
Abstract
Our objectives were to automate radiolabeling of therapeutic activities for safe, reliable, cost-effective, practical routine preparation of 177Lu-radiopeptides, 131I radioimmunotherapeutic agents, and 68Ga-peptide PET diagnostics and, in particular, minimize radiation exposure to the radiopharmaceutical chemist. Reprogramming and adaptation of a commercially available synthetic module (IBA molecular; Synthera®) allowed high yield, fully automated, in-house radiolabeling of novel therapeutic and diagnostic radiopharmaceuticals under remote shielded sterile conditions. Radiochemical yield and purity was measured by instant thin-layer chromatography and high-performance liquid chromatography. 68Ga-octreotate and 177Lu-octreotate were synthesized, resulting in both radiochemical yield and radiochemical purity greater than 99%. Synthesis of 131I-rituximab resulted in a yield of 60%, with a radiochemical purity greater than 99%. Using 400 MBq 68GaCl3 per synthesis, the estimated absorbed body and hand dose for a manual synthesis was 2 and 27 μSv, contrasting with automated synthesis exposure of 1.3 and 7.9 μSv. Using 8000 MBq 177LuCl3 per synthesis, the estimated absorbed body and hand dose for a manual synthesis was 44.7 and 75 μSv, contrasting with automated synthesis exposure of 2.5 and 20 μSv. Using 6000 MBq 131I per synthesis, the estimated absorbed body and hand dose for a manual synthesis was 83.7 and 335 μSv, contrasting with automated synthesis exposure of 10.9 and 54.7 μSv. The reduction in radiation exposure by automated synthesis of radiopharmaceuticals in the Synthera® module was at least five fold. Automated synthesis of therapeutic 177Lu and 131I radiopharmaceuticals and 68Ga PET agents in the shielded sterile Synthera® module is simple, practical, and efficient and virtually eliminates radiation exposure to the radiopharmaceutical chemist.
Introduction
The continuing rapid development of therapeutic nuclear oncology with the advent of novel radioimmunotherapy and radiopeptide treatment of metastatic cancer is dependent upon practical, affordable, and safe provision of therapeutic activities of targeted radiopharmaceuticals.
Safety not only requires good manufacturing practice and standard operating procedures to ensure sterility and purity of the radiopharmaceutical, but also incorporates radiation protection of the radiopharmaceutical chemist during manufacture, quality control, and dispensing.
Typical activities of radiopharmaceuticals prepared for therapeutic applications are in the range 10–50 GBq, which require special remote shielded manipulation to avoid radiation exposure, particularly to fingers of the radiopharmacist. The radiolabeling of monoclonal antibody proteins and peptides for targeted tumor therapy with high activities in relatively small volumes inevitably causes radiolysis which is minimized by in-house preparation of each radiopharmaceutical immediately before administration to the patient. Such customized on-site radiolabeling is cost-effective and reliable, given that delivery of the therapy radionuclides Iodine-131 and Lutetium-177 from a reactor is elective and PET diagnostic Gallium-68 is available daily from an in-house Germanium-68 generator.
In our 10 year experience of 131I-rituximab radioimmunotherapy of non-Hodgkin lymphoma 1 and 177Lu-octreotate radiopeptide therapy of neuroendocrine tumors 2 we have progressed from manual radiolabeling 3 through semiautomated methodology to the current fully automated synthesis achieved by reprogramming a commercially available module as described in this paper. This methodology is now also routinely applied in our hospital to synthesize 68Ga peptides for PET diagnostic imaging.
Materials and Methods
Automated module
A standard commercially available synthetic module, designed for preparation of 18 F-FDG (IBA molecular; Synthera® module), was adapted by reprogramming to allow automated synthesis of gallium-68, lutetium-177, and iodine-131 radiopharmaceuticals according to purpose written script files for each radiolabeling.
The associated sterile single use cassette (Integrated Fluidic Processor, IFP™, ABX) was used for sequential syntheses of each radiopharmaceutical on the automated module. Following completion of each radiolabeling, the cassette was dropped from the module into a shielded bin. The entire synthesis was performed in a lead-shielded cell.
