
Abstract
The primary treatment for nasopharyngeal carcinoma (NPC) is external beam radiotherapy. However, until now, there is little experience with the management of NPC occurred after solid organ transplantation. In this report, a 60-year-old man was found to have NPC (T2N1M0; stage III) 3 years after orthotopic liver transplantation treatment for hepatocellular carcinoma. Intensity-modulated radiotherapy (IMRT) was performed for NPC. One month after IMRT, complete response of NPC was achieved. However, multiple lung metastases occurred 18 months after the IMRT with the largest lesion measuring 4.1×5.5 cm and confirmed to be originated from NPC. Combined chemo-/targeted therapy consisted of capecitabine, and nimotuzumab was administered for four cycles. One month after initiation of capecitabine plus nimotuzumab treatment, a near-complete response was achieved for lung metastases. A repeat CT scan 1 year later showed sustained resolution of the lung metastases. The patient is still alive 16 months after the combined chemo-/targeted therapy.
Introduction
Cancer relapse and development of a new malignancy are the major problems after solid organ transplantation. A new malignancy after solid organ transplantation is called a de novo tumor (DNT). Long-term use of immunosuppressive is widely accepted as the major cause of a DNT, possibly through interleukin-2/T cell pathways. 1 Furthermore, there is mounting evidence that some specific viral infections, such as human papillomavirus (HPV), are closely related to certain kinds of solid tumors. 2 Herein, we report a case of nasopharyngeal carcinoma (NPC) post liver transplantation treatment for hepatocellular carcinoma (HCC) who was successfully treated with radiotherapy to the primary site and then chemo-targeted therapy for multiple lung metastases. The Institutional Review Board of the authors' hospital approved the retrospective report of this case. Informed consent was also obtained from the patient. DNT represents a distinct category of disease with unique carcinogenesis and prognosis. Personalized therapy is required for patients like the current NPC case.
Case Report
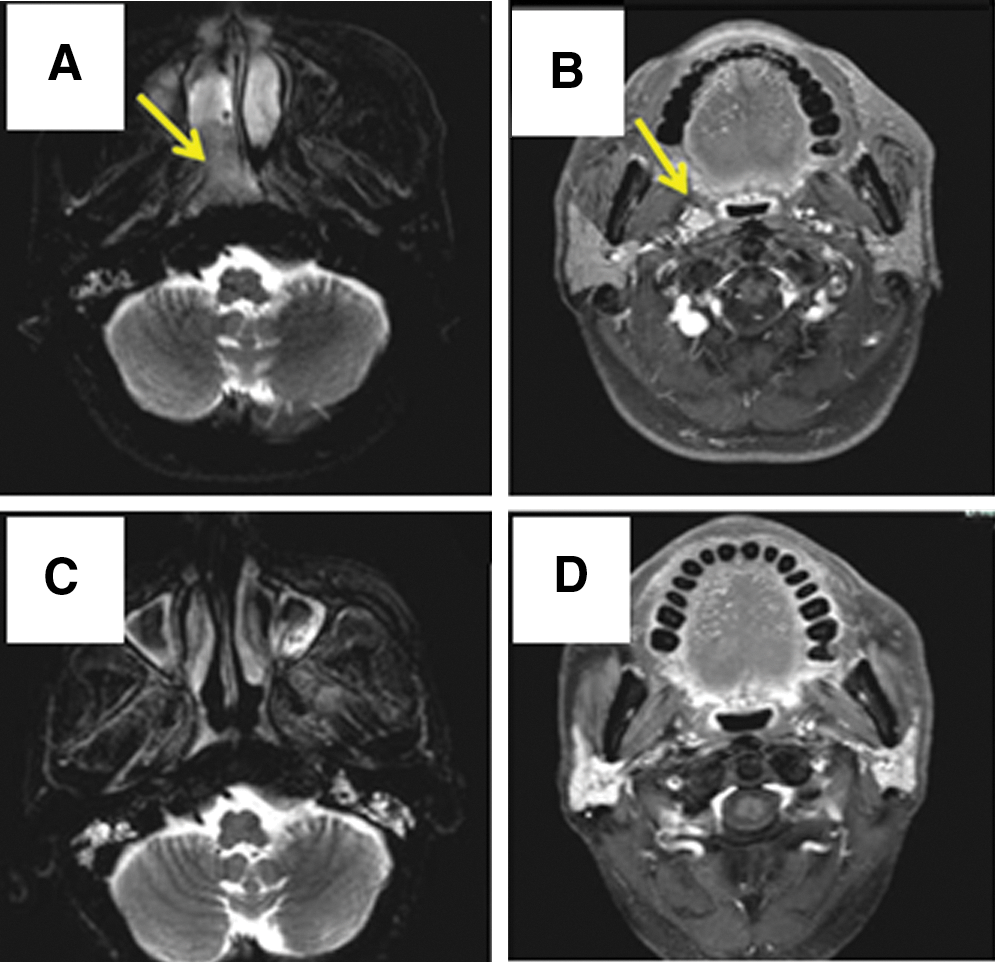
A 60-year-old man, who was found to have HCC and subsequently received a partial hepatectomy in 2003, received orthotopic liver transplantation (OLT) in 2006 for multiple intrahepatic metastases of HCC. The patient has been taking antirejection medications since OLT, and iatrogenic diabetes mellitus developed 1 year later. In February 2009, this patient experienced severe right-sided rhinocleisis with intermittent epistaxis. Nasopharyngoscope-guided biopsy revealed a nonkeratinizing differentiated NPC. Further magnetic resonance imaging (MRI) and other imaging studies concluded the diagnosis of NPC, classified clinically as T2N1M0 (AJCC stage III) (Fig. 1A, B). This patient's Karnofsky performance status (KPS) scored 80. This patient also had degree II leucopenia and thrombocytopenia caused by hypersplenism.
