
Abstract
Introduction:
Currently, the best sequence of targeted therapy in patients with metastatic renal cell carcinoma (mRCC) has not been sufficiently defined and is based on the patient's and physician's decision, which may be influenced by comorbidities and toxicity profiles. The aim of this study was to evaluate the outcome of target therapies on clinical practice after the era of cytokine-based therapy in mRCC.
Materials and Methods:
We retrospectively analyzed all consecutive patients with mRCC treated at our Clinical Oncology Unit from June 1998 to September 2010.
Results:
We evaluated 61 patients: 21 (34.4%) with only cytokine-based therapy (95.2% interferon-α), 24 (39.3%) with target therapies in first line (100% sunitinib), and 16 (26.2%) with target therapies in second or subsequent line. Median time follow-up was 16.18 months (range 2.1–171.1). Considering the type of therapy, the univariate analysis for overall survival showed statistically significant advantages for the use of target therapies in second or subsequent line (p=0.024).
Conclusions:
Our data and consequently our proposal to revaluate the role of immunotherapy (also with the possibility of adding bevacizumab) in the first line are heavily provocative to point out the attention to this actually partially unsolved question; other larger experiences, pre-eminent opinion, and clinical trials are needed.
Introduction
In recent years, an improved understanding of renal cell carcinoma (RCC) tumor biology has translated into major advancements in the treatment of patients with metastatic RCC (mRCC). 1 Up to the end of the last decade, cytokine-based therapy was the only, even if only moderately, effective systemic therapy for mRCC. 2 The treatment of mRCC has changed dramatically over the past few years: targeted therapies have fundamentally altered the therapy of mRCC. In particular, the hypoxia-inducible factor (HIF)/vascular endothelial growth factor (VEGF) pathway and the mammalian target of rapamycin (mTOR) signal transduction pathway have been exploited: 3,4 sunitinib (Sutent®) 5 and sorafenib (Nexavar®) 6 as multikinase inhibitors, everolimus (Afinitor®) 7 and temsirolimus (Torisel®) 8 as mTOR inhibitors, and bevacizumab (Avastin®) as an antibody against VEGF in combination with interferon-α (IFN-α). 9 Actually sunitinib is a reference standard of care in the first-line therapy for the treatment of mRCC. 10,11 Currently, the best sequence of targeted therapy in patients with mRCC has not been sufficiently defined and is based on the patient's and physician's decision, which may be influenced by comorbidities and toxicity profiles. 12,13 The advent of targeted therapy in mRCC does not eliminate the potential utility of immunotherapy, but rather requires a rational refinement of this approach through improvements in patient selection and combination therapy that may increase the cure rate for patients with this disease. 1 The aim of this study was to evaluate the outcome of target therapies on clinical practice after the era of cytokine-based therapy in mRCC.
Materials and Methods
We retrospectively analyzed all consecutive patients with mRCC treated at the Clinical Oncology Unit of the University Hospital of Ferrara from June 1998 to September 2010; this period was selected to have three groups of patients balanced each other, reflecting the most important changes in mRCC treatment. All information was obtained from the case history, and we reviewed the patient's medical history (from hospital records only). All data were registered in an Excel workbook. We excluded patients in which the time follow-up was <1 month; time follow-up was defined as the time in which patients have been followed at our institution since initiating first treatment for mRCC for all patients. The measurements of all laboratory values were made in the same structure. A univariate analysis for different prognostic variable on overall survival (OS) was estimated according to the Kaplan–Meier method with statistical significance (p<0.05) of differences evaluated by the log-rank test; the initial date for survival was calculated from the date mRCC was first recognized. The multivariate analysis was executed with the Cox regression model. We chose to consider only OS and not progression-free survival (PFS), because in the absence of a prospective design to determine whether disease progression has occurred at specific defined intervals, this measurement is fraught with potential bias because patients may be followed with differing frequencies depending on whether they are in a clinical trial or what specific therapy they are receiving. We divided the general case study into three subgroups: patients treated only with immunotherapy, patients treated with immunotherapy in first line and with target therapies in second or subsequent lines, and patients treated with target therapies in first line, and we compared results in term of OS, censoring surviving patients at the time of last follow-up. Finally, we compared the kind of therapy with the Memorial Sloan-Kettering Cancer Center (MSKCC) risk score 14 and the modified Motzer risk score 15 using Cross-tabulation– Pearson Chi-Square, to exclude any possible relationship between results and different risk categories.
