
Abstract
Episcleral plaque brachytherapy using 125I seed is a viable option for the management of intraocular cancer with minimal invasiveness and surgical complications. This article describes the fabrication of 125I seeds and initial experience on their use for the management of intraocular choroidal melanomas. The process of 125I seed fabrication includes immobilization of 125I into palladium-coated silver wires, its encapsulation in titanium capsules using Nd: YAG laser and quality control to assure safety. Plaque preparation consists of the assignment of seeds to slots on the plaque to achieve a desired dose rate distribution. The clinical study reported here includes the retrospective review of 9 eyes of 9 patients who underwent ophthalmic brachytherapy between May 2008 and June 2011. The average apical diameter before brachytherapy was 7.6 mm and the average largest basal diameter was 12.1 mm, which reduced to 3.3 and 7.2 mm, respectively, after the procedure at an average follow-up of 24 months. Patients in our studies experienced good local tumor control. The results of this study represent a significant step forward in the management of intraocular tumors in India.
Introduction
Uveal melanoma is the most common primary intraocular malignancy in lightly pigmented persons and is infrequently seen in nonwhite races. India enjoys a low incidence of malignant melanoma of the uveal tract. It is a rare malignancy, but threatens the patient with visual deficit, loss of the eye, and metastatic death. Owing to the relative rarity of the condition, uveal melanoma is not often suspected till the tumor is large enough to cause a secondary retinal detachment. Clinical diagnosis is mostly based on indirect ophthalmoscopy combined with ultrasonography. Many patients with uveal melanoma have a reasonable chance of surviving and retaining the eye with good vision. The goal of treating uveal melanomas is to identify cancerous lesions and begin treatment to prevent the metastatic spread of tumor from the eye to other parts of the body. Various treatment techniques exist for patients with metastatic ocular melanoma, including plaque brachytherapy, proton beam radiotherapy, stereotactic radiotherapy, transpupillary thermotherapy (TTT), cryotherapy, trans-scleral local resection, and transretinal endoresection. 1,2
Radiation therapy has assumed the most important role for the management of ocular melanomas. The utility of radiation therapy depends on the therapeutic index one can achieve using well-reasoned indications and optimal techniques of irradiation. Episcleral brachytherapy using removable plaques containing sealed radioisotope sources is now the modality of choice for the treatment of choroidal melanomas. 3 It is aimed at effective local tumor control, destruction of metastatic potential, and preservation of ocular and visual function. Titanium-encapsulated 125I seeds containing 18.5–74 MBq (0.5–20 mCi) of activity is currently the most commonly used isotope for such modality. Fontanesi et al. 4 presented results of 144 patients treated with 125I plaques and reported 90% local control, while Quivey et al. 5 reported 81% local control for 150 patients treated between 1982 and 1990. The Collaborative Ocular Melanoma Study (COMS) randomized clinical trial of 125I brachytherapy versus enucleation for medium-sized choroidal melanoma (2.5–10.0 mm in thickness and≤16 mm in diameter) showed that for patients who met the eligibility criteria, there was no statistically significant difference in all-cause mortality between 125I brachytherapy and enucleation 5, 10, and 12 years following treatment. 6 –8 The COMS supported the use of globe-conserving 125I brachytherapy.
The Radiopharmaceuticals Division, Bhabha Atomic Research Centre (BARC), has successfully completed development of a technology for the production of indigenous 125I brachytherapy sources (“BARC I-125 Ocu-Prosta seed”) 9 in the year 2003. The dosimetric studies of sources were carried out at the Radiological Physics and Advisory Division (RP&AD) of BARC, which revealed that the “BARC 125I Ocu-Prosta seed” is similar to the commercial source 6711 Oncoseed of Amersham International. 10,11 The driving force behind this initiative was to provide 125I brachytherapy sources to meet the domestic needs and to promote the beneficial use episcleral brachytherapy in India. In this current work, we describe an overview of our experience, the efforts made and implementation of episcleral brachytherapy using indigenous 125I brachytherapy sources for the treatment of intraocular choroidal melanomas.
