
Abstract
Aim:
Fractionation is generally used as a mean to improve radioimmunotherapy (RIT). Since RIT is considered suitable for small-volume disease, the aim of the current study was to investigate whether repeated administration of 177Lu-labeled mAb BR96 was tolerated and could delay or prevent metastatic disease after complete remission of the tumor obtained by the first administration.
Methods:
Immunocompetent rats bearing a syngeneic colon carcinoma were first treated with 400 MBq/kg 177Lu-DOTA-BR96, an activity resulting in complete response in 29 of 30 animals. On day 21, two groups of rats were given an additional activity of 150 or 350 MBq/kg resulting in total administered activities corresponding to 0.9 and 1.3 times the maximal tolerated dose.
Results:
The additional treatment resulted in tolerable myelotoxicity; however, the frequency of metastatic disease and survival were not affected. Immunohistochemistry demonstrated binding of the BR96 antibody to tissue sections of analyzed metastases.
Conclusions:
In our model, development of metastatic disease after treatment of the manifest tumor was not prevented by an additional treatment with the same radioimmunoconjugate. Therefore, the antibody should be labeled with a more suitable radionuclide for treatment of metastases. The repeated targeted therapy was well tolerated in aspects of myelotoxicity.
Introduction
Fractionated radioimmunotherapy (RIT) is used to increase the total amount of activity that can be administered without reaching dose-limiting toxicity (DLT), and to improve the homogeneity of the distribution of radioimmunoconjugates in the tumor. 1 Fractionated RIT has been successful in the treatment of B-cell lymphomas, 2 –5 and studies on RIT of colon carcinoma in xenografted mouse models have also indicated that fractionation is beneficial. 6,7 A phase I study of the 177Lu-labeled mAb J591 for the treatment of prostate cancer showed that fractionation increased the tolerated dose, but the therapeutic benefits of fractionation were not evaluated. 8
In a previous study, we treated rats bearing a syngeneic colon carcinoma with a single administration of the maximal tolerable dose (MTD) of a 177Lu-labeled antibody, which resulted in complete response (CR) of the manifest tumors, but metastases subsequently developed in half of the animals. 9 In the clinic, treatment of the primary tumor with standard therapies is often successful; instead metastatic disease is responsible for 90% of cancer-related mortality. 10 Thus, there is a need for consolidation treatment to prevent or delay the development of metastatic disease. RIT is considered a suitable mode of treatment for small-volume disease, 11 and 177Lu-labeled antibodies have been evaluated in studies for the treatment of metastases of colon carcinoma 12 –14 and lymphoma. 15
The aim of the current study was to investigate whether repeated administration of 177Lu-labeled antibodies was tolerated, and whether the consolidation therapy could delay or prevent the development of distant metastatic disease. The study was conducted in two parts. We first determined the minimal effective dose of 177Lu-DOTA-BR96, defined as the lowest single administered activity (MBq/kg body weight) resulting in CR in 5 of 6 rats. In the second part of the study, rats were first treated with this minimal effective dose, followed by a second treatment with two different activities of the same radioimmunoconjugate. The treatment strategy, with induction of CR by the first administration and metastatic disease as the main target of the second administration of RIT, differs from the application of fractionation schedules investigated by others, which focus mainly on rejection and recurrence of a local tumor.
Materials and Methods
Monoclonal antibody
The chimeric (mouse/human) monoclonal IgG1 antibody BR96 (Seattle Genetics, Inc.), binding the tumor-associated Ley, was used. Ley is expressed on the majority of human epithelial tumors, including breast, gastrointestinal, pancreatic, nonsmall-cell lung, cervical, and ovarian cancers, as well as some melanomas. As with the majority of tumor-targeting mAbs, BR96 also reacts with several normal tissues, primarily the epithelial cells of the gastrointestinal tract. 16 The binding affinity of BR96 to the BN7005 cell line is high. The dissociation constant determined by saturation binding curve analysis was found to be 4 nM (see below under radioimmunoconjugate section).
The radioimmunoconjugate
BR96 was conjugated with the DOTA-chelate [S-2-(4-isothiocyanatobenzyl)-1,4,7,10-tetraazacyclododecane tetraacetic acid; Macrocyclics] according to the method described by Forrer et al. 17 Briefly, the antibody was transferred to 0.2 M sodium carbonate buffer, pH 9.5, by repeated centrifugation using an Amicon-15 filter (Millipore; 30,000 MWCO). The DOTA-chelate (2 mg/mL H2O) was added to the BR96 antibody (100 mg/mL) at a molar ratio of 3:1 (DOTA:IgG), and incubated for 1 hour at 37°C. The conjugate was transferred to 0.25 M ammonium acetate buffer, pH 5.3, by repeated centrifugation using an Amicon-15 filter. The final concentration was adjusted to 10 mg/mL BR96. All buffers were pretreated with chelex-100 (BioRad), and all vials were pretreated with 1% HNO3 to remove metals.
