
Abstract
Aim:
To verify the potential role and feasibility of carbidopa premedication in pediatric patients undergoing 18F-DOPA (Fluorine-18 fluorodihydroxyphenylalanine) PET scanning.
Materials and Methods:
For this limited study, 5 patients (M:F=3:2; mean age 4.8 years) with a positive history for neuroblastoma who had been referred to our institution for instrumental monitoring during clinical follow-up were enrolled. In all cases, two consecutive 18F-DOPA PET scans, the first without carbidopa and the second with carbidopa premedication, were scheduled: patients received 4 MBq/kg of radiotracer and a dose of 2 mg/kg of carbidopa. Dedicated VOIs were drawn on the basal ganglia, pancreas, liver, and renal cortex. These regions were semiquantitatively analyzed at both the first and at the second 18F-DOPA scan, and mean SUVmax values were compared using the t-test.
Results:
On a visual basis, a clear reduction in the abdominal accumulation of 18F-DOPA was observed in all cases after carbidopa premedication. This reduction related both to the biliary structures and the excretory system, and was accompanied by a generalized increase in soft tissue uptake. The semiquantitative analysis documented an absolute increase in SUVmax after carbidopa premedication in the basal ganglia (3.4±1.3 vs. 2.1±0.8) and liver parenchyma (2.2±0.5 vs. 1.5±0.5), whereas SUVmax decreased in the renal cortex (1.7±0.8 vs. 3.7±1.0) and the pancreas (2.3±0.6 vs. 3.5±0.5). The changes in SUVmax were statistically significant for the pancreas and liver parenchyma (p=0.022 and 0.045, respectively), but not for the basal ganglia and renal cortex (p=0.143 and 0.15, respectively).
Conclusions:
Carbidopa premedication in the pediatric population appears feasible and seems to influence 18F-DOPA distribution in the liver and pancreas in a manner similar to that reported in adults. Larger series are however needed to properly define the clinical role of carbidopa premedication in children.
Introduction
Fluorine-18 fluorodihydroxyphenylalanine ( 18 F-DOPA) is a polyvalent tracer successfully utilized in the functional imaging of several pathologies related to dopaminergic metabolism in the striatal region, such as neurodegenerative and movement disorders, and in the detection of primary and metastatic neuroendocrine tumors (NETs). 1 –8 18 F-DOPA is the radiolabeled form of the amino acid dihydroxyphenylalanine, a direct precursor of the endogen neurotransmitter dopamine and in general of the metabolism of catecholamines. 4 Accordingly, the tracer is actively taken up via the large amino acid transporter and subsequently decarboxylated within the cell into dopamine, by the action of aromatic acid decarboxylase (AADC). 8 Both these mechanisms are reported to be increased in NETs, 9,10 opening the way for functional imaging of these tumors with 18 F-DOPA PET. 11
PET imaging with 18 F-DOPA has been demonstrated to be of high diagnostic accuracy in many NETs, with results superior to those obtained with other imaging modalities, such as 123I-MIBG scan or conventional computed tomography (CT)/magnetic resonance imaging. 12 These findings are related to the elevated 18 F-DOPA avidity of neuroendocrine cells and secondarily to the high tumor-to-background ratio when excluding aspecific accumulation in nontarget tissues, such as pancreatic parenchyma, biliary ducts, and the urinary drainage system. This aspecific activity is irrelevant in most of cases, but tends to be a drawback when imaging abdominal structures and, more precisely, retroperitoneal involvement (i.e., paraganglioma, pheochromocytoma, and neuroblastoma). In the adult population, the solution to this issue is carbidopa premedication: data derived from several studies have demonstrated that this significantly improves 18 F-DOPA PET imaging, with an optimized tracer distribution in both target and nontarget tissues. 13 –15 However, no similar investigations have been conducted in a pediatric population, with the main reason appearing to be that the only indication for 18 F-DOPA in children is congenital hyperinsulinism, and that premedication with carbidopa for this specific indication is not judged effective. 16
In our department, the role of 18 F-DOPA in pediatric patients affected by neuroblastoma is currently under investigation. 17,18 The aim of the present study was to explore the potential role of carbidopa premedication in this oncologic setting and to provide some initial information on its feasibility in children.
