
Abstract
Purpose:
To investigate the association of the CD44+/CD24− cancer stem cell (CSC) ratio with clinicopathologic features and its prognostic value in breast cancer.
Materials and Methods:
The CD44+/CD24− CSC ratio was determined in formalin-fixed, paraffin-embedded breast cancer tissues from 1350 breast cancer patients by double immunofluorescence staining. The Cox regression analysis was performed to evaluate whether the CD44+/CD24− CSC ratio is an independent prognostic factor. The Kaplan–Meier survival analysis was conducted to determine the association of the CD44+/CD24− CSC ratio with cancer-specific survival.
Results:
The mean average CSC ratio in clinical specimens was 8.06% (range from 1.02% to 37.54%). The CD44+/CD24− CSC ratio, together with histological grade, molecular type, and clinical stage, was independent prognostic factors of breast cancer. The CD44+/CD24− CSC ratio was significantly correlated with estrogen receptor (ER), progesterone receptor (PR), and Ki67, but not the Her-2 and P53 status. Furthermore, the CD44+/CD24− CSC ratio was significantly associated with 5-year breast cancer-specific survival in 1242 cases (88.97% vs. 75.76% vs.52.11% for ≤5%, 5%–10% and >10% CSC ratio cases, respectively, p=0.001). The linear regression analysis showed that the CSC ratio was borderlinely correlated with the N stage related (R=0.397 p=0.06), and significantly correlated with distant recurrence (R=0.487, p=0.01) in 1350 specimens. After the survival analysis, the 5-year distant recurrence rates were (57/435 [13.10%] vs. 159/594 [26.77%] vs. 114/213 [53.52%] for ≤5%, 5%–10%, and >10% CSC ratio cases, p=0.001).
Conclusion:
The CSC ratio was an independent prognostic factor for breast cancer as well as a potential predictive marker for chemotherapy in breast cancer.
Introduction
Breast carcinoma is the most common type of malignancy in women and is the second leading cause of cancer mortality in women. 1 More than 4.0 million new patients are diagnosed with breast cancer each year worldwide, and there are more than 1 million deaths according to the World Health Organization (WHO) each year. 2 Although a variety of therapeutic strategies have been available for fighting against breast cancers in clinic in recent years, 3 including surgical resection, chemotherapy, radiotherapy, and endocrine therapy, more than 40% of patients with breast cancer develop tumor recurrence after they have received comprehensive antitumor treatments. 4
Recent studies identified tumor-initiating cells, also referred to as cancer stem cells (CSCs) in solid tumors. These self-renewal CSCs are considered to be the main cause of therapeutic resistance and treatment failure in cancer. 5 Using a breast cancer xenograft model, Al-Hajj et al. reported that a small proportion of highly tumorigenic progenitor cells, namely, CD44+CD24−/low cells, maintained the ability to self-renew, differentiate, and metastasize. 6
A few studies have reported the clinical implications of CD44+CD24− CSCs in breast cancer. However, the clinical and prognostic implications of the CSC ratio in breast cancer are still controversial. Lee et al. demonstrated that CD44+CD24− cells were resistant to chemotherapies and associated with tumor progression in breast cancer, emphasizing the need for targeting of CSCs in the breast cancer therapeutics. 7 However, in another study, Abraham et al. reported that the higher percentage of CD44+CD24− cells did not correlate with clinical outcome. 8
In CSC, the transmembrane protein ABC is activated, and the multidrug resistance gene (MDR1) and ABCG could pump the DNA-binding dye Hoechst 33342 out of cells. Hence, the CSC-rich population within the tumor cells may be the culprit that is responsible for the multi-drug resistance of chemotherapy. 7,9 If the postoperative recurrence, metastasis, and response to chemotherapy could be predicted through the detection of breast CSCs, it would provide a strong theory for the management of breast cancer. Currently, there is no such study addressing the relationship between the CD44+CD24− cell ratio and clinicopathologic features or cancer-specific survival in Asian breast cancer patients. Therefore, in the present study, we examined 1350 mastectomy specimens obtained from patients with breast cancers to investigate the CSC ratio in relation to clinicopathological features, and known breast cancer markers and chemotherapy sensitivity in breast cancer, and determined the prognostic impact of the CSC ratio in these patients.