The number of DOTA moieties per BR96 molecule was determined by matrix-assisted laser desorption ionization mass spectroscopy measurements. The sample was desalted to 18 MΩ·cm H2O using a centrifugation filter device. The number of DOTA moieties per BR96 molecule was obtained by dividing the increase in molecular mass by 688 (molecular mass of p-SCN-Bn-DOTA).
The antigen binding properties (immunoreactivity) of DOTA-BR96 relative to BR96 were determined by saturation binding curve analysis, using BN7005 cells as the target antigen. Briefly, increasing concentrations of DOTA-BR96 and BR96 (40 ng/mL–40 μg/mL) were added to the cell plate in triplicates. After incubation at room temperature for at least 1½ hours, the bound DOTA-BR96/BR96 was detected by HRP-antihuman-IgG (Dako), and the equilibrium binding constant (K d) was calculated utilizing Prism 5.02 software (binding saturation–one site total, nonspecific binding and background constrained to a constant value of zero). The immunoreactivity is given by the ratio: K d(BR96)/K d(DOTA-BR96).
The following procedure was used for labeling with 177LuCl3 (MDS Nordion). Both the DOTA-BR96 conjugate in 0.25 M ammonium acetate buffer and the radionuclide solution were preheated to 45°C for 10 minutes. The DOTA-BR96 solution was then added to the radionuclide-containing vial and incubated at 45°C for 15 minutes. The reaction was quenched with an excess of diethylene triamine pentaacetic acid (DTPA) for 5 minutes. The radiolabeled immunoconjugate was then diluted in 1% human serum albumin (HSA; Baxter Medical AB). The radiochemical purity of the labeled immunoconjugate was determined by instant thin-layer chromatography (ITLC) using 1×9 cm silica gel–impregnated fiberglass sheet, eluted in 0.1 M ethylene diamine tetraacetic acid (EDTA). Separation by size-exclusion chromatography together with high-performance liquid chromatography (HPLC) (7.8×300 mm molecular sieving column, Phenomenex SEC S3000; Phenomenex, eluted in 0.05 M sodium phosphate at 1.0 mL/min) was used to determine the radiochemical purity and to detect signs of aggregation or fragmentation.
Rat tumor model
Sixty male Brown Norway (BN) rats (Harlan) with a mean body weight of 225 g [standard deviation (SD) 18 g] were used. These animals are immunocompetent and express the BR96 antigen in some normal tissues, mainly in the epithelium of the gastrointestinal tract, 18 hence mimicking the human situation. The animals were housed under standard conditions and fed with standard pellets and fresh water, ad libitum. All experiments were conducted in compliance with Swedish legislation on animal rights and protection, and were approved by the regional animal ethics committee.
BN7005-H1D2 is a cell line established from a 1,2-dimethylhydrazine–induced BN rat colon carcinoma. The radiosensitivity, determined as the fraction of survival after 2 Gy (S2Gy), was 0.5 for this cell line (data not published), which is similar to human colorectal cell lines. 19 The cells were cultured in RPMI-1640 medium (PAA Laboratories GmbH) supplemented with 10% fetal calf serum (PAA Laboratories), 1 mM sodium pyruvate (Gibco, Invitrogen), 10 mM HEPES buffer (Gibco), and 14 mg/mL Gentamicin (Gibco) at 37°C, in a humidified environment containing 5% CO2. Cells were washed in phosphate-buffered saline, detached by trypsin treatment, and washed in medium with supplements. The animals were subperitoneally inoculated with 3×105 cells under anesthesia (Isoflurane; Abbott Scandinavia AB). Treatment with radiolabeled BR96 was started 13–14 days after tumor inoculation. Tumor volumes were calculated as tumor length×tumor width 2 ×0.4. CR was defined as a nonpalpable tumor for at least one week.
Determination of the minimal effective dose
The MTD, defined as 100% survival without clinical signs of toxicity, has previously been determined to be 600 MBq/kg and resulted in CR in 6 of 6 animals. 9 In the current study, the minimal effective dose was determined by the administration of different activities of 177Lu-DOTA-BR96. Thirty rats were allocated into 5 groups of 6 to receive comparable tumor size distribution, and given activities of 60, 135, 270, or 400 MBq/kg 177Lu-DOTA-BR96, or 150 μg unlabeled DOTA-BR96. All groups of rats treated with the radioimmunoconjugate were given 150 μg 177Lu-DOTA-BR96. The minimal effective dose was defined as the activity resulting in CR in 5 of the 6 rats in the group, and was determined to be 400 MBq/kg (see Table 1).