Materials and Methods
For this limited study, 5 patients (M:F=3:2; mean age 4.8 years) with a positive history for neuroblastoma who were referred to our institution for instrumental investigation during clinical monitoring were enrolled (Table 1). In all cases, two consecutive 18 F-DOPA PET scans, the first without carbidopa and the second with carbidopa premedication, were scheduled. The scans were performed as close as possible to each other, with a maximum interval of 3 months, according to the checkup timing established by the referring pediatric oncohematologist. No clinically or instrumentally detectable modifications in patients' status were reported between the scans, and since the primary target of the study was the feasibility of carbidopa premedication in children, tumor uptake in the analysis was not considered.
F-DOPA, Fluorine-18 fluorodihydroxyphenylalanine; CT, computed tomography; NB, neuroblastoma.
For the study, 18 F-DOPA produced as previously described 19 (IASOdopa®) at a dose of 4 MBq/kg (0.1 mCi/kg), with a range of administered activity of 50–100 MBq (1.4–2.7 mCi), was utilized.
18 F-DOPA PET was carried out 1 hour after tracer injection on an integrated PET-CT system with 3D modality (Discovery STE; GE Medical Systems). Whole-body image acquisition included 4 to 10 bed positions (4 minutes/bed position), with four to seven fields of view of 15 cm, each of 3.5 minutes, and nine slices of overlap. A low-dose CT scan (thickness 3.75 mm, 80 kV, 50–60 mA, 0.6 seconds per rotation) was used for attenuation correction and for anatomical localization. Images were subsequently reconstructed using an iterative reconstruction algorithm (OSEM).
At the second PET/CT scan, patients received carbidopa premedication 1 hour before the tracer injection. Pharmaceutical Lodosyn® (Bristol Myers) was given at a dose of 2 mg/kg, up to a maximum of 50 mg of carbidopa (Table 1).
Dedicated volumes of interest were drawn on the principal tissues expected to show variation in tracer uptake under carbidopa premedication, namely the basal ganglia, pancreas, liver, and renal cortex. These regions were semiquantitatively analyzed in at both the first and at the second 18 F-DOPA scan, and mean SUVmax values were compared using the t-test with p<0.05 considered statistically significant.
Results
The pharmaceutical carbidopa was administered as small caps, which children could easily swallow, the maximal dosage being of two caps of 25 mg each in an older patient (Table 1). Administration 1 hour before 18 F-DOPA injection was judged sufficient to determine the effects on 18 F-DOPA distribution. On a visual basis, in all cases, a clear reduction in aspecific tracer uptake was observed in the abdomen. This was especially evident in the pancreatic parenchyma and biliary structures (Fig. 1), and there was also a notable decrease in 18 F-DOPA accumulation in the renal cortex and urinary excretory system (Fig. 2).
