
Abstract
The aim of this study was to develop new Lipiodol formulations with increased viscosities to augment Lipiodol embolic effect and optimize efficiency of radiolabeled Lipiodol in hepatocarcinoma treatments. New Lipiodol formulations consist of Lipiodol mixtures with different stearic acid concentrations (0.8%, 1.3%, and 1.8%). These formulations were fully characterized in vitro (viscosity, rheologic profiles) and labeled with 99mTc. Their viscosities at 20°C are 54, 60, and 67cP respectively, versus 45cP for Lipiodol ultra-fluide. Second, their biodistribution profiles were studied in vivo, at 24 and 72 hours, in hepatoma-bearing rats, and compared to control group (99mTc-Lipiodol). Biodistribution at 24 hours show a Gaussian tumor uptake profile with a maximum obtained with 1.3% stearic acid, and a tumor uptake superior to control group (+67%) (p<0.05). At 72 hours, optimal tumor uptake is reached with the 0.8% formulation, with 89% increase compared with control group (p<0.05). Moreover, we show a tendency to the decrease of pulmonary uptake for the new formulations at 24 hours and 72 hours. These results suggest a correlation between viscosity and Lipiodol tumor uptake. The new 0.8% stearic acid/Lipiodol formulation appears to be the optimized formulation for Lipiodol treatments of hepatocarcinoma, since it leads to a significant increase of tumor uptake at 72 hours and possibly to a decrease of undesirable pulmonary effects.
Introduction
Lipiodol® ultra-fluide, commonly named Lipiodol, is an oily mixture of polyunsaturated fatty acid esters, enriched in iodine that has the ability to selectively remain in hepatocarcinomas (HCC) when administered through the hepatic artery. 1 This enhanced retention may be explained by the fact that HCC is mainly irrigated through the hepatic artery, receiving no or little portal blood. After intra-arterial injection, Lipiodol has two major effects: first, it slows down arterial circulation, leading to a temporary embolic effect, 2 and second, it preferentially fixes on the tumor and penetrates in tumor cells. 3 These properties have been exploited for several years in the treatment of HCC, with trans-arterial chemoembolization and also with iodine-131 labeled Lipiodol radioembolization. Both these techniques have proven their efficacy but they need to be improved because HCC prognosis stays grim. Their main limitation is the variability of tumor uptake. And yet, it is proven that there is a relation between tumor uptake of Lipiodol formulations and their efficacy. 4,5 Optimization of Lipiodol tumor targeting is thus a lead to increase therapeutic efficacy of intra-arterial Lipiodol treatments.
Some studies having shown a significant increase of tumor uptake when viscosity of oils increased. 6,7 We postulated that an increase in Lipiodol viscosity would lead to an increase of its tumor retention and thus to the tumor absorbed dose with radiolabeled Lipiodol. The aim of this study was to increase the embolic effect of Lipiodol, to augment the time of contact with the tumor, to favor irradiation, and cellular penetration and thus to optimize therapeutic efficacy of Lipiodol based-treatments. To do this, we prepared new Lipiodol formulations with increased viscosity, and studied their biodistribution in hepatoma-bearing rats.
Materials and Methods
Preparation of new Lipiodol formulations labeled with 99mTc
A variety of oily preparations with different viscosities have been produced. They consist of Lipiodol (Lipiodol® ultra-fluide; Guerbet) mixtures with different stearic acid concentrations (ranging from 0% to 5%). The Lipiodol/stearic acid mixtures are heated at 65°C in a water bath, for 15 minutes, with stirring, until complete dissolution of stearic acid in Lipiodol. They are then cooled to room temperature.
A viscosimetric analysis at low and high shear speeds have been carried out at 20°C and 37°C, and results were compared to Lipiodol alone. The fluids stability was also checked.
After this study, three concentrations have been chosen to study their in vivo biodistribution: 0.8%, 1.3%, and 1.8%. Beyond (2.3%), viscosity was too high to be easily injected. The labeling of these Lipiodol/stearic acid formulations with 99mTc was done as previously described. 8
Animal tumor model
Experiments were performed on 55 female Sprague Dawley rats weighing 180–200 grams (Depré) in compliance with French regulations in force (law 0189.4 of 24th January, 1990). They were maintained in cages with corn-cob bedding, on 12 hours-light/12 hours-dark cycles and were given free access to rat food (Alphadry® SDS-Dietex) and tap water.