Results
We evaluated 61 patients: 21 patients (34.4%) were treated with only cytokine-based therapy (because nothing else was available at the time; INF-α was used in 95.2% of patients; see Fig. 1), and 24 patients (39.3%) were treated with target therapies in first line (100% sunitinib), and 16 patients (26.2%) were treated with target therapies in second (sunitinib was used in 9 cases, corresponding to 56.3%) or subsequent line (INF-α was used in 93.7% of patients; see Fig. 2; in these cases, patients received immunotherapy first and target therapies at disease progression; no patients received target therapies first and immunotherapy at relapse or as a planned sequence of therapy). There were no patients that were treated in clinical trials. Thirty-one patients (50.8%) have received a second-line therapy: 9 patients (29.0%) have received sunitinib (100.0% of these patients have received INF-α in first line); 8 patients (25.8%) have received sorafenib [first line: 12.5% INF-α, 12.5% interleukin-2 (IL-2), 75.0% sunitinib]; 5 patients (16.1%) have received chemotherapy (first line: 60.0% INF-α, 40.0% IL-2); 4 patients (12.9%) have received only IL-2 (first line: 75.0% INF-α, 25.0% chemotherapy); 2 patients (6.5%) have received chemotherapy plus IL-2 (100.0% INF-α in first line); 2 patients (6.5%) have received chemotherapy plus INF-α (first line: 50.0% INF-α and 50.0% INF-α plus IL-2); and 1 patient (3.2%) has received everolimus (sunitinib in first line); 11 patients (17.7%) have received a third line, 4 patients (6.5%) a fourth line, and 1 patient (1.6%) a fifth-line therapy. At the last follow-up (September 2010), 16 patients (26.2%) were alive with metastasis; 40 patients (65.6%) were deceased, and 5 patients (8.2%) were lost during follow-up (PFU). The median time follow-up was 16.18 months (range 2.1–171.1). Considering each of these treatment-based subsets of patients, for patients treated with only immunotherapy (especially in early years, before 2007), the median time follow-up was 24.3 months (range 2.1–70.4); for patients treated with target therapies in second or subsequent lines (especially in late years, after 2007 for patients with previous treatment for mRCC), the median time follow-up was 25.2 months (range 5.8–171.1), and for patients treated with target therapies (especially in late years, after 2007 for patients with new diagnosis of mRCC) in first line, the median time follow-up was 11.6 months (range 3.5–47.2). The median age was 62.0 years (range 37–81 years); 47 patients were male (77.0%) and 14 female (23.0%); prevalent histology (52 patients) was clear cell carcinoma (85.2%); in 2 cases (3.9%), grading was 1, in 23 cases (45.1%) was 2, in 16 patients (31.4%) was 3, and in 10 (19.6%) was 4. In 52 patients (86.7%), a nephrectomy for the primary site was performed: in 19 cases (35.8%), patients were metastatic after surgery. Twenty-three patients (37.7%) had 1 site of metastases, and 16 patients (26.2%) had 2 sites and 22 patients (36.1%) more than 3 sites at the time of diagnosis of metastatic disease. According to the MSKCC risk