
Abstract
Metastatic disease after successful treatment of the primary tumor continues to be a therapeutic challenge. Enhancement of therapeutic effects by the administration of unlabeled monoclonal antibodies (mAbs) after radioimmunotherapy (RIT) may provide a means of preventing or delaying the development of metastatic disease. In the present study, Brown Norway rats with syngeneic grafted colon carcinomas were administered the minimal effective therapeutic dose of 400 MBq/kg lutetium-177 (177Lu)-DOTA-BR96. After 2 weeks, half of the animals were given 15 mg/kg unlabeled mAb BR96 as consolidation therapy. Treatment response and toxicity were monitored 100 days after the treatment with unlabeled BR96. The treatment with unlabeled mAb after RIT resulted in a complete response (CR) in 19 of 19 animals, while RIT alone resulted in a CR in 17 of 19 animals. The additional treatment did not affect the number of animals with metastatic disease or the time to clinical symptoms of metastases. RIT resulted in reversible myelotoxicity. The unlabeled mAb BR96 did not cause any additional toxicity, making it possible to repeat the consolidation therapy.
Introduction
While the treatment of primary tumors is often successful, metastatic disease still poses a considerable challenge. More than 90% of cancer-related deaths are due to metastases. 1 Novel modes of treatment are, thus, needed to reduce or delay the development and growth of distant metastases.
Radioimmunotherapy (RIT) using monoclonal antibodies (mAbs) labeled with radionuclides has been suggested as a suitable method of treating small-volume disease. 2 Lutetium-177 (177Lu) has a physical half life of 6.7 days, which is appropriate for mAbs when considering the biological half life and the kinetics of tumor accumulation. Recently, 177Lu has been used in animal studies on RIT of both established tumors 3,4 and metastases 5 –7 resulting from colon carcinoma and other malignancies. In clinical studies, 177Lu-labeled mAbs have been evaluated as a therapeutic against prostate and ovarian cancer. 8 –11
In an effort to improve RIT, we have used a syngeneic rat colon carcinoma model utilizing the cell line BN7005, in which a complete response (CR) of inoculated tumors was achieved after a single administration of RIT consisting of 177Lu-labeled mAbs, but with the development of distant metastases in about half of the animals after the treatment. 12 In the present study, we evaluate whether consolidation therapy with unlabeled antibodies after RIT enhances the therapeutic effect and/or delays the clinical symptoms of metastatic disease. The choice of unlabeled antibodies for consolidation therapy is based on the well-established therapeutic effects of various unlabeled antibodies in clinical cancer care. 13 In our rat model, we have previously shown that treatment with unlabeled BR96 resulted in a relatively short period of CR of established tumors. 14 Since we use immunocompetent animals, some immunosuppressive treatment should probably be used to prevent the development of immune response to the therapeutic mouse/human chimeric antibodies. We selected and evaluated Cyclosporin A according to Andersson et al. 15 To the best of our knowledge, studies on RIT with subsequent administration of unlabeled mAbs have only been conducted in xenograft models of lymphomas, and not on solid tumors or in syngeneic animal models.
Materials and Methods
Monoclonal antibody
The chimeric (mouse/human) monoclonal IgG1 antibody BR96 (Seattle Genetics, Inc.), binding the tumor-associated antigen Ley, was used. Ley is expressed in the majority of human epithelial tumors, including breast, gastrointestinal, pancreas, non-small-cell lung, cervical, and ovarian cancers, as well as some melanomas. As with the majority of tumor-associated mAbs, BR96 also reacts with some normal tissues, primarily the epithelial cells of the gastrointestinal tract. 16 The binding affinity of BR96 to the BN7005 cell line is high. The dissociation constant by the saturation binding curve analysis was determined to be 4 nM (see next).
The radioimmunoconjugate
BR96 was conjugated with the DOTA chelate (S-2-(4-isothiocyanatobenzyl)-1,4,7,10-tetraazacyclododecane tetraacetic acid; Macrocyclics) according to the method described by Forrer et al. 17 Briefly, the antibody was transferred to 0.2 M sodium carbonate buffer, pH 9.5, by repeated centrifugation using an Amicon-15 filter (Millipore; 30,000 MWCO). The DOTA chelate (2 mg/mL H2O) was added to the BR96 antibody (100 mg/mL) at a molar ratio of 3:1 (DOTA:IgG) and incubated for 1 hour at 37°C. The conjugate was transferred to 0.25 M of ammonium acetate buffer, pH 5.3, by repeated centrifugation using an Amicon-15 filter. The final concentration was adjusted to 10 mg/mL BR96. All the buffers were pretreated with chelex-100 (BioRad), and all the vials were pretreated with 1% HNO3 to remove metals.