Materials and Methods
Materials
Silver wires of 0.5 mm (φ) with guaranteed purity was procured from M/s Hindustan Platinum Ltd., Mumbai, India. 125I as Na125I used in this investigation was available in-house. Titanium capsules were fabricated by the Centre for Design and Manufacture (CDM) of BARC, Mumbai, India. Unrimmed slotted plaques were procured from M/s Eyephysics, LLC, Los Alamitos, CA (Fig. 3). A tissue-compatible autopolymerizing acrylic resin was obtained locally.
Equipment
The Model-1008 well-type re-entrant ion chamber procured from M/s Sun Nuclear Corporation, USA was used for source activity measurement. A 50W Nd: YAG laser welding system M/s Quanta Systems, Italy was used for welding the sources. A well-type NaI(Tl) scintillation counter obtained from Electronic Enterprises (I) Pvt. Ltd., Mumbai, India was used for the measurement of water samples of the immersion and leachability tests. Optical density measurements of exposed X-ray films (Kodak-400; Industrial Grade) were made by using OPTEL - B&W transmission densitometer. Plaque simulator software version 5.3.9 was procured from Bebig GmbH, Berlin, Germany.
Methods
This is a retrospective case series from May 2008 to June 2011. Nine patients were operated. Eight were with posterior choroidal melanomas and one with ciliary body melanoma. All the cases underwent a thorough systemic work-up to rule out metastasis. This included chest X-ray, ultrasound of abdomen, and clinical examination by an oncologist. The steps involved in brachytherapy were the following.
125I sources
125I sources were prepared following the reported procedure developed by our laboratory 10,11 In brief, cleaned silver wires [3 mm (l)×0.5 mm (φ)] were treated with 0.05% PdCl2 solution at ∼100°C for 30 minutes. Palladium-coated silver wires were removed and washed with double distilled water to get rid of traces of loosely held palladium. In a typical batch preparation, 15 Pd-coated silver wires were immersed in 750 μL of 125I solution of activity in the range of 1.665–2.22 GBq (45–60 mCi) containing 75 μg KI as carrier at 60°C–70°C for 6 hours. By this method, more than 80% of the radioactivity could be firmly deposited on the source core. About 111–148 MBq (3–4 mCi) of radioiodine could be irreversibly adsorbed on the palladium-coated silver wires. 9 –11 These source cores were encapsulated in titanium capsules of 4.75 mm (l)×0.8 mm (φ) and welded in one extremity using a 50 W, Nd:YAG laser welding system. 10 The schematic diagram of the source is shown in Figure 1.

Schematic diagram of the titanium encapsulated 125I source.
Quality control of 125I seeds
Before therapeutic use, each 125I seed was subjected to numerous quality control tests following the reported procedure. 12 The dimension of individual-encapsulated seeds, such as the length and diameter, were checked using a profile projector to ascertain that the seeds were free from any distortion. The source strength of the individual seeds was measured in a precalibrated ionization chamber. The surface contamination test was performed by swiping the external surfaces of the sealed sources using alcohol-immersed cotton wool and checking the radioactive content of the swipe in a NaI(Tl) scintillation counter of known efficiency. To ascertain leak tightness, the laser-welded sources were subjected to a bubble test in which each source was individually placed in nearly boiling water (∼25 mL) kept in a glass beaker for about 2 minutes. Appearance of bubbles from the sealed sources indicates improper sealing and such sources were discarded. The hot water immersion leakage test was performed by immersing the seed in 100 mL of distilled water at 50°C for a period of 5 hours and subsequently assaying the total activity released with the help of a NaI(Tl) scintillation counter. Each 125I source was supplied with information regarding the description of the radioactive material (125I), radioactive contents (in terms of MBq), and the manufacturing date. These sealed sources were then transported to the hospital for treatment.
Dosimetry
In this investigation, the plaque simulator software version 5.3.9 (Bebig GmbH, Berlin, Germany) having a three-dimensional treatment planning software was used. For dose calculation, modeling of the eye is done first using computerized tomography (CT) or magnetic resonance imaging (MRI) of axial cut from the center of the eye. Next, modeling of the tumor is done using the ocular ultrasound. A detailed fundus diagram with orientation of the tumor borders relative to surrounding structures, including the optic nerve, foveola, equator, ora serrata, and center of the lens, was made. The longitudinal, circumferential, and apical diameters (ADs) are entered in the software. The fundus image is next uploaded on the software to chart the exact tumor location and also to measure the exact distance from the optic disc to the fovea. This creates a precise computer model of the patient's eye and tumor. For tumors which are 5 mm or greater in apical height, the tumor dose is prescribed at the apex of the tumor; whereas for tumors that are 2.5–5 mm in apical height, the prescription point is 5 mm from the interior surface of the sclera. The prescription point was tumor height plus 1 mm for the sclera with a calculated dose of 85 Gy. Figure 2 depicts the dose distribution from a typical plaque. The average dose rate in our study was 0.58 Gy/hour (range 0.44–0.89 Gy/hour), given over 4 to 8 days depending on the tumor size.
