
Abstract
Purpose:
The purpose of this study is to assess the potential of 18F-fluorodeoxyglucose (18FDG) positron emission tomography/computed tomography (PET/CT) imaging for the diagnosis of cervical metastasis of carcinoma of an unknown primary tumor (CUP) and to determine whether the maximum standardized uptake value (SUVmax) is a prognostic factor.
Methods:
Twenty-five consecutive patients with cervical metastasis of CUP were retrospectively analyzed by PET/CT between July 2007 and July 2011.
Results:
FDG PET/CT suggested a primary tumor in 21 out of 25 patients (84.0%). The sensitivity of FDG PET/CT in detecting the primary tumor was 73.3% (11 of 15), and the positive predictive value was 52.4% (11 of 21). The median follow-up duration of survival patients was 10.4 months (range: 0–30 months). The estimated 2-year overall survival rate of all patients was 50.0%. Univariate analyses did not reveal a significant difference in overall survival between the group of 11 patients identified by pathology and the 14 patients not identified by pathology (overall survival was 57.1% and 49.1%, respectively; p=0.468). The median SUVmax was 7.6. In the log-rank test, patients with a low SUVmax (≤7.0) in cervical lymph nodes had a significantly higher survival rate at 2 years (87.5% vs. 21.2%; p=0.007) than patients with a high SUVmax (>7.0).
Conclusions:
Although our study was inconclusive due to the small sample size, our results suggest that FDG PET/CT may be an effective diagnostic workup in the cervical metastasis of carcinoma from an unknown primary tumor (UPT). In the present study, SUVmax of PET/CT in the cervical lymph node may serve as a prognostic factor of cervical metastasis of carcinoma from a UPT based on the limited number of patients. Further studies are needed to confirm these findings.
Introduction
Metastasis with an occult primary is a challenging issue. Cervical metastasis of carcinoma accounts for approximately 3%–7% of all head and neck cancers. 1 Although the primary carcinoma of some cervical metastases of carcinoma may be found by a routine examination, including a complete physical examination, panendoscopy, and conventional imaging, such as computed tomography (CT), magnetic resonance imaging (MRI), and even “random” biopsies, such as tonsillectomies, 2 most carcinomas of unknown primary tumors (CUP) remain undetected by conventional diagnostic procedures. 1 The prognosis of patients with CUP is unfavorable, with a median survival time of less than 1 year. If the primary site is identified and specific therapy is started, the median survival time can be increased to 23 months. 3 –5 Therefore, the accurate identification of occult primary sites is important, as therapy can then be focused on the known site of origin, decreasing treatment-related morbidity and improving therapeutic efficacy. 3 –7
18F-fluorodeoxyglucose (FDG) positron emission tomography (PET/CT) has provided new insights to this diagnosis. 1,8 The comprehensive review of Rusthoven et al. on the use of 18FDG-PET in the detection of CUP, which comprised 16 studies with 302 patients, reported 88.3% sensitivity, 74.9% specificity, and 78.8% accuracy. 8 In contrast to PET, relatively few studies have been published on the effectiveness of PET-CT fusion studies in cervical metastasis of carcinoma from an unknown primary tumor (UPT). 2,4,9 However, studies show a large difference of between 0% and 44% in PET/CT sensitivity in localizing an occult primary. 2 –4,9 Therefore, the efficacy of PET/CT in detecting primary sites in patients with CUP remains to be determined.
This study aimed at assessing the potential of 18FDG PET/CT imaging for the diagnosis of cervical metastasis of CUP and at determining whether the maximum standardized uptake value (SUVmax) is a prognostic factor.
Materials and Methods
Patients
Twenty-five consecutive patients who presented to the Department of PET/CT Center at First Affiliated Hospital, College of Medicine, Zhejiang University, with cervical metastasis of CUP were retrospectively analyzed by PET/CT between July 2007 and July 2011.
The inclusion criteria were biopsy-proven cervical metastasis of carcinoma before PET/CT. Patients were excluded from the study if they had a history of head and neck cancer, if a primary tumor site was evident on a physical examination, or if primary tumors of the neck (such as lymphoma or sarcoma) were diagnosed. Patients with primary tumors detected by visual panendoscopy were also excluded. Once patients were enrolled, a complete medical record review was performed. Records from the Department of Medical Records of our hospital as well as relevant departments (Department of Otolaryngology, Oral and Maxillofacial Surgery, Radiotherapy, and Surgical Oncology) were included in the analysis. Data collected included demographic information, physical examination findings, CT imaging results (all patients who had undergone CT scanning in different sites, including head and neck, or/and lung, or/and abdomen, etc), and pathology results.
