
Abstract
68Ga labeled NOTA-RGD was a recently developed positron emission tomography (PET) radiotracer for the visualization of angiogenesis, and is regarded as a promising imaging agent for cancer and several other disorders. In this study, we investigated the whole-body distribution and radiation dosimetry of 68Ga-NOTA-RGD in humans. Ten cancer patients (53.7±13.5 years; 61.5±7.4 kg) participated in this study. PET scans were performed using a PET/computed tomography (scanner in three-dimensional mode). After an intravenous injection of 172.4±20.5 MBq of 68Ga-NOTA-RGD, eight serial whole-body scans were performed during 90 minutes. Volumes of interest were drawn manually over the entire volumes of the urinary bladder, the gallbladder, heart, kidneys, liver, lungs, pancreas, spleen, and stomach. Time-activity curves were obtained from serial PET scan data. Residence times were calculated from areas under curve of time-activity curves and used as input to the OLINDA/EXM 1.1 software. The uptake of 68Ga-NOTA-RGD was highest in the kidneys and urinary bladder. Radiation doses to kidneys and urinary bladder were 71.6±28.4 μGy/MBq and 239.6±56.6 μGy/MBq. Mean effective doses were 25.0±4.4 μSv/MBq using International Commission of Radiation Protection (ICRP) publication 60 and 22.4±3.8 μSv/MBq using ICRP publication 103 weighting factor. We evaluated the radiation dosimetry of 68Ga labeled NOTA-RGD, which has an acceptable effective radiation dose.
Introduction
Angiogenesis is the physiological process involving the growth of new blood vessels, and an essential developmental process. It is regulated by the interplay of growth factors and inhibitors, and their imbalances can lead to disease. Therefore, the regulation of angiogenesis offers a strategy for the treatment of cancer and other disorders, and intensive efforts have been undertaken to develop such therapeutic strategies. 1 –3
The integrins are a family of cell-surface receptors that bind extracellular matrix components, organize the cytoskeleton, and activate intracellular signaling pathways. 4 Integrin αvβ3 is a member of this family of receptors, highly expressed on activated endothelial cells during angiogenesis, and associated with the tumor growth, invasion, and metastasis. 5 –7
For the targeting of αvβ3, Arg-Gly-Asp (RGD) derivatives labeled with various radioisotopes, such as, 125I, 99mTc, 18F, 90Y, 111In, and 64Cu, have been developed 8 –13 and their biodistribution and dosimetry studies have been examined. 14,15 Recently, 1,4,7-triazacyclononane-1,4,7-triacetic acid (NOTA)-based bifunctional chelating agent was employed to label an RGD peptide to 68Ga. 16 The importance of 68Ga for clinical positron emission tomography (PET) imaging has increased recently, because it has several inherent advantages for positron imaging in humans. 17,18 The 67.6 minutes half-life of 68Ga is suitable for PET imaging, and expected radiation dose is lower than those of other radioisotopes with a longer half-life. High positron yield (89%) and easy accessibility by use of in-house 68Ge/68Ga generators are also beneficial physical characteristics. 19 Furthermore, the long half-life (270.8 days) of the parent nuclide 68Ge allows generators to be used for more than a year.
Human radiation dose evaluation of a new radiotracer is important for risk-benefit assessments in clinical application. The aim of this study was to evaluate the whole-body distribution and radiation dosimetry of 68Ga labeled NOTA-RGD in humans using biodistribution data obtained by a PET/computed tomography (CT) scanner.
Materials and Methods
Radiochemistry
The radiotracer, 68Ga-NOTA-RGD was synthesized using a minor modification of a previously reported method. 16 Briefly, a NOTA-RGD kit, which contains NOTA-RGD (10.7 μg, 10 nmol), sodium acetate (49.0 μg, 0.6 mmol), and acetic acid (1.8 mg, 29 μmol), was prepared and used for 68Ga labeling. Freshly eluted 68GaCl3 (1.0 mL, ∼740 MBq/0.1 M HCl solution) solution from a 68Ge/68Ga-generator was added to the NOTA-RGD kit using a 24 gauge I.V. catheter and a fluorinated ethylene propylene needle to avoid metal contamination. The reaction mixture was mixed vigorously, and kept at 90°C–95°C for 5 minutes. After the reaction, the reaction mixture was passed through an Alumina N light Sep-Pak® cartridge (Waters), which was preconditioned with water (5 mL) and a syringe filter (0.2 μm Supor® Membrane Low protein binding; PALL Co.). 68Ga-NOTA-RGD was eluted with isotonic saline (2 mL). Radiochemical yields and purities were checked by radio-TLC; radiochemical yields were >98% after the 68Ga labeling procedure, and radiochemical purities were >99.5% after purification.