score, 9 5 patients (8.2%) had a favorable risk, 34 patients (55.7%) an intermediate risk, and 22 patients (36.1%) a poor risk; according to the modified Motzer risk score, 10 28 patients (45.9%) had a favorable risk and 33 patients (54.1%) a poor risk. Considering all variants of these categories, 27 patients (44.3%) had anemia (median value=12.1 g/dl, range: 7.7–17.0), and the LDH levels were>1.5× upper limit of normal in 6 patients (9.8%, median value 384 U/L, range: 196–3059), and 50 patients (82.0%) had a high corrected serum calcium level (median value=12.1 mg/dL, range: 7.1–19.6); ECOG performance status (PS) was 0 in 18 patients (29.5%), 1 in 26 patients (42.6%), and 2 in 17 patients (27.9%); in 35 patients (57.4%), the time between initial diagnosis and therapy was <1 year. Univariate analysis for OS (Kaplan–Meier method) showed statistically significant differences for the number of sites of metastasis (p=0029), the presence of metastasis to central nervous system (CNS) (p<0.001), the presence of anemia (p=0.027), high LDH (p=0.007), ECOG PS (p=0.002), time between initial diagnosis and therapy <1 year (p=0.022), the prognostic categories according both to the MSKCC risk score system (p=0.022), and to the modified Motzer risk score (p=0.001). All the results are summarized on Table 1. At the multivariate analysis, the presence of CNS metastasis (p<0.001), the presence of anemia (p=0.033), high LDH (p=0.002), and ECOG PS (p<0.001) have shown as prognostic-predictive factors. There was no statistical relationship between the kind of treatment and the risk categories according to both the MSKCC and modified Motzer risk scores. The univariate analysis for OS (Fig. 3) showed statistically significant advantages for the use of target therapies in second or subsequent line (p=0.024). Median OS for patients treated only with immunotherapy in first line (21 patients, 34.4%) was 20.4 months (95% Confidence interval [CI]: 2.8–38.0); for patients treated with immunotherapy in first line and with target therapies in second or subsequent lines (16 patients, 26.2%), OS was 47.4 months (95% CI: 12.9–81.8), and for patients treated with target therapies in first line (24 patients, 39.3%), OS was 16.4 months (95% CI: 10.8–22.0). Comparing sequential therapy (median OS: 47.4 months, 95% CI: 12.9–81.8) versus other two curves combined (median OS: 19.8 months, 95% CI: 13.8–25.7), the univariate analysis showed statistically significant (p=0.007) for the use of target therapies in second or subsequent line (Fig. 4). Comparing sequential therapy versus only immunotherapy (median OS: 20.4 months, 95% CI: 2.8–38.0), the univariate analysis showed statistically significant (p=0.005) for the use of target therapies in second or subsequent line (Fig. 5). Comparing sequential therapy versus target therapies in first line (median OS: 16.4 months, 95% CI: 10.8–22.0), at the univariate analysis, there was no statistical significance difference in OS (p=0.101) between the two subgroups, with only a positive trend for the use of target therapies in second or subsequent line (Fig. 6).
