hybridoma 528 cells. The fluid was collected from the mice at 2–4 weeks after inoculation and centrifuged at 10,000 g for 10 minutes to remove debris. The purified monoclonal (528) antibody was prepared using the Mab Trap™ kit (GE Healthcare).
Preparation of the verteporfin–PMBN–antibody complex
PMBN (Fig. 2A) was synthesized from (monomer ratios) 60 mol% MPC, 20 mol% BMA, and 20 mol% MEONP, as previously described. 35 The molecular weight of PMBN was ∼10,000 Da. The PMBN–antibody complex was prepared by gently mixing 10 mg of PMBN with 1 mg of the anti-EGFR antibody in 5 mL of PBS (final concentration: 200 μg/mL) for 24 hours at 4°C. Verteporfin (0.2 mg; final concentration: 40 μg/mL) was immediately added before use. Figure 2B shows a schematic view of the resulting complex. As a control, verteporfin was mixed with PMBN without the anti-EGFR antibody. The prepared complexes were filtered using a cell strainer (100 μm; BD Falcon).

Chemical structure of PMBN
Measurement of complex size
The diameters of PMBN, PMBN–antibody, verteporfin–PMBN, and verteporfin–PMBN–antibody complexes were measured using a Zetasizer nano (Malvern Instruments).
Measurement of absorbance
The PMBN solution of aggregate (2 mg/mL) was centrifuged at 20,000 g for 5 minutes and the absorbance of p-nitrophenol was measured using a spectrophotometer (U-0080D; Hitachi). Verteporfin (0.1 mg/mL) was dissolved in 0.6 mg/mL PMBN polymer or N,N-dimethylformamide.
Visualization of verteporfin uptake in A431 cells in vitro
A431 cells were seeded onto 24-well plates at 1×104 cells/well and cultured for 24–48 hours before use. Under strict low-light conditions, 100 μL of verteporfin–PMBN–antibody and verteporfin–PMBN was added to 1 mL of the cells/culture medium and incubated for 10, 20, or 30 minutes. Then, the cells were washed three times with PBS and the medium was replaced with fresh medium. Verteporfin uptake was measured within 1 hour. To measure verteporfin uptake, the plates were mounted in a laser-scanning confocal fluorescence inverted microscope (Leica TCS-SP5; Leica Microsystems, Inc.). Light optical and fluorescence images were simultaneously obtained for direct intracellular visualization of fluorescence signals. The cells were scanned at 488 nm (Ar laser) and fluorescence at 650–700 nm was recorded.
Measurement of the tissue verteporfin concentration in vivo
A431 or H69 cells (1×107 cells in 100 μL of PBS) were subcutaneously implanted in mice. When the tumors had reached the size of ∼5 mm in diameter, verteporfin–PMBN–antibody or verteporfin–PMBN was administered as a single bolus intravenous injection at a dose of 6 mg/kg. Tissue samples (liver, lung, heart, muscle, skin, and tumor) were taken after 30 minutes, 1 hour, 24 hours, or 48 hours, weighed, and lyophilized. Then, 500 μL of N,N-dimethylformamide was added to all freeze-dried samples, which were then homogenized using a MagNA Lyser (Roche) at 6500 rpm for 30 seconds and centrifuged to extract verteporfin. The concentration of verteporfin was calculated by measuring the fluorescence emitted at 700 nm (with excitation at 430 nm) using a Synergy 4 Multimode microplate reader (BioTek).
Evaluation of the effects of anti-EGFR receptor on PDT using verteporfin–PMBN in vivo
A total of 1×107 A431 or H69 cells in 100 μL of PBS were subcutaneously implanted in nude mice. When the tumors reached ∼5 mm in diameter, verteporfin–PMBN–antibody or verteporfin–PMBN was intravenously injected at a dose of 6 mg/kg. One (1) hour later, the mice were exposed to a diode laser light (at 640 nm) using an Optical Fuel laser (Sony). Q-band excitation was established at this wavelength. The light dose was 75 J/cm2 and irradiance ranged from 0.18 to 0.76 W/cm2; laser light was applied for a period of time (range: 84–469 seconds) calculated based on the volume of the tumor. During irradiation, the temperature was kept at 20°C. Tissue surrounding the tumor was covered with a black cloth to avoid irradiating normal tissue. The lengths and widths of tumors were measured by the same observer using sliding calipers. Tumor volume was calculated as 0.4×longest diameter×width2.
