
Abstract
Objective:
The purpose of this study was to explore the radionuclide distribution and metabolism of 131I and 125I dual-labeled gelatin microspheres (131I-125I-GMSs) implanted in rabbit liver.
Methods:
The simultaneous radiolabeling of 131I and 125I into GMSs was performed by a chloramine-T method to prepare biodegradable dual-labeled radionuclide microspheres. The microspheres were injected into rabbit liver. Radionuclide distribution and metabolism in vivo were examined using single photon emission computed tomography (SPECT) and by blood and urine radioactivity counting.
Results:
131I and 125I were labeled into the biodegradable GMSs in accordance with the mixture ratio of batch feeding. After 131I-125I-GMSs had been implanted in rabbit liver, small amounts of 131I and 125I were released into the blood along with the degradation of microspheres and excreted via the urine within 24 days. The radionuclides in the rabbit liver injection site could be detected by SPECT until day 48. The microspheres could be observed by histological methods on day 32. No signs of thyroid damage were observed throughout the entire experimental period.
Conclusion:
131I-125I-GMS can be retained long term in the injection site. Due to the advantages of combining two radionuclides, 131I-125I-GMS may be a safe and effective choice for cancer brachytherapy.
Introduction
In recent years, the application of radionuclide microspheres or radionuclide particles in the brachytherapy of malignant tumors by vascular intervention or by direct implantation has achieved remarkable success. 1 –3 A radionuclide microsphere is comprised of carriers and radionuclides. At present, the carrier includes glass, resin, and proteins. 2 For glass and resin carriers, mature products targeting various treatments have been developed. For instance, in 1999, 90Y glass microspheres (TheraSpheres) were approved by the U.S. Food and Drug Administration (FDA) for the treatment of primary and metastatic hepatic carcinoma; the resulting products are of utmost significance in the history of radionuclide brachytherapy, as this was the first time that a safe and effective drug has been provided for radionuclide brachytherapy. 4 Hundreds of papers have already reported its therapeutic effects and its remarkable achievements. 5 –8 Another brachytherapy drug approved by the FDA consists of 90Y resin microspheres (SIR-Spheres), and it labels the radionuclide 90Y to the resin microspheres. 9 Since the resin density is close to that of physiological saline, the resin microspheres can be easily prepared in a suspension with demonstrated superiority in both administration and distribution. However, the resin cannot be degraded; for instance, the glass in the treatment remains permanently in the body. The development of new radionuclide microspheres for safe and effective radiation brachytherapy is of great significance in improving the treatment of malignant tumors and improving disease prognosis.
The development of biodegradable radionuclide microspheres is a key area of research in radionuclide brachytherapy. A carrier made from biodegradable material can be degraded in vivo by enzymes so that it does not leave behind long-term foreign matter after treatment. For instance, Yu et al. labeled 188Re to polylactic acid (PLA) and made PLA-his microspheres with [188Re(CO)3(H2O)3]+. In vitro stability experiments confirmed that 188Re retains 80% of its original activity after 3 days. 10 Zielhuis et al. developed 166Ho-labeled PLA microspheres; in vitro and animal trials demonstrated a good level of safety for these radionuclide microspheres. 11 –14 Smits et al. conducted preclinical trials and preliminarily demonstrated that 166Ho-labeled PLA microspheres had good safety and a few side effects. 15
Taking into account the harmlessness of gelatin to the human body and its wide clinical application, we have labeled biodegradable GMSs with 131I and implanted these radionuclide microspheres into rabbit liver to observe their in vivo distribution and metabolism. The results showed that the radioactive iodine-labeled GMSs were safe to be directly implanted into rabbit liver, suggesting the possibility of radionuclide brachytherapy. 16 However, the half-life of 131I is short (8.04 days), and though the γ-ray emission detected by radionuclide single photon emission computed tomography (SPECT) imaging is conducive to observing the distribution of microspheres in vivo, its high energy damages normal tissue. Therefore, in this study, both 131I and 125I, which have the same chemical properties, were used to simultaneously label GMSs following the same method. These two types of radionuclides have differences in ray pattern and half-life; simultaneously labeling GMSs with them may produce anti-tumor properties of the resulting radionuclide microspheres with complementary and enhanced effects. The purpose of this study was to verify whether the two radionuclides 131I and 125I can simultaneously be used to label GMSs successfully and to determine whether the proportion of the final labels is the same as the initial proportion of the added radionuclides. More importantly, this study aimed at continuously observing the distribution of the de-iodination process in vivo and at identifying any damage to sensitive tissues and organs in animals over an extended period.
Materials and Methods
Materials
Type A gelatin was purchased from Sigma-Aldrich Co (St. Louis, MO); Na131I solution (37 GBq/mL) and Na125I solution (37 GBq/mL) were purchased from Chengdu Qualcomm Isotope Co., Ltd. of the China Nuclear Industrial Group (Chengdu, China); other reagents were of analytical-grade products.
Measurement of mixed radionuclides
Using two groups of radioimmunoassay tubes, group A contained different doses of Na131I solutions, while group B contained different doses of Na125I solutions. The true radioactivities were measured using a CRC-15R-type medical radiometer (Capintec, Inc., Ramsey, NJ) with the appropriate measuring channels. Then, the two groups exchanged measuring channels (i.e., 131I was measured using a 125I-channel and vice versa), and the radioactivities were also recorded. Groups A and B were then mixed together, and the amounts of 131I and 125I in the mixture were measured with the appropriate measuring channels using the CRC-15R-type medical radiometer, which determined the relationship between the measured values and the actual values, such that the measured values of the two types of radionuclide microspheres were reverted to their actual values.