N1S1 cell line from Novikoff hepatocarcinoma in rat (purchased from ATCC in 2008) was used for tumor induction as previously described. 9 The rats were anesthetized with intra-peritoneal injection of 0.15 mL of xylazine (Rompun® 2%; Bayer) and 0.15 mL of ketamine (Ketalar® 1000; Vetoquinol).
A 1.5 to 2 cm-long sub-xiphoidian laparotomy was carried out, and the left hepatic lobe was exteriorized on a sterile compress. Then, 6×106 N1S1 cells in 0.15 mL DMEM were very slowly injected (30–40 seconds) with a 27 G1/2 needle (MicrolanceTM 3; BD) under the hepatic capsule. A gentle compression was then applied for 15 seconds with absorbent gauze composed of cotton and polyamide (B Braun) to avoid bleeding and reflux of the cells. The incision was closed up by two planes.
Arterial catheterization
Fourteen days after tumor inoculation, intra-arterial injection of Lipiodol formulations were carried out as previously described. 9 Volume and activity of each injected solution were 0.1 mL and 2.6 MBq.
Biodistribution studies
Biodistribution of the various 99mTc-labeled Lipiodol/stearic acid formulations have been studied at 24 and 72 hours, and compared to a control group injected with 99mTc-Lipiodol. Viscosity of tested formulations and number of rats per group are displayed on Table 1.
LUF, Lipiodol® ultra-fluide.
The rats were euthanized (anesthesia by xylazine and ketamine, then intracardiac injection with 0.1 mL KCl) 24 or 72 hours after injection of Lipiodol formulations. Tumor, liver, and lungs were then removed, their total activity being measured in a well counter (Auto gamma cobra II; Packard) and expressed as a percentage of the injected activity per gram of tissue (% IA/g).
The tumor-to-nontumor ratio has been calculated by dividing total activity in the tumor (expressed in% IA/g) by total activity in healthy liver (expressed in% IA/g).
Statistical analysis
Statistical analyses were performed with SPSS 13 (SPSS Inc.). Data are expressed as mean±SD. Multiple comparisons among the groups were performed using nonparametric Mann–Whitney test. An analysis of variance (ANOVA) test has been done to study the biodistribution of the different formulations between them. Differences are considered significant at p<0.05.
Results
In vitro study of the different Lipiodol/stearic acid formulations
The study realized at low shear speed shows that the more the stearic acid concentration increases, the more the representative curve of the stress according to the shear speed deviates from linearity (Fig. 1). Therefore, until 3.5% stearic acid, the fluid keeps its Newtonian character. Beyond, it loses its Newtonian character and becomes more and more rheofluidizing as the stearic acid concentration increases. Moreover, above 3.5% stearic acid, a variation of fluidity as a function of time has been observed (relaxivity measure), which is characteristic of thixotropic fluids.
Assessment of rheologic behavior of the Lipiodol/stearic acid system at 37°C, compared to Lipiodol alone.
Radiochemistry
Radiochemical purities (RCP) and labeling yields obtained for the different stearic acid concentrations are displayed in Table 2.
RCP, radiochemical purities.
Animal experiments
Eighty-five rats were inoculated with N1S1 cells; 62 tumors were observed at 14 days, that is, 73%, of which 55 were kept for study (89%) after catheterism. Weight of the tumor was 2.75±1.32 g (0.58–5.9 g).
Biodistribution of the new Lipiodol formulations at 24 hours, compared to control group tumor uptake at 24 hours
With the 0.8% stearic acid concentration, tumor uptake increased by 46% compared with control group (13.81±5.20%IA/g vs. 9.45±4.44%IA/g) but the difference is not statistically significant (p=0.124) (Fig. 2). On the contrary, there is a significant increase of tumor uptake with the 1.3% stearic acid concentration, with a mean fixation of 15.79±5.06%IA/g versus 9.45±4.44%IA/g (+67%) (p<0.05). With the 1.8% stearic acid concentration, there is a tendency to a decreased tumor uptake, without significant difference, compared with control group (7.96±4.22%IA/g vs. 9.45±4.44%IA/g).