Statistical analysis
Values are given as means±standard error (SE). Differences in tumor volumes were analyzed using unpaired Student's t-test. The survival of mice was analyzed by the Kaplan–Meier method and differences in survival were compared using the log-rank test. A p-value of <0.05 was considered statistically significant.
Results
Characterization of the verteporfin–PMBN–antibody complex
The mean±SE diameters of PMBN alone, PMBN–antibody,verteporfin–PMBN, and verteporfin–PMBN–antibody were 59.8±1.5, 101.5±5.5, 125.0±4.1, and 129.7±3.9 nm, respectively. In terms of optical properties, when PMBN is conjugated with a protein, p-nitrophenol is released (Fig. 3A), which has a yellow color with an absorption at 250–450 nm. Normally, p-nitrophenol does not absorb light at a wavelength above 500 nm; however, in the presence of verteporfin, the optical spectrum is significantly altered, as shown in Figure 3B.
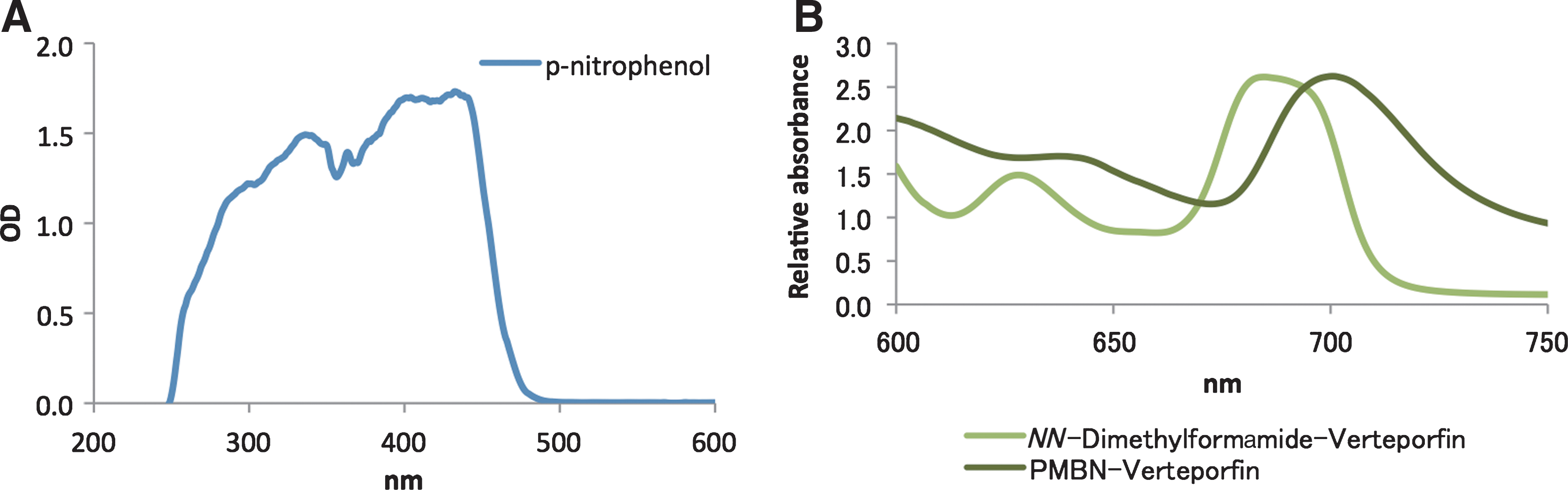
Relative absorbance of p-nitrophenol
Effects of complexing with the anti-EGFR antibody on verteporfin uptake in vitro
To determine whether the PMBN–antibody complex enhances cellular uptake of verteporfin, the fluorescence intensity of the emission peak between 650 and 700 nm was measured. A431 cells, which overexpress EGFR, were used in this experiment. Representative optical and fluorescence images are shown in Figure 4A for verteporfin in the presence and absence of the antibody. As shown in Figure 4B, the fluorescence intensity increased over time in both groups of cells, but was consistently higher in cells exposed to the verteporfin–PMBN–antibody, and was three times higher at 30 minutes than in cells exposed to verteporfin–PMBN. This indicates that cellular verteporfin uptake was increased when administered in the presence of PMBN and the antibody complex in vitro.