Preparation of gelatin microspheres
Mechanical agitation was performed in a 120-mL round-bottom flask containing 80 mL of liquid paraffin and 1 mL of Span 80 in a 50°C water bath. Dropwise addition of 10 mL of 10 wt% gelatin solution was performed at a speed of 30 drops/min into liquid paraffin with mechanical stirring at 600 rpm. About 15 minutes later, the solutions were rapidly cooled to 4°C with continuous stirring. Cross-bonding was performed by adding 4 mL of 5% glutaraldehyde with stirring for 30 minutes. Dehydration was performed by adding 30 mL of acetone. Leaching was performed, followed by three consecutive washings with acetone. Air drying was performed at room temperature, followed by sieving the microspheres of size 10 to 30 microns with a stainless steel sieve.
Preparation of 131I and 125I dual-labeled gelatin microspheres
Swelling was conducted in a reaction tube for ∼10 minutes by adding 50 mg of gelatin microspheres (GMSs) into 200 μL of phosphate saline buffer (PBS, composed of 0.2 M sodium dihydrogen phosphate and 0.2 M disodium hydrogen phosphate, pH=7.0). The 74-MBq Na131I and 148-MBq Na125I solutions with a radioactivity ratio of 1:2 were added. Then, 200 μL of 20 g/L chloramine-T were added, followed by mixing for 3 minutes with a vortex at room temperature. The reaction ceased after adding 200 μL of 15 g/L sodium metabisulfite. Labeled microspheres were precipitated by centrifugation at 4400 rpm for 4 minutes at 4°C using a refrigerated centrifugal machine (Eppendorf 5702R; Eppendorf Co., Hamburg, Germany), followed by washing four times with physiological saline. Air drying, sterilization by cobalt-60 irradiation, and measurement of radioactivity were successively performed.
Animal experiments
A total of 14 healthy male New Zealand white rabbits with a body weight of 1.8–2.5 kg were provided by the West China Medical Education Center Laboratory Animal Center of the Sichuan University. The animals were raised with a granulated feed of 3–5 mm and were allowed free drinking water in stacked stainless steel wire cages with an air humidity of 50%–70% and a temperature of 20°C–29°C. The protocol was approved by the Animal Ethics Committee of the Sichuan University.
Implantation of 131I-125I-GMSs in rabbit liver
Each animal was anesthetized by an intramuscular injection of the anesthetic Sumianxin II (xylazine hydrochloride; Veterinary Institute of the Chinese Military Academy of Medicine, Changchun, China) with a dose of 0.1–0.2 mL/kg, according to the weight of each rabbit. Fixation of rabbits on the operating table and preoperative preparation of skin in the epigastric region were then performed. Each anesthetized animal underwent laparotomy by a median abdominal incision about 5 cm in length. The right middle lobe of the rabbit liver was raised by the left index finger inserted into the abdominal cavity, and the lobe of the liver was fixed together with the aid of the left thumb. Since there was no backflow for withdrawing, a slow injection with solutions composed of 85 mg of 131I-125I-GMS (131I is 44.528±6.327 MBq and 125I is 90.539±8.991 MBq) and 1 mL of 25 wt% glucose solutions was performed by a 4-gauge needle puncture into the liver adjacent to the gallbladder. For each injection, 2–3 points were selected with 0.3–0.5 mL per point, compressing 1 minute at the injection site after the needle withdrawal. The abdomen was closed if the injection site in the rabbit liver had no bleeding. At the end of the surgery, the intramuscular injection of 4 million units of gentamicin was then performed once immediately.
Radioactivity monitoring of rabbit serum and urine
One milliliter of blood was collected by ear vein, and 5 mL of blood were collected from 4 random rabbits once a day until postoperative day 12, every 2 days from days 12–51, and once on day 64. Centrifugation at 4400 rpm was performed. Then, 100 μL of the supernatants from the blood and urine samples were measured using a γ counter (FJ2021-based RIA counter; Xi'an 262 Instrument Factory, Xi'an, China).
Whole-body SPECT imaging
At 1, 4, 8, 16, 24, 32, 48, and 64 days after the operation, whole-body SPECT images were acquired using a Philips Skylight SPECT (Skylight SPECT Camera; Philips Co. Ltd., Amsterdam, Netherlands). The parameters included an energy peak of 306 KeV, a window width of 15%, 1× magnification, a 64×64 matrix, anteposition scanning, and an acquisition time of 2 minutes. At postoperative days 48 and 64, whole-body SPECT images were acquired using the same parameters just mentioned, except with an energy peak of 35 KeV.
During the first 32 days, each SPECT image acquisition used a region of interest (ROI) program that outlined the liver and measured the radioactivity by radioactive counting; then, the time-radioactivity (T-A) curves were plotted, followed by the calculation of the actual radionuclide half-life in vivo. The abscissa was time, and the vertical coordinates were calculated by (liver count minus background count at each time point)/(the liver count minus background count at the first day). The radioactivity of the thyroid gland was measured using the same ROI program during the first 32 days, from which the T-A curves were prepared.
Histological examination
At postoperative days 1, 6, 16, 32, 48, and 64, two animals were sacrificed for liver harvesting. The livers were fixed for 24–48 hours in 10% formalin. Paraffin embedding, slice sectioning, and hematoxylin-eosin staining staining were routinely performed for a histological examination.
Statistical analysis
The statistical software SPSS 13.0 was used for statistical analysis. Descriptive statistics were calculated; measurement data meeting the parametric test conditions were compared by t-testing, and count data were analyzed using chi-square tests.
Results
The standard curve of mixed-radionuclide measurement
When measuring the radioactivity of 125I using a 131I-channel versus the actual radioactivity of 125I, there was a linear relationship between the measured value and the true value of 125I (Fig. 1). In addition, when measuring the radioactivity of 131I using a 125I-channel versus the actual radioactivity of 131I, there was also a linear relationship between the measured value and the true value of 131I (Fig. 2). When the mixtures of 125I and 131I with different doses were tested with the 125I-channel and the 131I-channel of a CRC-15R-type medical radiometer, respectively, the results (Table 1) were impacted by the two linear relationships just described. If the radioactivity value of adding actual 131I is set to m, the radioactivity of adding actual 125I is set to n, the measured radioactivity value of the mixture using a 131I-channel is set to M, and the measured radioactivity value using a 125I-channel is set to N, then there exists the following relationship: M=m+1.7142n; N=n+0.5828m; m:n=1:2. If M and N values are measured, then m and n can be calculated by this formula.