Subjects
All procedures of this study were approved by the Institutional Review Board of Seoul National University Hospital, Seoul, Korea. Ten patients (4 women and 6 men) with lung cancer or lymphoma were enrolled in this study. Mean patient age and weight were 53.7±13.5 years (range: 31–72 years) and 61.5±7.4 kg (range: 49–73 kg), respectively.
PET/CT procedure
A Biograph TruePoint TrueV PET/CT scanner (Siemens Medical) was used in this study to acquire serial emission and transmission scan data sets. The scanner was composed of 4 rings of detector blocks. Each ring contained 48 detector blocks, and each detector block consisted of a 13×13 array of lutetium oxyorthosilicate scintillation crystals, which has a dimension of 4×4×20 mm3. The axial field-of-view of the PET scanner was 216 mm. The scanner was operated only in the three-dimensional (3D) mode for PET emission scans.
In all patients, the upper body from the neck to the upper thigh was covered by a 5-bed emission scan. To obtain the time-activity curves of organs, eight serial emission scans were performed on all patients over 1.5 hours (about 1.3 times the half-life of 68Ga) after an intravenous injection of 68Ga-NOTA-RGD (172.4±20.5 MBq). The durations of emission scans varied from 30 to 300 seconds per bed (30, 30, 30, 45, 60, 180, 180, and 300 sec/bed). Scans were started at 1, 4, 7, 10, 15, 30, 46, and 62 minutes postinjection. All patients voided urine after the fifth emission scan to reduce urinary bladder dose. X-ray CT transmission scans were performed twice, before the first and sixth emission scans, to correct for γ ray attenuation and to obtain the anatomical data required for drawing volumes of interest (VOI). The second CT scan was required, because we could not guarantee patient position after voiding is identical with before voiding.
All emission data were reconstructed using the 2D OSEM algorithm with four iterations and eight subsets after random, scatter, attenuation, and normalization corrections and data re-binning. Reconstructed images had dimensions of 256×256×165 with 2.67 mm transaxial pixel spacing and 5 mm axial slice interval.
The calibration factor required to convert pixel count rate on emission PET image to activity per volume (MBq/cc) was determined from a 68Ge/68Ga phantom study.
Data analysis
The VOIs of the nine different organs (gall bladder, heart, kidneys, liver, lungs, pancreas, spleen, stomach, and urinary bladder) were drawn to obtain their time-activity curves. VOIs were drawn on CT images for volume invariant organs (gallbladder, heart, kidneys, liver, lungs, pancreas, spleen, and stomach). VOIs drawn on CT images were transferred to eight serial PET emission images, and time-activity curves were obtained. However, since the volume of the urinary bladder increased with time, its VOI was drawn directly on emission PET images.
VOIs were drawn over entire organ volumes. 20,21 The mean activity per unit volume of sub-sampled VOI was not applied in this study, because average subject weight was significantly lower than the standard adult male and female model (73.7 and 56.9 kg) in OLINDA/EXM software (version 1.1, Vanderbilt University, 2007), which was used for dose calculation. 21,22 Furthermore, subject organ volumes were not identical with those of standard phantom models.
Residence times (normalized number of disintegrations) were calculated from time-activity curves. Cumulative activities were obtained by calculating areas under time-activity curves. The area under the curve of each time-activity curve was calculated as the trapezoid sum of observed data and the integral of physical decay for the curve tail after the last scan except the urinary bladder. 23,24 Residence times (hour) were obtained as the ratio of cumulative activity (MBq×hour) and injected dose to subject (MBq).
Time-activity curves of the urinary bladder showed a pattern unlike that of the other organs. Total urinary bladder activities continuously increased up to the final emission PET scan (62–87 minutes postinjection). Therefore, the assumption made regarding physical decay of the tail of the curve after the last scan was not appropriate for the urinary bladder, and special modeling of urinary activity was required. The whole-body retention curve of radiotracer was derived from activities in urinary bladder and voiding time (22 and 90 minutes) using dynamic bladder model of Thomas et al. 25 From the whole-body retention curve, time-activity curve and cumulative activity of urinary bladder were estimated.
