
Abstract
The primary goals of this study were to determine the biodistribution and excretion of 18F-EF5 in oncologic patients, to estimate the radiation-absorbed dose and to determine the safety of this drug.
Methods:
Sixteen patients with histologically confirmed malignancy received a mean intravenous infusion of 217 MBq (range 107–364 MBq) of 18F-EF5. Over a 4–6-hour period, four to five serial positron emission tomography (PET) or PET/computed tomography (CT) scans were obtained. To calculate the radiation dosimetry estimates, volumes of interest were drawn over the source organs for each PET scan or on the CT for each PET/CT scan. Serial blood samples were obtained to measure 18F-EF5 blood clearance. Bladder-wall dose was calculated based on urine activity measurements.
Results:
The urinary bladder received the largest radiation-absorbed dose, 0.12±0.034 mSv/MBq (mean±SD). The average effective dose equivalent and the effective dose of 18F-EF5 were 0.021±0.003 mSv/MBq and 0.018±0.002 mSv/MBq, respectively. 18F-EF5 was well tolerated in all subjects.
Conclusions:
18F-EF5 was demonstrated to be safe for patients, and the radiation exposure is clinically acceptable. As with any radiotracer with primary excretion in the urine, the bladder-wall dose can be minimized by active hydration and frequent voiding.
Introduction
Tumor hypoxia contributes to treatment resistance and is thought to be important in the evolution of the malignant phenotype. 1 It has been shown to adversely affect the clinical outcome of patients with head and neck cancer, soft tissue sarcomas, prostate cancer, and uterine–cervix carcinomas receiving radiotherapy and/or other treatment modalities. 2 –5 Oxygen measurements in these seminal studies were made using polarographic oxygen electrodes (Eppendorf pO2 Histograph). The electrodes consisted of semiautomatically driven 26-gauge needles. The needles are invasive, and their use was technically demanding, so they are not optimal for general clinical practice. In addition, large intratumoral variations of pO2 exist. Thus, multiple measurements throughout the tumor are required to obtain a reproducible estimate of an individual tumor's oxygenation status.
To address these issues, there has been a great deal of interest in the development of radiopharmaceutical agents that could noninvasively delineate areas of hypoxic tissue. Most agents under current development are either 2-nitroimidazoles or copper chelates labeled with positron-emitting isotopes. 18F-fluoromisonidazole (FMISO) is an example of the former and has been the most widely studied PET-based hypoxia marker. 6 The prototype for the latter is 64Cu-diacetyl-bis(N(4)-methylthiosemicarbazone) (Cu-ATSM). 7
Most of the second-generation 2-nitroimidazoles under current study as hypoxia-imaging agents are more hydrophilic than FMISO (partition coefficient 0.43). 6 Hydrophilic drugs generally have rapid renal excretion, which can assist in lowering the background of noninvasive imaging agents. However, they also distribute slowly, especially to lipophilic tissues such as the brain. EF5 is 2-nitroimidazole, which contains 5 fluorine atoms in its side chain and is quite lipophilic (octanol-to-water coefficient=5.7) 8,9 as compared to other 2-nitroimidazole hypoxia markers such as FMISO and fluroazomyciu arabinoside (FAZA). 6,10 EF5 was specifically developed on the opposite principle to that described above (i.e., to achieve rapid equilibration with all tissues and low rate of renal excretion). Both labeled EF5 and unlabeled EF5 have been documented to cross the blood–brain barrier and to bind in central nervous system (CNS) tumors at a rate that is inversely proportional to the tissue oxygen level. 11,12 EF5 adducts form with protein thiols following a multielectron reduction process by cellular nitroreductase enzymes. 13,14
The primary goals of this Phase I dosimetric study were to determine the safety, biodistribution, and excretion of the radioactive drug (18F-EF5) in subjects with known malignancies and to estimate the radiation-absorbed dose of this drug. Our data provide a much more detailed assessment than were published in a recent pilot study. 15 Additionally, the current study was performed at two independent sites (University of Pennsylvania, Philadelphia, PA, USA [Penn] and University of Turku, Finland [Turku]) using similar protocols and comparable analyses.