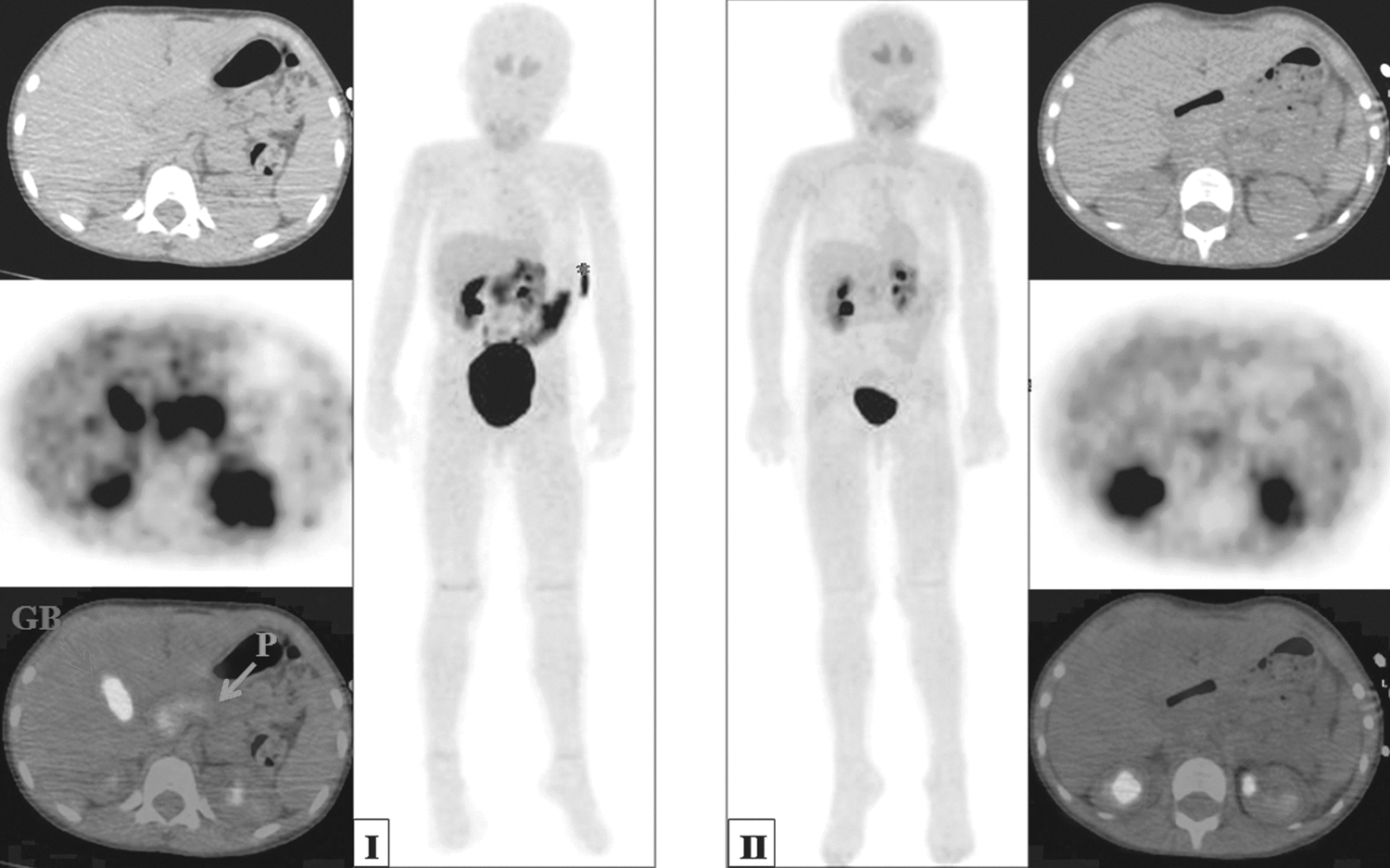
Multipanel image showing two consecutive 18F-DOPA PET/CT scans of the same patient (patient 2) before and after carbidopa premedication (left and right panels, respectively). The central panels represent corresponding maximal intensity projection images before
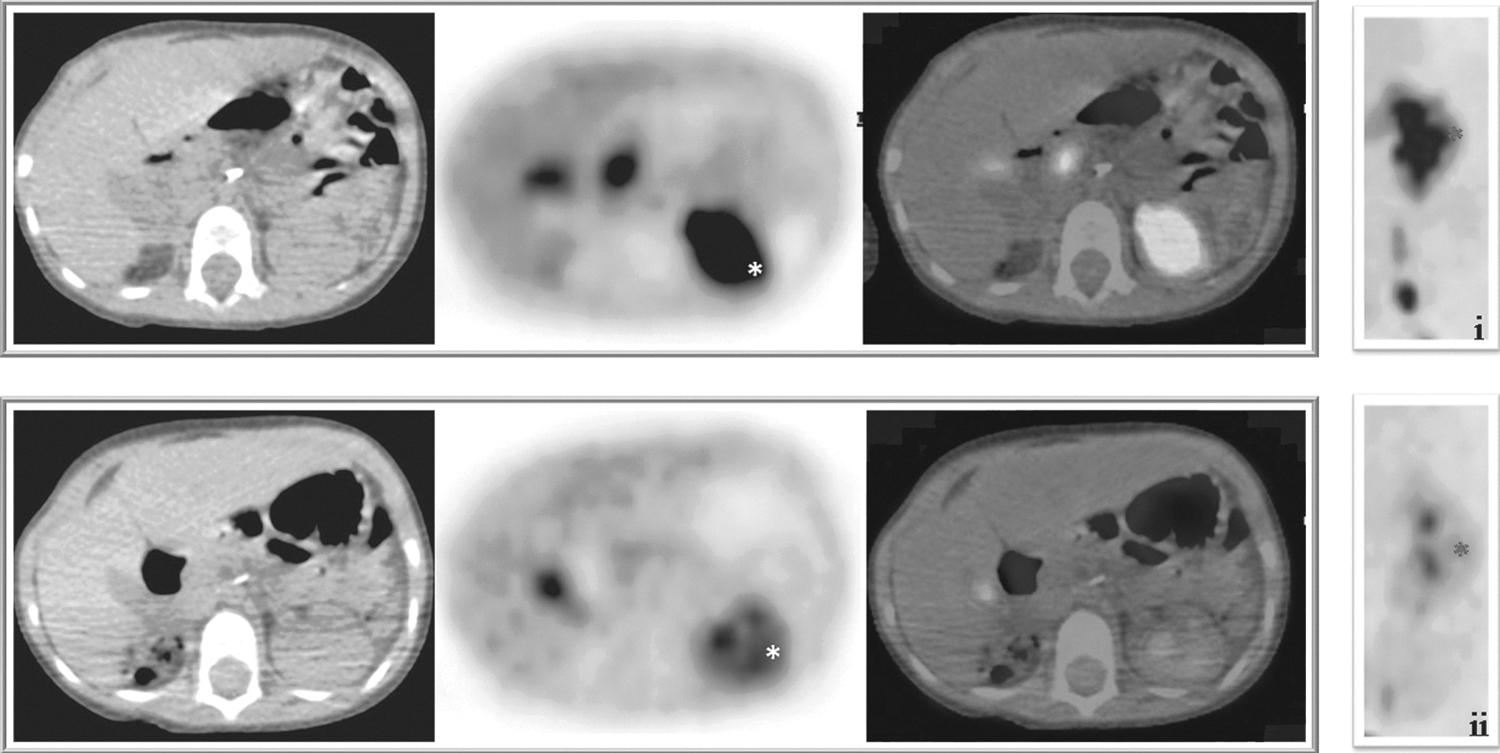
Axial images at the abdominal level of two different 18F-DOPA PET/CT scans of another patient (patient 4), obtained before and after carbidopa premedication (upper and lower panel, respectively). Note the reduced tracer accumulation in the excretory system (*indicates renal cortexes). The panels on the far right show segmental coronal images of the left kidney and renal pelvis before
The semiquantitative analysis conducted in respect of the principal tissues involved in the carbidopa effect (i.e., basal ganglia, pancreas, liver, and renal cortex), documented an absolute increase in SUVmax after carbidopa premedication in the basal ganglia (3.4±1.3 vs. 2.1±0.8) and liver parenchyma (2.2±0.5 vs. 1.5±0.5); in contrast, SUVmax decreased in the renal cortex (1.7±0.8 vs. 3.7±1.0) and the pancreas (2.3±0.6 vs. 3.5±0.5). As shown in Table 2, application of the t-test revealed the changes in SUVmax to be statistically significant for the pancreas and liver parenchyma (p=0.022 and 0.045, respectively), but not for the basal ganglia and renal cortex (p=0.143 and 0.15, respectively).