The minimal effective dose was defined as CR in 5 of 6 animals in one group (i.e., 400 MBq/kg).
CR, complete response.
Repeated therapy with 177Lu-DOTA-BR96
To study the effects of repeated RIT, 30 animals were divided into 3 groups (10 rats/group) with similar distributions of body weight and tumor volumes. All groups were given the minimal effective dose of 400 MBq/kg 177Lu-DOTA-BR96 (150 μg DOTA-BR96 in 0.4 mL saline with 1% HSA) on day 0. Group 1 was not given any additional treatment, while Groups 2 and 3 were given a second administration of 177Lu-DOTA-BR96 and Cyclosporin A (Sandimmun®; Novartis). The Cyclosporin A treatment (0.2 mL, 10 mg/kg body weight, in saline) was given daily for 5 days starting 1 day before the first injection of radiolabeled BR96 to prevent development of antibodies against the radioimmunoconjugate, as described by Eriksson et al. (manuscript under preparation). The second treatment with 177Lu-DOTA-BR96 was administered on day 21 when the number of white blood cells had started to recover in our previous studies. Group 2 was given 150 MBq/kg, resulting in a total administered activity of 0.9×MTD, and Group 3 was given 350 MBq/kg, resulting in a total administered activity of 1.3×MTD. All therapeutics were administered via a tail vein. The successful injection of 177Lu-DOTA-BR96 was verified by activity measurements of arterial blood samples drawn from the tail a few minutes after injection. All injections were based on the average body weight.
Monitoring of treatment effects
Animals were monitored up to 119 days after the first administration of 177Lu-DOTA-BR96 (day 0). The follow-up time was based on the results of a previous study in which treated rats were followed up to 180 days after treatment, and all metastases were detected before day 100. 9 Body weight was recorded, and the diameters of the inoculated tumors were measured with a digital caliper twice a week (all measurements were performed by the same investigator). After RIT, the largest change in body weight after injection was calculated compared with the day of administration (day 0 and day 21, respectively). Arterial blood sampling was performed twice a week for the first 7 weeks and then once a week. Myelotoxicity was determined by counting the white blood cells and platelets with a Vet CA530 Medonic Cell Analyzer (Boule Medical).
Rats were sacrificed if the maximal tumor size of 25×25 mm was exceeded, if body weight decreased >20% compared with normal weight progression, if the general health of the animal was affected, or at the end of the study (day 119). At the time of sacrifice, all rats were dissected by the same person, in a similar way, and the number of metastatic sites was noted. Tumor findings were fixed in 4% paraformaldehyde and embedded in paraffin.
Immunohistochemistry
Paraffin-embedded tumors and metastases were sectioned and stained for detection of the BR96 target antigen. Briefly, 4-μm-thick sections were rehydrated and antigen retrieval was performed using the PT Link pretreatment module (Dako) with acidic target retrieval solution (pH 6), preheated to 65°C and heated to 99°C for 20 minutes, followed by rinsing of the slides. Sections were incubated with 5 μg/mL BR96 in Antibody dilutent (Dako) overnight at room temperature. After washing, sections were incubated with antihuman IgG H+L donkey F(ab)2 HRP (Jackson ImmunoResearch Laboratories, Inc.) in Antibody dilutent for 3 hours at room temperature. Finally, diaminobenzidine (Dako) was added before dehydration and mounting.
Statistical analysis
Statistical analysis of experimental data was conducted utilizing Prism, vers. 5.02 (GraphPad Software, Inc.).
Results
Radioimmunoconjugate
The molecular weights of BR96 and DOTA-BR96 were determined to be 149,202 and 150,800, respectively. The increase in molecular mass, 1,596, was divided by 688 (molecular mass of p-SCN-Bn-DOTA) giving 2.32 DOTA moieties per BR96 molecule. The immunoreactivity, expressed as the ratio of the K d for BR96 and DOTA-BR96, was found to be 0.90. The K d of DOTA-BR96 was within the 95% confidence interval for the K d of BR96.
After radiolabeling, the specific activity of the 177Lu-DOTA-BR96 conjugate was 695 and 571 MBq/mg on the first and second labeling occasions (day 0 and day 21). ITLC showed the radiochemical purity to be 99% on both occasions. No aggregation or fragmentation was observed with HPLC.