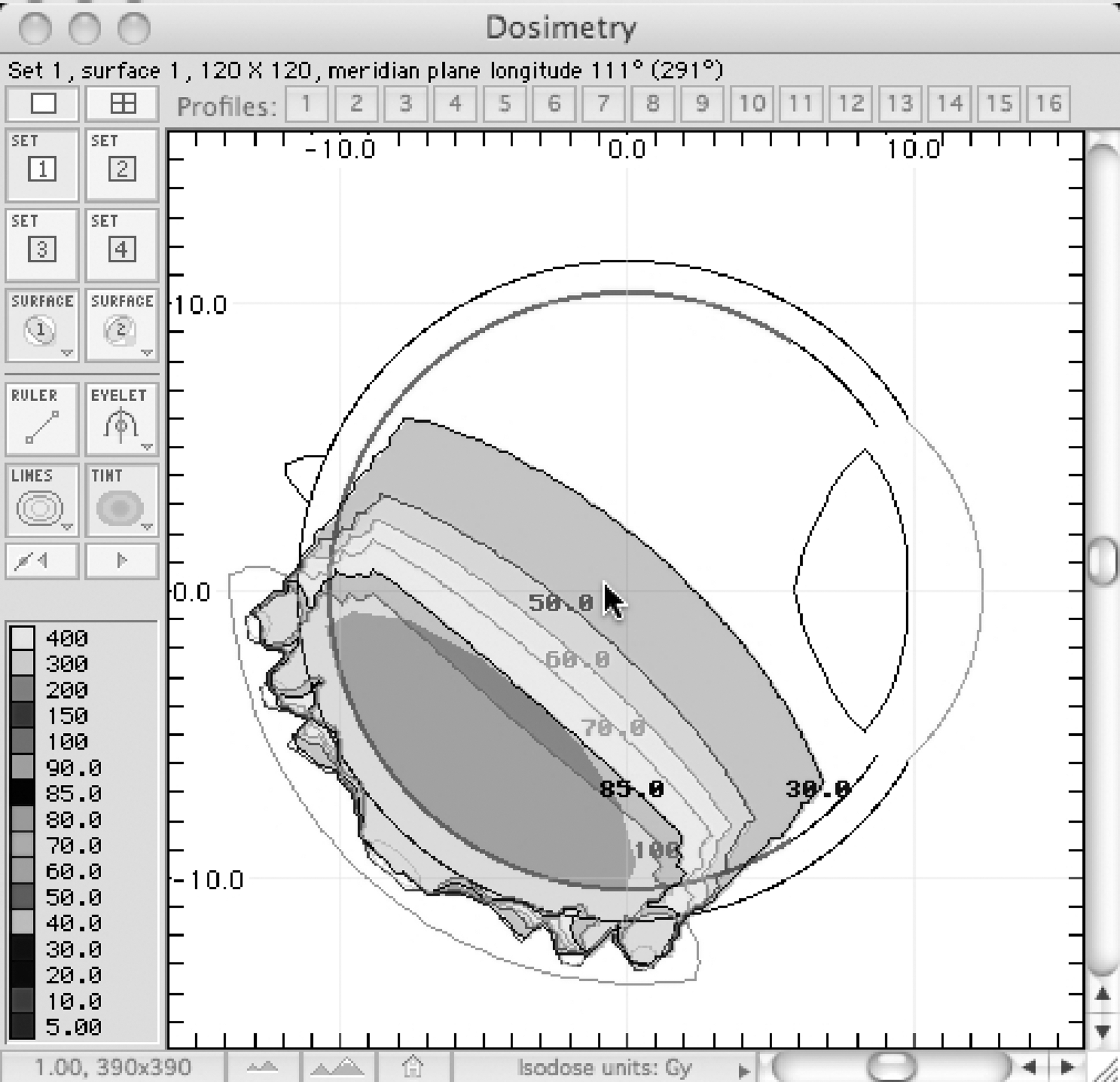
Longitudinal section of computerized model of the eye ball with posterior choroidal melanoma as seen in the planning software. The various doses of radiation the tumor is exposed is demonstrated in different colors. Note 85 is just covering the apex of the tumor.