The t-test was used to evaluate differences between means, with p>0.05 considered significant.
Data obtained from 4 patients.
Discussion
The first article to be published on carbidopa premedication in PET scanning with 18 F-DOPA was by Hoffman et al., 13 who demonstrated the impact of AADC inhibition on tracer uptake in the striatal and cerebellar regions. Their findings were attributed mainly to the increased availability of 18 F-DOPA in the blood rather than to a direct effect of its intracellular management secondary to carbidopa premedication. Later on, Timmers et al. 14 highlighted the importance of carbidopa administration for imaging of pheochromocytomas and paragangliomas. They reported a direct improvement in 18 F-DOPA PET performance after carbidopa premedication owing to an increased tumor-to-background ratio, which led to an enhanced sensitivity of the method for the aforementioned tumors.
It is also known, however, that carbidopa premedication before
18
F-DOPA PET is not of benefit for all NETs.
15
In particular, it seems that insulinomas and β-cell hyperplasia may be falsely negative on
18
F-DOPA PET, with active lesions being fully masked when decarboxylation is prevented. This justifies the decision not to employ premedication with carbidopa when investigating focal β-cell hyperplasia in children with congenital hyperinsulinism.
16
In fact, no data are as yet available on carbidopa premedication in the pediatric population primarily because
18
F-DOPA is exclusively employed for congenital hyperinsulinism, and also because the main clinical role of carbidopa is in conjunction with
The present study, specifically addresses the question of whether carbidopa premedication is feasible in children as well as in adults, thus appears to be the first of its kind. Our preliminary findings seem to verify the feasibility of carbidopa premedication in children, which is important given that its use may become necessary in the context of potential new clinical indications for 18 F-DOPA in pediatric oncology. 17,18
The significant decrease in 18 F-DOPA uptake that was observed in the pancreas is attributable to the direct effect of carbidopa on the tracer retention in this tissue. 23 While the underlying mechanism is not fully understood, this effect seems to be related to intracellular inhibition of the enzyme AADC and retrograde diffusion of 18 F-DOPA in the interstitium. 24 In contrast, increases in 18 F-DOPA uptake were observed in the liver and basal ganglia, reaching significance in the former case; such increases are attributable to reduced decarboxylation after carbidopa premedication, which leads to a decrease in the excretion of 18 F-DOPA (Fig. 2) and an increase in the amount of circulating tracer, with enhanced bioavailability for these tissues.
Although tumor uptake—which could be the focus of further investigations—was not considered, it can be inferred that the effect of carbidopa on tracer distribution may be particularly relevant in case of neuroblastoma. In fact, this tumor most often presents in the retroperitoneum, with 35%–40% of cases in the adrenal glands and 30%–35% in the paraspinal ganglia. 25,26 Thus, the presence of physiologic uptake of the tracer in the pancreas and in the urinary system is a potential cause of a significant reduction in the sensitivity of 18 F-DOPA PET in these anatomic regions.
Undoubtedly, the reported study provides only extremely limited evidence, but the findings significant and worthy of communication to the scientific community were nevertheless considered. In our opinion, the introduction of carbidopa premedication in 18 F-DOPA PET scanning could in due course have an important impact on pediatric oncology. Further investigations and possibly multicenter studies on the subject therefore seem warranted.
Conclusions
Despite the very limited number of patients investigated in this study, some preliminary conclusions can be derived. First, carbidopa premedication in the pediatric population appears feasible.
Second, it seems to influence 18 F-DOPA distribution in normal tissues, particularly in the liver and pancreas, similarly to observations in adults. Investigations in larger series are however needed to validate the current findings and to properly assess the clinical role of carbidopa premedication in children.
Footnotes
Disclosure Statement
The authors declare to have no conflict of interest.