Methods
Patients
Patients with present or former malignancy were eligible for inclusion. Patients had to be at least 18 years of age with an Eastern Cooperative Oncology Group (ECOG) performance status of <2 and no evidence of New York Heart Association Class III or IV cardiac disease. Patients had to have adequate results of clinical laboratory tests, including values of liver and kidney function, and blood chemistry. Those who were pregnant, nursing, or have a history of allergic reactions attributable to metronidazole were excluded. The study protocol was approved by the ethics committee at the University of Turku and the Institutional Review Board at the University of Pennsylvania. All patients provided written informed consent before study enrollment.
Radiopharmaceutical
The allyl precursor for EF5 was synthesized, as previously described. 16 18F-EF5 was prepared from this precursor using radioactive fluorine in a one-step reaction in the presence of trifluoroacetic acid at low temperatures. In Turku, high specific activity 18F-fluorine was used, 17 whereas 18F-fluorine with an ∼100-fold lower specific activity was used at Penn. 16 This resulted in final drug-specific activities of about 4 and 0.04 GBq/mmol, respectively. Before imaging, two intravenous lines were placed in the antecubital fossa, the first for drug infusion and the second for blood sampling (see below). Each subject received an intravenous dose of 107–364 (mean 217) MBq of 18F-EF5 in a volume no greater than 10 mL administered as a bolus. The radiopharmaceutical dosage (i.e., activity) was assayed in a dose calibrator before and after injection to yield the net injected activity.
PET imaging
At the University of Pennsylvania, PET studies were performed on a Philips Allegro PET scanner. This system has an axial and transverse field of view of 18 and 57.6 cm, respectively. It consists of a gadolinium oxyorthosilicate crystal-based PET camera with an internal 137Cs transmission source for attenuation correction. The scanner has a spatial resolution of 5.3-mm transverse and 5.6-mm axial. 18 At the University of Turku, PET/computed tomography (CT) studies were performed on a Discovery (GE Healthcare) VCT PET/CT (combined helical 64-slice CT) scanner. The PET component has an axial and transverse field of view of 15 and 70 cm respectively, with bismuth germinate crystal detectors. Attenuation corrections were performed using the self-contained diagnostic CT. The spatial resolution of the system is 5–6 mm.
All images were performed from vertex to mid thigh. Images were acquired at 15 minutes postinjection, and repeated at ∼1, 2, and 4 hours postinjection. One subject at Turku (#5) was imaged five times with the final image acquired at ∼6 hours postinjection. For patients imaged at Turku, 7–8 bed positions were required depending on the length of the subject. The imaging time for the 1st and 2nd scan was 3 minutes per bed position, and for the 3rd–5th scan, the imaging time was 4 minutes per bed position. For patients imaged at Penn, emission images were acquired for between 60 and 100 seconds per bed position followed by a standard transmission scan, with a total imaging time of 50–60 minutes. Otherwise, all aspects of the protocol were similar between the two sites.
After PET image data acquisition, reconstruction was performed using a filtered back projection or iterative ordered-subset expectation maximization (OSEM) method with 2 iterations and 28 subsets. Attenuation, random, scatter, decay, detector deadtime, and nonuniformity corrections were performed on all emission acquisitions.
Source-organ residence times
To obtain the activity data in each organ for Penn patients, volumes of interest (VOIs) were drawn in all axial planes (where the organ was visible) for all PET image datasets using the attenuation-corrected PET image sets. The VOIs widely covered the target organ to ensure that the entire accumulated radioactivity was encompassed. The VOI activity concentration data were recorded for the following sites: urinary bladder, kidney, liver, gall bladder, heart, brain, lungs, muscle, and red marrow (from femur). Red marrow was defined by delineating a circular region of interest around the uptake in the center of the femur, which was assumed to be red marrow, and the activity per cc was determined. The reconstructed pixel values were recorded for each VOI, which was then multiplied by an acquisition-specific calibration factor to obtain the activity data.
For each patient imaged at Turku, the organ volumes were delineated on the CT images using iPlan RT Image version 4.1 (BrainLab AG). The activity concentration values were average values measured from these delineated VOIs of the organs. Due to the added capability of the CT to define the organ position, it was also possible to define activity concentrations for the spleen, pancreas, and blood (aorta) in the Turku dataset.