Selection of plaques
Commercially, both rimmed and unrimmed plaques are available. The COMS plaques are circular rimmed plaques available in five sizes, 12, 14, 16, 18, and 20 mm. There are several disadvantages of COMS plaques. First, they are rimmed and, hence, bulky. Thus, they cannot be passed behind the rectii muscle without resecting them. Second, as they are circular in shape, they cannot be used for tumors near the optic nerve, which would require a notched plaque. Third, the seeds have to be loaded on a Siliastic™ carrier, which is then fitted over the plaque. Thus, when placed over the eye, there is a 1-mm gap between the seeds and the sclera. Hence, higher doses are required to reach the tumor apex, which correspondingly increases the scleral dose and also to the structures distal to the apex. Fifth, as there is lateral overlap of the radiation from the corresponding seeds, the effective dose to the sclera is higher. Sixth, they are expensive. All these disadvantages are partly overcome by the use of unrimmed slotted plaques (Eyephysics, LLC, Los Alamitos, CA). Three of the currently available plaques are models 517, 917, and 2025. The inner surface of the plaque is concave and raised from the surface of the sclera to reduce the dose to the sclera and increase the depth dose. These plaques are less bulky and can often slide under the extraocular muscles more easily than the rimmed plaques. The model 917 also has a notch that can accommodate the optic nerve for tumors close to it. The plaque selected for each treatment was of sufficient size to encompass the base of the tumor and a tumor-free perimeter of 2 mm. Figure 3 depicts the photograph of slotted gold plaques used for treatment.

Slotted gold plaques of three different sizes along with dummy plaques (wire frames). The center plaque is a notched one.
With the knowledge of the tumor size and the radioactivity content of the prepared 125I seeds, computer calculations determined the orientation and number of seeds to be placed in each plaque. Because the 125I seeds are glued into individually collimating slots carved into the concave surface of the gold plaque, the seeds can be moved closer to the sclera compared to the seeds in the Siliastic carrier of a COMS plaque. Most of the laterally directed soft radiation emanating from the seeds is thus blocked by the gold carrier, eliminating much of the radiation overlap immediately in front of the plaque.
Preparation of plaque
After the completion of basic dosimetry, the requirements of the approximate number of seeds of required strength were known. 125I seeds of required activity were fabricated in BARC and were dispatched to user's institution after quality assurance 13 . The activity content of individual seeds was again verified at the hospital using a calibrated ion chamber. 125I seeds were then placed into the slots of the plaque by the medical physicist to attain the desired dose rate distribution. The typical activity used was 74–111 MBq (2–3 mCi) per seed so as to achieve treatment dose rates of 0.5–1.25 Gy/hour, with a prescription dose of 80 Gy delivered in 4 to 8 consecutive days. Seed assignment was straightforward as seeds were fabricated as per requirement. They are then glued over night by using a tissue-compatible autopolymerizing acrylic glue. Before surgery, the plaque was sterilized by flash autoclaving for 4 minutes.
Surgical procedure
Under peribulbar block, localized peritomy is done in the quadrant where the tumor is present. Bridle sutures of the corresponding rectii muscles are taken. The tumor margins were identified using trans-scleral illumination and indirect ophthalmoscopy. A dummy plaque (cold plaque) is first secured with temporary knots. The placement of the dummy plaque is confirmed by indirect ophthalmoscopy and scleral indentation. A minimum safety margin of 2 mm was maintained. The dummy plaque is then replaced with the hot plaque containing the radioactive seeds, and then the suture knots are made permanent. The plaque is then covered with the conjunctiva. The surgical procedure is depicted in Figure 4. The plaque removal is then done after 4 to 5 days, as per the dosimetry. During that time, the patient is kept in an isolated room with the eye covered with an appropriate lead shield.

Surgical procedure
Radiological safety
All steps of the treatment procedure were planned in advance to minimize radiation exposure of personnel. All radioactive source movements and inventory were recorded. The personnel involved in this work were monitored for radiation exposure levels by the thermoluminescent dosimetry badge and pocket dosimeter.