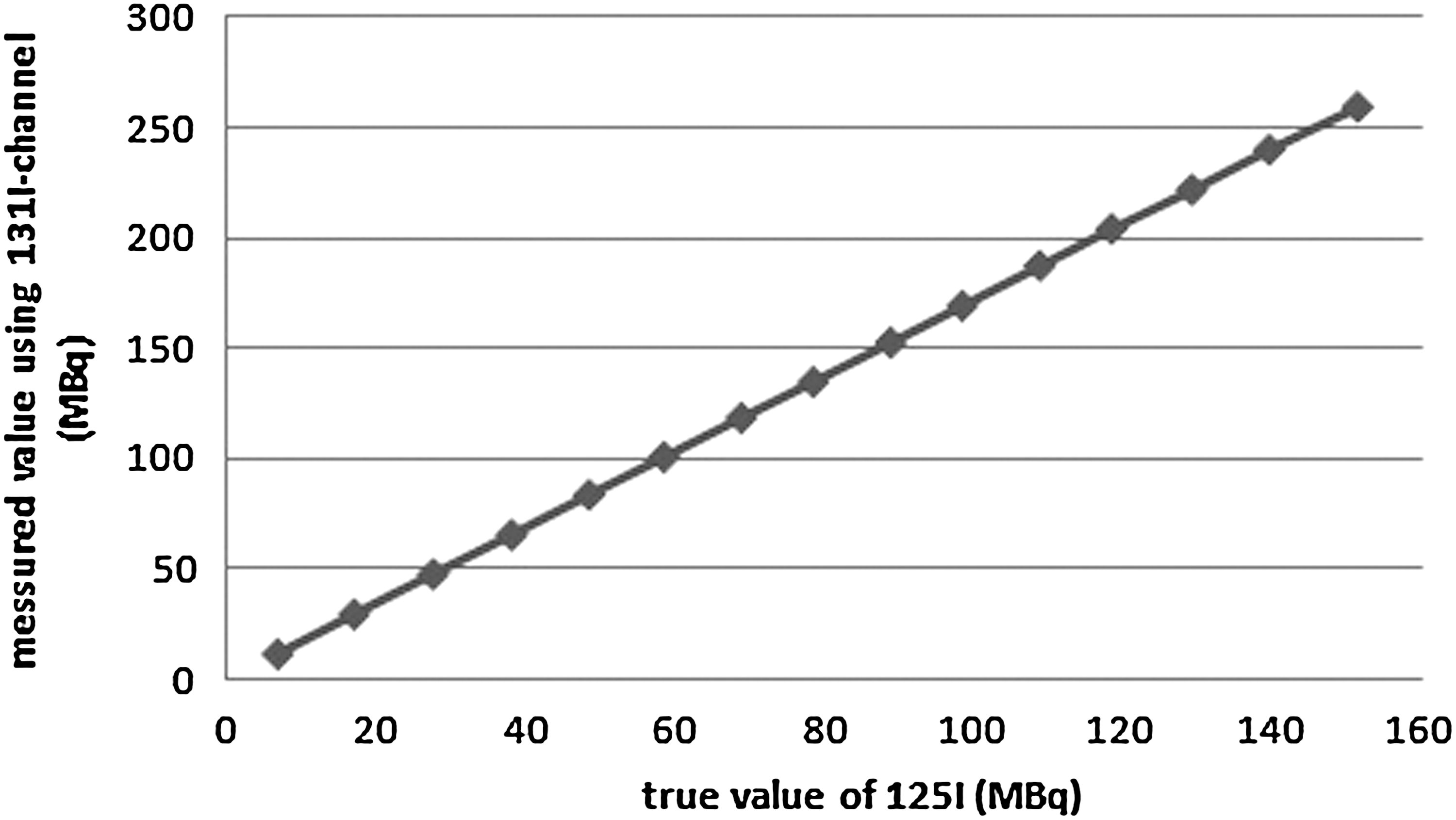
Measurement of 125I radioactivity using a 131I-channel (unit: MBq). The fitting formula is Y=1.7142×(R 2=1).

Measurement of 131I radioactivity using a 125I channel (MBq). The fitting formula is Y=0.5828×(R 2=0.9999).
The radioactivity value of adding actual 131I is set to m, and the radioactivity of adding actual 125I is set to n; the measured radioactivity value of the mixture using a 131I-channel is set to M, and the measured radioactivity value using a 125I-channel is set to N. Then, there exists the following relationship: M=m+1.7142n; N=n+0.5828m; m: n=1:2. If M and N values are measured, then m and n can be calculated by this formula.
Characterization of 131I-125I-GMSs
Microspheres of regular spherical shape were 10–30 microns in diameter (Fig. 3). Dual-labeled microspheres (30 mg, n=6) had an M value of 69.671±0.518 MBq and an N value of 40.663±0.629 MBq. According to the formula just cited, 30 mg of microspheres carried 131I 15.725±0.111 MBq and 125I 31.487±0.481 MBq. The calculated labeling rate was 33.94%. Microspheres were stored for 60 days in an appropriate place (the time period was more than 7 half-lives for 131I, resulting in m=0, and just one half-life for 125I). The measured M value was 30.287 MBq, and the measured N value was 17.637 MBq, that is, n=17.637 MBq. According to the formula, the calculated M value was 30.326 MBq, which was very close to the measured M value of 30.287 MBq. The computed radioactivity of 125I before 60 days was 35.274 MBq, close to 31.487±0.481 MBq, which was the calculated radioactivity of 125I before 60 days. This demonstrates that first, according to the formula, the actual radioactivity of each of the two radionuclides may be obtained from the measured values. Second, the initial actual ratio of 131I versus 125I was 1:2 in the reaction system, and, ultimately, the ratio carried by the GMSs was also 1:2.
