
Abstract
Background:
Fluorodeoxygluose (FDG) positron emission/computed tomography (PET/CT) is emerging as a useful tool for the diagnosis of peritoneal carcinomatosis (PC). In this study, we assessed whether dual-time point imaging can improve the accuracy of FDG PET/CT for the diagnosis of PC after colon rectal cancer (CRC).
Methods:
Thirty-nine patients with past history of CRC were evaluated. Whole-Body PET/CT scan was acquired 1 hour after tracer injection. If one or more focal areas of increased FDG uptake (standardized uptake value, SUV max>2.5) were found in the abdomen, 1 L of carbonated water was orally administered to patients and a delayed scan of the abdominal region was acquired at 2 hours. The SUV max and the mean Delta (Δ) SUV were calculated. The scintigraphic results were compared with the results of colonoscopy and histology and with the clinical follow-up.
Results:
Thirteen out of the 39 patients did not show any significant area of FDG uptake at the whole-body scan. The remaining 26 patients showed an overall number of 27 sites of focal increased uptake, showing a mean SUV max of 6.5+3.3. Late scan of the abdomen showed vanishing spots in 11 cases. Focal and increasing FDG uptake was found in 15 subjects (for an overall number of 16 sites) with SUV max of 15.6+4 and mean Δ SUV of +26.3%±7.5%. In these cases, final diagnosis was PC in 10 patients (according to cytology or histology) and dysplastic polyp in 5 cases. No significant difference in Δ SUV was found between patients with PC and those with polypoid formations.
Conclusions:
According to our results, dual-time point imaging after carbonated water may increase the accuracy of FDG PET/CT for the imaging of PC in patients affected by CRC.
Introduction
Peritoneal invasion is a severe complication of colon rectal cancer (CRC). The presence of carcinomatosis has significant implications for patients' treatment and outcome. In particular, it is considered the most negative prognostic factor in CRC, even more important than tumor local extension or lymph node metastases. 1
The diagnosis of peritoneal metastases still represents a serious challenge for physicians. Early diagnosis is of utmost importance since surgery may be mandatory to obtain an effective cytoreduction. 2 The accuracy of computed tomography (CT) in detection of peritoneal foci depends on several factors, such as size, morphology, and presence of ascites. 3 MRI has been applied for the diagnosis of carcinomatosis, but even this imaging modality presents some limitations. 4
18F-FDG positron emission tomography (PET) has been proved useful to diagnose peritoneal carcinomatosis (PC) in patients with stomach, ovarian, adrenal cancer, and mesothelioma, in particular, when peritoneal biopsy is unavailable or inappropriate. 5 PET imaging provides functional information by qualitative and semiquantitative (i.e., standardized uptake value, SUV) analysis. Nevertheless, since bowel is a physiological site of accumulation of 18F-FDG, the diagnosis of peritoneal involvement remains difficult.
The combined PET and CT gantries allow a precise anatomical functional correlation in a single session. Thanks to its precise anatomical functional correlation, the hybrid PET/CT increases the diagnostic accuracy of 18F-FDG PET in many clinical scenarios, including the detection and characterization of peritoneal pathological localizations. 6 However, the main limitation of 18F-FDG PET is the lack of specificity in discriminating tumor versus inflammation as the tracer accumulates not only within tumors, but also in inflammatory lesions. Since the pattern of 18F-FDG uptake significantly varies between tumor and inflammation, dual-time point imaging greatly helps differentiation. 7
Our hypothesis was that the 18F-FDG uptake due to peritoneal lesions is expected to be unchanged in morphology and increasing in SUV between early and delayed imaging after peristalsis stimulation, when compared with the physiological accumulation and transit in jejunum. The aim of this study was to assess the potential usefulness of dual-time point 18F-FDG imaging to detect PC in patients with CRC.