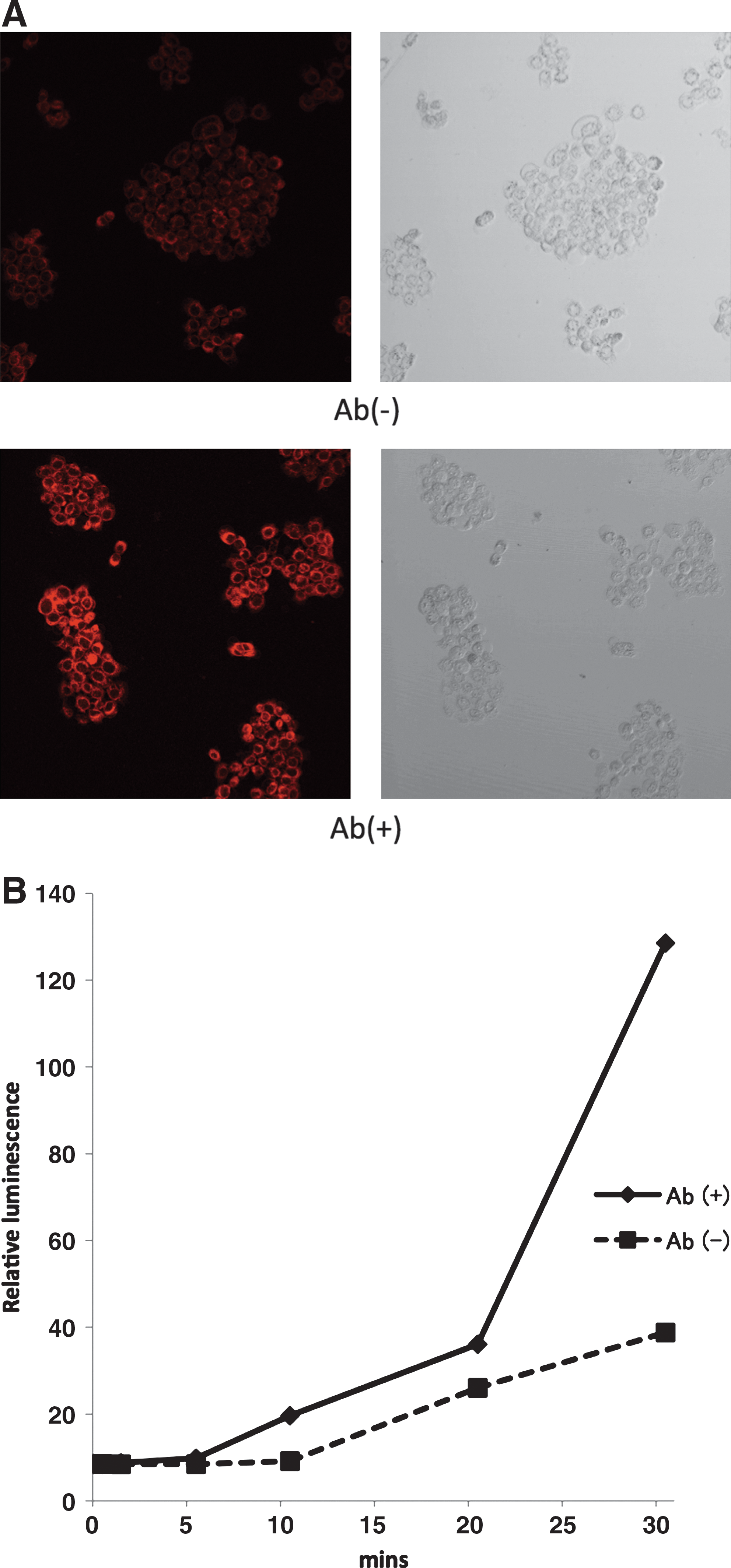
Cellular uptake of verteporfin–PMBN with [Ab(+)] and without [Ab(−)] the anti-epidermal growth factor receptor (anti-EGFR) antibody in A431 cells in vitro.