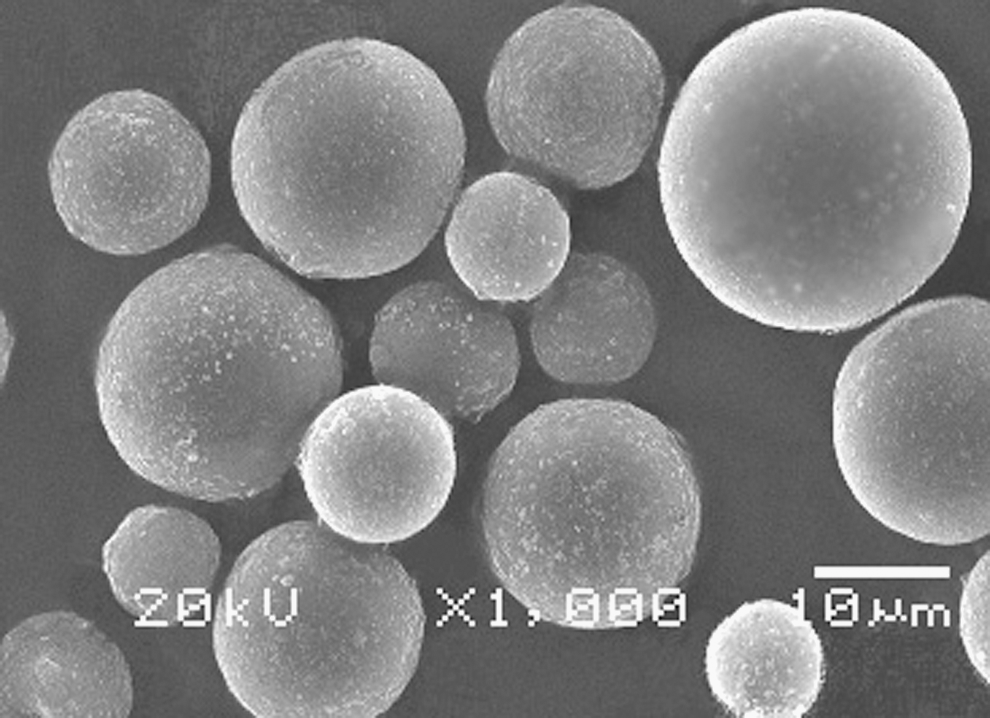
Electron micrographs of gelatin microspheres with 1000× magnification; the bar is 10 microns.
Postoperative condition of the animals
All animals survived the operation; there was some loss of appetite 1 day after the operation for some animals, but most animals returned to a normal diet by 2 days. Animal activities were not restricted. None of the animals died accidentally during the experimental period.
SPECT images
The postoperative use of a high-energy probe (306 KeV) 1–32 days after the operation detected the distribution of 131I in vivo. 131I was mainly distributed in the injection site, and a small amount of 131I accumulation in the thyroid was seen 4–16 days after the operation. There were no 131I images 48 days after the operation (6 half-lives of 131I) by the high-energy probe; rather, a low-energy probe (35 KeV) detected 125I distribution in the rabbit liver injection site (Fig. 4). Radionuclides were not detected by either probe 64 days after the operation.
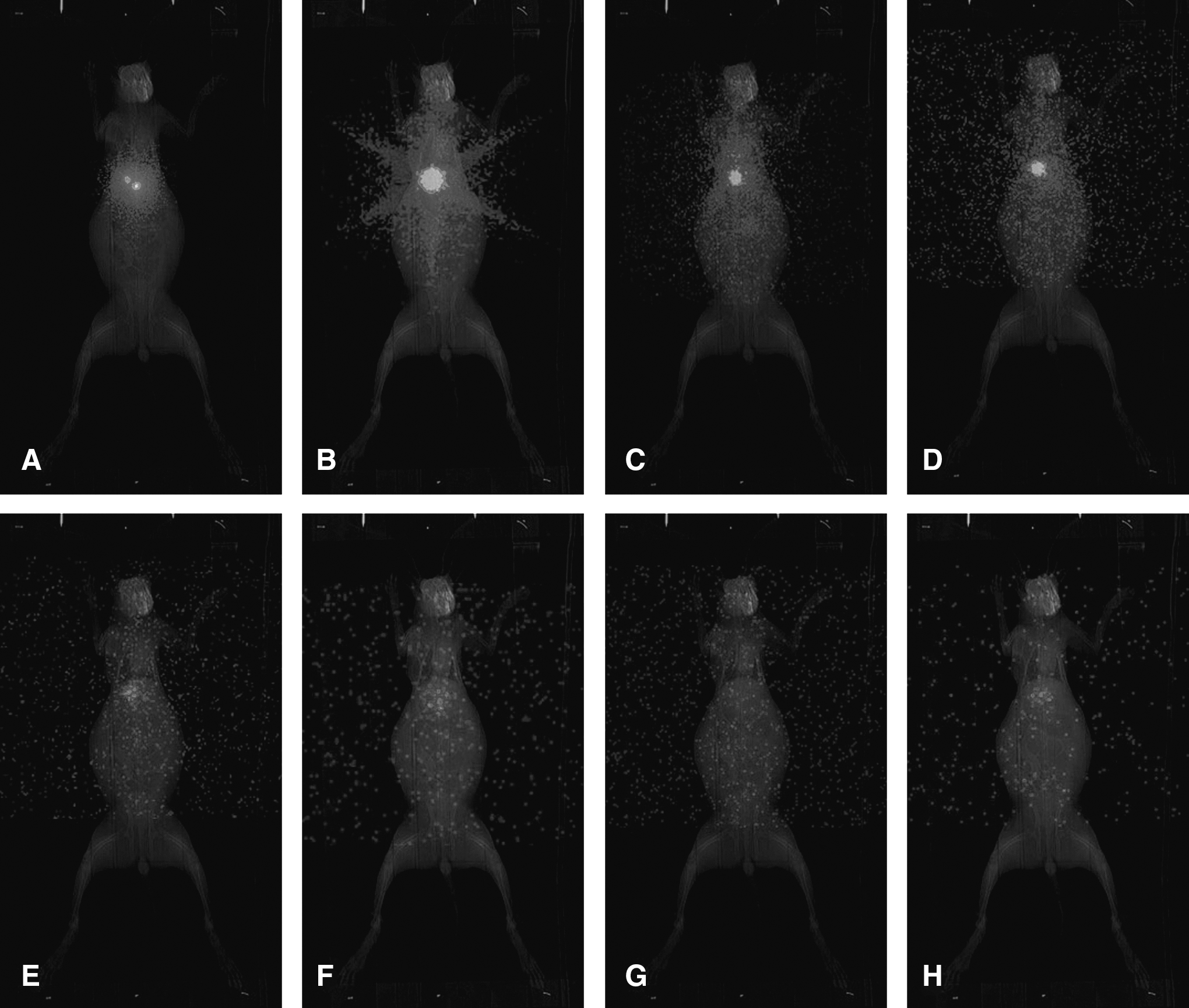
Postoperative SPECT imaging results.