Results
The goal of this article is to report the successful adaptation of an indigenously developed 125I brachytherapy seeds for the management of intraocular choroidal melanomas.
Fabrication and quality control of 125I seeds
Following the reported procedure, a number of batches of 125I sources were prepared. Each seed before treatment was tested in BARC in accordance with a strict quality control protocol and in compliance with the guidelines prescribed limit of the Atomic Energy Regulatory Board (AERB), India 13 . The mean activity of the source used were ranged from 90 to 118 MBq (2.5–3.18). Before medical use, these sealed sources were subjected to quality control to evaluate their integrity. Results of the surface contamination test conducted on the sources revealed that the removable radioactivity levels were found to vary from 40–136 Bq, which were well below the prescribed limit of AERB. India. To prevent the radioactive contamination risks during the use of 125I sources, they were subjected to leak tests. Results of the leak test conducted on the sources show that the radioactivity leakage from the source was in the range of 104–170 Bq, which was well below the regulatory limit. The quality control result of a typical batch of 125I seed is depicted in Table 1.
The assessment of radioactive content of individual seeds at the hospital is obligatory to evaluate variations among seeds and to ensure the absence of cold seeds. The variation of radioactive from seed to seed was consistent as seen by a±5% standard deviation. So far, a cold seed was not detected in the hospital.
Before treatment, factors such as tumor size, activity, location, growth pattern, the patient's general health, age, and status of the other eye were taken into consideration. During the period of this study, from 3 years, 9 eyes of 9 patients were operated. Majority of patients had a decreased visual acuity at the time of presentation.
The goal of episcleral plaques 125I brachytherapy is the preservation of the eye and visual function by intraocular progression. Therefore, delineating the tumor to optimize radiation doses, allowing minimization of dose to adjacent developing tissues is a crucial goal. To this end, multimodal imaging was carried out to avail information on physical density for dose calculation and morphological volumetric information. Ophthalmologic examination with 2D and 3D ultrasound and fundus pictures allow a very accurate definition of the tumor volume. Using the developed plaque simulator software and taking into account the physical characteristics of the eye plaque, dosimetric calculations were carried out. The dose calculation was carried out by a dosimetrist, and the plan was approved by a radiation oncologist before implementation in actual patient treatments. The prescription point was the tumor height plus 1 mm for the sclera. Treatment time was calculated from the central axis depth dose curve. The tumor was localized with transillumination, using a fiber optic probe or indirect ophthalmoscopy with scleral indentation. The plaque was positioned based on the location of the tumor, extraocular muscles, and the limbus as landmarks. Of the nine cases of choroidal melanomas, eight were posterior, while one case involved the ciliary body region. Tumor characteristics of the patients are shown in Table 2.