When imaging studies detected suspicious primary tumor sites after the PET/CT scan, we obtained biopsy specimens by endoscopy or puncture biopsy. Directed biopsies, tissue excisions (e.g., tonsillectomy), and a neck dissection were performed under the same general anesthetic.
The study was approved by the institutional review board of the First Affiliated Hospital, College of Medicine, Zhejiang University.
PET/CT scan
Whole-body imaging was performed using a combined PET/CT scanner (Biograph Sensation 16, LSO 39-ring; Siemens Medical, Erlangen, Germany). After at least 4–6 hours of fasting, patients received an intravenous injection of FDG at 5.5–7.4 MBq (0.15–0.20 mCi)/kg of body weight. Patient blood glucose levels were checked before the 18F-FDG injection. Data acquisition of the diagnostic CT was started 60–90 minutes after FDG administration. The data acquisition procedure was as follows: first, a 16-section multi-detection row CT scanning was performed from head to mid-thigh at 120 kV, 50 mAs; then, with a tube rotation time of 0.5 seconds, a 2–5-mm-thick section was matched to the PET section thickness, followed by a three-dimensional PET, with the patient in the same supine position. The PET emission scan covered the region from subcranial to mid-thigh; the brain scan required another bed position. Acquisition time was 2 minutes per bed position. The total imaging time of a PET/CT study lasted approximately 20 minutes. Attenuation correction was based on CT. The PET images were reconstructed iteratively using ordered subset Syngo Speaking software (Wizard Workstation; Siemens Medical). PET, CT, and fused PET/CT images were generated and reviewed on a computer; co-registered images were displayed on a workstation.
Data and statistical analysis
The PET/CT scans were independently interpreted by two experienced members of our PET center who were unaware of the histology of the metastatic sites. Any differences in their respective interpretations were settled with a final unanimous opinion. The standardized uptake value (SUVmax) was collected from the predominant lesion and calculated based on the attenuation-corrected images, amount of injected 18F-FDG, and body weight: {SUV=[decay corrected activity (kBq)/tissue volume (mL)]/[injected FDG activity (kBq)/body weight (g)]}. 10 When multiple lymph nodes were found, only the lymph node with the highest SUV was used.
Statistical analysis was performed using SPSS 16.0 software (SPSS Inc., Chicago, IL).
Results
Tables 1 and 2 summarize the characteristics of 25 patients with cervical metastasis of a CUP. The study comprised 18 men and 7 women, with a mean age of 54.5 years (range: 32–77 years). All known sites of lymph node involvement were visualized on PET/CT. The metastatic lymph nodes were located in neck regions II, III, IV, V, or VI or in overlapping regions. The involved levels of the neck were as follows: level I, 1 patient (4.0%); level II, 10 (40.0%); and level V, 1 (4.0%); 13 patients (52.8%) had nodes involving multiple levels. Fifteen lymph nodes were smaller than 3 cm in diameter, and 10 were larger than 3 cm but smaller than 6 cm in diameter.
Pt, patient; PDMS, poorly differentiated metastatic carcinoma; PR, pathological result; ND, neck dissection; SCC, squamous cell carcinoma; CCR, concurrent chemoradiotherapy; CLN, cervical lymph node; SUVmax, maximum standardized uptake value; FDG, fluorodeoxyglucose.
When multiple lymph nodes were found, only the lymph node with the highest SUV was used.
NED, no evidence of disease; DOD, die of disease.
FDG PET/CT suggested a primary tumor in 21 out of the 25 patients (84.0%) localized in the nasopharynx (5 cases), lungs (5 cases), tonsils (3 cases), thyroid gland (3 cases), mediastinum (2 cases), gingival (1 case), esophagus (1 case), sigmoid (1 case), and sinonasal site (1 case). Among these, two cases showed multiple sites (nasopharynx and thyroid gland; Fig. 1). The primary tumors of 11 of 21 patients (52.4%) were confirmed by pathology, whereas those of 10 patients were not confirmed (Table 1). Four patients did not show a high FDG uptake on the PET/CT. (These fourteen patients should be false negatives, according to de Bree et al. 1 ) The sensitivity of FDG PET/CT in detecting the primary tumor was 44.0% (11 of 25), and the positive predictive value was 52.4% (11 of 21).

A 54-year-old man with left cervical lymph node metastasis from an unknown primary tumor (patient 8): biopsy of the left cervical lymph node. The pathology revealed poorly differentiated metastatic carcinoma of lymph nodes. PET/CT showed a hypermetabolic lesion (SUVmax=5.52) in left cervical lymph node (arrow) at level Vand VI; there was FDG uptake, suggesting a primary site in the upper mediastinum (SUVmax=5.52). Pathology showed non-small-cell poorly differentiated lung carcinoma (mediastinum type). PET/CT, positron emission tomography/computed tomography; FDG, fluorodeoxyglucose; SUVmax, maximum standardized uptake value.