Biodistribution at 24 hours for the different Lipiodol/stearic acid formulations in the liver, tumor, and lungs compared to control group (99mTc-Lipiodol alone). Results are expressed in percentage of injected activity per gram of tissue (mean and standard deviation). *p<0.05. Δ is the percentage of variation of tumor uptake compared to control group.
Hepatic and pulmonary uptakes at 24 hours
There is a significant decrease of hepatic uptake with the 0.8% stearic acid/Lipiodol formulation compared with Lipiodol alone (−26%) (p<0.05) (Fig. 2). For the other formulations with increased viscosity, no significant differences have been found compared to Lipiodol alone, even if there is a tendency to decreased hepatic uptake (−18% and −16% for 1.3% and 1.8% stearic acid respectively).
Concerning pulmonary uptake, a decrease has been shown for the formulations with increased viscosity (−30%, −14%, and −26%, with 0.8%, 1.3%, and 1.8% respectively), but it is not statistically significant.
Tumor-to-liver ratio at 24 hours
Compared with the control group, there is a significant increase of this ratio for the 0.8% and 1.3% concentrations of stearic acid, +81% and +85% respectively (p<0.05) (Fig. 3). For the 1.8% stearic acid concentration, no difference between this formulation and the control group has been shown (1.09±0.66 vs. 1.13±0.66).
Tumor-to-liver ratio at 24 hours for the different Lipiodol/stearic acid formulations compared to control group (99mTc-Lipiodol alone). *p<0.05. Δ is the percentage of variation compared to control group.
Comparison of biodistributions between the different formulations at 24 hours
An ANOVA test has been done to search for a biodistribution difference between the different Lipiodol formulations. There is a significant difference in tumor uptake for the 1.3% and 1.8%, with a mean tumor uptake of 15.79±5.06%IA/g versus 7.96±4.22%IA/g respectively (p<0.01). Other sites of uptake do not show any significant differences between the different formulations.
Biodistribution of the new Lipiodol formulations at 72 hours, compared to control group
Because of the low tumor uptake with the 1.8% stearic acid/Lipiodol formulation at 24 hours, the 0.8% and 1.3% formulations were the only ones studied at 72 hours.
Tumor uptake at 72 hours
There is a significant increase of the 0.8% stearic acid/Lipiodol tumor uptake, compared with Lipiodol alone, with a 14.13±4.44 versus 7.49±3.95%AI/g (+89%) (p<0.05) (Fig. 4).
Biodistribution at 72 hours for the 0.8 and 1.3% Lipiodol/stearic acid formulations in the liver, tumor and lungs compared to control group (99mTc-Lipiodol alone). Results are expressed in percentage of injected activity per gram of tissue (mean and standard deviation). *p<0.05. Δ is the percentage of variation of tumor uptake compared to control group
On the contrary, there is no significant difference in tumor uptake between Lipiodol alone and the 1.3% stearic acid concentration; even if, with that one, there is a 69% increase compared with control group (12.64±5.03 vs. 7.49±3.95%AI/g) (p=0.06).
Hepatic and pulmonary uptakes at 72 hours
There are no significant differences of hepatic and pulmonary uptakes between stearic acid/Lipiodol formulations and Lipiodol alone (Fig. 4). There is nonetheless a tendency to increased hepatic uptake (+35% and +15% for 0.8% and 1.3% concentrations respectively) and to decreased pulmonary uptake (−6% and −52% for 0.8% and 1.3% concentrations respectively) in comparison with control group.
Tumor-to-liver ratio at 72 hours
There are no significant differences between the three groups, but a tendency to an increase ratio for the formulation with increased viscosity (+26% and 25% for 0.8% and 1.3% concentrations respectively) (Fig. 5).