MCBM, medium ciliary body melanoma; MPM, medium posterior melanoma; LPM, large posterior melanoma.
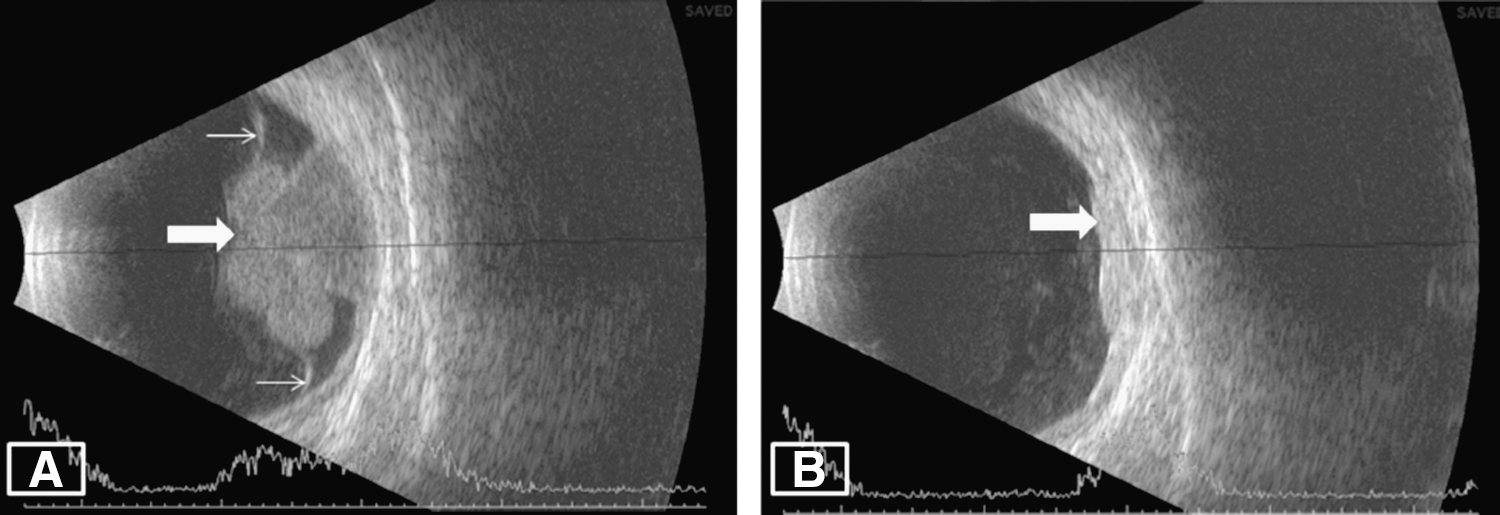
The COMS study had divided the choroidal melanomas into three types, namely, small, medium, and large according to the size. 14 Tumors with AD <1 mm and the largest basal diameter (LBD) <5 mm are called as choroidal naevi. Tumors with AD between 1 to 3 mm and LBD between 5 to 16 mm were classified as small melanomas. With AD between 3 to 10 mm and the LBD between 5 to 16 mm are classified as medium (unless it is located within 2 mm from the optic disc), the tumors with AD >10 mm and LBD >16 mm are classified as large melanomas. Six were medium sized and three were large melanomas, in our study. The mean AD was 7.6 mm (range 3.8–13.4 mm), and the mean LBD was 12.1 mm (range 5.2–17.3 mm). The average seed strength was 111 MBq(3.0 mCi) [range 93–119 MBq (2.5–3.2 mCi)], and the average number of seeds used was 16.1 (range 9–25). The average number of days for plaque removal was 6.4 days (range 4–8 days), and the average dose rate was 0.58 Gy/hour (range 0.44–0.89). Model 2025 was used for five cases while model 917 was used for remaining four. TTT was given in the three large melanomas, 2 days before plaque removal as part of the sandwich technique described by Kreusel et al. 15 The average duration of TTT was 9.21 minutes and the average power was 223 mV. In the immediate postoperative period, case 1 had vitreous hemorrhage with hemorrhagic choroidal detachment and case 3 had bleeding inside the tumor. Both these complications were assumed to be due to the sharp tip of the diaphanoscope, which is the instrument used for transillumination. After these two initial complications, we did localization of posterior tumors by indirect ophthalmoscopy and scleral indentation without using the diaphanoscope, and did not face similar complications. The mean follow-up was 24 months (range 6.5–40 months). The average AD reduced to 3.3 mm and 7.2 mm, respectively, at last follow-up. Two eyes needed enucleation after brachytherapy. Both cases developed active exudation and hemorrhage suggestive of advanced radiation retinopathy. Although in both cases the tumor had not increased in size, there was optic nerve infiltration in one case and the other one was case 3, which had got injured by the diaphanoscope during the surgery. Both eyes were enucleated at 10 and 18 months, respectively. The tumor almost completely disappeared in a large- and a medium-sized posterior melanoma. The preoperative B scan and the postbrachytherapy B scan of the same patient scan picture of a typical case is shown in Figure 5. The treatment outcome for each patient is shown in Table 3.
AD, apical diameter; LBD, largest basal diameter; LPM, large posterior melanoma; MCBM, medium ciliary body melanoma; MPM, medium posterior melanoma; FAD, last follow-up apical diameter, FLBD, last follow-up largest basal diameter.
In terms of radiation exposure during the procedure, pocket dosimeters used by the hospital staff have shown exposures of 0.05 to 0.2 mSv, which is well within the weekly permissible dose limit.