Both sites provided the source organ activity amounts as VOI activity concentrations (kBq/mL). The total activity in each organ was obtained by multiplying the VOI concentration value by that organ's volume, as given in OLINDA/EXM (Vanderbilt University, Nashville, TN 19 ) software adult male phantom.
At both sites, blood was collected from the arm contralateral to that used for injection to determine 18F-EF5 blood activity. Samples were collected at ∼15 minutes before injection, then at 15 minutes, 1, 2, and 4 hours after injection, and at the conclusion of the final imaging session.
At both sites, patients were instructed not to void 45 minutes before 18F-EF5 injection. After injection, patients were requested to void before each scan, with time and volume of excretion recorded. The activity concentration in each urine aliquot was measured, and the fraction of injected activity excreted into urine was calculated for all patients and for all aliquots of urine collected.
Blood and urine samples were diluted 1+1 (by volume) with iced trichloroacetic acid and left on ice for 10 minutes. These acidified samples were centrifuged at 10,000 g, and the supernatants were analyzed with a liquid-scintillation counter (LSC). Values from the LSC were decay-corrected and calculated as kBq/mL. Blood standardized-uptake values (SUVmass) were obtained by normalizing kBq/mL values with the injected dose and the patient weight. Representative samples were also assessed by high-performance liquid chromatography (HPLC) using conditions described previously. 8
Biological samples
Lab measurements consisting of a complete blood-count, complete serum biochemical analysis, and urinalysis were performed at baseline and repeated after the scans.
Safety monitoring
A complete physical exam, including assessment of medical history, was performed on each subject before enrollment on the study. A 12-lead electrocardiogram was obtained 15 minutes before and within 15 minutes after 18F-EF5 infusion. Vital signs (heart rate, systolic and diastolic pressure, respiratory rate, and body temperature) were recorded with the patient in the supine position at the following time-points: 1–2 hours preinjection, 15 minutes preinjection, and 15 minutes, 1, 2, and 4 hours postinjection.
Patients were questioned about any discomfort or adverse experiences during the study procedure and during a follow-up call 24 hours after the imaging study. Any observed adverse events were noted and scored using Common Terminology for Adverse Events version 3.0 (CTCAE).
Statistics
All subjects who received the radioactive drug were included in the safety, biodistribution, and excretion evaluations. Two-tailed t-tests were used to determine whether there were any significant changes in liver or renal function tests. A p-value of less than or equal to 0.05 was considered statistically significant.
Source-organ time-activity curve fitting
Data describing the percent of the injected activity in each source organ were mathematically simulated. For this dataset, a monoexponential function was iteratively fit to each source-organ time-activity curve using a nonlinear least-squares regression algorithm (SAAM II v1.2 software; The SAAM Institute, Inc.). The form of this equation, A(t), is given below:
where A0 is the extrapolated activity at zero time (total number of radioactive decays per unit administered activity), and λ is the removal rate (hour−1). The source-organ cumulative activity is obtained by analytically integrating the curve-fit equation, A(t) from time equals zero to infinity, after correcting each term by the isotope decay.
Excretory clearance and total body residence times
The imaging data (see Results) suggested that EF5 was mainly excreted via kidney/bladder, although a small amount of activity was also present in the gall bladder, and thus should appear in feces as expected for a lipophilic drug. Because of the relatively slow clearance of the tracer from the gall bladder, it was assumed that only small amounts of activity would reach the small bowel. This is a reasonable assumption for dosimetric estimates given the short physical half-life of 18F (109.8 minutes). Urinary excretion was measured directly and was assumed to account for the main biological loss of 18F from the body. Based on this assumption, we computed the total body retention as 100% minus the urinary-excreted activity (expressed as a percent of the injected activity). This total body retention curve was simulated using monoexponential functions as described above, with the coefficient, A 0, fixed at 1.0 (i.e., 100%).