Materials and Methods
Patients and tissue specimens
We selected 1350 advanced breast cancers between Jan 2005 and Dec 2006 for double immunofluorescence staining and prognostic analysis. The mean age was 49.83±10.12 years (range from 29 to 84 years). The inclusion criteria were as follows: (1) curative operations were performed; (2) resected specimens were pathologically examined; (3) more than 15 lymph nodes were pathologically examined after operation; and (4) a complete medical record including the estrogen receptor (ER), progesterone receptor (PR), Her2, p53, and Ki67 status was available. The study protocol was approved by the Ethics Committee of the China Medical University and The Liaoning Tumor Hospital.
Double immunofluorescence staining
Briefly, surgically resected breast cancer tissues were fixed and cut at a thickness of 4 μm. The specimens were stained with control IgG, mouse antihuman CD44 (1:50 dilution, Santa Cruz Biotechnology, Santa Cruz, CA), rabbit antihuman CD24 (1:50 dilution, Santa Cruz Biotechnology), and polyclonal antibodies at 4°C for 12 hours. After being washed, the cells were incubated with biotinylated goat antimouse IgG secondary antibodies (1:1000 dilution) in PBS for 30 minutes at room temperature and the bound antibodies were detected with PE and FITC, followed by mounting with the DAPI medium (Vector Labs, Burlingame, CA). The expression of CD44 and CD24 was examined under a fluorescence microscope. The CSC ratio is the ratio of CD44+/CD24− cells (PE+/FITC−) to all the cells (DAPI+). We randomly selected five regions under the fluorescence microscopy and the CSC ratio was the mean of the five ratios in the selected areas.
Immunohistochemical analysis
Thin slices of tumor tissue of all cases received in our histopathology unit were fixed in a 4% formaldehyde solution (pH 7.0) for periods not exceeding 24 hours. The tissues were processed routinely for paraffin embedding, and 4-mm-thick sections were cut and placed on glass slides coated with 3-aminopropyl triethoxy silane (APES) for immunohistochemistry. Tissue samples were stained with hematoxylin and eosin to determine the histological type and grade of the tumor.
The pathological information was mainly based on the histopathological reports for initial screening. Then, another independent pathologist reexamined all the slides to confirm the pathological findings for all the cases.
Nuclear staining for ER (Santa Cruz Biotechnology) and PgR (Santa Cruz Biotechnology) was graded as 1+ if <10% of the cells were stained, 2+ when 10%–50% of the cells were stained, and 3+ if >50% of the cells were stained. Grades 2+ and 3+ were considered positive, whereas absence of staining and 1+ staining was considered negative. Nuclear staining for Ki67 (Santa Cruz Biotechnology) was considered positive if >20% of the cells were stained. Membrane staining for HER-2/neu (Santa Cruz Biotechnology) was graded similarly in terms of intensity of staining, and only grade 3+ (high intensity) was considered positive.
Statistical analysis
All data were analyzed with SPSS statistics software (Version 13.0, Chicago, IL). Numerous and continuous data were analyzed by the Student's t test and categorical data were analyzed by the Chi-square or Fisher exact test. Disease-specific survival was analyzed using the Kaplan–Meier method. The log-rank test was used to analyze survival differences. The multivariate analysis was performed using the Cox proportional hazards model selected in forward stepwise. A p-value of less than 0.05 was considered statistically significant.
Results
Detection of CD44+/CD24− cell ratio in breast cancer tissues by fluorescent immunohistochemical staining
To investigate the clinical implications of the CD44+/CD24− CSC ratio in Chinese breast cancer patients, we applied fluorescent immunohistochemical staining to quantify the proportion of CD44+/CD24− cells in each of the 1350 breast cancer clinical specimens. The mean average CSC ratio in clinical specimens was 8.06% (range from 1.02 to 37.54%) (Fig. 1).