Discussion
Risk factors for intraocular melanoma include Caucasian race, light skin or eye color, dysplastic nevus syndrome, oculodermal melanocytosis, sun exposure, and occupational exposure (welders, chemical workers). The etiology for the most part is multifactorial or unknown. 15 Most patients with ocular melanoma have symptoms such as blurry vision, loss of vision, floaters, visual field loss (as in our patients), growing dark spot on the iris, or alteration in the size or shape of the pupil. Pain is a very rare symptom. 16,17 Diagnosis is accomplished by a comprehensive eye examination alone by an ophthalmologist. 18
Intraocular melanomas are generally made up of two different kinds of cells, namely, spindle (long, thin cells) and epitheloid (round, straight) cells. Most tumors are composed of both kinds of these cells. Epitheloid tumors are more likely to metastasize to distant sites than the spindle cell variant. The mode of metastasis is hematogenous for both histological subtypes, with the first site being the liver. 17,18 There are very few cases reported of spread of choroidal melanoma into the conjunctiva via regional lymphatics 19 and/or spread to the maxillofacial bones. 20 Every patient deserves a thoughtful individual assessment before therapeutic avenues are pursued. Management of intraocular melanomas depends on several factors, including the patient's age, tumor size and location, systemic health of the patient, and the status of the other eye. Plaque radiotherapy is the first choice of treatment in most of the cases.
Selection of radioisotopes for use in episcleral plaque brachytherapy is an issue to be addressed appropriately. The four radioactive isotopes currently used in ocular oncology are 125I, palladium-103, cesium-131, and ruthenium-106.
Ruthenium-106 is not very commonly used, although it is convenient for the user in terms of logistics due to long half life (∼1 year). Owing to the short distance range in tissue, 106Ru plaques cannot completely irradiate tumors more than 5 mm tall. Although 106Ru minimizes the dose to contralateral structures, it delivers a very high dose to the sclera and unsuitable for the treatment of tumors with an apical height greater than 3 to 5 mm. Owing to the limited side-scatter, 106Ru plaques can more easily be placed in the wrong spot. This is why many surgeons use larger 106Ru plaques to allow more room for error. Furthermore, the radiation window of the plaque, under which the radioactive material sits, is only 0.1 mm thick. Therefore, it is imperative to take precautions not to scratch that delicate inner surface. Several authors have reported that local tumor control rates and need for enucleation appear to be inferior with 106Ru compared to 125I, especially when the apical tumor height is considered. These failure rates are likely higher because the tumor apex can fall outside of ideal dosimetry (beyond the radiation dose fall-off). 21 –24
125I for choroidal melanoma was first described by Sealy in 1976. 24 The major advantage of this radioisotope is the ability to protect the surrounding ocular structures, including the eyelids and lacrimal system, and reduce the radiation exposure to the surgical staff. 25,26 The excellent screening characteristics, good tissue penetration, the low oxygen enhancement ratio, and high relative biological effectiveness make 125I an ideal source for choroidal melanomas and other tumors in and around the eye. Overall, medium-sized ocular melanomas can be controlled using 125I seed plaques delivering a dose of 75–85 Gy to retain vision.
Palladium-103 has been proposed as an alternative to 125I to treat choroidal melanomas. 27 Compared with 125I, 103Pd has a lower energy and a more rapid dose fall-off resulting low incidence rates of radiation retinopathy. 28 More extensive trials using this isotope are required to assess its efficacy in tumor control rates in comparison to 125I. 29 Palladium-103 is more expensive and its lower penetration makes it less suitable for treating large tumors.
Cesium-131 seed offers a significantly shorter radiation half-life than 103Pd and 125I, which results in a substantially faster delivery of therapeutic radiation, a theoretically improved radiation delivery against aggressively replicating cancer, 30 and the potential for a reduced longevity of common brachytherapy side effects. 31 In December 2007, IsoRayI, Inc. (Amex: ISR; Richland, WA) began launching its Proxcelan™ Cs-131 seeds for the treatment of ocular melanoma. IsoRay is gathering data on the effectiveness of this isotope in this indication and publications are expected as the data matures.
A large-scale production process to avail 103Pd and 131Cs for seed brachytherapy application has not been established in India. The logistics and cost considerations of these isotopes do not permit their use at present from an Indian perspective. On the other hand, 125I with its relatively longer half-life and suitable gamma energy coupled with in-house availability is a cost effective proposition. The Indian pursuit of developing technology for 125I brachytherapy sources was driven mainly by three considerations, namely, (1) well-established and ease of reliable production of 125I in several GBq quantities in the research reactor (Dhruva) in BARC, (2) need to provide 125I- brachytherapy sources at an affordable cost to meet the domestic needs, and (3) help to ease reliance on import and to promote the beneficial use of 125I- brachytherapy sources in the country.