Radiation-absorbed dose calculation
OLINDA/EXM software was used to estimate the absorbed doses. The Adult Male phantom was used to compute the radiation doses for each subject. This phantom is hermaphroditic, in that a complete set of male and female organs is present. Thus, the use of this phantom generates radiation dose estimates for testes, breast, ovaries, and uterus.
Results
Sixteen patients (8 men and 8 women) underwent 18F-EF5 PET or 18F-EF5 PET-CT imaging to characterize the biodistribution and dosimetry of 18F-EF5. Turku accrued 6 subjects (4 men and 2 women), and Penn accrued 10 subjects (4 men and 6 women). Patient characteristics are outlined in Table 1. The mean patient age was 43 years (range 21–62), and the mean patient weight was 84.1 kg (range 58.0–128.1 kg).
P#, patient number; UC, urinary clearance; BSUV, blood standardized-uptake value; IA, injected activity; CT, computed tomography; PET, positron emission tomography.
Patients received a mean 18F-EF5 dose of 217 MBq (range 107–364 MBq). The mean, minimum, and maximum residence times for each directly measured organ are presented in Table 2. The critical organ was the urinary bladder wall followed by the gall bladder, liver, kidney, brain, lung, and heart wall. Organs contoured and analyzed within only the Turku dataset were the pancreas, spleen, and cortical bone as a result of the availability of the co-registered CT images.
18
Note that values for the pancreas, cortical bone, and spleen were only available for the Turku patients, due to availability of the PET/CT camera; n=6.