Toxicity
After the first administration of radiolabeled BR96 (400 MBq/kg), the mean weight loss was 6% (range 2%–10%) (Groups 1–3; day 3 compared with day 0), with a nadir on day 3 (no significant differences were seen between the groups) (Fig. 1). Three days after the second administration, Group 2 showed a weight gain of 1% (range −1%–2%), while a small weight loss was seen in Group 3 (−1%, range −3%–1%) (day 24 compared with day 21). Group 1, not given further treatment, showed a weight gain of 3% (range: 2%–5%). The effect on body weight after the second injection was significantly lower than the first injection (p<0.0001, Kruskal–Wallis test). Later in the study, 4 rats had lost ∼20% of their body weight (compared with normal weight progression): 2 rats in Group 2 (sacrificed at the end of the study [day 119]) and 2 rats in Group 3 (sacrificed on day 91). Three of these rats were free from detectable disease at autopsy, while one (from Group 3) had metastases in the mesentery and the abdomen. Local, reversible fur loss was seen in all groups. No skin infections were detected.
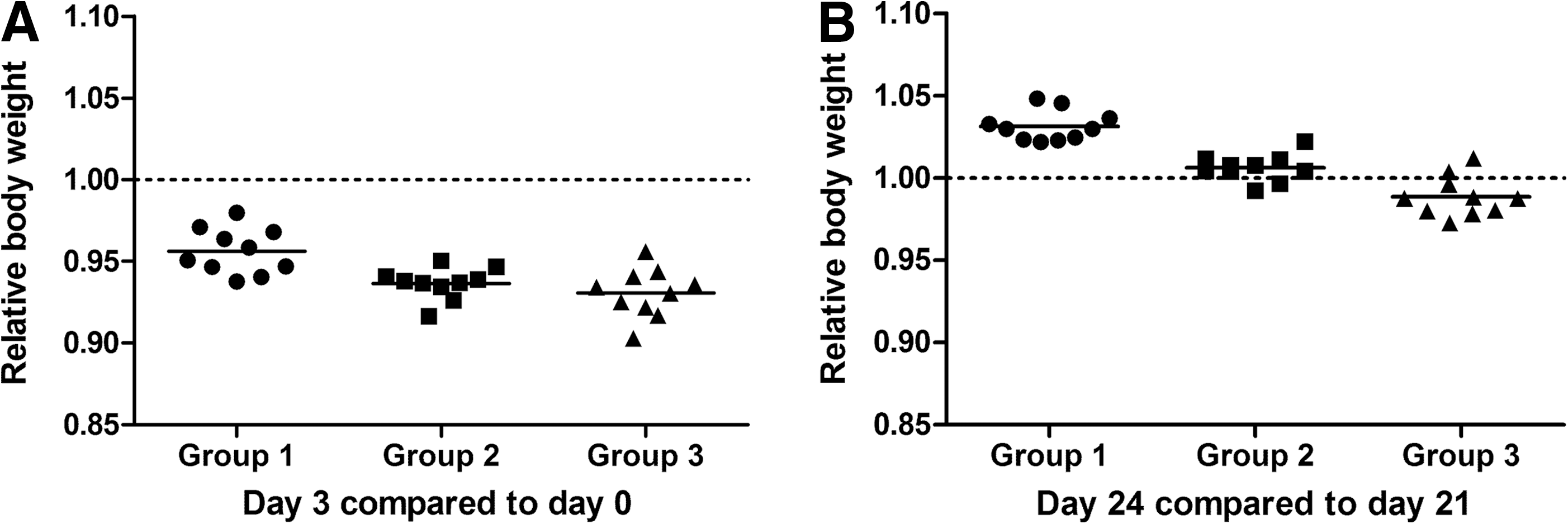
Change in body weight 3 days after the first
The white blood cell counts showed a decrease during the 3 days after the first administration of RIT, with a nadir on days 7–10 (Fig. 2A). The number of white blood cells started to increase after day 10, and stable levels were fully observed by day 45 (Group 1). The additional administration of 150 MBq/kg on day 21 (Group 2) resulted in only in a minor decrease in white blood cells, but the recovery was delayed to day 56. The additional administration of 350 MBq/kg on day 21 (Group 3) led to a second decrease in white blood cells; the second nadir being seen 3 days after the second treatment (day 24), and recovery on day 63. The rate of recovery in Group 3 was similar to that in the other two groups. The differences in white blood cell counts between all groups were significant (p-value <0.0001, two-way ANOVA) from day 21 to day 63. Platelet counts reached a nadir on day 14 after the first treatment (Fig. 2B). The rebound effect peaked on day 24. The second treatment (21 days after the first treatment) resulted in a dose-dependent decrease in platelets, with a nadir on day 35 (i.e., 14 days after the second treatment). At this time (day 35), Group 1 (the group not given any consolidation therapy) showed a small decrease in platelet counts at the end of the rebound period as reported in a previous study. 20 The difference in platelet counts on day 35 was significant (p-value=0.0002, Kruskal–Wallis test, Prism software).