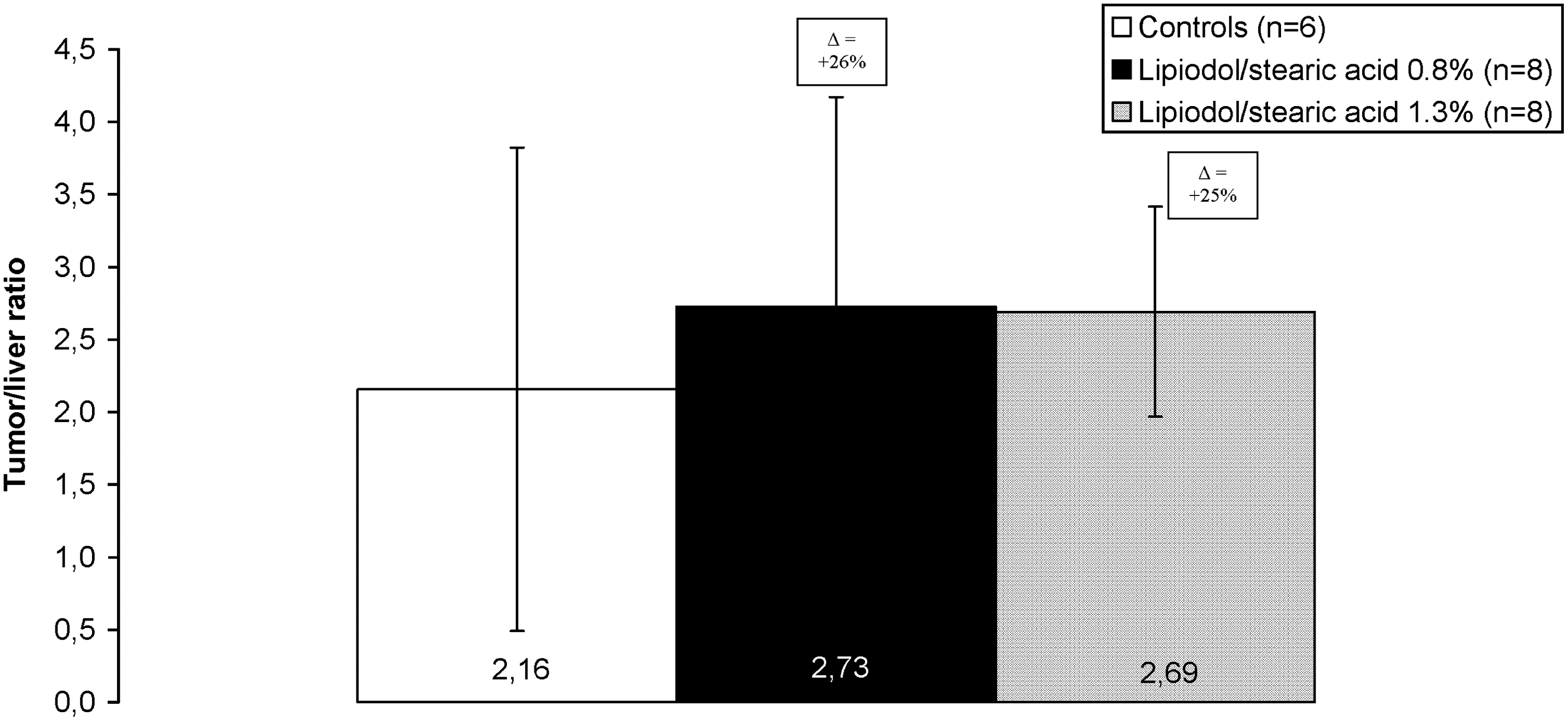
Tumor-to-liver ratio at 72 hours for the 0.8% and 1.3% Lipiodol/stearic acid formulations compared to control group (99mTc-Lipiodol alone). *p<0.05. Δ is the percentage of variation compared to control group.
Comparison of biodistributions between the different formulations at 72 hours
No significant differences have been shown between the different biodistributions, be it for tumor, liver, or pulmonary uptake and for tumor-to-liver ratio.
Comparison of biodistributions with time (24 and 72 hours)
At 72 hours, there is a significant decrease of hepatic uptake for control group and the 1.3% stearic acid/Lipiodol formulation, in comparison to uptake at 24 hours. Other sites of biodistribution (tumor, lungs) do not show any significant variations between 24 and 72 hours. With the 0.8% stearic acid/Lipiodol formulation, no significant difference in biodistribution has been identified between 24 and 72 hours.