The radionuclide accumulations at the liver injection site and in the thyroid region were radiocounted by ROIs. A T-A curve was plotted with time as the abscissa, with the count at the liver injection site at postoperative 1 day functioning as the base value, and the count versus base ratio at 4, 8, 16, 24, and 32 days functioning as the vertical ordinate; this plot is shown in Figure 5. The existence of radionuclides in the thyroid gland after the operation accounted for a very small proportion of the total implanted radionuclides; the radioactivity in the thyroid gland 4 days after the operation reached its highest level, though this was only 3.29%. In terms of stability, 4 days after the operation, more than 80% of the radionuclides were still bound to the microspheres; stability then decreased rapidly with subsequent degradation of the microspheres. Sixteen days after the operation, it remained at only 20% (Fig. 6).
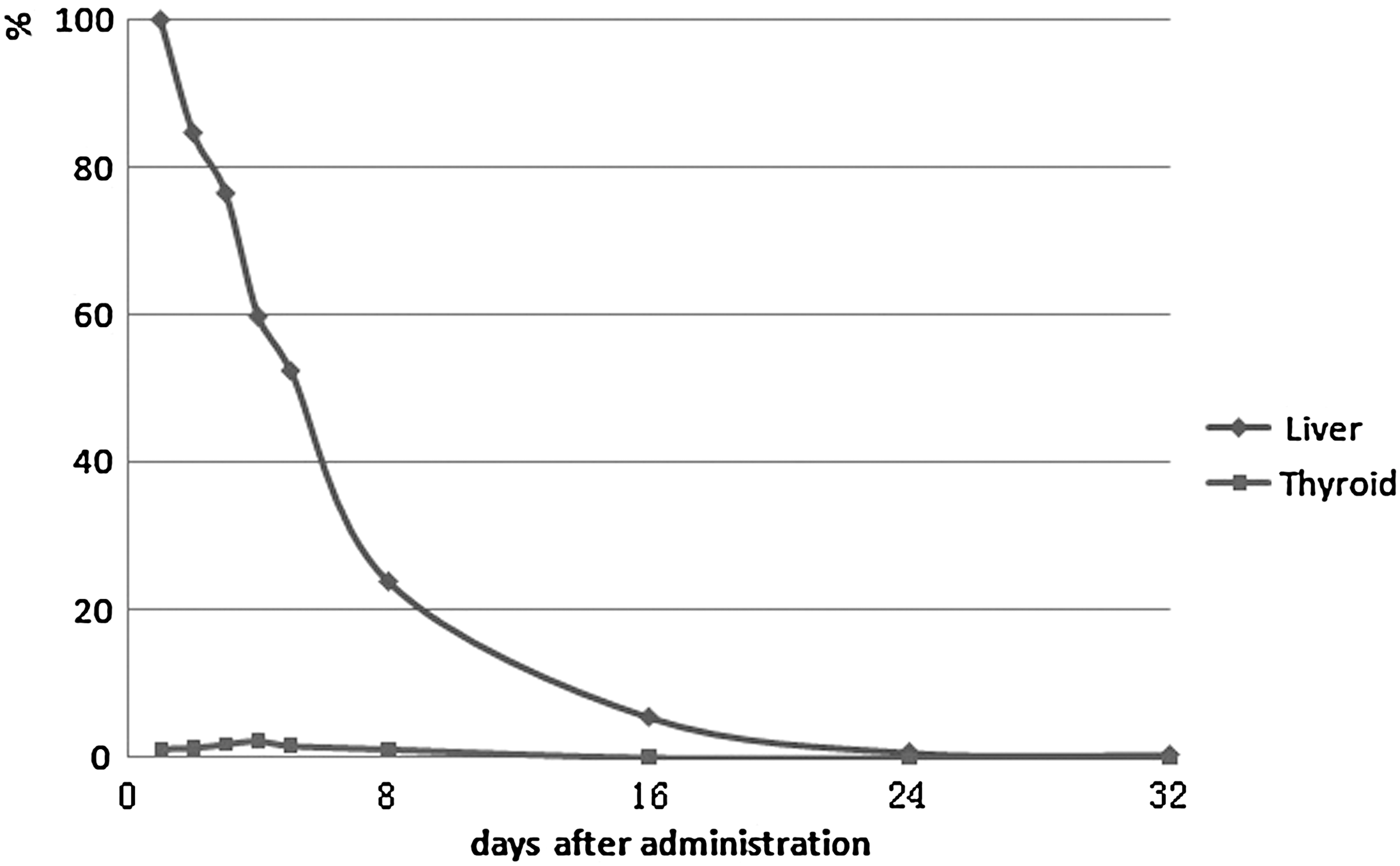
T-A curves for the liver and the thyroid 32 days after the operation. T-A, time-radioactivity.