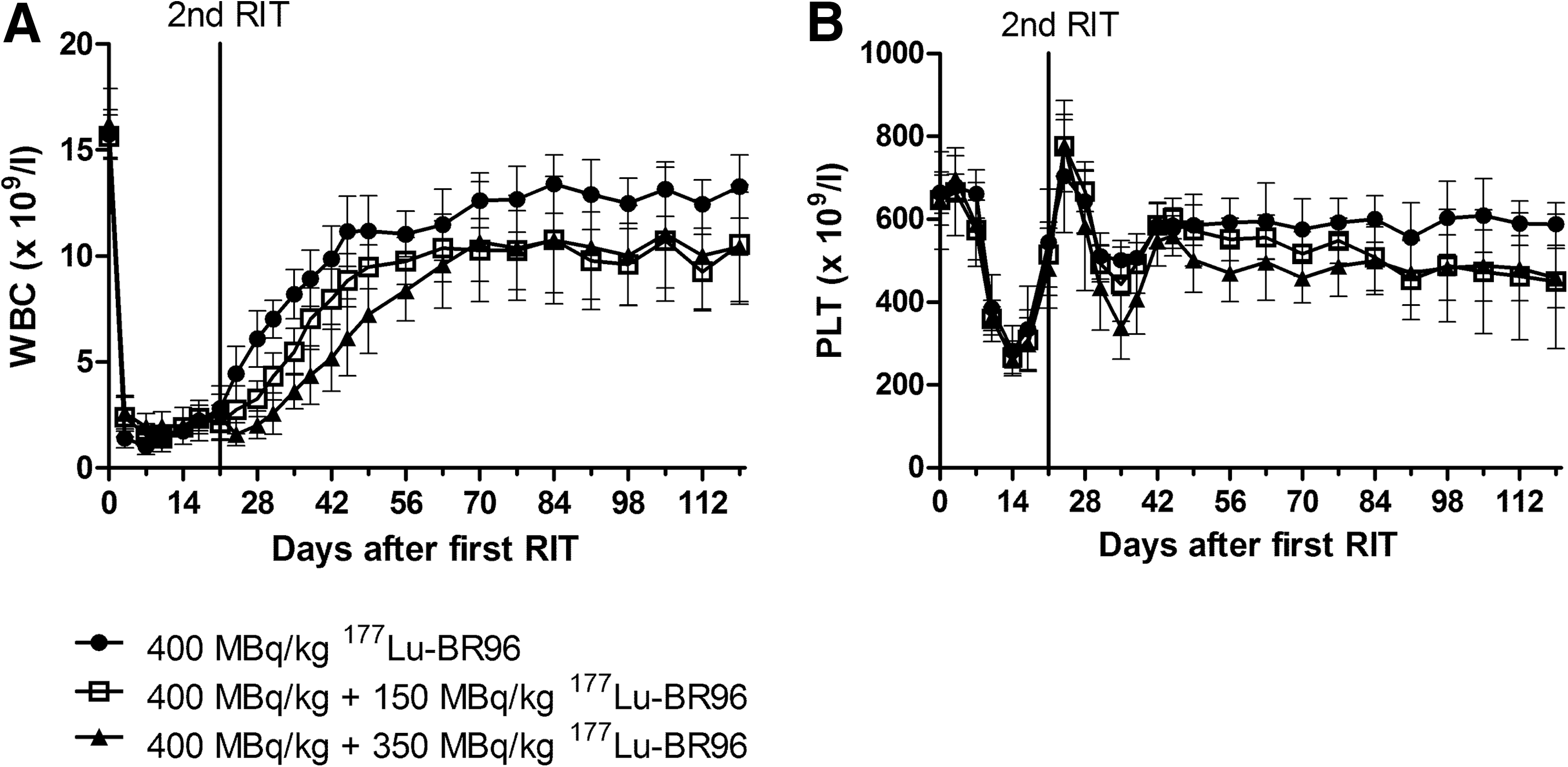
White blood cell counts
Tumor response
The initial average tumor volume (day 0) was 380 mm3 in Group 1 (SD 111 mm3), 310 mm3 in Group 2 (SD 209 mm3), and 340 mm3 in Group 3 (SD 216 mm3). The total injected activity in Group 1 was 102 MBq/animal (range 96–107 MBq); in Group 2, 138 MBq/animal (range 133–145 MBq); and in Group 3, 188 MBq/animal (range 183–194 MBq). These values correspond to 434 MBq/kg (range 367–515 MBq/kg) in Group 1, 569 MBq/kg (range 500–654 MBq/kg) in Group 2, and 803 MBq/kg (range 734–888 MBq/kg) in Group 3. The major cause of the variation in injected activity per kg body weight is the difference in body weight between the animals, since the average weight was used for calculation of the activity to be administered.