In addition, the voiding cycle has to be taken into account to calculate residence time for the remainder of the body, because it is also an input parameter of OLINDA/EXM. If voiding urine is prohibited, total residence time (RT
total), which is the summation of residence times for all organs and the remainder of body, can be simply calculated using the following equation:
where A 0 is the initial activity of injected dose, and λ is the decay constant of the radioisotope. Total residence time is almost 1.443 times the half-life (T 1/2) of the radioisotope. On the other hand, if voiding urine is considered, total residence time cannot be obtained using the equation just cited, because excreted activities by voiding have to be subtracted. In this study, voiding excretion (“urine out” in Table 1) was taken into account to calculate residence times for the remainder of the body.
Number of patients in whom the organ could be identified.
%ID, percentage of injected dose.
The radiation dose to each organ, effective dose (ED), and effective dose equivalent (EDE) were calculated using individual organ residence times. These variables were also calculated using 1-hour and 1.5-hour voiding models.
Effective radiation dose estimation
The residence times obtained using the procedures just mentioned were used as input parameters for OLINDA/EXM 1.1 software. OLINDA/EXM 1.1 reports individual doses for 24–25 target organs and effective radiation doses (EDE and ED). Effective radiation doses are obtained using weighted sums of individual doses to each target organ. EDE was defined as in International Commission of Radiation Protection (ICRP) publication 26 (1977), and was calculated using weighting factors and doses to six major target organs and five remainder organs. The EDE was revised to ED as defined by ICRP publication 60 (1990), which used revised radiation detriment values and tissue weighting factors. In addition, the ED takes more organs into account than the EDE. Eleven major organs and 10 remainder organs were included to calculate EDE. These 2 effective radiation dose calculations were implemented in OLINDA/EXM 1.1 software.
Recently, new tissue weighting factors were introduced in ICRP publication 103 (2007). 26 In this publication, more organs are considered than in ICRP60, and the weighting factors of two critical organs were changed significantly (gonad 20%→8%, breast 5%→12%).
Although the ICRP103-defined ED is not implemented in OLINDA/EXM software, it can be calculated using tissue weighting factors and individual target doses. In this article, 3 types of effective radiation doses were estimated.
Results
Figure 1 shows the serial emission PET scan data of a patient. High accumulation of 68Ga-NOTA-RGD was observed on urinary excretion tracks (i.e., kidneys and the urinary bladder). The liver was also found to be a high accumulation organ in all time frames. Activity in the urinary bladder dropped after the 5th emission scan because of urine voiding.

Transmission and emission scan data set of a 49 year-old male subject. Two X-ray CT transmission scans were performed before the 1st and 6th emission PET scans. High accumulation of radiotracer was shown in the urinary bladder, kidneys, and liver. Activity in the urinary bladder dropped after the 5th emission scan because of urine voiding. The injected radiation dose of 68Ga-NOTA-RGD was 167.4 MBq. CT, computed tomography; PET, positron emission tomography.
Graphs of percentage of injected dose (%ID) versus time are shown in Figure 2 (uncorrected for radiation decay). As was expected, the %ID of urinary bladder dropped after voiding. Cumulative activity percentages and organ residence times are shown in Table 1, and as expected, high %ID values and residence times were shown for the urinary bladder, kidneys, and liver. The residence time of urinary bladder was much higher than those of other organs, even though a 2-hour voiding model was employed. About 10.8% of injected doses concentrated in the urinary bladder. In tumor lesion, the %ID per unit volume (liter) was comparable to the liver.