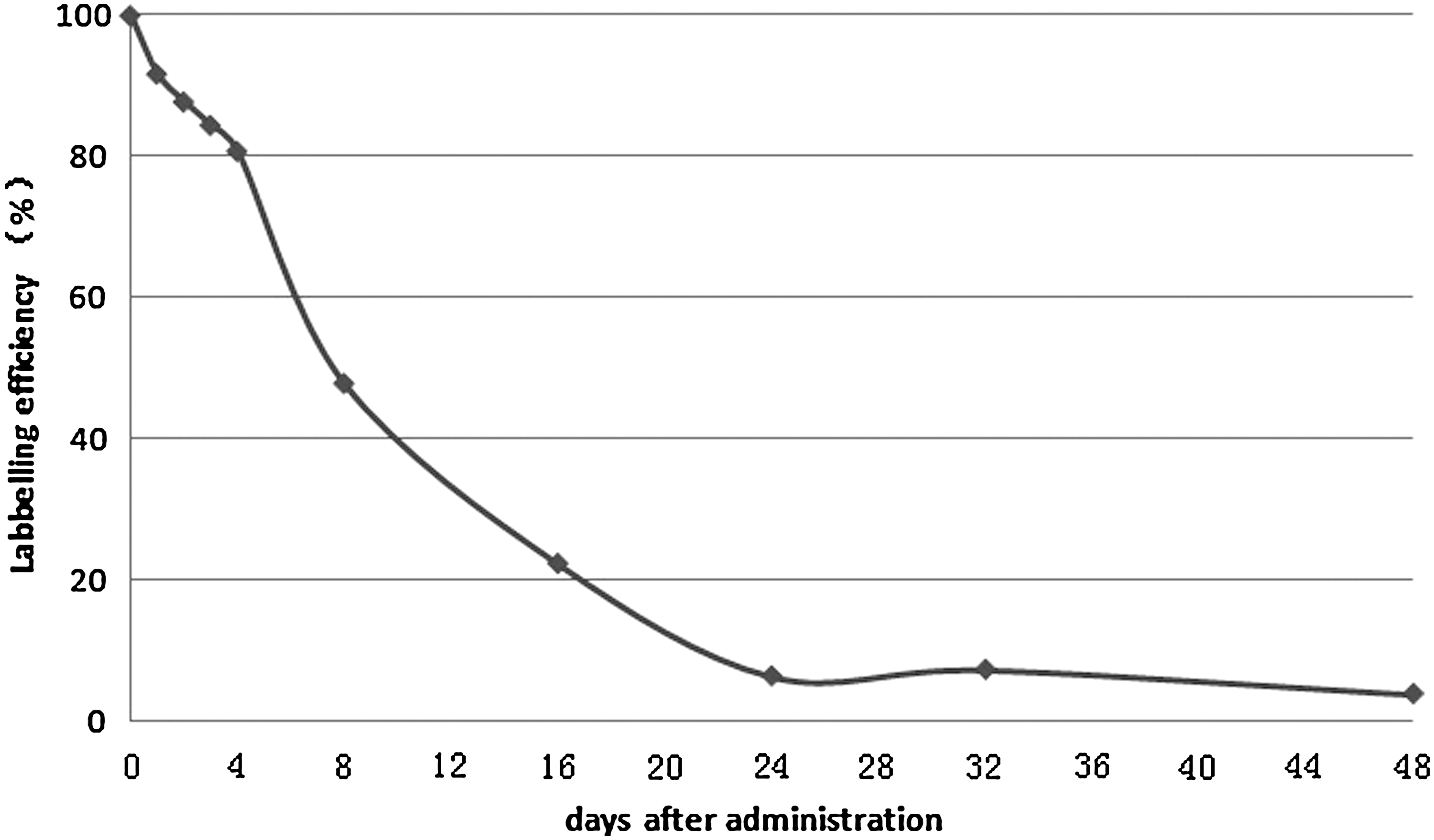
The stability of the experiment. There is still 80.77% of the original radioactivity 4 days after the operation, 22.37% after 16 days, and 3.92% after 48 days.
Radiation testing of serum
Serum radioactivity decreased rapidly during the first 3 days, and 3 days later, it slowly declined. By 24 days, it was indistinguishable from background radioactivity. Radioactivity in urine decreased rapidly during the first 7 days and then slowly declined. By 24 days, it was indistinguishable from background radioactivity (Fig. 7).

Changes in the radioactivity in serum and urine.
Liver and thyroid functions
Preoperative and postoperative indicators of liver function showed that both alanine aminotransferase and aspartate aminotransferase experienced a sequential process of increase, decrease, and stabilization. They increased 1 day after the operation and decreased to preoperative levels 4 days after the operation. The levels of free triiodothyronine and free thyroxin, both of which are indicators of thyroid function, were relatively stable during the experiment.