The median follow-up duration of survival patients was 10.4 months (range: 1–30 months). The estimated 2-year overall survival rate of all patients was 50.0%. Univariate analyses did not reveal a significant difference in the overall survival between the group of 11 patients identified by pathology and the 14 patients not identified by pathology (overall survival was 57.1% and 49.1%, respectively; p=0.468; Fig. 2A).
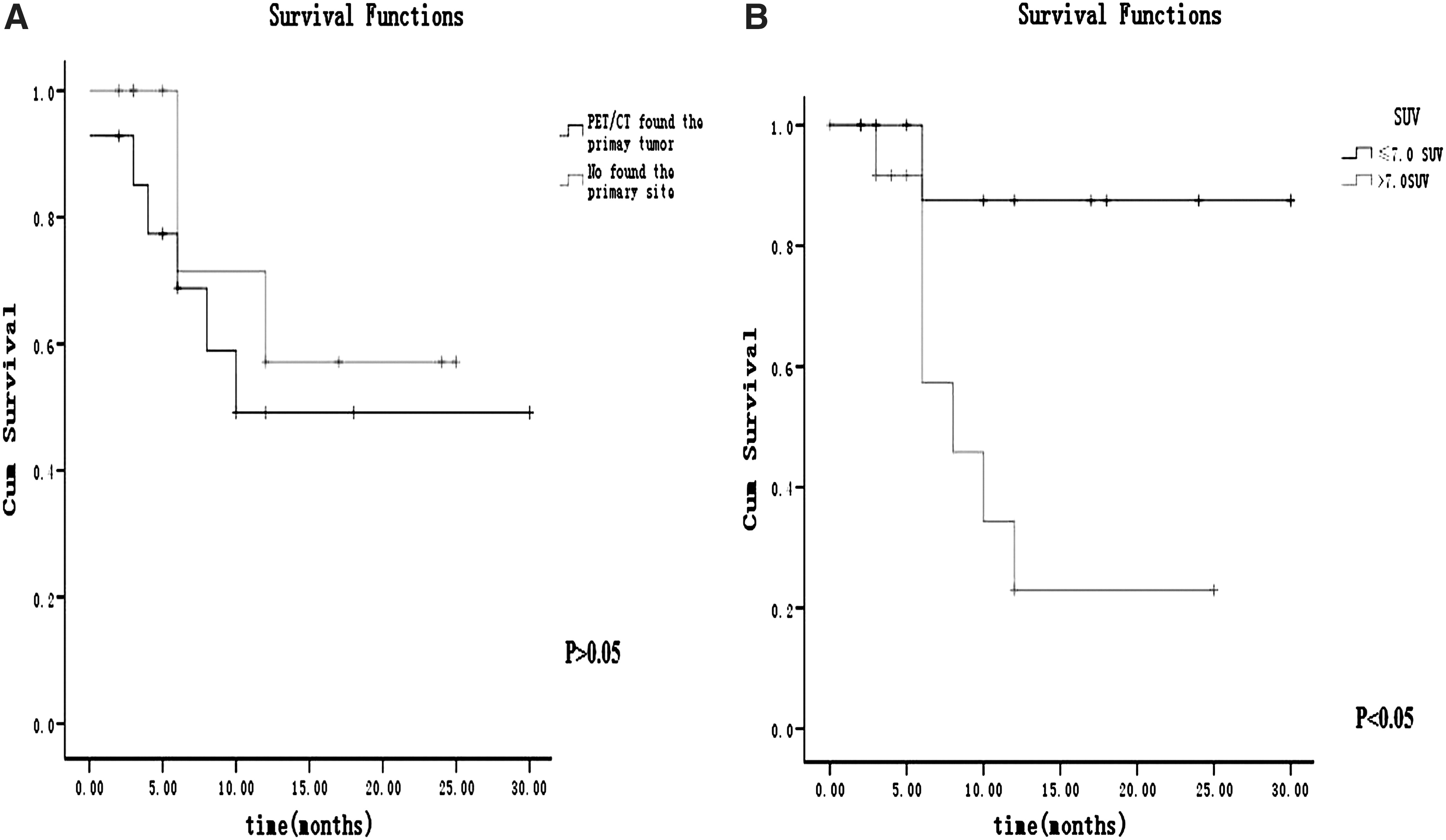
Univariate analyses did not reveal a significant difference in overall survival between the group of 11 patients identified by pathology and the 14 patients not identified by pathology
The median SUVmax was 7.6. In the log-rank test, patients with a low SUVmax (≤7.0) in cervical lymph nodes had a significantly higher survival rate at 2 years (87.5% vs. 21.2%; p=0.007; Fig. 2B) than patients with a high SUVmax (>7.0; Table 2).