Effects of complexing with the anti-EGFR antibody on verteporfin uptake in vivo
Next, whether the tissue uptake of verteporfin by EGFR-expressing tumors in vivo was enhanced by complexing with the anti-EGFR antibody was examined. A431 tumor-bearing mice were administered with verteporfin corresponding to a dose of 6 mg/kg. As shown in Figure 5, the concentration of verteporfin in A431 tumors in mice treated with verteporfin–PMBN–antibody was 9.4 times higher than that in skin at 1 hour after administration. In contrast, in verteporfin–PMBN-treated mice, the verteporfin concentration was only 3.6 times higher in the tumor than in skin. The tumor concentration of verteporfin was 1.74 times higher in verteporfin–PMBN–antibody-treated mice compared with verteporfin–PMBN-treated mice at 1 hour after administration. Surprisingly, the concentration of verteporfin tended to be higher in muscle than in skin, although the concentrations were still lower than those in the A431 tumor. Relatively high concentrations of the verteporfin–PMBN and verteporfin–PMBN–antibody complexes were also detected in the liver, lung, and heart (Supplementary Table S1; Supplementary Data are available online at
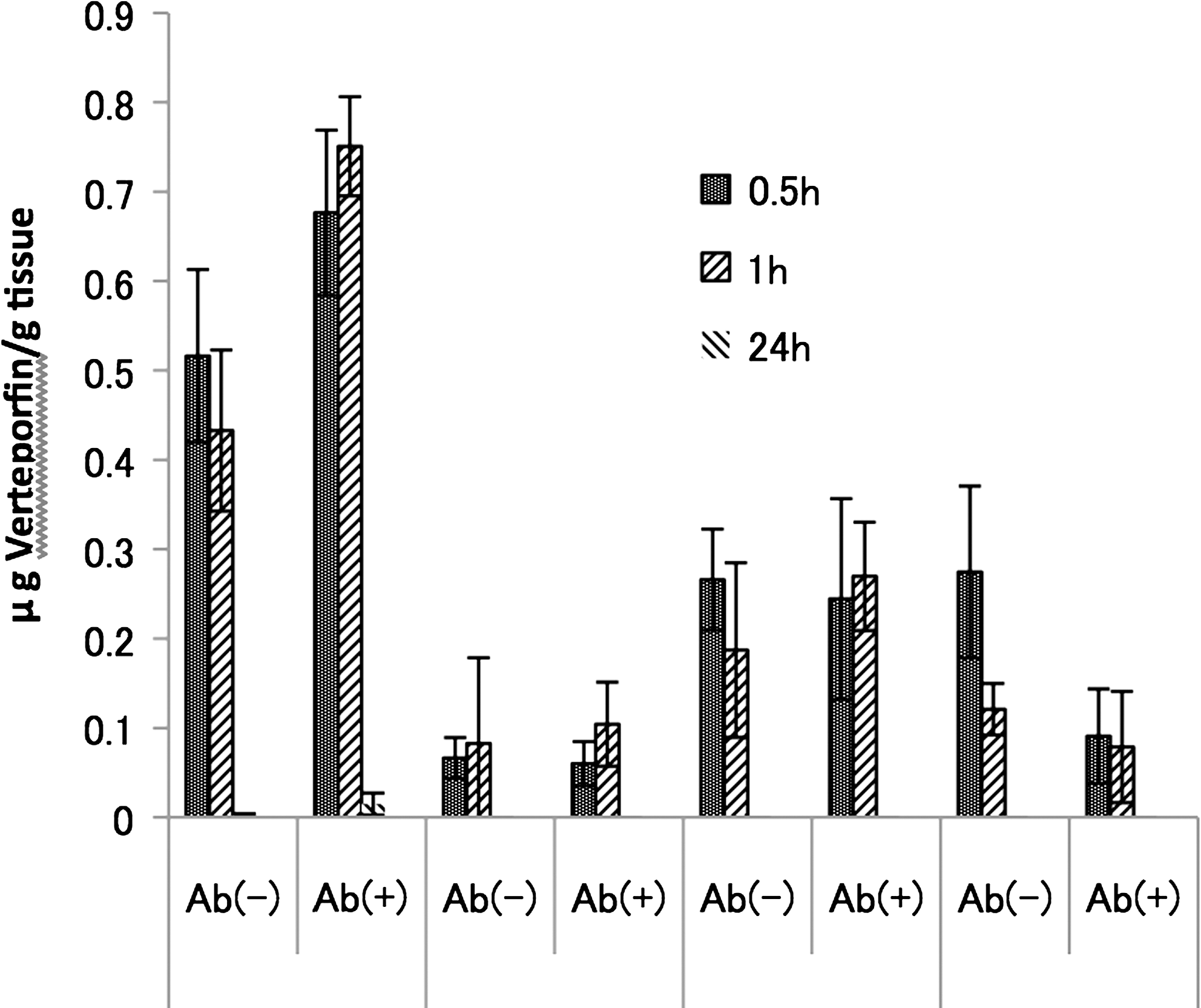
In vivo concentrations of verteporfin in tumor tissue, muscle, and skin of mice bearing A431 or H69 tumors following intravenous administration of verteporfin–PMBN with [Ab(+)] and without [Ab(−)] the anti-EGFR antibody.