After the first treatment, none of the animals in Group 1 had a palpable tumor on day 7 (see Table 2). The animals in the other two groups (2 and 3) became tumor free on day 3–24, that is, as late as 3 days after the second treatment. One animal in Group 3 (given a second administration of 350 MBq/kg) showed a good initial tumor response after the first treatment, but progressed locally after the second treatment, and therefore had to be sacrificed on day 56. This tumor demonstrated intense immunohistochemical staining of the target antigen. One animal in Group 2 (treated with an additional administration of 150 MBq/kg) was free from a detectable tumor for 2 weeks, that is, defined as CR, but the tumor recurred on day 35 and grew slowly to a volume of ∼200 mm3 by the end of the study. Immunohistochemical evaluation showed no positive staining of the target antigen in this tumor, which consisted of stromal tissue without visible tumor cells.
PD, progressive disease.
Disseminated disease
Half of the animals in Groups 1 and 3 (5 out of 10) were free from detectable disease at autopsy at the end of the study (see Table 2). In Group 2, 8 of the 10 rats were free of detectable metastases on day 119, although one of the metastasis-free rats had a local tumor recurrence (described above under the Results, tumor response section). Metastatic disease was observed in 5 rats in Group 1, on days 56, 70, 91, 91, and 119. In Group 2, metastatic disease was observed in 2 rats, on days 63 and 81. In Group 3, metastatic disease was observed in 5 rats, on days 56, 56, 77, 77, and 91. Metastases were usually multiple, and located at several different sites in the same rat, mainly in the abdomen. The exact number of metastases per animal was not determined. Tissue sections from all 12 animals with detected metastases were immunohistochemically stained with the mAb BR96 to detect the expression of the target antigen (Fig. 3). The stained metastases were located in the abdominal cavity (n=9), in the mesentery (n=8), thoracic lymph nodes (n=2), liver (n=1), and lung (n=1). Nine of these metastases showed a strong complete membrane staining of >90% of the tumor cells. The other metastases showed a mixed pattern with both areas of complete and incomplete membrane staining (Fig. 3D). Only very small areas lacked staining (stroma excluded). In 6 cases, where two or more metastases from the same rat were stained, the staining patterns were similar in all cases. The staining pattern and intensity showed no relation to treatment (i.e., total administered activity), or metastatic site.