Radiation dose estimates were calculated for the equivalent adult male phantom and are detailed in Table 3. The dose estimates were conservatively based on an assumed bladder voiding every 4.8 hours. For all 16 subjects, the mean urinary bladder wall radiation-absorbed dose was the highest at 0.12±0.034 mSv/MBq (mean±SD), with a range of 0.069–0.20 mSv/MBq. The mean organ radiation dose was not greater than 0.026 mSv/MBq in any of the other organs studied (Table 3). In addition, no individual patient had an organ radiation dose (other than the bladder wall) exceeding 0.051 mSv/MBq. The effective dose equivalent (EDE) and the effective dose were estimated to be 0.021±0.003 and 0.018±0.002 mSv/MBq, respectively. Table 3 also details the comparison between the mean radiation dose values for the Turku patients versus the Penn patients (presented as a ratio of Turku:Penn). All values were within a few percent at both sites, except for the urinary bladder wall (1.5×) and gall bladder (1.5×). This is reflected in the overall faster drug-decay coefficients calculated by Equation 1. Using heart as a surrogate for blood (since by HPLC, we know that blood contains almost entirely nonmetabolized drug), the apparent drug half-lives are ∼7.5 and 10.5 hours, for Turku and Penn, respectively.
Values expressed as 1.0E-02 are equivalent to 1.0×10−02.
COV, coefficient of variation.
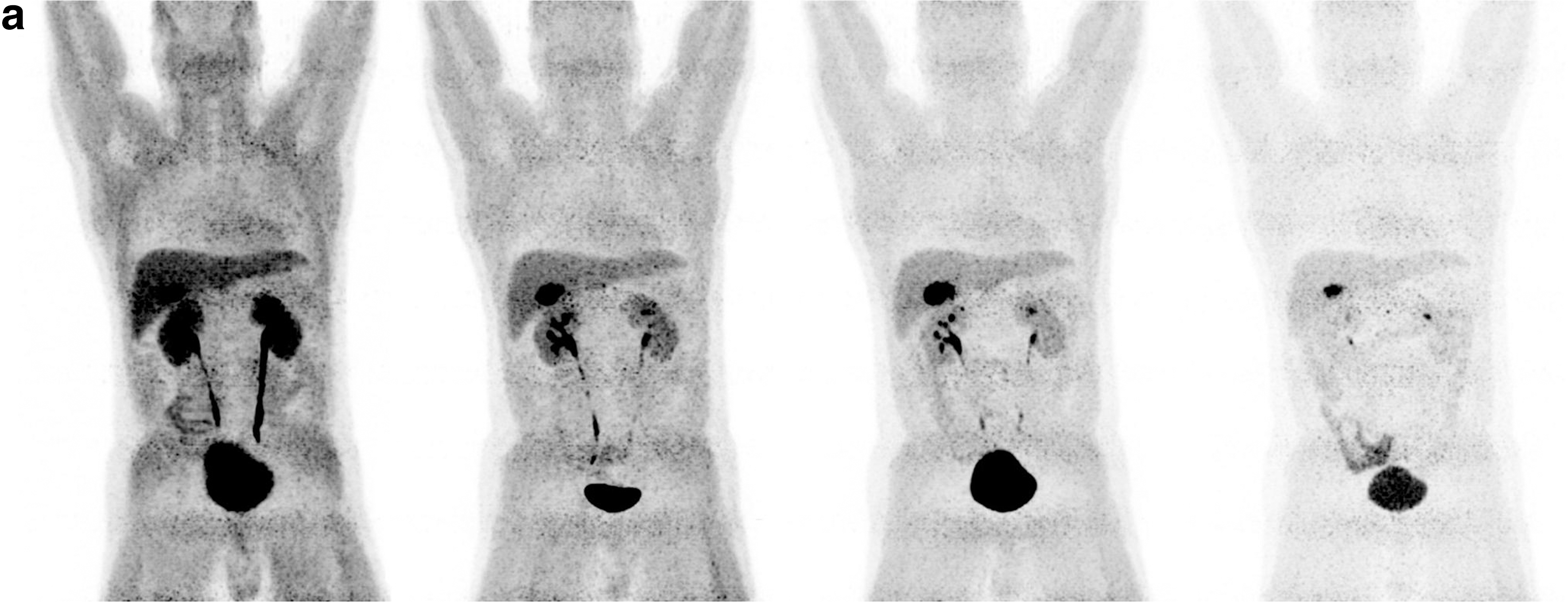
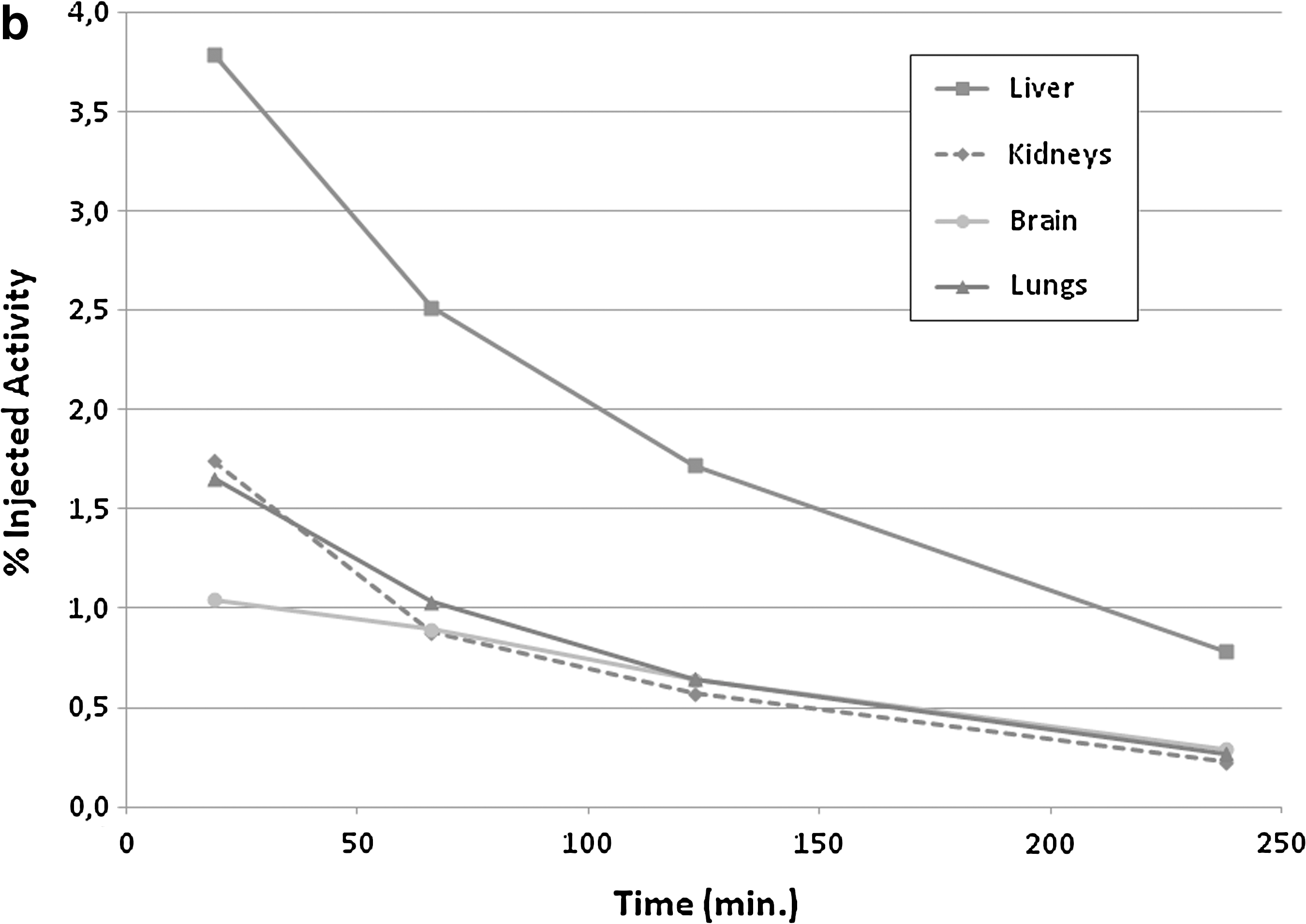