The number of DOTA moieties per BR96 molecule was determined using matrix-assisted laser desorption ionization mass spectroscopy. The sample was desalted to 18 MΩ·cm H2O using a centrifugation filter device. The number of DOTA moieties per BR96 molecule was obtained by dividing the increase in molecular mass by 688 (the molecular mass of p-SCN-Bn-DOTA).
The antigen-binding properties (immunoreactivity) of DOTA-BR96 relative to BR96 were determined by saturation binding curve analysis, using BN7005 cells as the target antigen. Briefly, increasing concentrations of DOTA-BR96 and BR96 (40 ng/mL–40 μg/mL) were added to the cell plate in triplicate. After incubation at room temperature for at least 1½ h, the bound DOTA-BR96/BR96 was detected by HRP-anti-human-IgG (Dako), and the equilibrium-binding constant (K d) was calculated using Prism 5.02 software (binding saturation; one site total, nonspecific binding and background constrained to a constant value of zero). The immunoreactivity is given by the following ratio: Kd(BR96)/Kd(DOTA-BR96).
The following procedure was used to label the DOTA-BR96 conjugate with 177LuCl3 (MDS Nordion). Both the DOTA-BR96 conjugate in 0.25 M of ammonium acetate buffer and the radionuclide solution were preheated at 45°C for 10 minutes. The DOTA-BR96 solution was then added to the radionuclide-containing vial and incubated at 45°C for 15 minutes. The reaction was quenched with an excess of DTPA for 5 minutes. The radiolabeled immunoconjugate was then diluted in 1% human serum albumin (HSA; Baxter Medical AB). The radiochemical purity of the labeled immunoconjugate was determined by instant thin-layer chromatography (ITLC), using a 1×9 cm silica-gel-impregnated fiberglass sheet and elution in 0.1 M EDTA. Separation by size-exclusion chromatography together with high-performance liquid chromatography (HPLC) (7.8×300 mm molecular sieving column, Phenomenex SEC S3000; Phenomenex, eluted in 0.05 M sodium phosphate at 1.0 mL/min) was used to check the radiochemical purity and to detect signs of aggregation or fragmentation.
Rat tumor model
Fifty-eight male Brown Norway (BN) rats with a mean body weight of 237 g (SD 15 g) (Harlan) were used. This rat strain is immunocompetent and expresses the BR96-binding antigen in normal tissues, mainly in the epithelium of the gastrointestinal tract, 18 hence mimicking the human situation. The animals were housed under standard conditions and fed with standard pellets and fresh water ad libitum. All experiments were conducted in compliance with Swedish legislations on animal rights and protection, and were approved by the regional animal ethics committee.
BN7005-H1D2 is a cell line established from a 1,2-dimethylhydrazine-induced BN rat colon carcinoma. The radiosensitivity, determined as the fraction of survival after 2 Gy (S2Gy), is 0.5 for this cell line (data not published), which is similar to human colon carcinoma cell lines. 19 The cells were cultured in RPMI-1640 medium (PAA Laboratories GmbH) supplemented with 10% fetal calf serum (PAA Laboratories), 1 mM sodium pyruvate (Gibco, Invitrogen), 10 mM Hepes buffer (Gibco, Invitrogen), and 14 mg/L Gentamicin (Gibco, Invitrogen) at 37°C in a humidified environment with 5% CO2. The cells were washed in phosphate-buffered saline (PBS) and detached by trypsin treatment. Animals were inoculated between the peritoneum and the abdominal wall with 3×105 cells under anesthesia (Isoflurane; Abbott Scandinavia AB).
Treatments
Two weeks after the inoculation with tumor cells, the animals were divided into groups with comparable distributions of body weight and tumor volumes. Group 1 (n=19) was given 400 MBq/kg 177Lu-DOTA-BR96 (150 μg DOTA-BR96 in 0.4 mL saline with 1% HSA). Group 2 (n=10) was given 400 MBq/kg 177Lu-DOTA-BR96 in combination with Cyclosporin A (Sandimmun®; Novartis Sverige AB). The Cyclosporin A treatment (0.2 mL; 10 mg/kg body weight; in saline) was given daily for 5 days starting 1 day before injection of the radiolabeled BR96. Group 3 (n=19) was treated with 400 MBq/kg 177Lu-DOTA-BR96 in combination with Cyclosporin A (administered as just stated). In addition, this group was given unlabeled BR96 (15 mg/kg body weight; in 0.4 mL PBS) 2 weeks after RIT. Both groups 1 and 3 included animals from two experiments.
To evaluate the effect of Cyclosporin A on the development of rat anti-human antibodies (RAHAs), a fourth group of rats (group 4; n=10) was treated with 400 MBq/kg 177Lu-DOTA-BR96 and on day 15, with BR96 (15 mg BR96/kg body weight; in 0.4 mL PBS), without any coadministration of Cyclosporin A.