After careful evaluation of the patient's KPS and hematological studies, radiotherapy alone was applied with the support of granulocyte-colony stimulating factor (G-CSF) and recombinant human thrombopoietin (rhTPO). Specifically, intensity-modulated radiotherapy (IMRT) was used to deliver the prescribed doses of 7194 cGy/33 fractions to the gross tumor volume in the nasopharynx, 6976 cGy/32 fractions to the metastatic cervical node, and 6016 cGy to elective nodal stations (Fig. 2). The patient tolerated the treatment well, except for frequent degree II–III hematological events that did not lead to symptomatic infection or bleeding (Fig. 3).
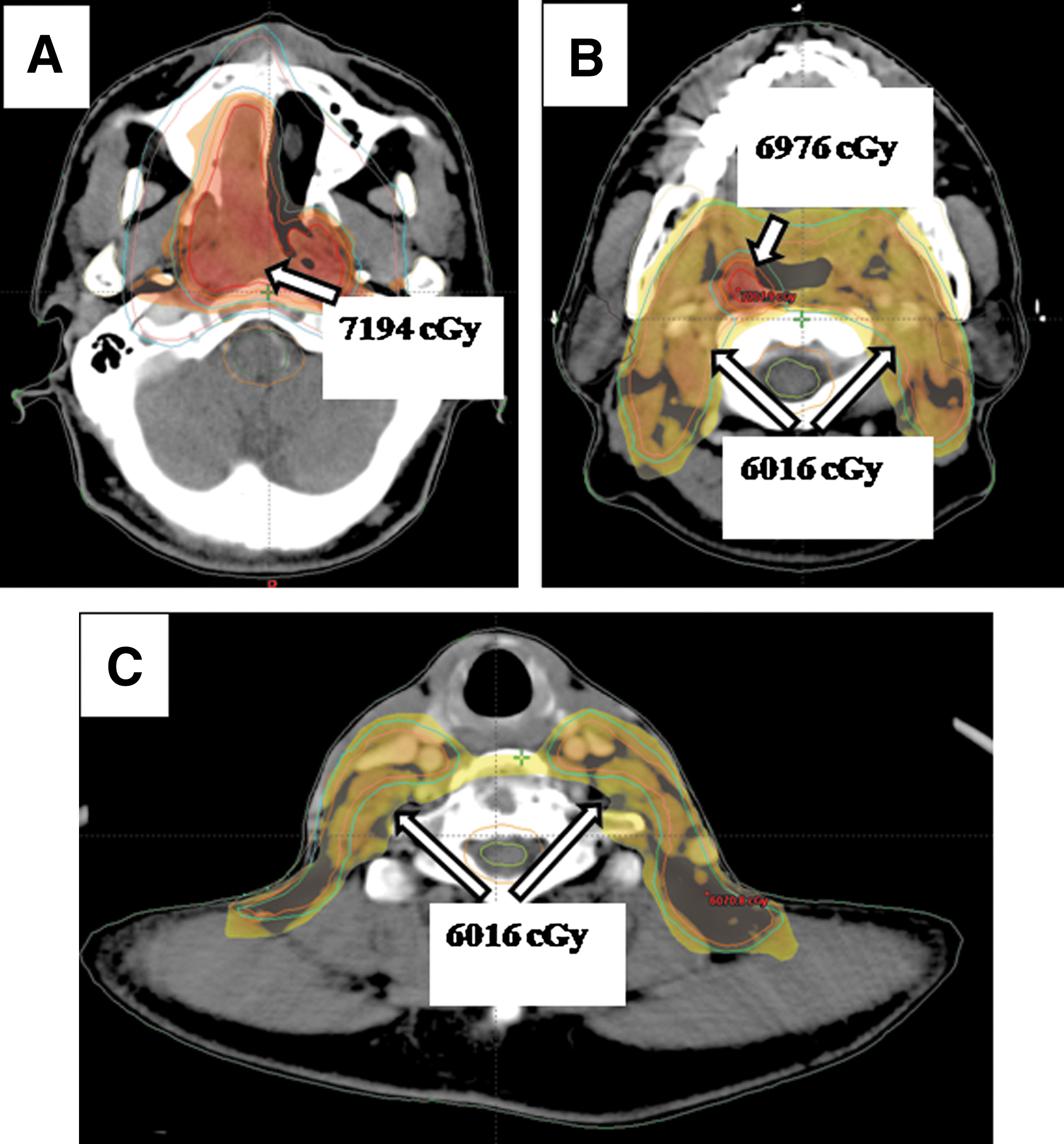
Display of isodose lines with IMRT at three different levels.
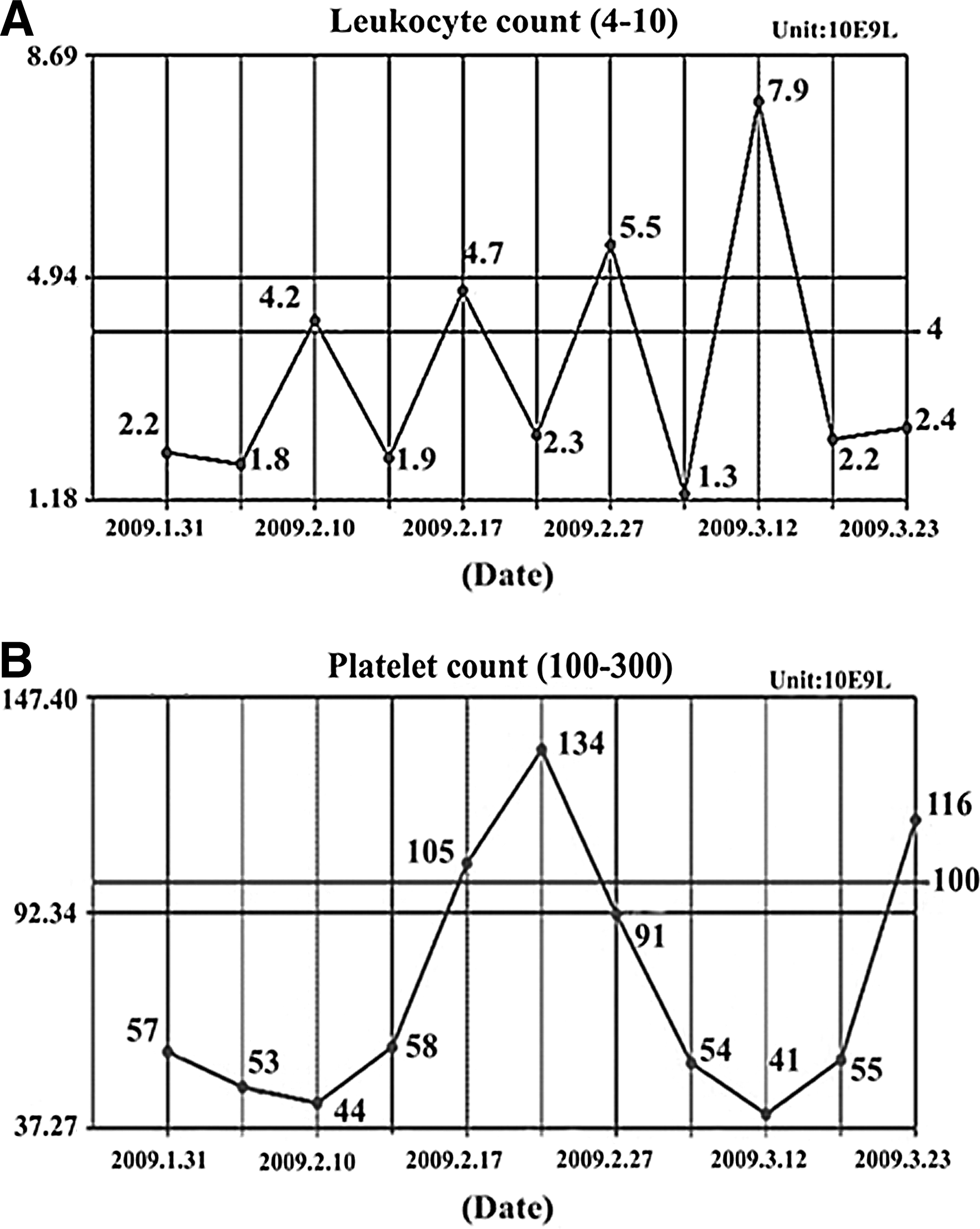
The curves of leukocyte count
One month after radiotherapy, a complete response (CR) was achieved at both the primary site and the metastatic lymph node based on MRI studies (Fig. 1C, D). No locoregional or distant relapse was found on routine follow-up until October 2010 (i.e., 18 months after radiotherapy), when chest CT revealed multiple mass lesions in bilateral lungs (Fig. 4A, B). CT-guided needle biopsy of the largest lesion in the right upper lobe disclosed a moderately to poorly differentiated squamous cell carcinoma, indicating metastasis from the previously treated NPC rather than HCC. Considering that the patient could not tolerate an intensive chemotherapy, capecitabine (Xeloda; Roche Laboratories, Nutley, NJ) was given orally at a dosage of 1000 mg/m2, twice daily for 14 days in a 21-day cycle. In addition, an intravenous 100 mg nimotuzumab (YM BioSciences, Inc., Mississauga, Canada) was given weekly for 3 consecutive weeks. Nimotuzumab