Histological results
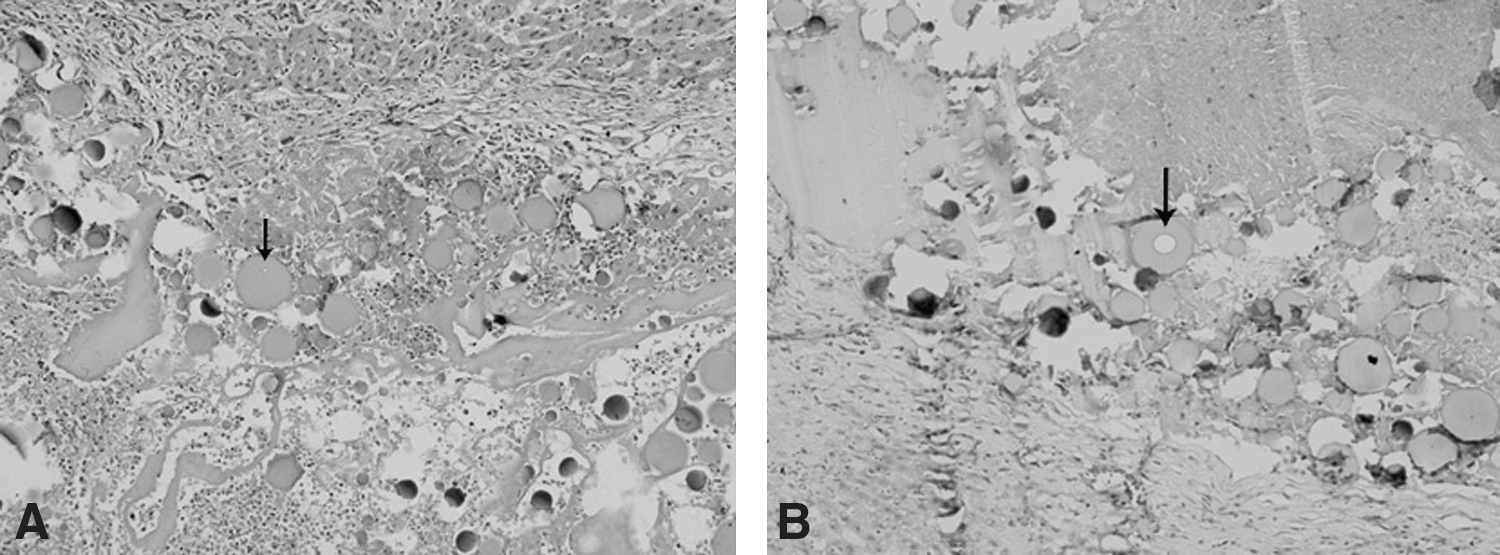
The microspheres remained for a long period at the liver injection site on histological examination. This result was consistent with the SPECT findings. In the slices taken during the first 6 days, it was observed that the microspheres began to degrade (arrow in Fig. 8A); this degradation was more clearly observed in the slices of the first 16 days, showing a greater proportion of degradation vacuoles (arrow in Fig. 8B). However, the degradation of microspheres was not uniform; in two slices, as some microspheres were degraded, some microspheres retained their complete morphology. At the first 32 days, residual microspheres were found in the tissues, but they showed irregular shapes, and their volume appeared small. At 48 days, there were no visible microspheres, but SPECT results suggested that the microspheres were not completely degraded at that time. The reason for the invisibility of the microspheres may have been that they were too small to be found.
Discussion
The underlying mechanism for the radiotherapy treatment of malignant tumors is mainly that a variety of radioactive rays act on the chromosomes, causing chemical changes in DNA and DNA strand breaks, which inhibit growth and reproduction in normal or tumor cells. However, the liver and the gallbladder in the depth of the abdominal cavity are more sensitive to low radiation doses and susceptible to radiation damage. Therefore, the application of conventional radiation therapy is quite limited. Brachytherapy for the treatment of tumors in these organs has a special advantage. Radionuclide microspheres and radionuclide seeds that are directly exposed to a tumor usually use ray sources of a small radio radius, which can greatly reduce the damage to adjacent normal tissue. In addition, tumor cells in the mitotic phase are more sensitive to radiation, while quiescent cells have a relatively weak sensitivity to radiation. The radioactive sources used in brachytherapy can continuously act over the course of tens of hours or even days during the whole cell cycle. As such, tumor cells can be continually exposed to the radiation of radionuclides carried by the microspheres throughout the cell cycle.
Implanted radionuclide microspheres, which are superior to external radiotherapy, can provide a more effective radiation dose and avoid excessive radiation to normal tissue; the tolerance of normal liver to radiation is ∼30 Gy. 17 –19 Thus, the use of radionuclide microspheres in the treatment of unresectable liver tumors has received increasing attention. 20,21 At present, 90Y glass microspheres and 90Y resin microspheres have been developed for the treatment of primary and metastatic hepatoma. 22 –25 Researchers are also developing a variety of radionuclide microspheres made of biodegradable materials. 26,27 These biodegradable microspheres may be degraded by the enzymes in tissues after the complete decay of radionuclides. The radionuclides carried by microspheres may be released (i.e., delabeling) with the degradation of the microspheres, and subject to blood flow, the delabeled radionuclides may reach various tissues and organs. Some radionuclides released in a small amount may cause irreversible damage to sensitive tissue, and so, whether these delabeled radionuclides may cause damage to healthy tissue should be given sufficient attention. Moreover, the tolerance of the body to the damage caused by the delabeled radionuclides should also be evaluated; this is even more important than determining the proportion of the delabeled radionuclides that are required to damage sensitive tissue.
The gelatin material used in this study is nontoxic to the body and has been widely used on a clinical basis with good histocompatibility; moreover, it serves as a mature technology for forming microspheres. Both 125I and 131I are effective radionuclides that are commonly used in anti-tumor treatment. 131I plays a very important role in the treatment of thyroid cancer. Brachytherapy of prostate cancer by the implantation of 125I radioactive seed sources achieves a good effect; indeed, it has become a standard therapy 28 with relatively few side effects. 29 Both of the nuclides have their own advantages. 125I has a relative long half-life (60.4 days) and mainly emits γ-ray of 35.5 KeV and X-ray of 27.4 KeV and 31.4 KeV; moreover, its energy is low. However, the effective radiation distance of its γ-rays in tissue is only 17 mm, so that it produces slight damage but is difficult to image. 131I has a short half-life (8.04 days) and yields γ-ray (1%, 0.364 MeV) and β-ray emissions (99%, 0.606 MeV); moreover, its energy is high enough for imaging through a γ camera easily, which is conducive for further studying the distribution of radionuclides and microspheres in vivo by SPECT. Although they have very different radioactive properties, they have the same chemical properties; that is, they can be simultaneously labeled to the target materials using the same method. Based on these features, we successfully simultaneously labeled GMSs with these two radionuclides using a very simple chloramine-T labeling method.