Figure 1a shows the typical biodistribution of 18F-EF5 over time as assessed with four sequential rapid PET/CT acquisitions over 4 hours (Turku subject #2). Each image shows the activity concentration (in the same plane) at each imaging time point. Intense uptake in the urinary bladder occurs relatively rapidly, but decreases over time as urine voiding occurs. This patient was in clinical remission at the time of imaging, and no disease was noted on interpretation of the CT scan. Figure 1b and c show the time-activity curves for the same subject for select organs and whole body versus urine, respectively.

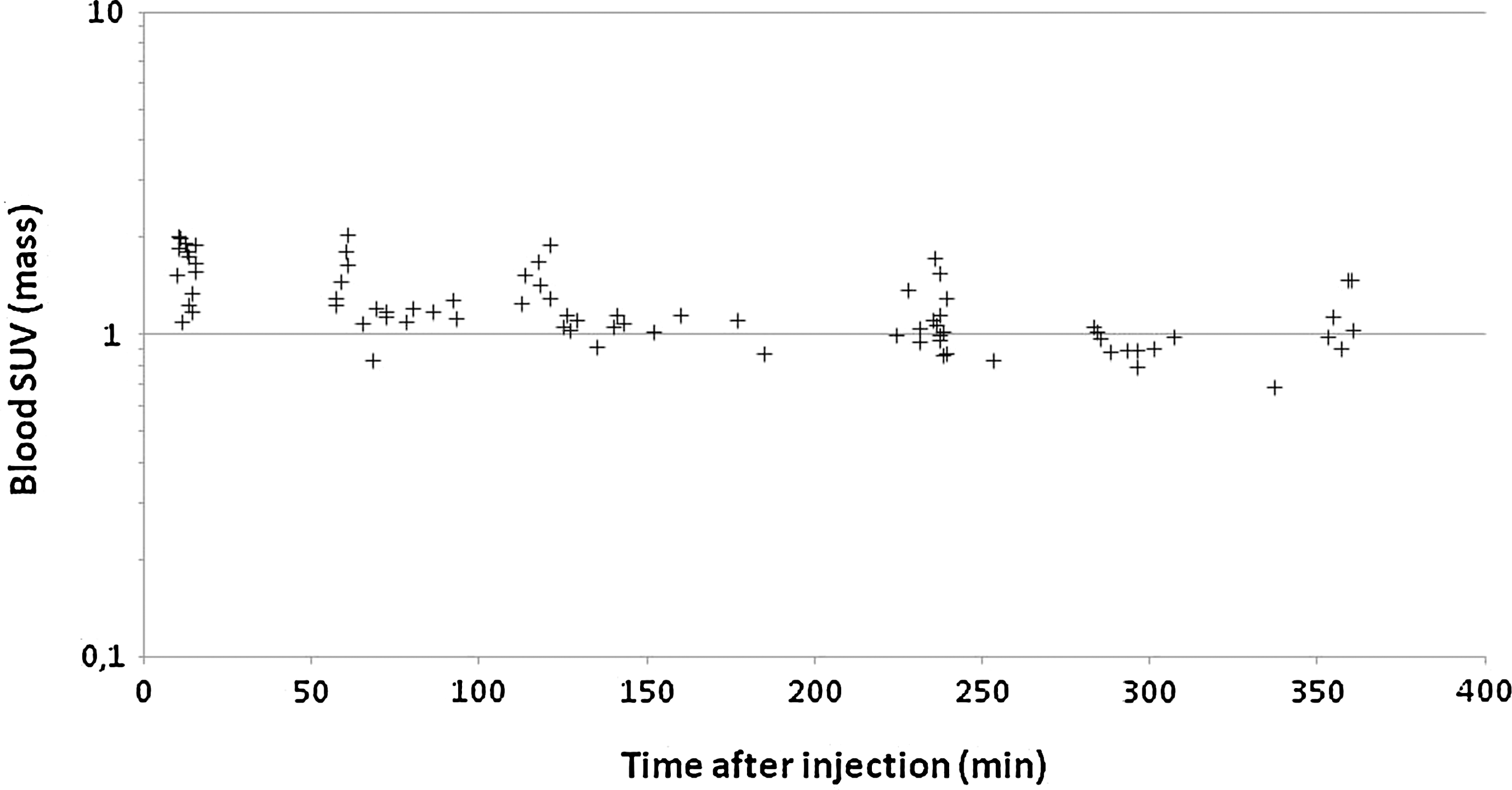
For all patients, urinary excretion of 18F-EF5 averaged 25% (range 12.4–50%) of injected activity over 320 minutes (range 233–364) postinjection. Evaluation of blood SUV data after 18F-EF5 infusion demonstrated rapid equilibration over the whole body with the initial mean blood SUV samples of 1.63±0.31 at times <15 minutes (see Figure 2). The overall blood SUV mean was 1.24±0.33 and was in equilibrium with the whole-body distribution at all times sampled (12–360 minutes), as shown in Figure 2.
Blood standardized-uptake value (SUV) values calculated from gamma counts.
18F-EF5 was well tolerated in all subjects. There were no significant adverse events noted. Similarly, there were no significant increases in serum creatinine, BUN, AST, ALT, or total bilirubin, based on samples taken 4 hours after injection of 18F-EF5 (p>0.05, two-tailed t-test). No clinically significant changes in vital signs (heart rate, systolic and diastolic blood pressure, respiratory rate, or temperature) and no electrocardiographic abnormalities were seen.
Discussion