is approved in this country for use in stage III/IV NPC. One month after initiation of capecitabine plus nimotuzumab treatment, a near CR was achieved in both lungs with only some patchy shadows remained, possibly representing fibrosis. In total, 4 cycles of capecitabine plus nimotuzumab were given. Dermatological reactions appeared 2 weeks postcapecitabine administration and aggravated rapidly to grade 3 hand-foot syndrome (HFS). No other adverse events were observed with clinical significance, and the transplanted liver has been functioning well during and after the treatment. A repeat CT scan 1 year later showed sustained resolution of the pulmonary metastases except for some fibrosis (Fig. 4C, D). The persistent HFS greatly influenced the patient's quality of life; hence, no further chemotherapy or targeted therapy was administered thereafter. The patient is still alive, till the time of this report, with no sign of disease relapse. Except for degree I xerostomia, the patient is free of any radiation-induced late events such as trismus, cranial neuropathy, or myelopathy. An immunohistochemical study was carried out for the biopsied NPC specimens from both the primary and the metastatic sites for possible p16 protein expression, which associates with a HPV infection. The result was negative for both specimens.

Discussion
Development of secondary malignancies is one of the medium- and long-term complications after solid organ transplantation. It is also considered as one of the obstacles toward the ultimate success of transplantation. Secondary malignancies after solid organ transplantation are also called de novo malignancies (DNT). Its occurrence rate is reported to be 5%–16% in cases of liver transplantation. 