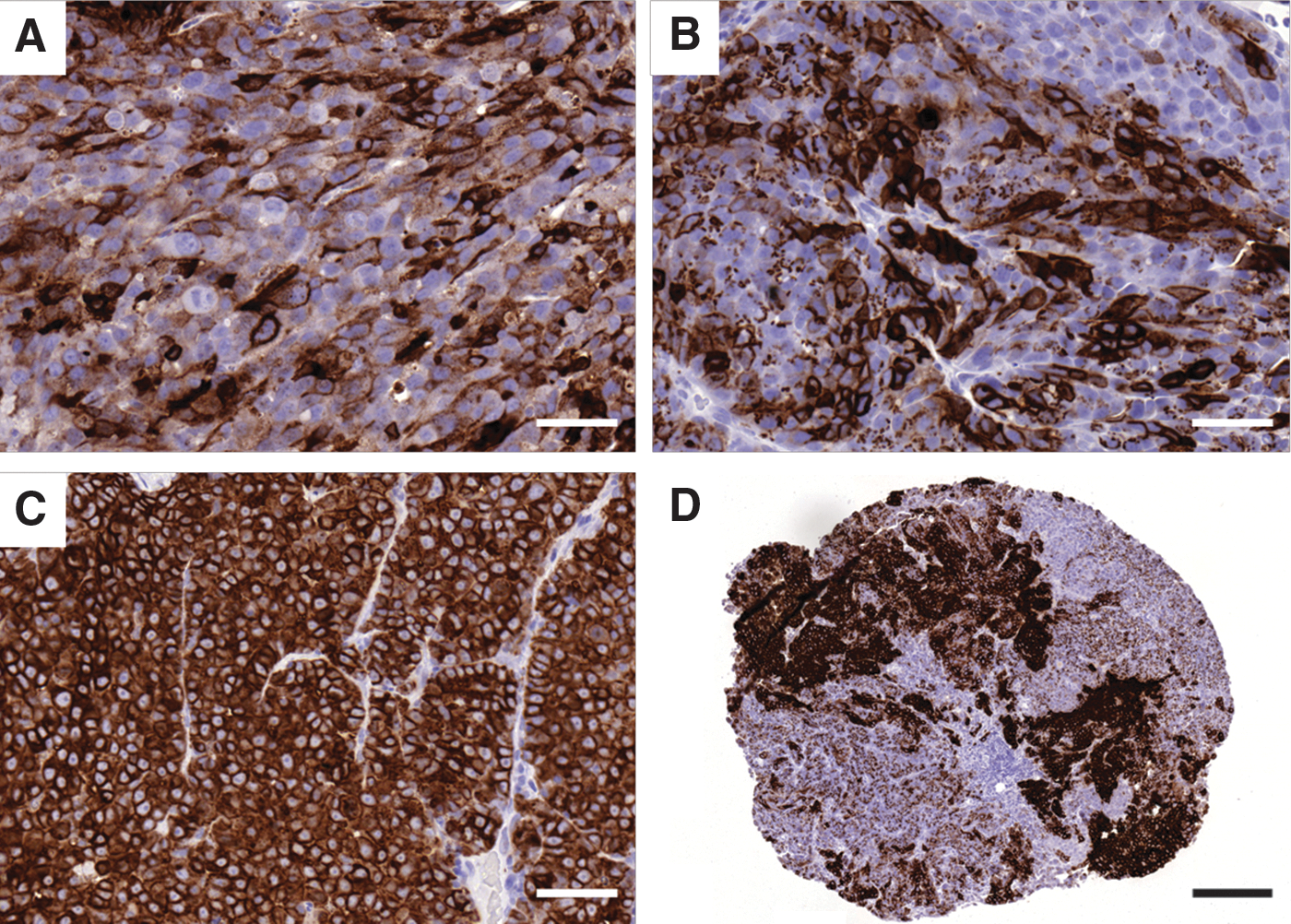
Examples of sections stained with BR96 for detection of the target antigen in
Survival
The mean survival was 102 days in Group 1 (range 56–119 days), 110 days in Group 2 (range 63–119 days), and 92 days in Group 3 (range 56–119 days). The differences in survival were not statistically significant (Mantel-Cox test).
Discussion
The reasons for using fractionation in RIT are to allow a higher total activity to be administered without reaching DLT, and to overcome reduced therapeutic effect due to heterogeneous uptake into the tumor. 1,2,4 In our syngeneic tumor model, CR was seen in 6 of 6 animals after a single administration of 177Lu-BR96 at MTD (600 MBq/kg). 9 Approximately half of the animals treated with 177Lu-labeled antibody showed clinical signs of metastases 40 days or later after the single treatment. In the current study, a second administration of radiolabeled antibody was given to prevent or delay metastatic disease.
The determination of the minimal effective dose clearly showed that the therapeutic effect is dose dependent (see Table 1). To allow an increase in the total administered activity, rats were first treated with the minimal effective dose instead of the MTD. The lower initial activity also enables consolidation therapy with radiolabeled antibodies. The activities administered were chosen to allow repeated therapy without dose-liming toxicity. The first administration of 400 MBq/kg body weight was 0.67 times the MTD and resulted in CR in 5 of 6 animals in the minimal effective dose–determination study, and in CR in 29 of 30 rats in the repeated RIT study (see Table 2). The second administration of 150 or 350 MBq/kg resulted in total administered activities corresponding to 0.9×MTD and 1.3×MTD, respectively. Treatment with a single administration of 135 MBq/kg resulted in CR in 2/6 animals in the prestudy, and this activity was considered suitable for consolidation. The second administration was given 21 days after the first administration. At this point in time, the number of white blood cells had started to recover. Our previous biodistribution studies have shown that no antibody is remaining in the blood at this time. Untreated animals sacrificed on the corresponding day had no visible metastatic disease at autopsy. The timing of the second RIT and the distribution of activity between the fractions may influence the outcome, in terms of both the therapeutic efficacy and toxicity, and must be carefully optimized during the development of a clinical treatment protocol including repeated RIT.