All compounds were administered via a tail vein. The successful injection of 177Lu-DOTA-BR96 was checked by activity measurements of arterial blood samples drawn a few minutes after the injection. All the injections were based on average body weight.
Monitoring of the effects of treatment
Animals were monitored up to 113 days after the administration of 177Lu-DOTA-BR96. Body weight was recorded, and inoculated tumors were measured with a digital caliper twice a week. Tumor volumes were calculated as tumor length×tumor width 2 ×0.4. CR was defined as a nonpalpable tumor for at least 1 week. Arterial blood sampling was performed twice a week for the first 6 weeks after RIT and then once a week. Myelotoxicity was determined by counting the white blood cells and platelets with a Vet CA530 Medonic Cell Analyzer (Boule Medical). In order to determine RAHA levels, blood plasma was collected from groups 1, 3, and 4 before RIT (day −3), between treatments (day 10), and after treatments (day 29). For the determination of BR96 levels in blood, plasma was collected 3 days after the administration of unlabeled BR96 (day 18).
Rats were sacrificed if the maximal tumor size of 25×25 mm was exceeded, or at the end of the study (day 113). If body weight decreased by more than 20% compared with normal weight progression, or if the general health of the animal was affected during the study, then metastatic disease was suspected and the rat was sacrificed and dissected to confirm metastatic growth. All the rats were systematically dissected by the same person at the time of sacrifice, and the location and number of metastatic sites were recorded. The tumor findings were fixed in 4% paraformaldehyde and embedded in paraffin.
Presence of RAHAs and BR96 in plasma
An ELISA method was used to determine the RAHA concentrations in blood plasma. Briefly, 96-well plates were coated with 50 μL 10 μg/mL DOTA-BR96 for the plasma samples and with 10 μg/mL streptavidin (Pierce) in PBS (Sigma-Aldrich) to determine the standard curve (incubated overnight at 4°C). The plates were then blocked with PBS with 0.05% Tween 20 (PBS-T) for 1 hour at room temperature (Sigma-Aldrich) before the addition of diluted plasma samples or 3.1–200 ng/mL rat IgG-biotin (Jackson ImmunoResearch Laboratories, Inc.) in PBS-T for standard curve determination (two dilutions per plasma sample, all dilutions in triplicate). After incubation for 1 hour at room temperature, the plates were washed, and donkey anti-rat IgG-HRP (Jackson ImmunoResearch) was added to all the wells. The plates were incubated for 1 hour at room temperature. After washing, the substrate solution containing substrate buffer, OPD (o-phenylenediamine dihydrochloride), and H2O2 was added immediately before kinetic measurement in the ELISA photometer (VERSAmax; Molecular Devices, Inc.). The Softmax software was used for calculation of the enzyme rates (mOD/min), for processing of the standard curve (4-parameter), and for calculation of the sample concentrations.
The BR96 concentration in plasma was determined in a corresponding way by first coating the plate with 6 μg/mL rabbit anti-human IgG (Dako) in PBS overnight at 4°C. After blocking with PBS-T, diluted plasma samples and standards (7.81–500 ng/mL BR96) were added in triplicate, and the samples were incubated for 1 hour at room temperature. After washing, rabbit anti-human IgG-HRP (Dako) was added to all wells, followed by incubation for 1 hour at room temperature. Finally, a substrate solution was added, and kinetic measurements were performed as just described.
Immunohistochemistry
Paraffin-embedded tumors and metastases were sectioned and stained for the detection of the BR96 binding antigen. Briefly, 4-μm-thick sections were rehydrated, and the antigens were retrieved using the PT Link pretreatment module (Dako) with an acidic target retrieval solution (pH 6), preheated to 65°C and then heated at 99°C for 20 minutes, followed by rinsing of the slides. Sections were incubated with 5 μg/mL BR96 overnight at room temperature. After washing, the sections were incubated with donkey F(ab)2 anti-human IgG-HRP (Jackson ImmunoResearch Laboratories) for 3 hours at room temperature. Finally, diaminobenzidine (Dako) was added before dehydration and mounting.
Statistical analysis
Statistical analysis of experimental data was conducted using Prism 5.02 (GraphPad Software, Inc.).
Results
Radioimmunoconjugate
The number of DOTA molecules per BR96 molecule was 2.3–2.4. The immunoreactivity, expressed as the ratio of Kd for BR96 and DOTA-BR96, was >0.9. The Kd of DOTA-BR96 was within the 95% confidence interval of Kd for BR96.
After radiolabeling, the specific activity of the 177Lu-DOTA-BR96 conjugate in the two separate experiments was 664 and 730 MBq/mg. ITLC showed the radiochemical purity to be 96%. Less than 2% aggregation and fragmentation were observed with HPLC.