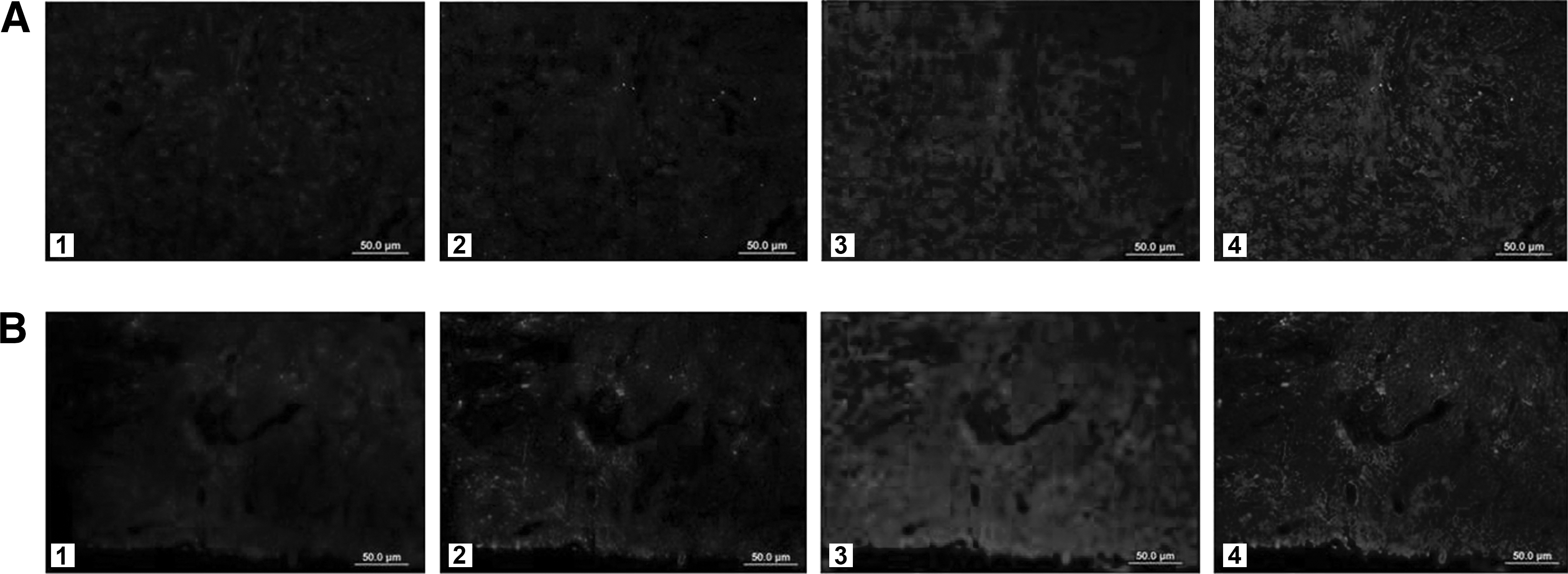
Various distributions of stem cells were observed.
The relationship between CSC ratio and clinicopathological features in breast cancer
We analyzed the association of the CSC ratio with patients' age, tumor size, node status, histological grade, and distant recurrence. Our data demonstrated that higher CD44+/CD24− ratio was significantly correlated with node positivity (p=0.001), higher histological grade (p=0.037), and distant recurrence (p=0.001), but not with age or tumor size (Table 1). A universal analysis revealed that the CSC ratio was associated significantly with the histological type, lymph node metastasis, and distant recurrence. The linear regression analysis showed that the CSC ratio was borderlinely correlated with the N stage related (R=0.397 p=0.06), and significantly correlated with distant recurrence (R=0.487, p=0.01).
The association of CSC ratio with breast cancer markers
The representative positive immunohistochemical staining of ER, PR, Ki67, and Her2 in the studying cases was shown in Figure 2. To determine the correlation of the CD44+/CD24− CSC ratio with clinical markers, the univariate analysis was performed and showed that the CD44+/CD24− CSC ratio was significantly higher in ER− and PR− cases than in ER+ or PR+ cases (p=0.01 and p=0.035, respectively) (Table 2). In addition, the CSC ratio was found to be significantly higher in Ki67− cases than in Ki67+ ones (p=0.001). However, the CSC ratio was not related to the P53 or Her2 status (p=0.450 and p=0.087, respectively). We next performed a logistic analysis on the above factors to exclude the effects of confounding factors. After the multivariate analysis, ER and Ki67 expression was found to be related to the CSC ratio (data was not show, p=0.001).

ER, PR, Ki67, and Her2-positive expression in breast cancers. ER, estrogen receptor; PR, progesterone receptor.