3 –6 According to a Finnish study, cancer incidence increased in patients received liver transplant compared to the general population, with an overall SIR (standardized incidence ratio) of 2.59 (95% confidence interval 1.84–3.53). 7 In their study, nonmelanoma skin cancers were by far the most common cancer types, and non-Hodgkin lymphoma ranked second. Rubio et al. reported a single-institutional experience of DNT after OLT in Spain. The incidence of DNT was as high as 7.8%, with the most frequent types being epidermoid carcinomas and smoking an independent risk factor. 8 In Asia, a recent report by Park et al. 9 from Korea showed that among 1952 OLT recipients, 44 (2.3%) developed DNT after a mean follow-up of 45 months, and the incidence of gastric cancer ranked first. Of the 44 DNT patients, 43 received aggressive treatment, including surgery, chemotherapy, and radiotherapy. Although a DNT can be associated with multifactorial combination, including the individual and regional predispositions, long-term use of immunosuppressives is considered the major cause. Our patient has been taking tacrolimus since OLT 5 years ago. Tacrolimus exerts its immunosuppressive actions through inhibition of interleukin 2 (IL-2) transcriptions, which in turn blocks T cell activation. Tacrolimus was also reported to inhibit IL-12 and tumor necrosis factor α production by monocyte-derived human myeloid dendritic cells, which in turn decreases the TH1 proliferation response. 10 Furthermore, an earlier study revealed that tacrolimus reversed multidrug resistance to antitumor agents in mammalian cells. 11 This may partially explain why combined capecitabine and nimotuzumab treatment achieved such a good clinical response in the current case of metastatic NPC.