Tumor response
The average tumor volume on day 0, when 400 MBq/kg 177Lu-DOTA-BR96 was administered, was 730 mm3 (SD 380 mm3) in group 1, 610 mm3 (SD 150 mm3) in group 2, and 730 mm3 (SD 340 mm3) in group 3. On day 15, when unlabeled BR96 was administered to group 3, 10 of the 19 animals in this group showed CR, compared with 16 of 19 rats in group 1, and 3 of 10 rats in group 2. Two weeks later (day 28), all the rats in groups 2 (10 of 10) and 3 rats (19 of 19) showed CR, while 17 of 19 rats in group 1 showed CR. The time before CR was reached was significantly longer in the animals given Cyclosporin A than in the animals treated with RIT only (ANOVA, p<0.0001) (Fig. 1).

The number of days elapsed before complete response (CR) in the different treatment groups
The two remaining tumors in group 1 started to grow again after day 15, and resulted in sacrifice of the rats on days 53 and 106. One rat in group 1 had local recurrence after 19 days of CR (recurrence detected on day 29, sacrificed on day 44). In group 2, one recurrence was detected on day 45 with subsequent sacrifice on day 73. In group 3, 3 rats had local recurrences after 42, 47, and 82 days of CR (detected on days 57, 57, and 92; sacrificed on days 78, 106, and 113, respectively) (see Table 1).
Disseminated disease
In all treatment groups, half of the animals (i.e., 5 of 10 or 10 of 19) were free from detectable disease at the end of the study (see Table 1). In group 1, treated with RIT only, symptoms of metastatic disease were observed, and metastases were confirmed in 8 rats on days 44–106. In group 2, treated with RIT and Cyclosporin A, metastatic disease was observed in 4 animals on days 31–105. In group 3, treated with RIT in combination with BR96 