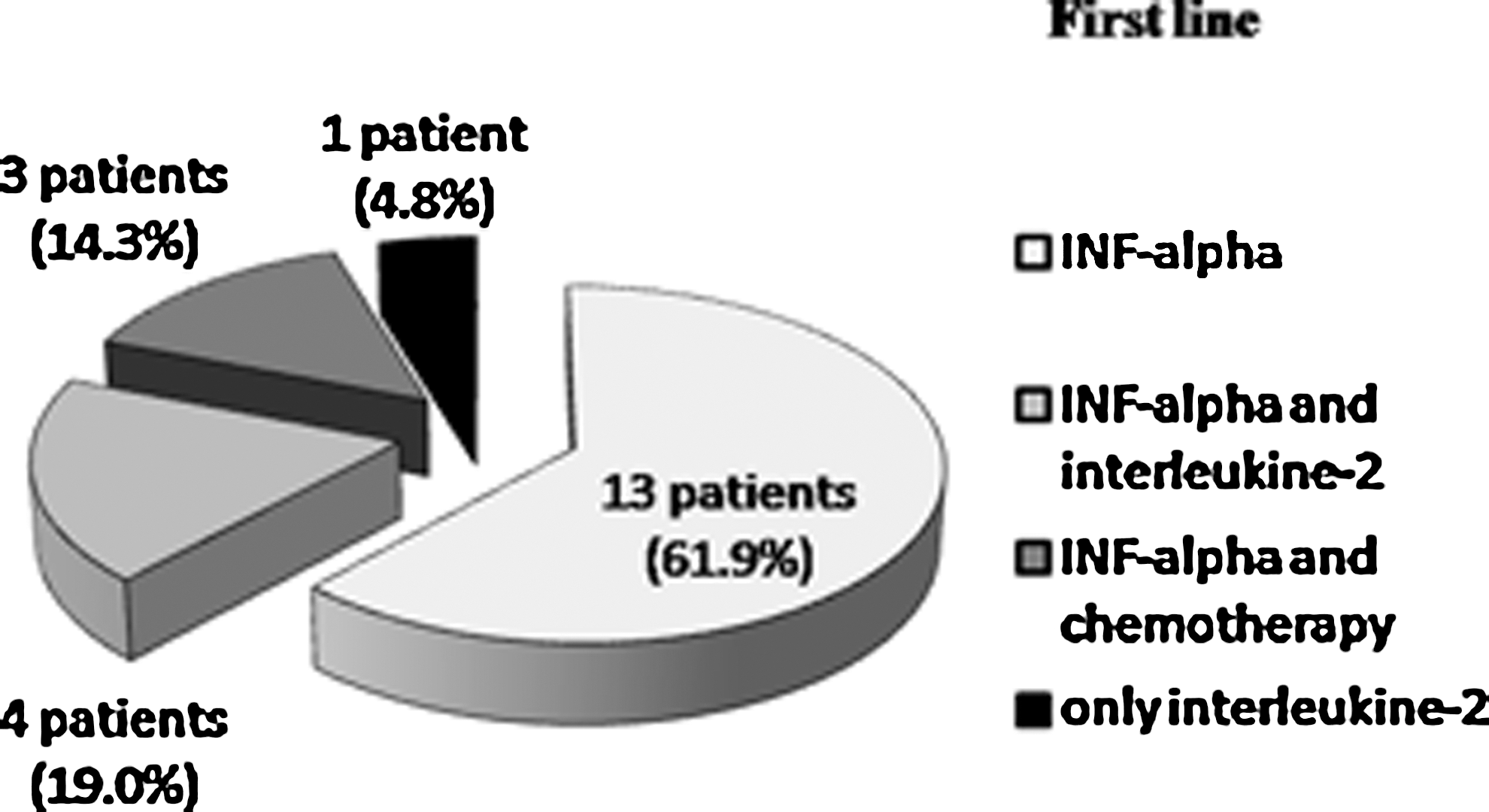
First line in patients with mRCC treated with only cytokine-based therapy. mRCC, metastatic renal cell carcinoma.