Effects of PDT with the verteporfin–PMBN–antibody complex on tumor size in vivo
To evaluate whether complexing with the anti-EGFR antibody enhanced PDT with verteporfin, mice bearing A431 tumors or H69 tumors were exposed to laser light at 640 nm with a dose of 75 J/cm2 at 1 hour after administration of the respective complex. Tumor size was then measured at 8 days after PDT. In mice bearing A431 tumors, administration of the verteporfin–PMBN–antibody decreased tumor volume at day 8 to 149.1±44.2 mm3, which was significantly smaller than that of mice treated with verteporfin–PMBN (1200.0±224.3 mm3, p=0.00098) and untreated mice (1937.3±285.2 mm3, p=0.000023). In contrast, the tumor volume at 8 days after PDT in mice treated with verteporfin–PMBN–antibody (109.3±39.6 mm3) was similar to that in verteporfin–PMBN-treated mice (100.0±32.7 mm3, p=0.893) and that in untreated control mice (176.9±39.6 mm3, p=0.397).
Next, the passive enhancement effect (tumor volume in the verteporfin–PMBN group divided by the tumor volume in the negative control group; Fig. 6A) and the active enhancement effect were calculated (tumor volume in the verteporfin–PMBN–antibody group divided by tumor volume in the verteporfin–PMBN group; Fig. 6B). Although no passive enhancement effect was found, a large enhancement effect was detected in mice bearing A431 tumors, but not in mice bearing H69 tumors.
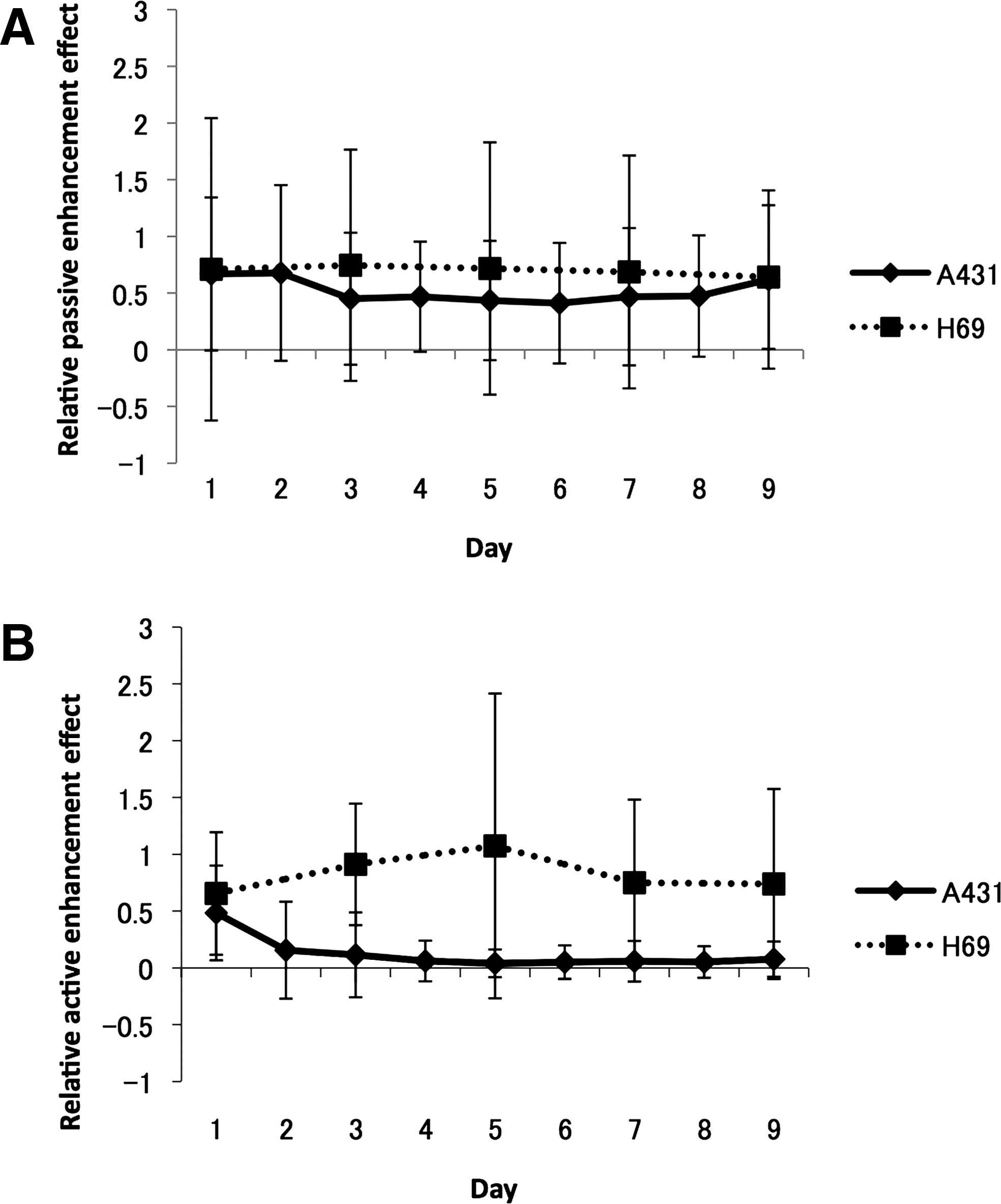
Relative passive enhancement effect
Effects of PDT with the verteporfin–PMBN–antibody complex on survival
Finally, the effects of PDT with the verteporfin–PMBN–antibody complex on overall survival (Fig. 7) were evaluated. The median survival of A431-bearing mice was 54 days [interquartile range (IQR)=40–88 days] in mice treated with the verteporfin–PMBN–antibody complex. In contrast, median survival was significantly shorter in mice treated with the verteporfin–PMBN complex (35 days, IQR=21–61 days, p=0.0251) and in untreated control mice (25.5 days, IQR=18–58 days, p=0.008).

Effects of verteporfin–PMBN with [Ab(+)] and without [Ab(−)] the anti-EGFR antibody on the survival of A431 model mice after photodynamic therapy. Survival was analyzed using the Kaplan–Meier method. NC, normal control.