and Cyclosporin A, clinical symptoms of metastatic disease were observed, and metastases were confirmed in 8 rats on days 78–106. The time before the detection of metastatic disease did not differ between the treatment groups (Fig. 1). Three rats, one from each group, were found to have metastatic disease at the end of the study without clinical symptoms. Metastases were found in several organs, often in the same rat; for example, in the liver, spleen, pancreas, lymph nodes (both thoracic and abdominal), mesentery, and lung. The distribution of metastatic sites did not differ between the treatment groups.
Immunohistochemistry
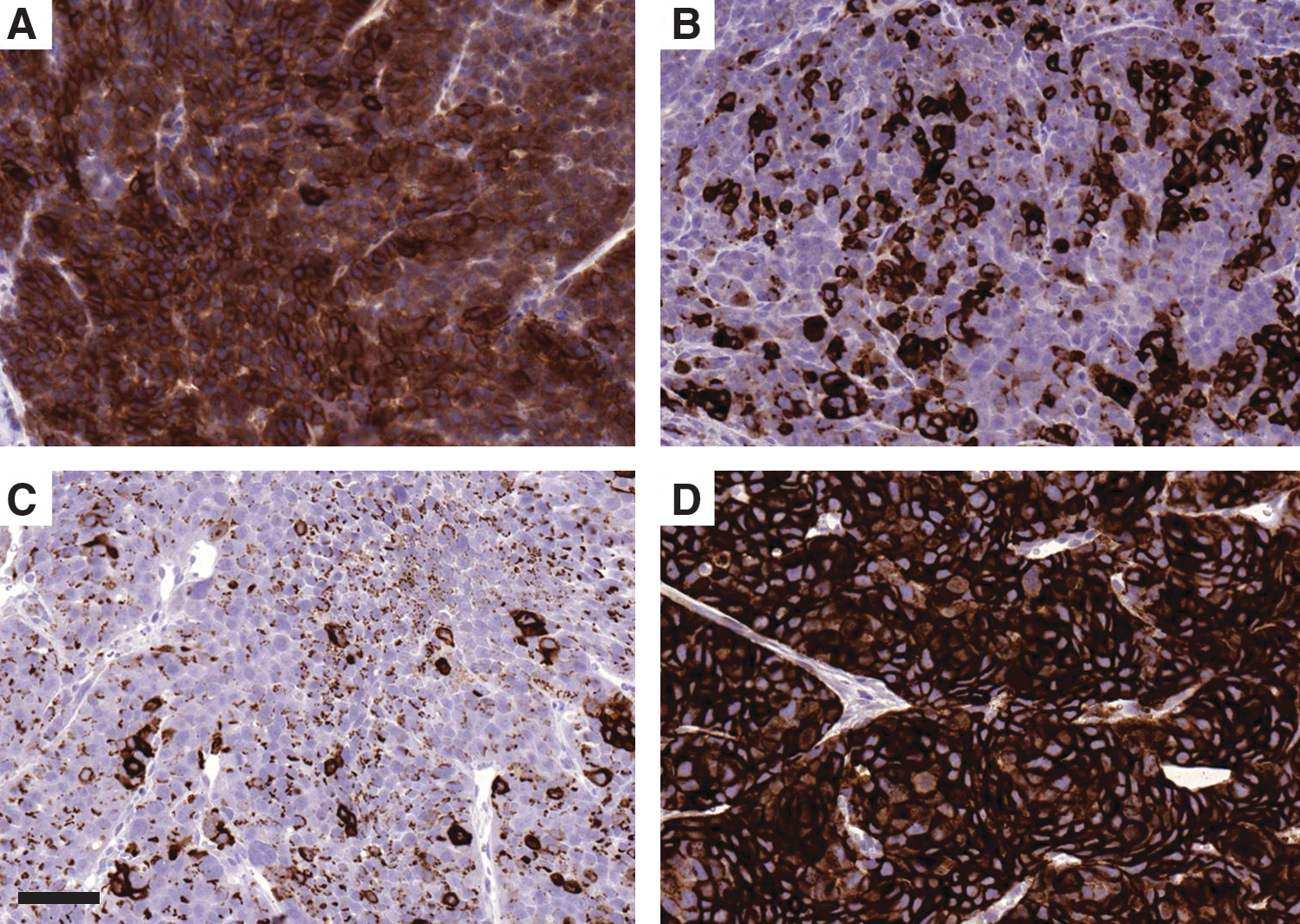
All tumors (inoculated and recurrent) and metastases stained with BR96 for the detection of antigen expression were positive, but differed in both staining intensity and pattern (Fig. 2). The differences in staining were not correlated to the treatment group. In cases where both local tumors and metastases from the same rat were stained, the staining was often comparable in both types of tissue.
Stained tumor sections showing the BR96 targeting antigen in untreated tumor
The effect of Cyclosporin A
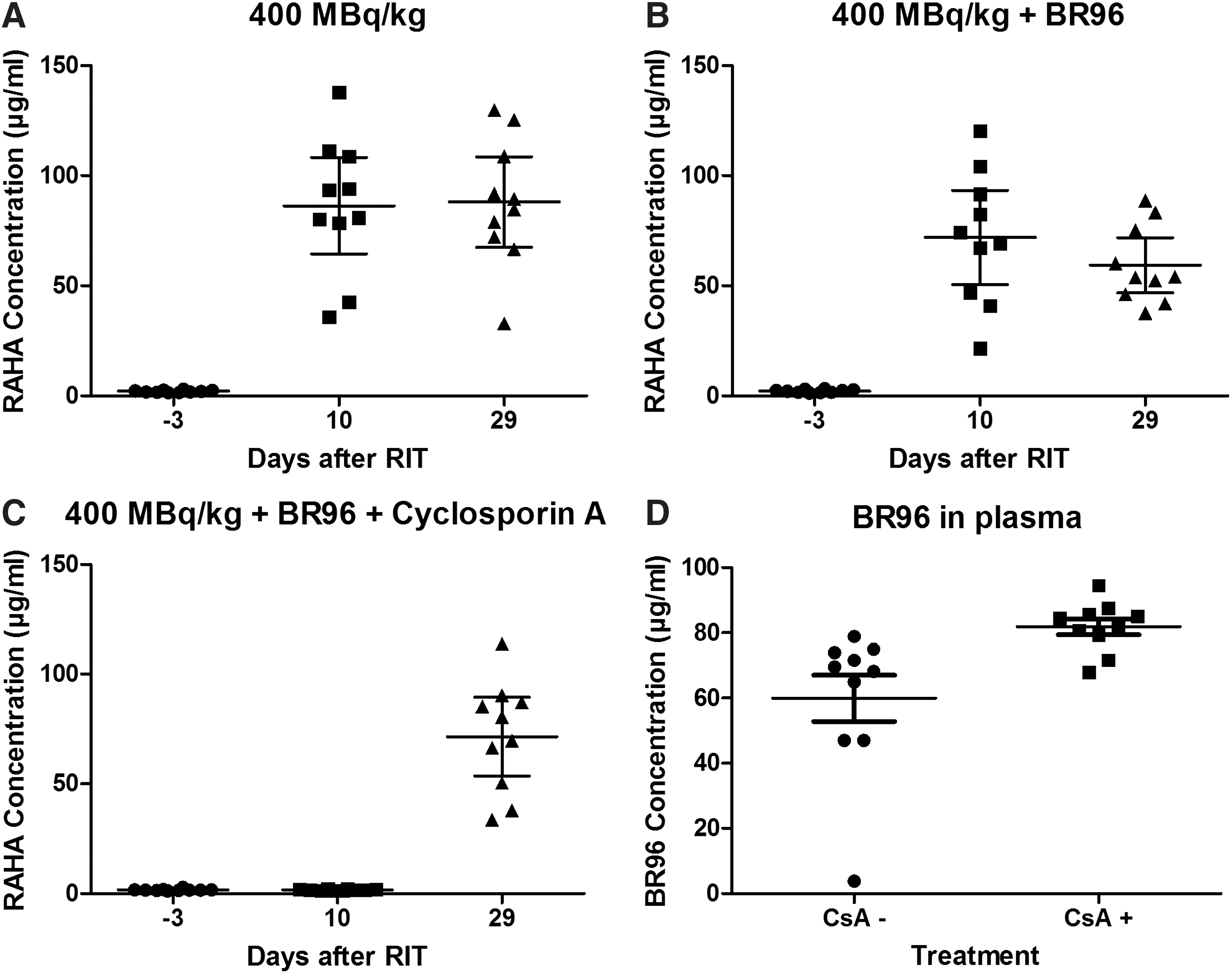
The effect of Cyclosporin A was evaluated as the presence of RAHAs before, between, and after treatments, and as an effect on the BR96 concentration in blood plasma 3 days after administration. The RAHA concentration in plasma before treatment was 2.0, 1.7, and 2.2 μg/mL in groups 1, 3, and 4, respectively (Fig. 3). Rats treated with Cyclosporin A and unlabeled BR96 (group 3) had 1.7 μg/mL RAHA in plasma 10 days after RIT treatment, while the groups not treated with Cyclosporin A had 86 (group 1) and 72 μg/mL (group 4) RAHA