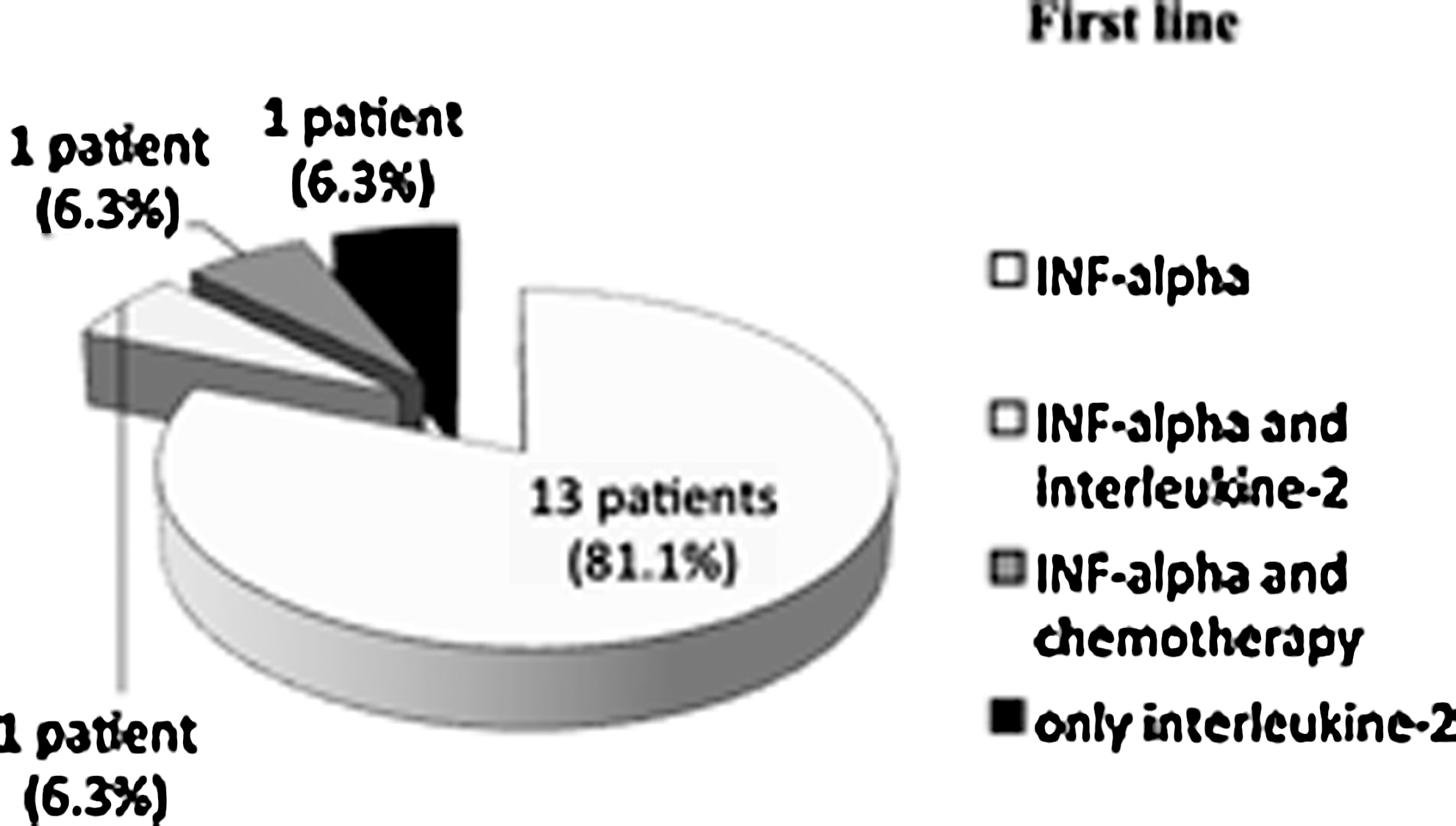
First line in patients with mRCC treated with target therapies in second or subsequent line.