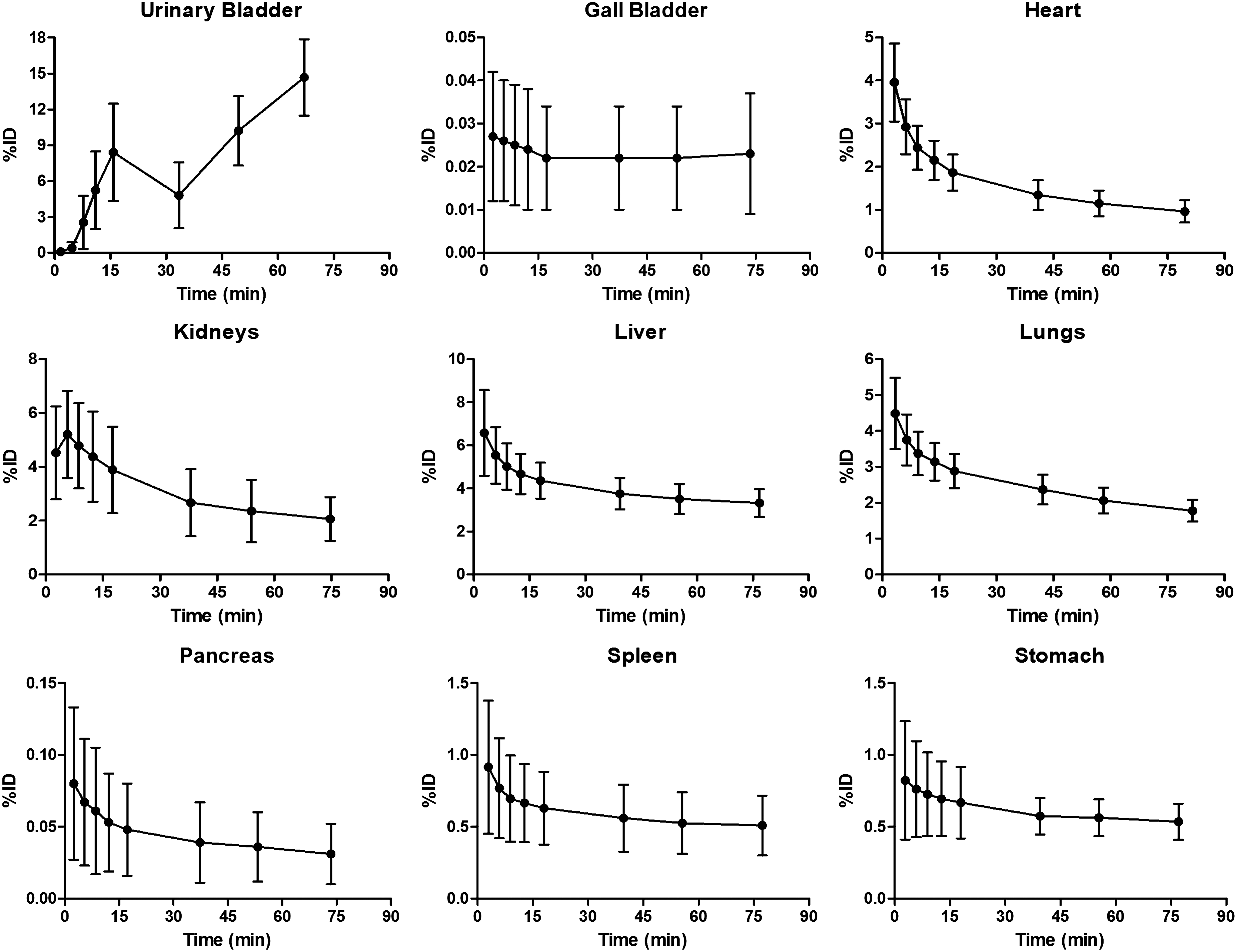
Graphs of percentage injected dose (%ID, mean±SD) versus time for the nine organs (uncorrected for radiation decay). The %ID of the urinary bladder dropped after the 5th scan. Those of all the other organs showed decreasing activity. SD, standard deviation.
The radiation doses absorbed by each organ, EDE by ICRP26, and ED by ICRP60 (all obtained using OLINDA/EXM 1.1 software), and ED by ICRP103 (calculated as the weighted sum of individual doses) are presented in Table 2. High radiation doses were reported for the urinary bladder wall (239.6±56.6 μGy/MBq) and kidneys (71.6±28.4 μGy/MBq). Mean EDE by ICRP26 and ED by ICRP60 and ICRP103 were 31.9±5.4 μSv/MBq, 25.0±4.4 μSv/MBq, and 22.4±3.8 μSv/MBq, respectively.
ED, effective dose; EDE, effective dose equivalent; ICRP, International Commission of Radiation Protection.
Residence times in urinary bladder, radiation doses to bladder walls, ED, and EDE values at various voiding frequencies after scans are listed in Table 3. More frequent voiding reduced radiation dose. The 1-hour voiding model yielded a 12.9% lower dose to the bladder wall, and a 6.6% lower ED (by ICRP60).