EF5 is a fluorinated derivative of etanidazole, which has a very high degree of biological stability, and is distinct from other 2-nitroimidazole derivatives because of its high lipophilicity (octanol-to-water coefficient=5.7). 15 This allows for a rapid and uniform biodistribution across all body organs and, with the lack of nonoxygen-dependent metabolism, an improved signal-to-noise imaging ratio. 15 Initial studies with head and neck cancer patients suggest that it is feasible to image hypoxia with 18F-EF5 and PET/CT, and its initial perfusion provides data comparable to labeled water. 20
Before investigating the use of 18F-EF5 in a broad range of malignancies, we studied the safety and radiation dosimetry of 18F-EF5 in patients with oncologic malignancies. As this was primarily a biodistribution study, patients with minimal disease or who had no active disease were included. The included patients did not have evidence of clinically significant cardiac, renal, or liver dysfunction. Thus, it is reasonable to assume that the biodistribution and excretion data of those patients are consistent with data of healthy subjects.
In this study, more detailed data were available for dosimetric calculations compared to the previously mentioned pilot study. 15 For Turku subjects, the CT image-based delineation of the organ VOIs allowed a more accurate definition of the individual organ activity concentration. The number of the patients in this study (n=16) was higher than in the pilot study (n=10). Two independent sites conducted the current study, and 18F-EF5 was synthesized according to local procedures approved by institutional quality-control policies.