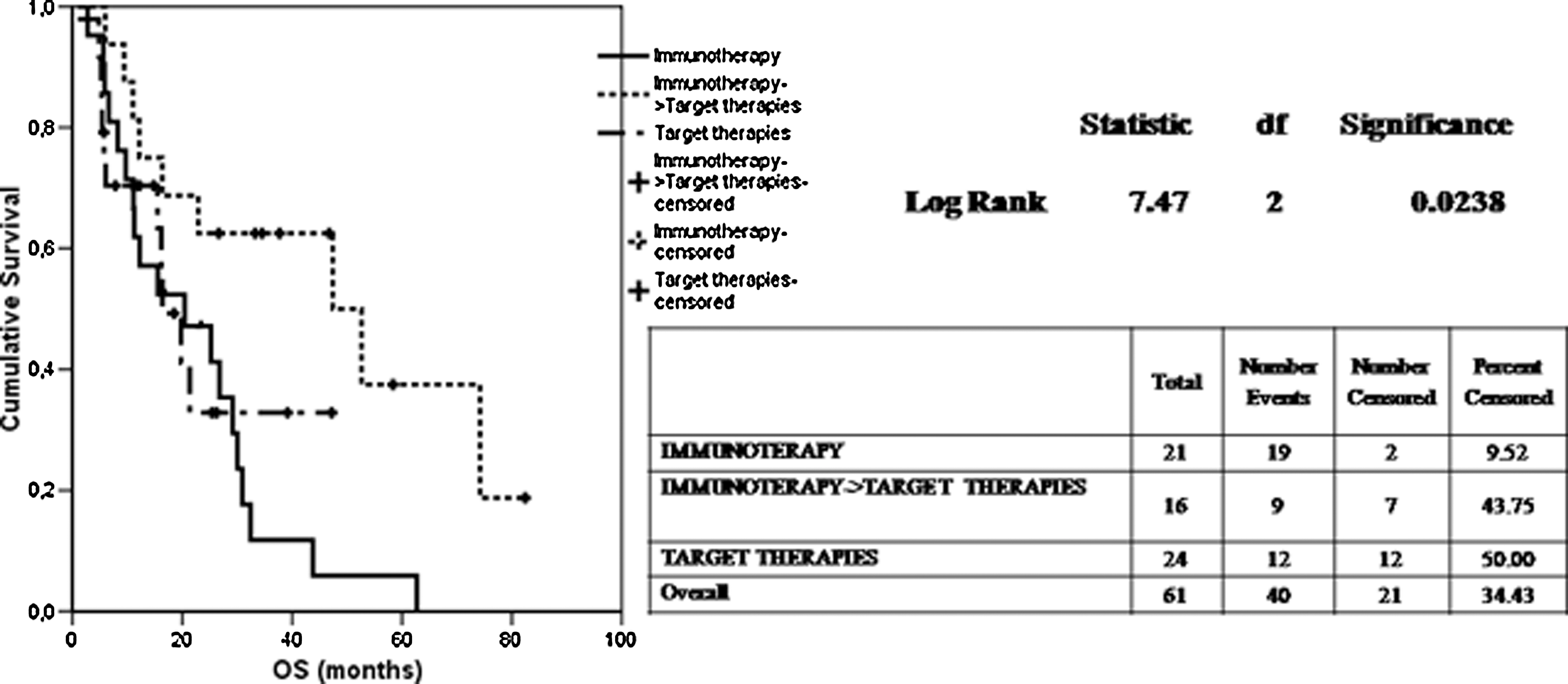
Univariate analysis for OS considering the different types of therapy. OS, overall survival.