68Ga-DOTA-Tyr3-octreotate
Gallium-68 was obtained from a tin-dioxide-based 68Ge/68Ga generator (IDB) as 68GaCl4, 68Ga (T 1/2= 68 minutes) being continuously produced by decay of its radioactive parent 68Ge (T 1/2= 270.8 days). Elution of the generator was performed in a shielded workstation with 0.6 M HCl Suprapure (Sigma—Aldrich). A Teflon tube was inserted into the eluate vial for transfer of the 68GaCl4 to the reaction vial within the Synthera® module.
Radiolabeling was remotely performed within the shielded, sterile module according to the general method described by Breeman et al. 4 Briefly, sodium acetate 2.5 M was used to adjust the pH of the 68GaCl4 eluate to 3.0–4.0. DOTA- Tyr3- octreotate, synthesized and supplied as a lyophilized powder in sterile vials by Auspep, was then added as a 20–30 nmol solution. After heating for 10 minutes at 98°C, 10 μL 4 mM EDTA (Sigma—Aldrich) was added (Fig. 1).
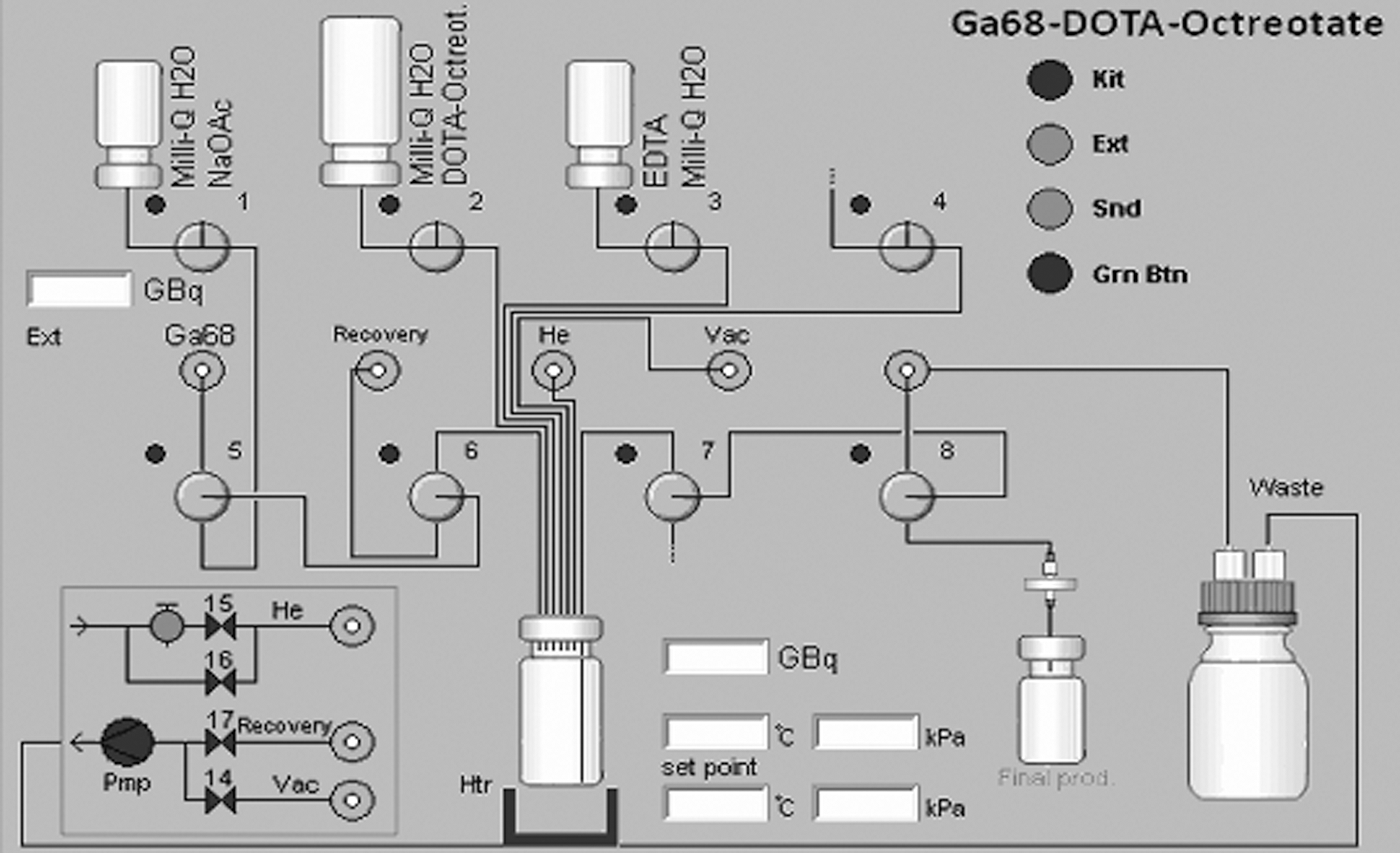
68Ga-DOTA-Tyr3-octreotate flowchart of the Synthera® module showing vials 1 (sodium acetate), 2 (DOTA-octreotate), and 3 (EDTA) mounted on the disposable, sterile cassette.