Discussion
The diagnostic and therapeutic management of an unknown primary cancer in the head and neck is still controversial. The use of PET-CT has been demonstrated as improving the rate of identification of occult distant or regional metastatic disease, which allows for more accurate staging and appropriate treatment intervention. 2,8 However, the efficacy of PET/CT for detecting cervical metastasis of carcinoma from CUP remains to be determined. Most studies recommend PET/CT as an early diagnostic modality in the workup for carcinoma of unknown primary and neck metastases. 2,7,8 A few studies have found that FDG-PET/CT did not identify a primary tumor 4 or that PET/CT did not confer any additional advantage in the detection of primary sites in patients with CUP. 3 In a review and meta-analysis of data from 11 published studies on the diagnostic performance of FDG-PET/CT in UPT detection, which included 433 patients, Kwee and Kwee 11 found that the overall primary tumor detection rate, pooled sensitivity, and specificity of FDG-PET/CT were 37%, 84%, and 84%, respectively. Nassenstein et al. 12 and Wartski et al. 13 reported the detection of occult primary tumors by PET/CT in 11 out of 39 patients (28.2%) and 13 out of 38 patients (34.2%), respectively. However, in both of these studies, PET-CT was performed after a panendoscopy (with negative biopsy results) had already been performed. In contrast, Waltonen et al., 2 Roh et al., 14 and Pelosi et al. 15 used PET/CT before panendoscopy, detecting occult primary tumors in 23 of 52 patients (44.2%), 14 of 44 patients (31.8%), and 8 of 18 patients (44.4%), respectively. In our study, CT found only 4 primary tumors in the 25 patients with CUP, for a sensitivity rate of 16.0%. PET/CT suggested a primary tumor in 21 of 25 patients (84.0%), with a sensitivity rate of 73.3% (11 of 15). This suggests that a PET/CT scan has a clearly higher sensitivity rate than CT alone (73.3% vs. 16.0%; p<0.01) of primary tumors in the head and neck of patients with CUP. The variable diagnostic yields might be due to different patient inclusion criteria and the extent of the diagnostic workup in the different studies. 4 For example, the definition of a UPT differs among studies. 1 In our study, the inclusion criteria were biopsy-proven cervical metastasis of carcinoma before PET/CT. Patients were excluded from this study if they had a history of head and neck cancer, if a primary tumor site was evident on a physical examination, or if primary tumors of the neck (such as lymphoma or sarcoma) were diagnosed. Patients with primary tumors detected by imaging or visual panendoscopy were also excluded. Differences in pathology and differentiation among the studies may also impact the determination of a primary tumor by PET/CT. 17 Park et al. 3 suggested that the metastases of poorly differentiated carcinomas would have marked cell turnover and apoptosis, leading to early regression of the primary site. A higher proportion of poorly differentiated carcinomas could be one reason for a low detection rate of primary sites in cases with cervical lymph node metastases. In this study, among 11 true-positive FDG PET/CTs, the primary tumors of four metastatic squamous cell carcinomas (SCC) and seven poorly differentiated metastatic carcinomas (PDMS) were detected by PET/CT. The 14 primary tumors undetected by PET/CT included 1 metastatic adenoid cystic carcinoma, 6 PDMS, and 7 metastatic SCC. The limited number of patients in this series may have affected the results. Publication bias may also contribute to the differences in detection rate. 17
In this study, FDG PET/CT detected all known neck metastases, confirming the avidity of FDG for metastatic carcinomas. However, the primary tumor remained undetected in 56.0% (14 of 25) of patients with cervical lymph node metastases of a carcinoma. False-positive and -negative results may still occur in FDG PET/CT. FDG is not tumor specific, 16 and this nonspecific uptake is the main reason for false-positive results. In this study, the most commonly detected location of the primary tumor by FDG-PET/CT was the nasopharynx (36.4%), and the most common location of false-positive findings was the lungs (40.0%). In this series, approximately 12 false-positive FDG accumulations (SUVmax) occurred in the ribs and lungs. Kwee and Kwee found that the most commonly detected location of the primary tumor by FDG-PET/CT was the lungs (33%), and the most common locations of false-positive findings were the lungs and oropharynx. 11 Rusthoven et al., 8 Keller et al.,18 and Nakamoto et al. 19 reported that the tonsils were the most likely site of false-positive FDG accumulations, probably because of some asymmetric physiological uptake. Differentiating between physiological and pathological uptake in the head and neck area can be difficult. 