Discussion
Embolic effects of Lipiodol have been widely investigated in vitro and in vivo. 3,10 –13 However, few studies looked at the consequence of modifying viscosity on embolic effect of Lipiodol. Lipiodol is often used in various formulations, especially in the form of emulsions. Indeed, when intra-arterially injected, Lipiodol is often mixed with other solutions, such as physiological serum, contrast agents, or anticancer drugs. These oil and aqueous mixtures always produce emulsions. Yet, little information is available on how to use these mixtures and authors scarcely describe the exact formulations. In fact, type (oil-in-water or water-in-oil), granulometry (droplet size) and proportions of each component are rarely described. Moreover, reproduction of emulsions is difficult to obtain because of the poor reproducibility of the three-way valve “back-and-forth” technique commonly used.
The main drawbacks of emulsions are their instability, with a non-Newtonian rheofluidizing type profile 14 (decrease of viscosity when shear speed increases) combined with the impossibility to prepare them at a patient's bed with radiolabeled Lipiodol, because of radioprotection constraints. Based on these major limitations, we chose to alter the chemical composition of Lipiodol to increase its viscosity.
To evaluate the embolic effect of a fluid, it is important to know whether there is a flow limit or not. Indeed, if a fluid is, for instance, of plastic type, shear stress can turn the fluid into solid at low pressure gradient. To determine the fluid's flow limit, a study at low shear speed must be done, which was the case in this work.
Our results show that adjunction of stearic acid does not alter the Newtonian profile of Lipiodol, until 3.5%. After that concentration, modified Lipiodol becomes rheofluidizing and viscosity decreases to an unstructured state. We chose to test stearic acid concentrations that enabled us to keep the Newtonian profile for the formulations, to obtain increasing viscosities and be freed from the rheofluidizing effect. Viscosities tested ranged from 54 to 67 cP at 20°C (or from 23.87 to 24.55 cP at 37°C) versus respectively 45 cP (and 23.36 cP) for Lipiodol ultra-fluide.
Injection of these new formulations, until 1.8% stearic acid, was not difficult, even through a small-diameter catheter. The 2.3% stearic acid formulation was too viscous to be injected (94 cP at 20°C). Incidentally, a strong increase of viscosity between 2% and 3% can be noticed on Figure 1. Moreover, replacement of Lipiodol by Lipiodol/stearic acid does not alter labeling, as can be attested by the excellent labeling yields and RCP observed (Table 2).
Even if the exact mechanism of Lipiodol retention in HCC is not completely elucidated, it is clear that tumor retention is due to retention difference between normal capillaries and neovessels. Tumorous neovessels have a muscular and nervous deficit, causing a flow variation in comparison with normal capillaries. In normal vessels, Lipiodol is rapidly eliminated, whereas it stays longer in neovessels.
Our study suggests that Lipiodol viscosity is an important factor in tumor distribution and retention. Indeed, at 24 hours, we can observe a significant increase of tumor uptake (p<0.05) for the 1.3% stearic acid formulation (viscosity of 24.2 cP) compared with Lipiodol alone (viscosity of 23.26 cP). Moreover, a profile of tumor uptake as a function of viscosity emerges, with an increase of tumor uptake in comparison with control group when viscosity increases up to 1.3% (+46% and +67% for 0.8% and 1.3% stearic acid respectively), followed by a decrease of tumor uptake with 1.8% stearic acid (−16%). The latter decrease could be explained by a too high embolic effect due to high viscosity, and thus a lesser penetration of Lipiodol in tumorous vessels.
At 72 hours, a 66%, nonsignificant, increase of tumor uptake for the 1.3% formulation is observed, in relation to that observed at 24 hours. On the contrary, the 0.8% formulation presents with a significantly superior uptake (p<0.05) compared with controls, with an 89% increase. These results suggest there is no late redistribution for the 1.3% formulation while there is for the 0.8% one, probably due to a passing from healthy liver to the tumor because of its mild embolic effect. The 1.3% formulation may present with a too high embolic effect and stays “blocked” in its initial biodistribution sites. As a result, biodistribution enabling an optimal tumor absorbed dose is reached with the 0.8% stearic acid concentration. These results are in accordance with literature, showing a correlation between tumor uptake and viscosity of the oily agents used. Natsume et al. 6 report a 6% IA/g tumor uptake at 24 hours, with a 120 cP viscosity (viscous ethyl oleate) versus a 2% IA/g at 4 cP (ethyl oleate) in rats. Biodistribution of Lipiodol ultra-fluide is not described.