The radiolabeled product was transferred to a sterile vial after end filtration using a 0.2 μm filter (Acrodisc 0.2 μm; Pall).Radiochemical yield and purity was determined by ITLC-SG in a sodium citrate buffer 0.1 M pH 5.5.
HPLC quality control analysis was performed (Shimadzu). A reversed phase column C18, 5 μm, 4.6×250 mm (Grace) was used as stationary phase with a solvent system of 0.1% trifluoroacetic acid (TFA) in H2O (solvent A) and 0.1% TFA in acetonitrile (solvent B) in a gradient protocol; 0–10 minutes 18%–60% solvent B, 10–12 minutes 60% solvent B. The flow-rate was 0.6 mL/min.
177Lu-DOTA-Tyr3-octreotate
Lutetium-177 trichloride was supplied by IDB Holland. Radiolabeling of DOTA-Tyr3-octreotate was performed by adding 400 μg peptide to the 177LuCl3 (10–50 GBq), followed by heating for 30 minutes at 98°C. After heating l ml EDTA (4 mg/mL) was added and the solution was transferred to a sterile vial after end filtration using a 0.22 μm filter (Fig. 2). Radiochemical yield and purity was performed by ITLC-SG in a sodium citrate buffer 0.1 M pH 5.5.
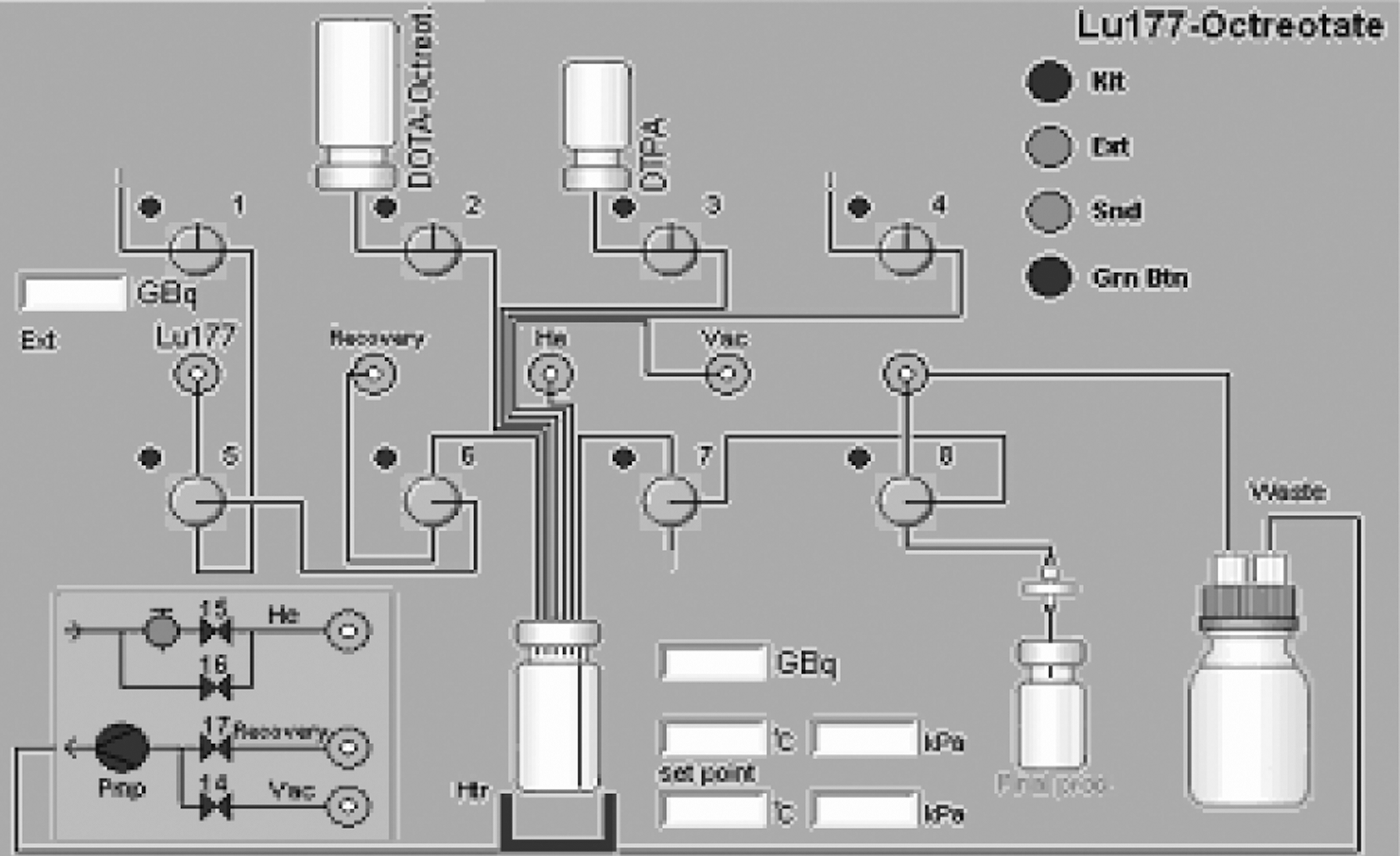
177Lu-DOTA-Tyr3-octreotate flowchart of the Synthera® module showing vials 2 (DOTA-octreotate) and 3 (DTPA) mounted on the disposable, sterile cassette.
HPLC quality control analysis was performed (Shimadzu). A reversed phase C18 column 5 μm, 4.6×250 mm (Grace) was used as stationary phase with a solvent system of 0.1% TFA in H2O (solvent A) and 0.1% TFA in acetonitrile (solvent B) in a gradient protocol; 0–10 minutes 100% solvent A, 10–40 minutes a linear gradient from 5% B to 90% B. The flow-rate was 0.6 mL/min.
131I-rituximab
Unstabilized sodium 131I iodide was supplied by Ansto Health.