Materials and Methods
Patients
Thirty-nine patients (30 males, 9 females; mean age 63+8 years) were evaluated. The enrolment criteria were history of CRC, increased serum levels of tumor markers (i.e., CEA), diarrhea, or constipation. Ten out of 37 patients underwent neoadjuvant radiation therapy and chemotherapy before surgery. All patients had received several chemotherapic treatments before the PET/CT examination. The mean interval between the last chemotherapy and PET scan was 40+20 days.
Imaging
All patients were submitted to PET/CT scan 60 minutes after the intravenous administration of 3,7 KBq/kg of 18F-FDG. The PET/CT device was a Discovery ST (GE) with bismuth germanate crystal units arranged to form 24 rings combined with a 16-slice Light Speed Plus CT scanner. The average FWHM axial resolution of PET (full width at half maximum) is 5.2 mm and system sensitivity 9.3 cps/KBq for the 3D acquisition mode. Scanning was performed from the neck to the proximal tight in 3D modality, with an acquisition time of 3 minutes per table position. Images were reconstructed by using an ordered subset expectation maximization iterative algorithm (OSEM-SV, VUEPoint HD, GE, 2 iterations, 15 subsets). The CT was performed immediately before PET in the identical axial field of view using a standardized protocol consisting of automatic tube current modulation with auto mA, tube rotation time of 0.5 sec/rotation, slice thickness of 3.75 mm. The CT data were resized from 512×512 to a 256×256 matrix to match the PET data.
The data were transmitted to a nuclear medicine database, fused, and displayed using dedicated software (Advantage, GE).
If one or more focal areas of significant focal uptake (SUV max> 2.5) were found in abdomen, 1 L of carbonated water (free C02: 2350 mg/L) was administered to patients and a delayed scan of the abdominal region was acquired (3 minutes/bed) 120 minutes after 18F-FDG administration.
Data analysis
PET images were independently assessed both qualitatively and semiquantitatively by three well experienced nuclear physicians. Images were elaborated through the dedicated software PET-Volume Computed Assisted Reading (VCAR, GE). Every lesion was segmented with a threshold of 42% of the maximum SUV value within the bounding box of the lesion. SUV max and SUV mean change were calculated in the early and delayed images. The dual-time technique was considered contributory if it allowed the accurate characterization of a suspected focus as pathological or physiological uptake.
Scintigraphic results were matched with the results of cytology after abdominal washing or histology after colonoscopy or surgery.
Statistics
Data of SUV and Delta SUV are presented as average±standard deviation (SD). Sensitivity and specificity of delayed scan were calculated as the fraction of false positive and negative results on the basis of final diagnosis.
A two-tailed paired Student's test was used to analyze differences in Delta (Δ) SUV between patients with PC and those with polypoid formations; significance was established at the p<0.0 5 level.
Results
Table 1 summarizes the results.
Diagnosis was based on:
cytology after abdominal washing.
histology after colonoscopy.
histology after surgical resection.
F, female; M, male; SUV, standardized uptake value.
Thanks to the mainly semi-quantitative nature of data, no disagreement occurred among the reviewers.
Whole-body PET/CT at 60 minutes
Thirteen out of the 39 patients did not show any area of 18F-FDG uptake suspected for carcinomatosis. Among these subjects, ten presented physiological serpiginous uptake along the large and small intestine, without any focal abnormality, and were considered negative for peritoneal localizations. Twenty-six patients presented an overall number of 27 sites of focal increased uptake in abdomen, suspected for peritoneal implants, showing a mean SUV max of 6.5+3.3.
Late scan at 120 minutes
Fifteen patients (for an overall number of 16 sites) showed focal and increasing FDG uptake in the delayed images. In these patients, the SUV max value was 8.4+3.4 at 60 minutes and 15.6+4 at 120 minutes with a mean Δ SUV of +26.3%±7.5 at PET-VCAR software.