Discussion
The development of alternative, minimally invasive therapies is desirable to improve the quality of life of patients undergoing cancer therapy. Although endoscopy-based techniques are possible for some lesions, such as early carcinoma of the esophagus, stomach, colon, and rectum, deeper cancers usually require invasive surgical resection. PDT using photosensitive chemicals is a promising approach that can be used in combination with endoscopic dissection, because organ damage is limited and patients can undergo further treatments. However, PDT is still not widely performed because of the limited specificity of the photosensitizers for cancerous tissue. Hence, healthy noncancerous tissue may also be damaged following irradiation. Clearly, methods to improve the delivery of photosensitizers to tumor tissue are needed before this approach will become widely used. The introduction and efficacy of molecular targeted drugs, such as gefitinib, erlotinib, and cetuximab, which are directed against EGFR, have renewed interest in PDT for cancer therapy. By complexing photosensitizers with antibodies that recognize antigens overexpressed on tumor tissue, the specificity of photosensitizers for tumor tissue should be improved. Therefore, in this study, whether complexing verteporfin with an EGFR antibody would enhance its antitumor effects was investigated.
Because verteporfin is a hydrophobic oligomer, a complex with PMBN, a water-soluble polymer, was prepared. PMBN was chosen, because it has been already shown that PMBN accumulates in cancer cells by attachment to the cell membrane, 36 processes that may be related to its hydrophilic components, although the precise mechanism remains unclear. In addition, PMBN contains an active ester that can bind to a protein of interest, in this case an antibody, which can bind to cells via antigen–antibody reactions or ligand–receptor reactions. Accordingly, complexing PMBN with a chosen antibody should facilitate its binding to a cell surface protein and subsequently translocate into the cell.