Repeated RIT with 177Lu-DOTA-BR96 in this syngeneic rat colon carcinoma model resulted in dose-dependent, reversible, and tolerable myelotoxicity (Fig. 2). There was an unexpected difference in weight loss after the first and second treatments in Group 3, although the difference in administered activity was only 50 MBq/kg (Fig. 1). The reason for this difference remains unclear. Late toxicity was seen as weight loss and shrinkage of the intestines. In a clinical phase I study with the 177Lu-labeled antibody J591 directed toward PSMA expressed in prostate cancer, dose fractionation resulted in cumulative myelotoxicity, and a 30% increase in tolerated administered activity. 8 In our study, an increase in administered activity of 30% compared with the MTD was tolerated regarding myelotoxicity. No acute DLT was observed. However, late DLT was probably reached in the 3 animals given repeated RIT that were sacrificed due to weight loss without any tumor findings. Other findings of late toxicity, such as shrinkage of the intestines, further indicate that DLT was reached. It is possible that late toxicity could be avoided by increasing the time between the first and second administration of the radioimmunoconjugate.
Approximately half of the animals in all groups had detectable distant metastases at autopsy (see Table 2). Metastases were found in several organs, mainly in the abdominal cavity. The target antigen for BR96 was detected by immunohistochemistry in all stained metastases (Fig. 3). The presence of antigen in all metastases indicates that additional RIT, or other antibody-based therapies, utilizing the same antibody is possible for the treatment of disseminated disease. The antigen expression was not as homogeneous in metastases as in untreated tumors, which showed strong homogeneous staining of all tumor cells (data not shown). No differences in antigen expression were seen between the treatment groups, indicating selection of cells with lower antigen expression already after the first RIT. Changing to an mAb with a different target antigen for the second administration may provide a means of improving the therapy. Another possible way to enhance the therapeutic effect is to change the modality of the additional therapy, and combine RIT with, for example, chemotherapy or tyrosine kinase inhibitors.
In this study, the number of animals with metastases was not affected by an additional administration of 177Lu-DOTA-BR96, and the survival did not differ significantly between the treatment groups. A possible explanation of this is the selection of more radioresistant tumor cells after the first treatment. Also, the chosen radionuclide, 177Lu, is often described as less effective for the treatment of single cells and cell clusters (less than 1 mm in diameter) due to its range in tissue. 21 However, in a number of recent publications it has been concluded that RIT with 177Lu-labeled antibodies maybe effective against metastatic disease. Aarts et al. showed that the intraperitoneal administration of 177Lu-mAb immediately after reductive surgery of peritoneal growth of colon carcinoma in rats prevented peritoneal metastases. 22 The same group showed that the effects were better when RIT was given directly after the surgery (rather than 4 or 14 days after surgery), 23 possibly due to increased tumor size and blockage of antibody binding by fibrin formation after surgery. In another study, RIT with 177Lu, given intravenously after partial hepatectomy in the treatment of colon carcinoma, improved survival, 14 both when administered 3 hours and 1 week after resection. 177Lu has also been used in a rat liver metastasis model in which the formation of colon carcinoma liver metastases was delayed by RIT when administered within a few hours after an intraportal injection of tumor cells. 13 The treatment was less effective when administered 14 days after inoculation with tumor cells, probably due to a lower uptake in larger tumor burdens. The number of cures was not affected by the treatment.
In the current study, we repeated RIT 3 weeks after the first RIT, when metastases probably were too small for 177Lu to be effective. In an SCID mice model with micrometastases of B-cell lymphoma, 177Lu antibody conjugates were less effective than conjugates of the low-energy electron (LEE) emitters 111In and 67Ga. 15 It is considered more appropriate to use short-range isotopes such as α-particle or LEE emitters for the treatment of microscopic disease. 24 The short half-life of most α-particle emitters makes them more suitable for locoregional administration, since most decays will occur before the target is reached when they are conjugated to a large molecule, such as antibodies, and given intravenously. 25 It is generally thought that LEE emitters need to be located close to the cell nucleus to be effective, 26 and therefore requiring internalization although in vitro studies have shown the opposite. 27 However, these radioisotopes may have a low therapeutic effect on nonantigen-expressing tumor cells, as the cross-fire from neighboring cells will be lower. The next step will be to evaluate an antibody labeled with an LEE or an α-particle emitter in consolidation therapy.
In conclusion, repeated administration of 177Lu-labeled antibody resulted in reversible, tolerable, and dose-dependent myelotoxicity. Metastatic disease was not prevented or delayed by the additional treatment in the syngeneic rat colon carcinoma model studied here.
Footnotes
Acknowledgments
The authors would like to thank Dr. Peter Senter (Seattle Genetics) for kindly providing the monoclonal antibody BR96. The research was supported by grants from the Swedish Cancer Society, Mrs. Berta Kamprad's Foundation, Gunnar Nilsson's Foundation, The Crafoord Foundation, Governmental Funding of Clinical Research within the National Health Service, Lund University Medical Faculty Foundation, and The Lund University Hospital Fund.
Disclosure Statement
The authors have no affiliations, memberships, funding, or financial holdings that might be perceived as affecting the objectivity of this publication.