in plasma. In rats treated with Cyclosporin A, the mean concentration of BR96 in plasma 3 days after administration was 82 μg/mL, and in rats not treated with Cyclosporin, it was A 66 μg/mL. Both parameters displayed significant differences between the treatment groups with p-values of <0.0001 (RAHA) and 0.0021 (BR96) (Mann–Whitney's test, GraphPad Prism Software).
Presence of rat anti-human antibodies (RAHAs) before RIT, after RIT, and after consolidation therapy with unlabeled monoclonal antibodies in group 1
Toxicity
A decrease in body weight (<10%, nadir day 3 p.i.) was seen after the administration of 177Lu-DOTA-BR96. Body weight was recovered at the time of the administration of unlabeled BR96 (day 15). Myelotoxicity was observed as a decrease in both white blood cell counts and platelet counts after the administration of 177Lu-DOTA-BR96 (Fig. 4). White blood cell counts reached the nadir on day 7 and were restored on day 50. Platelet counts reached their nadir on day 15 and were restored on day 22. No differences were found between the treatment groups. Treatment with unlabeled BR96 did not result in any observable toxicity, including weight loss.
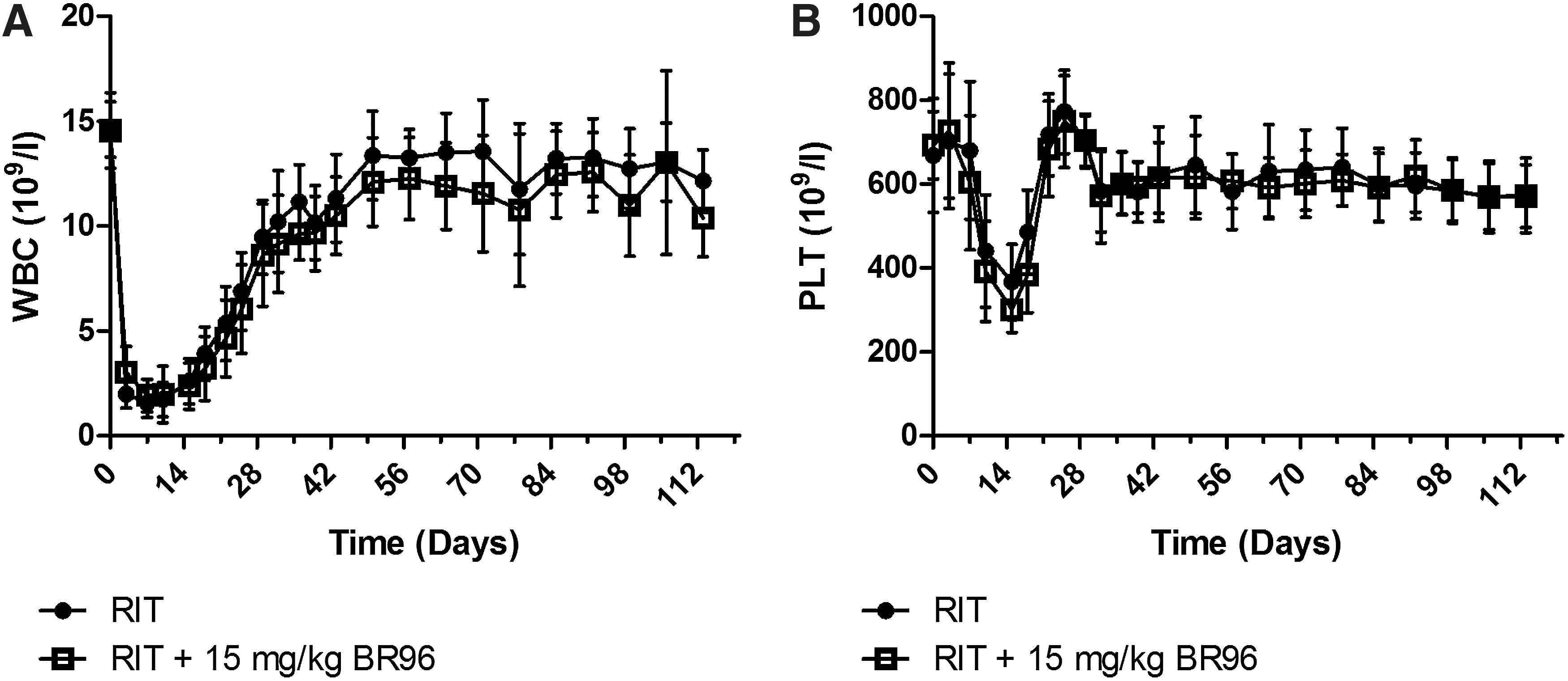
Myelotoxicity after RIT with 177Lu-DOTA-BR96. The consolidation therapy of 15 mg/kg body weight unlabeled BR96 was administered to one group 15 days after RIT. The blood levels of white blood cells (WBC)
Discussion
In this study, we evaluated consolidation therapy after RIT through subsequent administration of unlabeled mAbs. This additional treatment of 15 mg/kg unlabeled BR96 did not prevent the recurrence of the inoculated tumors, compared with animals only given RIT (400 MBq/kg 177Lu-DOTA-BR96). Cyclosporin A was coadministered to the animals to avoid an immune response to the mAbs. Treatment with Cyclosporin A did not affect the number of animals showing CR or metastatic disease, but the time required to achieve CR was prolonged (Fig. 1).