The final diagnosis was PC in 10 patients. In particular, three cases showed peritoneal seeding in the mesentery, one in the mesocolon, one in the paracolic gutter, four in the parietal peritoneum, one in the perihepathic and perisplenic space. The final diagnosis was based on the results of cytology after abdominal washing in eight cases. In one patient with a tracer uptake in mesocolon, histology after colonoscopy demonstrated tumoral cell implants in the perivisceral sierosa as shown in Figure 1. In one subject with a large hyperactive area next to the abdominal wall, the diagnosis of carcinomatosis was based on histology after surgical exeresis of the lesion.
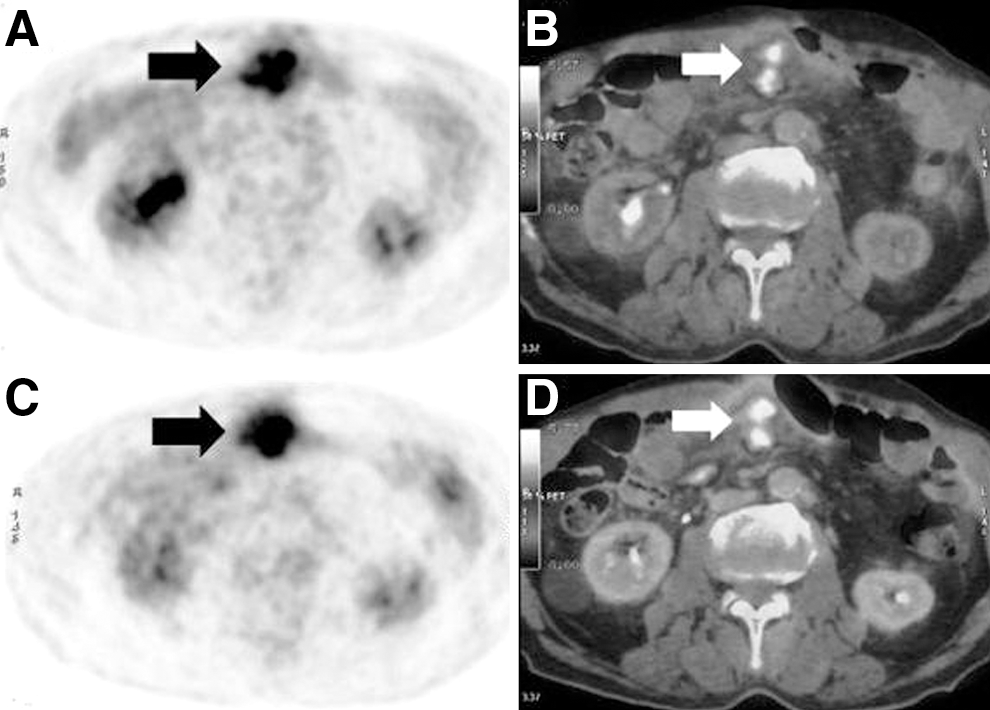
Male, 62 years, past history of CRC. Relapse was suspected on the basis of increased tumoral markers. Early 18FDG positron emission tomography (PET) scan
In the remaining 5 patients with positive delayed scan (mean Δ SUV: +30.1%±11.4%), the sites of 18FDG uptake were located in the colon wall in three cases and in the pelvis (sigma/rectum) in two subjects. All these patients underwent colonoscopic examination that showed the presence of polypoid formations. Subsequently, each patient underwent surgical resection of the polypoid lesions and histology revealed severe dysplasia in all cases, associated with intense lymphoid infiltration (Fig. 2). No significant difference in mean Δ SUV (p=0.17) was found between patients with PC and those with polypoid lesions.