Discussion
68Ga labeled NOTA-RGD was a recently developed radiotracer for PET to visualize angiogenesis, and is a promising candidate for cancer imaging. 8,16,18 The aim of this study was to evaluate radiation dose exposure to humans who undergo a 68Ga-NOTA-RGD emission PET scan. In this study, radiation dosimetry of 68Ga-NOTA-RGD was examined in 10 human subjects who underwent eight serial emission PET scans of the upper body from the neck to the upper thigh to obtain the time-activity curves of nine anatomic organs. Absorbed doses were estimated using OLINDA/EXM 1.1 software.
In the present study, the predominance of renal excretion of 68Ga-NOTA-RGD observed in mice 16 was also confirmed in humans (Fig. 1). Activities in urinary bladder dropped considerably after voiding urine, which usefully reduced dose to the urinary bladder wall. The 6th scan data acquired after voiding was found to be useful for highlighting tumor regions because of the reduced urinary bladder activity. Although a 2-hour voiding model was primarily employed in this study to estimate residence time in the urinary bladder contents, our results (Table 3) also showed that more frequent voiding, such as, 1- or 1.5-hour voiding, helpfully reduced urinary bladder activity and radiation dose. Accordingly, frequent urine voiding is recommended to patients who undergo a PET scan with 68Ga-NOTA-RGD.
The activities in urinary bladder contents were found to be increasing at the end of our study (∼90 minutes). However, the time-activity curve of the urinary bladder could be derived using the dynamic bladder model of Thomas et al. 25 This model was useful to estimate excreted activities by voiding and residence time for the remainder of the body.
In a previous study, the whole-body distribution and radiation dosimetry of 18F-galacto-RGD was performed in human subjects, which also shows rapid clearance, primarily via the renal pathway. 14 The ED and dose to the urinary bladder wall of 18F-galacto-RGD were 18.7 μSv/MBq and 220 μGy/MBq, respectively. In the present study, 68Ga-NOTA-RGD showed equivalent to or slightly higher radiation dose than 18F-galacto-RGD (Tables 2 and 3). Although 68Ga-labeled radiotracers have considerably shorter physical half-lives than 18F-labeled radiotracers (67.63 vs. 109.8 minutes), this difference is balanced in terms of the radiation dose by the initial kinetic energy of positrons emitted (E max=1899 keV for 68Ga vs. 633 keV for 18F). However, it should be noted that different internal distributions of these radiotracers is another determinant factor of the radiation dose.
The ED values of other PET radiotracers recently reported in the literature are listed in Table 4, which shows that the ED of 68Ga-NOTA-RGD is comparable to those of other 68Ga-labeled radiotracers. 14,15,26 –34 The ED values of 68Ga-labeled radiotracers lie between those of 11C-labeled and 18F-labeled radiotracers. 11C-labeled radiotracers have significantly lower doses than 68Ga- and 18F-labeled radiotracers, due to the much shorter half-life of 11C (20.4 minutes). On the other hand, the ED difference between 68Ga- and 18F-labeled radiotracers is not large because of the balance between half-life and positron energy just mentioned.
According to ICRP103.
In this study, ED by ICRP publication 103 was calculated using the weighted sums of individual organ doses, and compared with ED by ICRP60. Renal excretion is a predominant feature for 68Ga-NOTA-RGD; therefore, the radiation dose to the urinary bladder wall was particularly high. The tissue weighting factor for the urinary bladder wall decreased from 5% for ICRP60 to 4% for ICRP103. That would be why the ED by ICRP103 was lower than that by ICRP60.
In the present study, we evaluated the radiation dosimetry of 68Ga labeled NOTA-RGD, which has an acceptable effective radiation dose. Furthermore, the ED of 68Ga-NOTA-RGD was comparable with those of other 68Ga-labeled tracers.
Footnotes
Acknowledgments
This work was supported by grants from the Atomic Energy R&D Program (2008-2003852, 2010-0026012) and the World Class University Program (R32-10142) through the Korean Science and Engineering Foundation funded by the Korean Ministry of Education, Science, and Technology and the Korean Healthcare Technology R&D Project (A070001) funded by Ministry of Health and Welfare, Republic of Korea.
Disclosure Statement
The authors declare that they have no conflict of interest.