Metastases were found in various organs, for example, liver, lung, and throughout the abdomen. Some rats had metastases in more than one organ. The number of animals affected and the distribution of tumor sites did not differ between the treatment groups, and the additional treatment did not delay metastatic disease (Fig. 1).
Immunohistochemical staining for detection of the BR96-binding antigen in inoculated or recurrent tumors and in metastases resulted in positive staining in all sections (Fig. 2). The majority of the sections demonstrated intense staining of all tumor cells, indicating the possibility of repeating the targeted treatment with the same therapeutic antibody, with or without radiolabeling. There was a tendency toward the selection of tumor cells not expressing the BR96-binding antigen compared with untreated tumors (detected by hematoxylin staining, data not shown).
Body weight is a major indicator of general health. Treatment with 400 MBq/kg 177Lu-DOTA-BR96 resulted in temporary weight loss (nadir at day 3). Additional weight loss was not seen after the administration of 15 mg/kg BR96, which is in agreement with previous findings. 14 Later in the study, weight loss was correlated to confirmed metastatic disease (data not shown). The degree of myelotoxicity did not differ between the treatment groups (Fig. 4). The unlabeled BR96 was not expected to have any effects on the bone marrow. It appears that the treatment with Cyclosporin A did not result in any additional myelotoxicity.