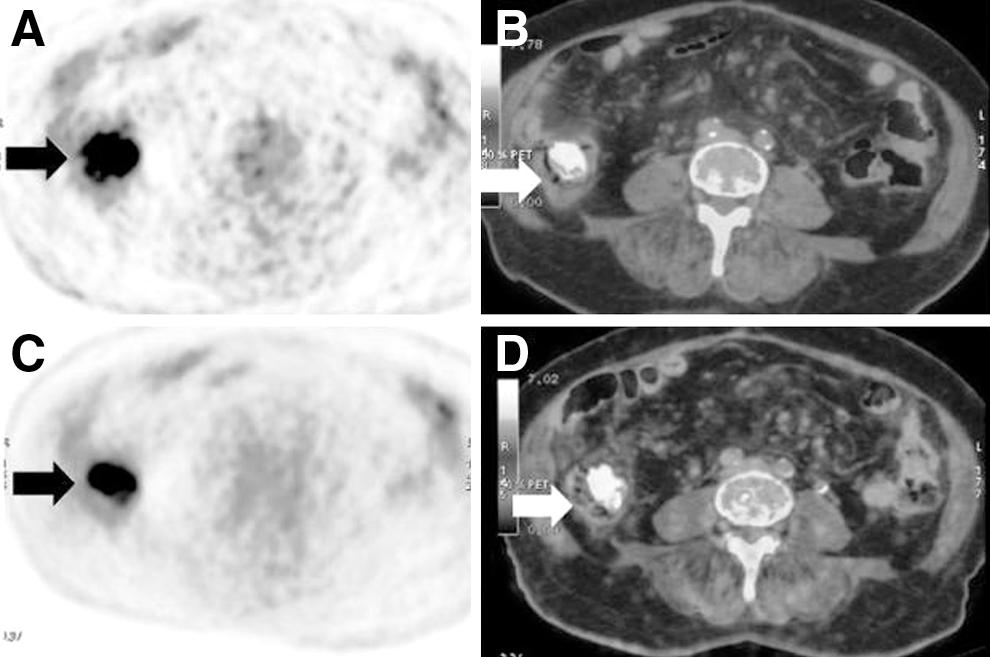
Female, 68 years, past history of CRC. Relapse was suspected on the basis of diarrhea and increased bioumoral markers. Early PET scan
Late scan was negative in the 11 patients with suspected abdominal focuses of FDG uptake at 60 minutes whole-body PET (Fig. 3). Patients with negative 60 minutes whole-body PET/CT scan or with vanishing spots at delayed imaging resulted free from peritoneal disease at follow up consisting of serial CT, clinical examination, and follow up of 24 months.

Female, 62 years, past history of CRC. Relapse was suspected on the basis of constipation and abdominal pain. The early PET scan
Sensitivity, specificity, the positive predictive value, the negative predictive value of delayed scan in detecting PC are reported in Table 2.
Results on 24 patiens submitted to cytology, histology or clinical follow up
PPV, positive predictive value; NPV, negative predictive value.
Discussion
Peritoneal localizations after colon cancer may be a serious challenge for physicians. While more advanced disease may be easily detected, small lesions are often missed by conventional imaging methods (CT or RM). The diagnosis is generally based on laparotomy and random peritoneal biopsy. However, this technique is not easily practicable during follow up because of its invasiveness. CT presents high sensitivity for peritoneal implants located in the paravertebral space or in the right paracolic gutter and for nodular lesions, but its accuracy dramatically drops for flat lesions (21%) or omental metastases. 3
In a group of 24 patients with suspected PC, Turlakow and colleagues 5 demonstrated that 18FDG PET was true positive in 13 cases and false positive in 1 case, with a sensitivity of 57%. CT performed independently of PET resulted positive in only 10 cases. Moreover, the authors identified two possible patterns of 18FDG uptake corresponding to nodular and diffuse carcinomatosis. Among our cohort, eight patients had nodular implants, one showed focal uptake in mesocolic sierosa, one had a flat lesion next to the abdominal wall that was missed by previously performed CT.
Suzuki et al. 8 reviewed CT and FDG PET findings and clinical features of 18 patients with PC and 17 subjects with neoplasia, but without PC. The pattern most frequently associated with carcinomatosis was intense abnormal focal uptake, with a SUV max threshold of 5.1 producing a diagnostic accuracy of 78%. Our data substantially agree with previously published reports, as patients with pathological findings at final diagnosis had a SUV max of 7.6+1.66 at 60 minutes whole-body PET/CT.