Radiolabeling of rituximab was performed using a chloramine-T method. 3 Purification of the radiolabeled product was done on a Pd-10 column (Sephadec G-25; GE Healthcare). The radiolabeled product was transferred to a sterile vial after end filtration using a 0.22 μm filter (Fig. 3).

131I-rituxmab flowchart of the Synthera® module showing vials 2 (rituximab+chloramine-T), 3 (sodium thiosulfate), and 4 (PBS) and Pd-10 column mounted on the disposable, sterile cassette.
Radiochemical yield and purity was performed by ITLC-SG in 85% methanol.
HPLC analysis was performed on a Shimadzu HPLC system. A macrosphere column (7 μm, 7.5×300 mm; Alltech) was used as stationary phase with sodium phosphate 0.05 M pH 6.75 as a solvent. The flow-rate was 1.0 mL/min.
Radiation exposure
For each radiolabeling radiation exposure was measured for manual, semiautomated, and automated syntheses. Absorbed body and hand doses were estimated using a thermoluminiscent dosimeter (ARPANSA) and electronic personal dosimeters (Aloka PDM-192; Hitachi Aloka Medical Ltd.).
Results
68Ga-DOTA-Tyr3-octreotate
68Ga-DOTA-Tyr3-octreotate was obtained with radiochemical purity greater than 95% for both manual and automated synthesis. The overall nondecay-corrected yield was 56.1%±6.2%. Using 400 MBq 68GaCl3 per synthesis, the estimated radiation absorbed whole body and hand dose for a manual synthesis was 2 and 27 μSv respectively, in comparison with exposures of 1.3 and 7.9 μSv, recorded during automated synthesis and dispensing.
177Lu-DOTA-Tyr3-octreotate
177Lu-DOTA-Tyr3-octreotate was obtained with a radiochemical yield and purity greater than 95%, for both manual and automated syntheses. Using 8000 MBq 177LuCl3 per synthesis, the estimated radiation absorbed whole body and hand dose for a manual synthesis was 44.7 and 75 μSv, in comparison with exposures of 2.5 and 20 μSv, recorded during automated synthesis and dispensing.