1 According to de Bree et al., 1 all undetected primary tumors in these patients should be considered as a false negative. In our study, fourteen patients were false negative. Therefore, the sensitivity was only 44.0%. Primary tumors may be undetected because of their biological characteristics. 3 They may disappear after seeding metastases, because their angiogenic incompetence leads to marked apoptosis and cell turnover. 3,4,20 Well-differentiated SCC may also be wrongly interpreted as negatives, because they take up less FDG. 11,18,21 One patient (no. 15) had a lower FDG uptake in the left maxillary sinus and left nasal cavity (SUVmax=4.02). The first biopsy of the nasal cavity showed inverted papilloma (IP); the next biopsy of the maxillary and nasal cavity that was done 9 months later showed PDMS. This suggested that the sinonasal IP may have been a local malignant transformation. Another hypothesis is that the occult primary tumors in this case were too small to be visualized on CT images or to generate a sufficient uptake of FDG for detection on PET/CT. 2,4,11
Studies have shown that survival is significantly longer for those patients in whom the primary can be identified. 5 However, the benefit of FDG-PET/CT to patients with CUP is not yet clear. 4,22,23 In theory, one might expect that once the primary tumor was identified by FDG PET/CT imaging, the patient could be given a more targeted therapy and have a better outcome. 24 Fencl et al. 22 reported that a significantly shorter overall survival was found among patients with at least one positive lesion found by FDG-PET/CT as compared with patients with negative findings (p=0.00001). However, Kaya et al. 24 found that the median overall survival rates of FDG PET/CT positive and negative groups were 8 (95% confidence interval [CI]: 4–12) and 10 (95% CI: 1–11) months, respectively, although this difference was not statistically significant (log-rank p=0.573). In this study, four patients (nos. 3, 8, 15, and 23) underwent a change in therapeutic management because of the PET/CT findings and enjoyed good outcomes. However, we also found no significant difference in overall survival between the group of 11 patients identified by pathology and the 14 patients not identified by pathology (overall survival: 57.1% and 49.1%, respectively; p=0.468).
Although we observed no statistical significance in overall survival between PET/CT-positive and -negative patient groups, our results showed that patients with a low SUVmax (≤7.0) in cervical lymph nodes had a significantly higher survival rate (87.5% vs. 21.2%; p=0.007) at 2 years than patients with a high SUVmax (>7.0). Similar reports on head and neck cancer have been published. 25 –28 Torizuka et al. 25 also found that patients with a high tumor SUV (>7.0) had a poorer outcome than those with a low tumor SUV (≤7.0). Kubicek et al. reported that a primary tumor with a SUVmax>8.0 was predictive of worse overall survival (p<0.045), and the SUV of the lymph nodes was predictive of distant recurrence at 1 year, with a mean SUV value of 10.4 for patients with distant failure versus 7.0 without (p<0.05). 26 Xie et al. concluded from 35 studies that pretreatment SUV was valuable in predicting long-term survival in head and neck cancer. 27 Machtay et al. found that low SUVmax of the primary tumor was significantly associated with longer disease-free survival after radiotherapy of HNSCC in a series of 60 patients. 28 However, Döbert et al. found no significant association between SUV and prognosis. 29 Haerle et al. revealed that there was no significant correlation of SUVmax and histological tumor grading, tumor grading after adjustment for T-stage, and anatomical localization of the tumor. 30 They suggested that clinicians should, therefore, exercise caution in attributing any clinical importance to SUVmax obtained from a single PET/CT exam. 30 Thus, the prognostic value of SUV should be further studied.
Conclusions
Although our study was inconclusive due to the small sample size, our results suggest that FDG PET/CT may be an effective diagnostic workup in cervical metastasis of carcinoma from an UPT. In the present study, SUVmax of PET/CT in the cervical lymph node may serve as a prognostic factor of cervical metastasis of carcinoma from a UPT based on a limited number of patients. Further studies are needed to confirm these findings.
Footnotes
Acknowledgments
The authors acknowledge the financial support provided by the Research Project of Public Technology Application, Science, and Technology Department of the Zhejiang Province (No. 2010C33G2010109 and No. 2009C33026), and the Research Project of Medical Science and Technology, Health Department of the Zhejiang Province (No. 2009A079).
Disclosure Statement
The authors declare that they have no proprietary, professional or other personal interest in any product, service, and/or company that could be construed as influencing the position presented in this article.