Plaque brachytherapy is now an established procedure world over for intraocular choroidal melanomas. 28 However, in India, it is not popular probably due to its rarity in the pigmented race. 32,33 To reap the benefits of episcleral plaque brachytherapy and achieve ocular retention with good visual acuity and local control, it is necessary to select patients carefully and appropriately when choosing modality. Accurate measurement of the tumor dimensions and design, placement, and verification of the plaque each contribute to the success or failure of this modality of treatment. Minimizing the delay between evaluation and treatment is also important.
Due to the anatomical location of ocular melanomas, critical structures are abundant and in close proximity to each other. In general, episcleral plaque brachytherapy can be associated with radiation-induced side effects, requiring frequent patient monitoring. Radiation side effects are dose dependent. Plaque treatment of an anterior tumor will tend to cause more cataract because the plaque is close to the lens, while treatment of a posterior tumor will tend to cause more radiation maculopathy and radiation optic neuropathy. It is important to note that less radiation to the macular retina will result in preservation of central vision. Combining seed position and activity allows the creation of a customized dose distribution for each individual patient. Precise absolute and relative preoperative dosimetry is therefore vital for both tumor dose prescription and judgment of the risk of normal tissue toxicity. As a general rule, precise dosimetry is essential with the intent to maximize tumor control and minimize normal tissue complications.
For choroidal melanomas, the local treatment failure rate in COMS trial was 13%, 34 while it was 22.2% in our study. Two eyes of 2 patients were enucleated in our study. The 5-year all-cause mortality was 19% in the enucleation group and 18% for the 125I- brachytherapy group, in the COMS trial. None of our cases had any metastasis till the last follow-up. However, in our study, the sample size was much smaller and the final follow-up shorter compared to the COMS study. We did not see other reported complications like corneal dryness and optic neuropathy, 35 in any of our cases.
We believe that a comparison of our results with the previous study of “BARC 125I Ocu-Prosta seed,” 36 was unsuitable because of the single case report that too of a patient with choroidal metastasis whose long-term follow-up is questionable. Thus, our study is the largest series of patients treated with these indigenous “BARC 125I Ocu-Prosta seed” and comparable to that of other studies. The reported outcomes need to be evaluated with caution owing to the small number of patient study.
Conclusion
Although episcleral plaques brachytherapy using 125I seed is technically challenging, it seems to be a safe and effective treatment option for the management and control of intraocular tumor. Despite the general axiom that ocular melanomas are radiation resistant, highly concentrated radiation therapy can be successful in promoting tumor regression. It provides a fair chance of preserving the eye with acceptable cosmesis and a reasonable chance of conserving useful vision. While there is still a long path to travel to find the ultimate cure for ocular melanoma, the results of this institutional retrospective study represent a significant step forward in the management of intraocular melanomas. We believe that the local availability of “BARC 125I Ocu-Prosta seed”, its favorable characteristic and adaptabilities to specific tumor locations and sizes, and cost effective ophthalmic brachytherapy can be offered in India. There is a great deal of anticipation that “BARC 125I Ocu-Prosta seeds” will find their way into many more institutions in India in the foreseeable future.
Footnotes
Acknowledgments
The authors wish to express their sincere thanks and gratitude to Dr. P. Namperumalsamy, Chairman Emeritus, Aravind Eye Care System and Dr. M. R. A. Pillai, Head, Radiopharmaceuticals Division, Bhabha Atomic Research Center (BARC) for their guidance, encouragement, and continued support. The authors wish to thank Dr. Meera Venkatesh, former Head, Radiopharmaceuticals Division, BARC for her administrative support during the course of this work. Our thanks goes to the Board of Radiation and Isotope Technology (BRIT) Mumbai, India for timely shipment of source consignments to the user's site.
Disclosure Statement
The authors have neither received any outside funding nor any grants from any external agencies in support of this study. Our institutions do not have a financial relationship with any commercial entity that has an interest in the subject matter or materials discussed in this manuscript. None of the authors in this manuscript have any conflict of interest, financial or otherwise in the publication of this material.