Hybrid devices combining PET and CT have been introduced with the aim of increasing the diagnostic accuracy of 18FDG PET in many clinical scenarios. FDG PET/CT proved more sensitive in detection of carcinomatosis when compared to PET and CT alone. 9 Moreover, the superimposition of anatomical and functional corresponding images can be useful to discriminate pathological versus physiological uptake.
Dual-time point imaging has been introduced to discriminate malignant from benign processes, as it has been demonstrated that tumoral lesions show an increasing SUV at late scan when compared with benign lesions, which exhibit a stable or decreasing tracer uptake over time. 7 Dobert et al. assessed the value of dual-time point technique in group of 56 patients with intense abdominal FDG uptake. In their study, the early acquisition started at 64.8 minutes, while the second at 211 minutes after FDG injection. 10 The scintigraphic results were matched with CT or MRI and with a follow up of 12 months. The authors found that malignancy could be excluded in all lesions with a SUV inferior to 2.5 and in all those focal areas changing their configuration between early and late scan. Furthermore, malignant focal lesions resulted to exhibit an uptake increase of 30% or higher. However, the percent increase of SUV max was evaluated, as observers' attention was focused on the maximally active portion of the suspected lesion. In our series, we used a dedicated software package (PET VCAR, GE) that allowed to delineate irregular ROIs based on a fixed percentage of the maximal pixel of the tumor (i.e., 42%), thus reducing the inter-operator variability in drawing ROIs. 11 We chose mean Δ SUV to characterize the suspected focal areas at early and late scan, since this parameter proved an accurate indicator of the global metabolic reponse. 12,13
The time interval between early and late scan in our series was shorter compared with the Dobert's group, but to our experience a distance of 60 minutes is sufficient to obtain changes in the physiologic intestinal activity if an adequate protocol is used. In fact, it has been demonstrated that at least 900 mL of water orally administered may provide bowel distension before radiological examination. 14 Moreover, carbonated water has been proved useful to stimulate peristalsis and gallbladder emptying. 15 Our hypothesis was that the combination of bowel distension provided by oral hydration and peristalsis stimulation due to carbon gas might allow discriminating physiological versus pathological uptake in the abdominal region. Our results confirmed that all focal areas at 60 minutes PET/CT showing unmodified morphology and increasing uptake at late scan after carbonated water always resulted as pathological findings at final diagnosis. On the contrary, all patients with vanishing hot spots at 120 minutes imaging were free from diseases according to all clinical parameters. Looking at our results, this protocol is quite easy to perform and not significantly time-consuming, with an extremely high predictive negative value (i.e., 100%) in excluding peritoneal implants. Therefore, when whole-body PET/CT is doubtful for abdominal localizations, dual-time imaging might be useful in preventing to submit patients to further examinations, such as explorative laparoscopy or colonoscopy.
In our series, we selected only patients with clinical or laboratoristic signs highly suspicious for relapse; therefore, the probability of peritoneal spread was quite high as compared to that of patients in follow up after CRC.
In 5 patients with persistent and focal uptake at delayed scan, the final diagnosis was dysplastic polyp associated with intense lymphoid infiltration. 16,17 It is worth noting that no significant difference in mean Δ SUV was found between patients with carcinomatosis and those with dysplastic polyps. Although such cases might be considered false positive results regarding the diagnosis of carcinomatosis (i.e., specificity: 68.7%), dual-time imaging resulted anyhow contributory for the early characterization and surgical exeresis of dysplastic lesions, thus, preventing clinical symptoms or potential neoplastic progression. 18,19
Conclusion
Dual-time point imaging can be a useful tool to increase the accuracy of 18FDG PET/CT for the diagnosis of PC after CRC. False positive results may occur due to tracer uptake in dysplastic lesions.
Footnotes
Disclosure Statement
No competing financial interests exist.