Most photosensitizers tested to date show some selectivity for tumor tissue. However, they also accumulate in normal tissues such as the skin. As a result, prolonged cutaneous phototoxicity after exposure to sunlight has been reported for many compounds. 37 Many cancer cells are hyperpermeable and have impaired lymphatic drainage. Therefore, polymers with a molecular weight of 10,000 can penetrate into and accumulate in tumor cells via the enhanced permeability and retention effect. 38 PMBN nanoparticles are spherical in shape and ∼200 nm in diameter 35 and are readily taken up by tumor cells. However, their relatively large size should limit nonspecific tissue accumulation, because such molecules are less able to pass through the tight junctions of tissue vasculature, except in tissues with a leaky vasculature, such as the liver, spleen, and tumors. Accordingly, complexing photosensitizers with relatively large nanocarriers, such as PMBN, should prevent their accumulation in many organs, including the skin, and thus reduce the risk of phototoxicity. 39
To expand on these principles, this proof-of-concept study was performed, in which verteporfin was complexed with PMBN and anti-EGFR antibodies to enhance the specificity of verteporfin. In vitro, the cellular uptake of the verteporfin–PMBN–antibody complex was enhanced compared with that of verteporfin–PMBN, and this was particularly evident within 30 minutes after administration.
Next, studies in vivo using mice bearing A431 tumors, which overexpress EGFR, or H69 tumors, which do not, were performed. The mice were treated with either verteporfin–PMBN–antibody or verteporfin–PMBN followed by a single irradiation at 75 J/cm2 delivered transcutaneously. Greater verteporfin concentrations in the tumor tissue of A431-bearing mice compared with H69-bearing mice was noted. Moreover, the concentration of verteporfin in the A431 tumor tissue was greater than that in either the muscle or skin in verteporfin–PMBN–antibody-treated mice. Tumor concentrations of verteporfin were also greater in verteporfin–PMBN–antibody-treated mice than in verteporfin–PMBN-treated mice. Notably, the tumor size at 8 days after PDT was significantly smaller and median survival was significantly longer in verteporfin–PMBN–antibody-treated mice than in verteporfin–PMBN-treated mice and untreated control mice. To confirm that the antitumor effect was due to PDT, the tumor size between nonirradiated verteporfin–PMBN–antibody-treated mice and control mice bearing A431 tumors was compared, and no difference in tumor growth between these two groups was found (data not shown). Similarly, laser irradiation alone did not affect tumor size (data not shown). Supporting these findings, no enhanced tumor killing effect in mice bearing H69 tumors treated with verteporfin–PMBN–antibody and laser irradiation was found.
The results of this proof-of-concept study should be interpreted with caution. First, only two cancer cell lines were used, one showing high EGFR expression and the other showing negligible EGFR expression. Further studies using other cell lines with intermediate expression of EGFR would be valuable to confirm these findings. Second, fixed doses of verteporfin and laser irradiation were used. Although the doses used achieved good antitumor effects, dose–response studies would help to determine the optimum doses of both verteporfin and laser irradiation. Third, the mean size of the PMBN complexes was relatively small compared with the size reported in another study (∼200 nm). 35 This may be at least partly responsible for the observed accumulation in muscle, skin, liver, lung, and heart, independent of the presence/absence of the antibody. As described earlier, the preparation of larger complexes may be advantageous to reduce their accumulation in healthy tissue. Another factor that should be addressed in future studies is the concentrations of verteporfin and antibodies in the complexes. It is possible that the complexes are not homogeneous in terms of either factor, which may ultimately influence not only their uptake by tumor tissue, but also nonspecific uptake by healthy tissue.
Taken together, these results indicate that complexing verteporfin with PMBN and an anti-EGFR antibody enhances the therapeutic effects of PDT with verteporfin. The results presented here are encouraging and warrant further research to expand and validate the present findings. In particular, studies are needed to confirm the mechanism of action and to demonstrate the molecular targeting properties of the complex, by incorporating other antibodies into the complex and using other cell lines or cancer models.
Footnotes
Acknowledgments
The authors thank Y. Nakamura for her continued support. This work was funded by a Grant-in-Aid of Scientific Research (A) and a grant from Keio Gijuku Academic Development Funds.
Disclosure Statement
The authors have no potential conflicts of interest to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.