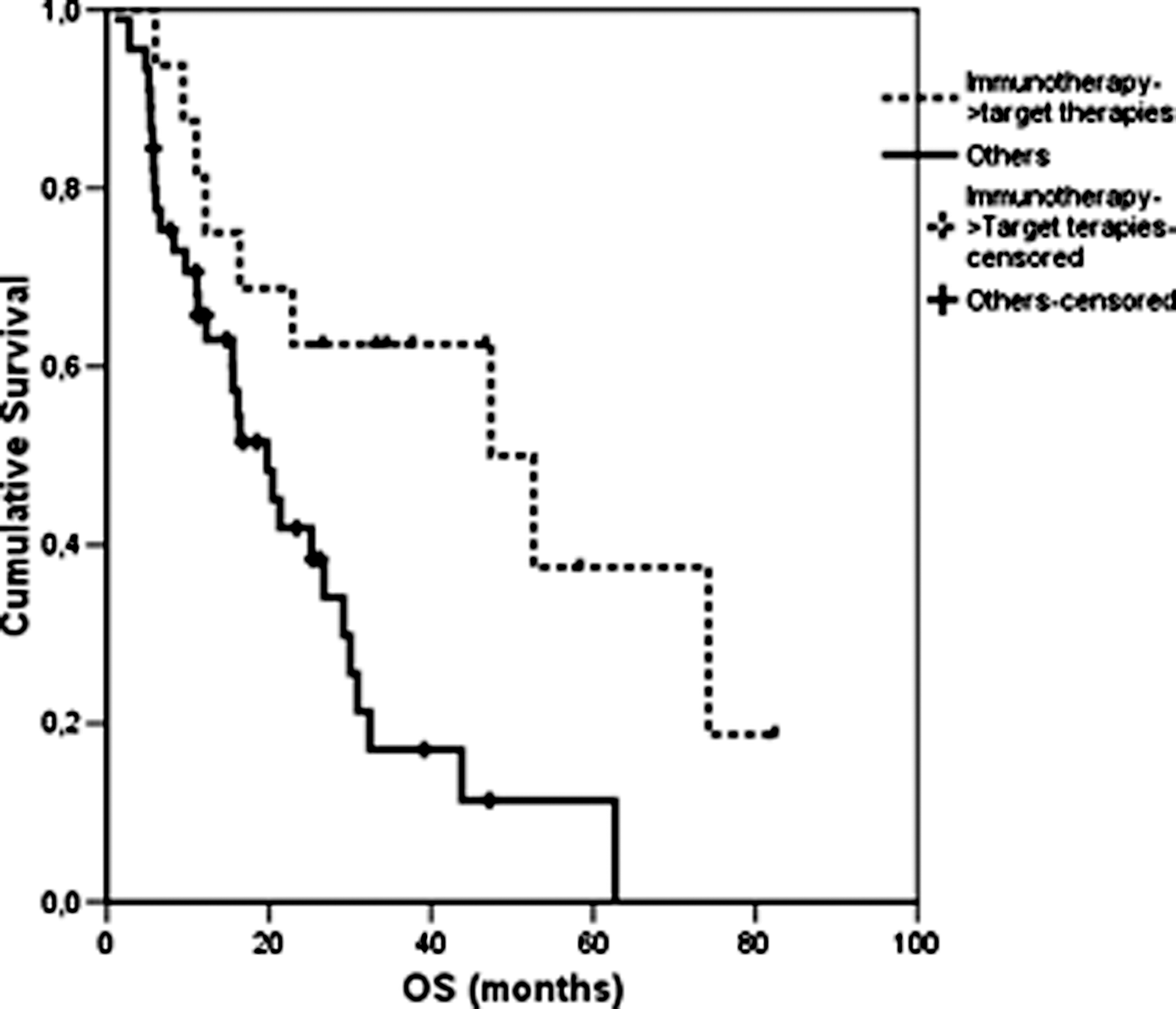
Univariate analysis for OS considering patients treated with sequential therapies versus patients treated with other therapies.