Hamuro et al. 7 show a 14-day tumor uptake three to five times greater with a Lipiodol/triolein mixture (31.8 cP) compared with Lipiodol (23.26 cP) and to a low-viscosity fatty acids mixture (4.5 cP) respectively. In the same way, Oda et al. describe longer tumor retention at 7 days with Lipiodol fluide compared with Lipiodol ultra-fluide, whose viscosity is three times lower, in rabbits. 15 They also describe a decrease of the tumor size with Lipiodol fluide and not with Lipiodol ultra-fluide. However, if these authors show a correlation between viscosity and tumor uptake, only one viscosity higher than that of Lipiodol is tested and the optimal viscosity is not described for each oily preparation.
In our study, we show there is a correlation between viscosity and tumor uptake, which presents with a Gaussian profile, with a maximum in tumor uptake for 0.8% stearic acid at 72 hours. This correlation is also found in the tumor-to-liver ratio at 24 hours, as it increases from 1.13±0.66 for Lipiodol alone to 2.05±0.63 for Lipiodol/stearic acid 0.8% and 2.09±0.76 for Lipiodol/stearic acid 1.3% (p<0.05). It drops to 1.09±0.66 for Lipiodol/stearic acid 1.8%. This ratio also has a tendency to increase for the 0.8% and 1.3%, compared with control group, at 72 hours, but without significant differences (+33% et +29% respectively), probably because of a slower hepatic clearance of the formulations with increased viscosity. These results are interesting because there is, besides the increased tumor uptake, a significant decrease (p<0.05) of hepatic uptake of Lipiodol/stearic acid 0.8% at 24 hours, and, consequently, a limitation of undesirable effects on healthy liver parenchyma. Concerning pulmonary uptake, results are also encouraging since there is a trend toward decreased uptake for the formulations with increased viscosity. Even if there are no statistically significant differences, pulmonary uptake decreases by an average of 30%, 14%, and 26% compared with Lipiodol at 24 hours for, respectively, 0.8%, 1.3%, and 1.8% stearic acid concentrations, and by 6% and 52% at 72 hours for, respectively, 0.8% and 1.3% concentrations.
These results are in contradiction with that reported by De Baere et al., which show an increased pulmonary uptake for the emulsions prepared with Lipiodol fluide compared with that with Lipiodol ultra-fluide. 16 A possible explanation may be that these emulsions are non-Newtonian fluids and the authors did not precise their viscosities for low shear speeds. Demachi et al. studied the same emulsions in vitro and show they are plastic fluids with a strong embolic effect at low pressure gradient. 13 However, they noticed a decrease of the viscosity at 1 hour due to the instability of these emulsions. The increased pulmonary uptake observed at 4 days by De Baere et al. could be the result of the emulsions decreased viscosity. Other studies evaluating the effect of viscosity on biodistribution did not describe pulmonary uptake.
Besides, we report lungs/lungs+liver ratios at 24 and 72 hours of 21% and 37% for Lipiodol alone, 21% and 29% for the 0.8% stearic acid concentration, and 22% and 19% for the 1.3% concentration. Results are in accordance with data on Lipiodol biodistribution, since it is known that Lipiodol redistribution in lungs increases with time. 17 –19 However, this ratio increases less for the 0.8% formulation, and even decreases at 72 hours for the 1.3% formulation. This probably reflects a decrease of the secondary Lipiodol release from liver to lungs because of the inability of these new formulations to go through arterio-veinous shunts due to their high viscosity.
In summary, these results suggest that the new 0.8% stearic acid/Lipiodol formulation appears to be the formulation of choice to optimize Lipiodol treatments for HCC, since it leads to a significant increase of tumor uptake at 72 hours and possibly to a decrease of pulmonary and hepatic secondary effects. These results also show that a slight increase of viscosity (+2.2% at 37°C) enables an increase of tumor uptake of 89%, leading to a significant increase of the absorbed dose from radiolabeled Lipiodol.
Footnotes
Disclosure Statement
No competing financial interests exist.