Treatment approaches for a DNT are in principal similar to those used for cancers in the general population. However, compliance with treatment is usually decreased in organ recipients. Patients after transplantation generally take immunosuppressives to counter rejection. Aggressive treatments may pose threats to an immunocompromised patient, sometimes even harmful to the grafts. It is well established that radiotherapy, not surgery, plays a major role for the treatment of early or locoregionally advanced NPC. It is also the current standard for concurrent chemoradiotherapy (CRT) to be used for NPC staged III or above. Our case was initially a stage III disease without distant metastasis other than an ipsilateral retropharyngeal lymph node (N1). CRT was not administered because of the unfavorable baseline hematological profile, including grade II leucopenia and thrombocytopenia, and the concerns about negative influence on graft function. Radiotherapy alone was considered a reasonable option for this patient. Supported by G-CSF and rhTPO, the patient eventually completed the planned course of radiotherapy without significant complications.
For multiple lung metastases, a satisfactory therapeutic response was achieved by combined chemo- and antiepidermal growth factor receptor (EGFR) therapies, although with severe HFS. Lung metastases from either NPC or HCC are commonly seen in clinical practice; however, treatment strategies differ greatly between the two entities. In cases of NPC diffusely metastasized to the lungs, cisplatin-based chemotherapy plus fluropyrimidine (5FU or capecitabine) is considered to be the most effective treatment. In the present case, capecitabine was attempted as first-line chemotherapy due to the patient's longstanding leucopenia and thrombothytopenia as well as the immunocompromized status postliver transplantation. Capecitabine is a new oral fluoropyrimidine carbamate that generates 5-FU selectively in tumors in the presence of thymidine phosphorylase that is richer in tumor cells than in normal tissues. A recent phase II study reported an objective response rate of 24.2%, CR of 6% for capecitabine in the palliative treatment of head and neck squamous cell cancers (HNSCC) with locoregional and/or metastatic relapse after previous platinum-based treatment. 12 Earlier studies in colorectal cancers have also proved that capecitabine is noninferior to 5-FU, with fewer side effects such as myelosuppression, stomatitis/mucositis, and diarrhea than 5-FU. On the other hand, one well-known side-effect of capecitabine is HFS. 13 Clinical trials have shown that HFS is the most common adverse effect of capecitabine administration, with an overall incidence of about 45–86%. 10,14 –17 Although no discontinuation or dose reduction was carried out during 4 cycles of treatment in the present case, no further cycle was given due to the patient's symptoms of HFS.
In recent years, the application of new molecular-targeted biologics in combination with conventional chemotherapy has been reported to improve the survivals of recurrent or metastatic HNSCC patients. 18 Cetuximab is the most studied recombinant immunoglobulin targeting EGFR. The rationale for adding cetuximab to chemotherapy is the fact that EGFR is overexpressed in most HNSCC and correlated with poor disease prognosis. 19 As one of the humanized antibodies against EGFR, nimotuzumab has also been shown to be potent in treating HNSCC, glioma, and NPCs. 20 Clinically, nimotuzumab has demonstrated a better toxicity profile, including less acneiform rash than cetuximab. Anti-EGFR antibodies are most often used in combination with platinum-based chemotherapeutics, especially in those chemonaive HNSCC patients. In the current case, capecitabine plus nimotuzumab was optioned after careful evaluation of the patient's physical status and laboratory data.
The incidence of HPV infection has been reported to be related to the occurrence of squamous cell carcinoma in solid organ transplantation recipients. 21 –24 HPV-derived oncoproteins E6 and E7 can inactivate the potent tumor suppressor gene pRb, which in turn leads to a significant overexpression of the p16 protein. 25,26 Clinically, p16 protein-positive tumors have the same characteristics as HPV-positive tumors, including an advanced overall stage and better prognosis. 27 However, the result for p16 expression was negative in the current case.
Conclusions
We report a case of OLT-related DNT-NPC that was successfully treated with IMRT initially in the primary site and then chemo-/targeted therapy for multiple lung metastases. DNT-NPC might represent a distinct category of disease with unique carcinogenesis and prognosis. Further studies are warranted to identify biomarkers that are related to the occurrence of DNTs, so that more effective treatment strategies for this subset of cancer patients can be developed.
Footnotes
Disclosure Statement
The authors declare no conflict of interest.