Higher CSC ratio in breast cancer is associated with poor survival
Of these 1350 cases, 1242 were successfully followed up at a rate of 92%. To evaluate the prognostic potential of the CD44+/CD24− cell ratio, we first performed the Cox regression analysis and revealed that the CSC ratio, histological grade, molecular types, and clinical stage were independent prognostic factors for breast cancer (Table 3). We next divided patients into 3 groups according to their CD44+/CD24− cell ratio (<5%, 5%–10%, and >10%, respectively), and accessed whether the percentage of CD44+/CD24− was associated with cancer-specific survival in these patients. As shown in Figure 3, the CSC ratio was significantly associated with the 5-year breast cancer-specific survival (88.97% vs. 75.76% vs. 52.11% for ≤5%, 5%–10% and >10%, p=0.001, log rank test). The 5-year distant recurrence rates were (57/435 [13.10%] vs. 159/594 [26.77%] vs. 114/213 [53.52%] for ≤5%, 5%–10% and >10% cases, p=0.001).
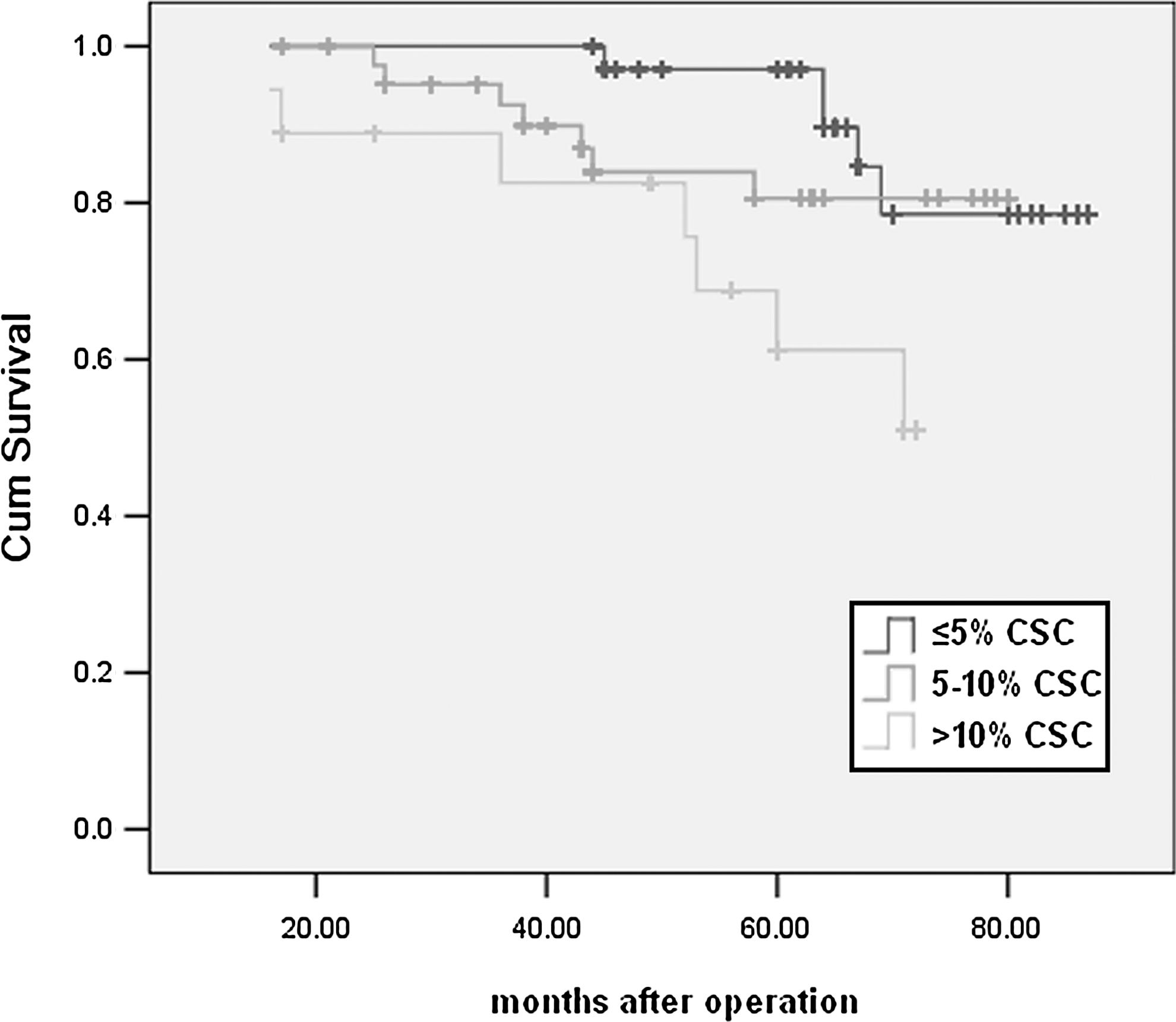
Five-year breast cancer-specific survival in 1242 cases. CSC, cancer stem cell.