The maximal tolerable dose (MTD) in this syngeneic rat tumor model had previously been determined to be 600 MBq/kg 177Lu-labeled BR96. 12 Mårtensson et al. showed that treatment with the MTD resulted in CR in all animals, although metastases were found in 3 of 6 rats. This indicated the need for maintenance treatment. The activity injected in this study (400 MBq/kg 177Lu-DOTA-BR96) was the minimal effective therapeutic dose, defined as the lowest activity resulting in CR in 5 of 6 animals after 14 days. 20 The minimal effective dose was chosen to prevent overtreatment during RIT, to provide for some toxic effects of the consolidation therapy, without reaching dose-limiting toxicity in the case of combined therapy. Unlabeled mAbs might have better “cell-killing potential” on single cells and small cell clusters than antibodies labeled with low-range β-emitters such as 177Lu. The unlabeled BR96 dose of 15 mg/kg was chosen, as it resulted in CR in 4 of 6 rats in a previous study in the same rat tumor model, 14 although the primary tumor recurred in 3 of these rats before 45 days after treatment, and the 4th rat with CR died due to disseminated disease on day 77. Hence, a single administration of unlabeled BR96 was not sufficient for the treatment. Unlabeled BR96 do not have cytotoxic effects on the used cell line in vitro (data not published), but might act via immunologic mechanisms such as “antibody-dependent cell-mediated cytotoxicity” or “complement dependent cytotoxicity” in vivo. 13,21 In the present study, the unlabeled BR96 was administered 15 days after the initial 177Lu-DOTA-BR96 treatment. This time interval between treatments was chosen for three reasons: (1) the remaining tumors were small, (2) the animals had recovered from early toxic events such as weight loss, and (3) the white blood cells had started to recover after the RIT. Clinical studies have proved that a combination of rituximab and 90Y-ibritumomab tiuxetan as consolidation therapy after initial chemotherapy results in improved progression-free survival in patients with non-Hodgkin lymphoma. 22 However, the rituximab was given before the RIT to prevent the binding of radiolabeled antibodies to CD20-positive cells in the blood and lymphoid organs. The preadministration of unlabeled mAbs might reduce the therapeutic effect of the RIT by blocking antigens in the tumor. 23 In our study, we administered the unlabeled antibody after the RIT, in an attempt to enhance the therapeutic effect and prevent metastatic disease. The consolidation therapy with the unlabeled antibody was not repeated, as the dose was high enough to result in CR in a previous study. 14 In addition, we wanted to be able to monitor possible late toxicity after the administration of unlabeled antibodies. The repeated administration of unlabeled mAbs after RIT might have delayed recurrence, resulting in a significantly prolonged survival. To the best of our knowledge, studies on RIT with subsequent administration of unlabeled mAbs have only been conducted in xenograft models of lymphoma. The administration of 4 weekly doses of unlabeled anti-CD20 IgG starting 1 week after RIT with the same mAb enhanced the effect of RIT and improved survival compared with RIT alone and starting the administration of unlabeled anti-CD20 IgG before RIT. 24 Biodistribution data showed a lower tumor uptake of the radioimmunoconjugate when unlabeled anti-CD20 IgG was administered before RIT, which might explain the lower therapeutic effect. Hence, consolidation therapy with unlabeled mAbs after RIT might be effective; however, it will probably be less effective in patients given a high predose. 25
Cyclosporin A has previously been used to prevent the formation of anti-murine antibodies in clinical studies of both fractionated RIT and combinations of imaging and therapy with the same mAb. 26 –29 The Cyclosporin A treatment resulted in significantly lower concentrations of RAHA in plasma, comparable to pretreatment levels (Fig. 3). The same finding was reported by Andersson et al. 15 in a preclinical study of Cyclosporin A in combination with immunotoxins. The range of RAHA concentration in the different groups in the present study may be explained by the myelotoxicity, as the production of RAHA might be lower when the number of white blood cells is decreased, or by individual differences. The effects of Cyclosporin A were also seen as higher plasma concentrations of BR96 3 days after administration in animals treated with Cyclosporin A, compared with nontreated animals. RAHA is expected to increase the clearance of BR96, resulting in decreased therapeutic effects. The effects of Cyclosporin A were not sustained after the administration of unlabeled antibodies and, therefore, additional Cyclosporin A treatment will be needed to be able to repeat the antibody treatment in this antibody/tumor animal model (except for the very last antibody administration). It has been suggested that Cyclosporin A itself may enhance tumor growth, 30 although no difference was seen between the treatment groups in the present study.
In a previous study using doxorubicin-conjugated BR96 (BR96-Dox) in the same syngeneic rat tumor model, treatment with 15-deoxyspergualin prevented the formation of RAHA. 18 Deoxyspergualin was not used in this study, as the combined treatment enhanced the therapeutic effects, thereby making it difficult to evaluate the effect of unlabeled mAbs alone. The need to prevent an immune response to the radioimmunoconjugate is reduced in the clinical situation by using humanized antibodies. However, the clinical application of immunotoxins may still require immunosuppressive treatment to prevent immune reactions to the toxin part.
In conclusion, treatment with unlabeled antibodies after RIT resulted in an enhanced therapeutic effect on inoculated tumors, but neither prevented metastatic disease nor improved survival. Cyclosporin A prevented an immune response to the radioimmunoconjugate but delayed the rejection of tumors.
Footnotes
Acknowledgments
The authors would like to thank Dr. Peter Senter (Seattle Genetics, Seattle, WA) for kindly providing the mAb BR96. The research was supported by grants from the Swedish Cancer Society, Mrs. Berta Kamprad's Foundation, Gunnar Nilsson's Foundation, The Crafoord Foundation, Government funding of clinical research within the Swedish National Health Service, the Lund University Medical Faculty Foundation, and The Lund University Hospital Fund.
Disclosure Statement
The authors have no affiliations, memberships, funding, or financial holdings that might be perceived as affecting the objectivity of this article.