131I-rituximab
131I-rituximab was obtained with a radiochemical yield of 60% and purity greater than 95% after purification on a Pd-10 column. Using 6000 MBq 131I per synthesis, the estimated absorbed whole body and hand dose for a manual synthesis was 83.75 and 335 μSv, in comparison with exposures of 10.95 and 54.75 μSv, recorded during automated synthesis and dispensing.
Discussion
The practice of therapeutic nuclear medicine has undergone a renaissance with the advent of novel tumor-targeted radiopharmaceuticals which may be manufactured in hospital radiopharmacies for customized radionuclide therapy of cancer patients. The efficacy and safety of such innovative personalized approaches to the control of disseminated cancer, such as radiopeptide therapy of neuroendocrine tumor with 177Lu-octreotate, has been demonstrated over the past 10 years. 5 However, such advances in radionuclide therapy have been often made without formal development of approved agents by pharma industry and in the case of radiopeptide therapy, no randomized controlled clinical trials have been performed. 6
Clinical evaluation of radiopeptide therapy of neuroendocrine tumors and other cancers thus depends upon multicenter physician-sponsored studies, performed within funding and regulatory agency constraints. Thus the ability to prepare affordable, safe, effective therapeutic radiopharmaceuticals on-site in existing radiopharmacies in hospital Nuclear Medicine departments is a prerequisite for the clinical application of novel targeted nuclear medicine therapy. 7
Many Nuclear Medicine departments offer a PET diagnostic service based upon 18 F-FDG prepared in a commercially available synthetic module, of which the IBA Synthera® is but one example. We have reprogrammed the basic Synthera® module simply by writing an individual script file for automated synthesis of each desired therapeutic radiopharmaceutical and PET diagnostic agent, and have accordingly adapted the standard single use sterile cassette system.
Manual handling of high amounts of radioactivity of 68GaCl3 results in a high finger-dose exposure. For routine production of 68Ga-DOTA-Tyr3-octreotate, the automated method resulted in a significant decrease of radiation absorbed dose to the operator. Further, an increase of the overall yield was observed, due to shorter synthesis time. The use of a cassette system makes it also possible to make adjustments to the synthesis, such as buffers, 8 in line prepurification of 68GaCl3 9,10 type of chelator 11,12 or peptide 13,14 to optimize yields and purity.
The amount of DOTA-Tyr3-octreotate required for 100% incorporation of lutetium-177 into the peptide increases with time from production of 177LuCl3. 7 Given the relatively long transit time of 177LuCl3 to Australia from Holland, we used a higher fixed amount of 400 μg than the standard 250 μg used for the same peptide in Europe. Clinical results of the lower specific activity 177Lu-octreotate are however comparable. 2,5
Mainstream clinical use of anti-CD20 monoclonal antibody radioimmunotherapy of non-Hodgkin lymphoma has been constrained by perceived lack of affordability and practicality. 15,16 However, the imminent availability of generic anti CD20 Mabs is expected to significantly lower costs and a safe, practical automated radiolabeling system for 131I-rituximab will provide widespread access to radioimmunotherapy of non-Hodgkin lymphoma throughout developing countries. Similarly the same module may be programmed for synthesis of 177Lu-rituximab 17,18 where local reactor-produced 177LuCl3 may be more cost-effective.
Ready availability of high-yield, radiochemically pure, clinical grade tumor-targeted therapeutic radiopharmaceuticals in-house facilitates research and development of personalized radionuclide treatment of cancer. Serial labeling of several radiopharmaceuticals on the same day, using the fully automated synthetic module does not expose the manufacturing radiopharmaceutical chemist to significant radiation exposure, which was a limiting factor when therapeutic radiopharmaceuticals were manually prepared.
Conclusions
The automated modular synthesis of therapeutic and PET diagnostic tumor-targeted agents is reliable, rapid and remotely controlled to achieve reproducible, quality-controlled, high-yield radiopharmaceuticals without radiation exposure to the laboratory staff and may be recommended as the standard operating procedure for preparation of radiopharmaceuticals for nuclear oncology.
Footnotes
Acknowledgments
The authors wish to thank Dr. Richard Zimmermann, Vice President Radiopharmaceutical Business Development iba Molecular for kind provision of the Synthera® module and Rony Boumon for valued advice and guidance in programme development for radiopharmaceutical synthesis. Manuscript preparation by Ms. Jenny Lavin is gratefully acknowledged.
Disclosure Statement
The authors disclose that there are no financial or other conflicting interests in this work.