OR, odds ratio; CI, confidence interval; CSC, cancer stem cell.
We further investigated the relationship between the CSC ratio and neoadjuvant chemotherapy sensitivity in 135 neoadjuvant chemotherapy breast cancers. The CSC ratio was significantly related to the neoadjuvant chemotherapeutic resistance in breast cancers (Table 4).
CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease.
Discussion
The CSC hypothesis posits that tumor growth is driven by a rare subpopulation of cells, designated CSC. Studies supporting this theory are based in large part on xenotransplantation experiments, wherein human cancer cells are grown in immunocompromised mice and only CSC, often constituting <1% of the malignancy, generate tumors. 10,11 According to the heterogeneity of tumor cells, different phenotypes of cells play a different role in the biological behavior of tumors. 12,13
In our previous work, CD44+/CD24− cell subsets were isolated from the tumor specimens collected using flow cytometry, and the CD44+/CD24− cell subsets showed a stronger tumor formation compared to the control group. CD44+/CD24− cells have previously been identified rich in breast CSCs. 14 In the study, the mean average content of CD44+/CD24− cell was 8.06% (range from 1.02 to 37.54%).
After analyzing the relationship between the CSC ratio and clinicopathological factors of breast cancer, it was found that the CSC ratio was significantly related to the histological type, lymph node metastasis, and distant recurrence, and it was also correlated with the N stage and distant recurrence. It showed that the CD44+/CD24− cell population could reflect the characteristics of breast cancer progress, which may be related to proliferation and invasion of CSCs. We also noticed that most of the CD44+/CD24− cells were distributed near the edge of the tumor, and high proportion of CD44+/CD24− cells were present in the vascular system.
After the multivariate analysis, ER and Ki67 expression was found to be related to the CSC ratio. Buess et al. reported that more than half of reported cases got <10% CSC ratio, and the CSC ratio was not verified as an independent prognositic factor though it was found that the cases with the CSC ratio had a tendency to get distant recurrence. 15 In the study, the survival analysis revealed that the CSC ratio was associated with 5-year breast cancer-specific survival, and was shown to be independent prognostic factors of breast cancer.
We further investigated the relationship between the CSC ratio and neoadjuvant chemotherapy sensitivity. The cases with the higher CSC ratio were found to be less sensitive to the chemotherapeutic response, while the ones with the lower CSC ratio intended to have a better treatment effect. CSCs are subsets of tumor cells defined through the capacity to initiate tumors and have been linked to therapeutic resistance. If the tumors contain greater numbers of CSCs that are also selected for greater resistance to therapy, the lethality of advanced cancers might be better explained. The cases with the high CSC ratio may contain greater numbers of CSCs compared to the ones with the low CSC ratio, which may result in the different chemotherapeutic sensitivity. It was reported that CD44/CD24, ALDH1A1, aldehyde dehydrogenase family 1 member A3 (ALDH1A3), and integrin alpha-6 (ITGA6) could be used to be markers of CSC. 16 It is a limitation of our study to use only one marker in this study. Future work will integrate the analysis of multiple markers.
In conclusion, CSC ratios vary in different individuals and are correlated with the lymph node metastasis and distant recurrence. It was shown to be independent prognostic factors of breast cancer as well as a potential predictor for chemotherapy sensitivity.
Footnotes
Acknowledgments
This study was funded by the China National Natural Science Foundation (No. 81102029 and 81172047).
Disclosure Statement
No financial conflicts declared.