The results of this study demonstrate that 18F-EF5 is safe, and that the radiation exposure is clinically acceptable. For all 16 subjects taken together, the mean urinary bladder wall radiation absorbed dose was the largest, 0.12±0.034 mSv/MBq (mean±SD), with a range of 0.069–0.20 mSv/MBq. Since 18F-EF5 is primarily excreted in the urine, it was a reasonable observation that the urinary bladder wall had the largest dose. Importantly, no individual subject had an organ radiation dose (other than the bladder wall) exceeding 0.051 mSv/MBq. The average EDE of 18F-EF5 was determined in this study to be 0.021±0.003 mSv/Mbq, which is comparable to that reported in the previously published pilot study (0.029±0.0056). 15 The reported EDE in this study is lower than that of 18F-FDG (EDE=0.027 mSv/MBq) 21 and comparable to what has been seen for 18F-FMISO at 0.013 mSv/Mbq. 22 Additionally, based on the blood and organ SUV values, EF5's biodistribution occurs uniformly within minutes of injection and remains relatively constant.
The average COV in this work's pooled dataset was only 8%. The average COV for the Penn and Turku datasets, separately, were 6% and 8%, respectively. We therefore conclude that it is reasonable to use the pooled data for radiation dose estimates for this radiopharmaceutical. In the pooled dataset, there were two organs whose COV approached or slightly exceeded 30%, namely the gall bladder (36%) and the urinary bladder wall (28%). Nevertheless, the variations of organ doses in this study were moderately low, and in most organs, the variations were lower than in the previous 18F-EF5 dosimetric study. 15
As can be seen from the absorbed dose estimates (Table 3), the highest coefficients of variation occurred for the two excretory paths (urinary bladder and gall bladder), where the ratio of calculated doses for patients from Turku:Penn averaged 1.5. We believe that this is caused by a faster rate of drug clearance in the Turku group, and this is most likely caused by the lower drug concentration allowed by their high-specific technique for making labeled fluorine gas. By considering the fitted exponential change in drug concentration with time (using data from heart, which is regarded as the best surrogate of blood activity), the apparent drug half-lives were 7.5 versus 10.5 hours, for Turku versus Penn, respectively. These correspond to initial drug concentrations of ∼0.5 versus 50 nM, respectively. The drug–decay estimates are not very accurate due to the short times involved in the measurements, but may be compared with those obtained in an earlier study using much higher EF5 concentrations (11.7 hour for 50-μM initial drug concentration). 8 Thus, the approximate initial drug concentrations now studied using EF5 involve a range of roughly 100,000, with a consistent trend of decreased half-life as the drug concentration decreases, though by a total of <2-fold for a 100,000-fold change in drug concentration. Nevertheless, a specific study focusing on the concentration difference would be needed to get more evidence of potential effect on biodistribution.
Conclusions
In this study, 16 patients with known or suspected oncologic malignancies underwent 18F-EF5 injection (mean of 217 MBq) with serial whole-body PET imaging. 18F-EF5 infusion was well tolerated without any significant adverse events. There were no clinically significant changes in blood chemistries or vital signs. As a result of our clinical study, we consider 18F-EF5 to be safe for patients. The biodistribution of 18F-EF5 demonstrates rapid equilibration with primary clearance through the urinary tract. As with any radiotracer with primary excretion in the urine, bladder doses can be minimized by active hydration and frequent voiding. The average EDE of 18F-EF5 was found to be 0.021±0.003 mSv/MBq, which is less than that of 18F-FDG (EDE=0.027 mSv/MBq). 21 Our study suggests further development of 18F-EF5 as a marker of tissue hypoxia and treatment resistance.
Footnotes
Acknowledgments
The authors wish to thank the medical and laboratory technologists at the Department of Radiation Oncology, the University of Pennsylvania, and at the Turku PET Centre for their assistance. This work was supported by the Varian Medical Systems, Palo Alto, California.
Disclosure Statement
Financial support was provided by the Varian Medical Systems.