Since the radioactivity of the mixtures was measured using a CRC-15R-type medical radiometer in this study, 131I and 125I interfered with each other. Therefore, the individual actual radioactivities of 131I and 125I and the individual measured radioactivity of the mixture using the medical radiometer were investigated, and the measured values were then reverted to their actual values. Consequently, the initial 131I-125I feed ratio was 1:2, and the measured 131I-125I ratio in the finished product was also 1:2, which demonstrates that 131I and 125I exist in GMSs in the same proportion as the initial feeding. Therefore, this relationship should follow with any proportion of 131I- and 125I-labeled GMSs. Future studies might investigate the appropriate ratio for maximizing the synergy of the 131I and 125I. If the radionuclide microspheres are used for the treatment of solid tumors, then the tumors can be first destroyed by the short-term and effective high-energy rays of 131I and then destroyed by the sustained low-energy rays of 125I over a long-term period in order to reduce recurrence and metastasis.
With SPECT, a high-energy probe was used for the first 32 days to explore the distribution of 131I. During the first 32 days, the radionuclides were mainly concentrated in the rabbit liver injection site. Since the thyroid has strong iodine absorption, the concentration of radionuclides was observed in the thyroid region using SPECT images during days 4–16, in addition to the injection site in rabbits; no concentration of radionuclides was seen in the other parts. A quantitative comparison using ROIs demonstrated that the concentration of radionuclides in the thyroid region only accounted for 3.29% of the injected radionuclides, and the radionuclide retention time in the thyroid region was much shorter than that in the liver injection site. In the first 48 days (i.e., 6 half-lives of 131I), 131I was not detectable by the high-energy probe, indicating that the 131I carried by microspheres decayed to trace levels that could not be imaged. A low-energy probe was used to detect radionuclides displayed originally in the injection site. This image was formed after the exposure of 125I to radiation. Although the rays of 125I can only effectively penetrate 17 mm tissues, some ray particles passed through the abdominal wall to the sensitive probe after attenuation, because rabbits' abdominal walls are thin, and the distance of the implanted microspheres in the liver from the abdominal surface is <17 mm. As such, changes in these dynamic images also confirmed that the GMSs were simultaneously labeled with 131I and 125I.
Changes in the serum and urine radioactivities in rabbits showed that the radioactive counts per minute (CPMs) in blood were high during the first 3 days, low after 4 days, and similar to the background count after 24 days. The radioactive CPMs in urine were high during the first 6 days, appeared to have a turning point at 7 days, and were similar to the background count after 24 days. During the first 24 days, the radioactivity count of urine was higher than the count for the same volume of blood. We believe that the radioactive iodine was excreted mainly through the urinary system, leading to a higher radioactivity in urine than in blood. The high blood and urine radioactivity in the first few days may indicate that the initial delabeling of radioactive-labeled microspheres caused an explosive release of radionuclides. The reason for this explosive release may be that chemical bonds which combined radionuclides with microspheres broke, or it may be that the microspheres within the narrow needle collided and/or became crushed during the injection, releasing radionuclides. After 24 days, blood and urine radioactivities were similar to the background count, but at this time, the SPECT images of the radionuclides at the liver injection site were still observable; they accounted for 6.44% of the original radioactivity, but they accounted for 3.92% of the original radioactivity at 48 days.
The damage to the thyroid caused by the delabeled radioactive iodine can represent further damage to the body caused by the delabeled radioactive iodine. Unlike the delabeled 90Y and 32P radionuclides used in brachytherapy that quickly enter into the bone marrow and a variety of tissues, radioactive iodine rarely remains in other tissues except thyroid. If the delabeled radionuclides are not high enough in number to cause damage to the thyroid, they are relatively safe to other tissues and organs of the body. In this study, thyroid function and liver function tests demonstrated that the radionuclides injected into rabbit liver may lead to liver tissue damage in a limited range around the injection site, while the delabeled radionuclides do not cause thyroid damage. In addition, based on the highly selective iodine absorption of the thyroid, sodium iodide can be orally administrated to animals in advance in an experiment so that the nonradioactive-free iodine will first occupy the binding sites in the thyroid gland. As a result, the uptake of delabeled radioactive iodine in the thyroid will be greatly reduced, thereby protecting the thyroid tissue. The radioactive iodine not absorbed by the thyroid is excreted primarily through the urinary system, rather than remaining in other organs of the body for long periods of time.
In this study, the process of the degradation of microspheres in vivo and the biodegradability of microspheres were confirmed by a histological examination of biopsy specimens. However, their degradation rate was not uniform. The degradation of microspheres was observed for up to 6 days, while some of them did not degrade by 32 days or even longer. This phenomenon only explains why radioactivity can be detected in urine and blood during the experiment, although blood and urine radioactivity at 24 days is close to the background count. The reason for the inhomogeneous degradation of microspheres is not yet clear; a likely explanation is that the microspheres injected into rabbit liver display a spherical distribution. The peripheral microspheres that are first exposed to degrading enzymes are degraded first, while those in the center are exposed to degrading enzymes later, thus degrading later.
This experiment leaves many uncertainties and areas for improvement, including further studies on what proportion of 131I and 125I is conducive to achieving the best efficacy in various cancers while avoiding excessive side effects, how to further prevent radionuclides from delabeling in vivo, and how to improve the radionuclide labeling rate.
Footnotes
Disclosure Statement
The authors declare that they have no conflict of interest.