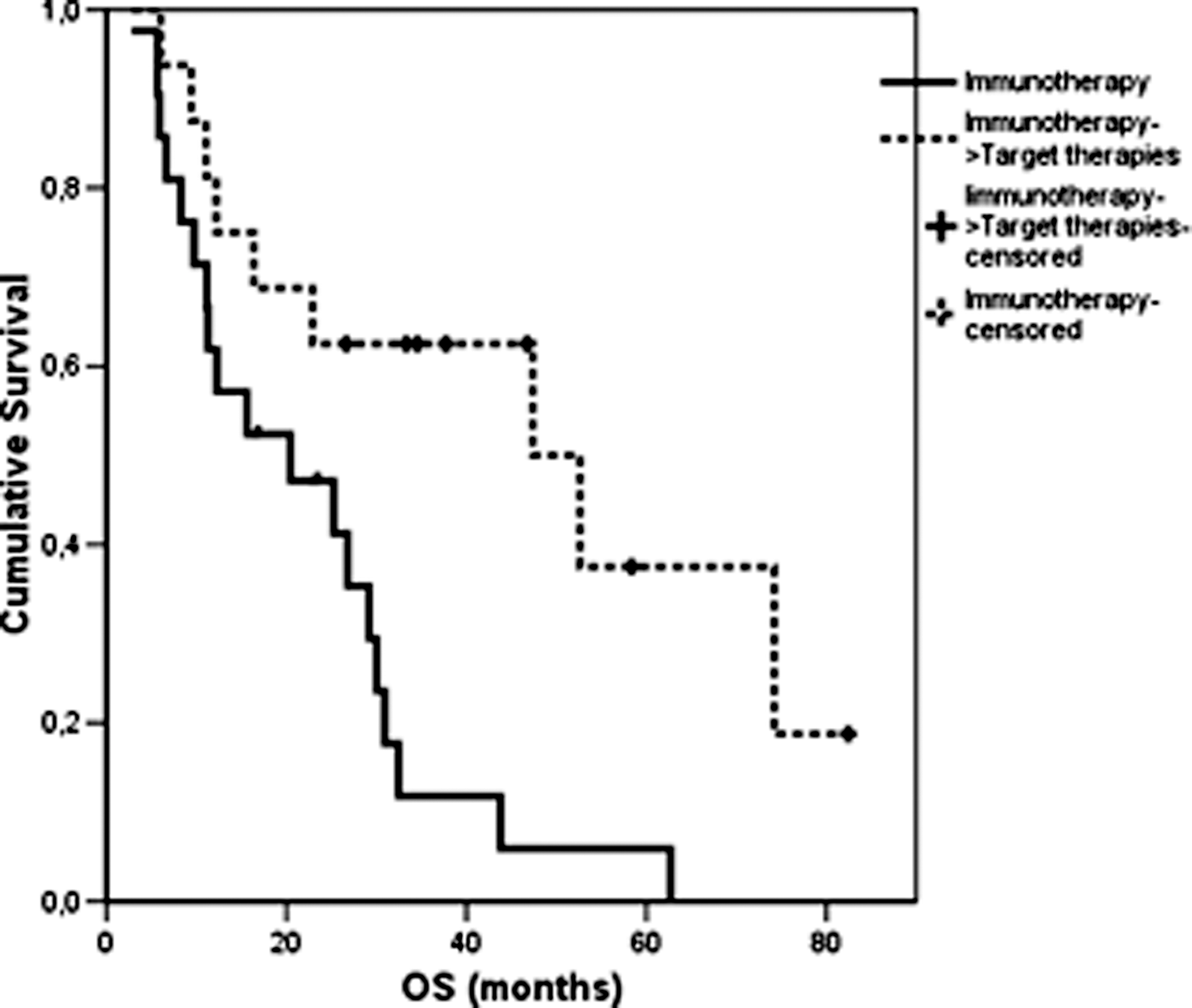
Univariate analysis for OS considering patients treated with sequential therapies versus patients treated with only immunotherapy.

Univariate analysis for OS considering patients treated with sequential therapies versus patients treated with target therapies in first line.
Bold type indicates values with statistical significance (p<0.05).
n, number of patients; LDH, Lactate dehydrogenase; CNS, central nervous system; OS, overall survival; MSKCC, Memorial Sloan-Kettering Cancer Center.
Discussion
Agents targeting VEGF and mTOR pathways improve PFS in both first-line and second-line settings. 16 Several clinical questions have thus emerged in regard to the optimal timing, type, and sequence of targeted therapy in mRCC. 17 Different retrospective experiences analyzed the clinical outcome of the sequential use of sunitinib and sorafenib in mRCC: differences in baseline characteristics, including histology and line of treatment, were not significant, and toxicity was not increased during the second part of the sequence with apparent more durable disease control when sorafenib was followed by sunitinib. 18,19 Our data show a possible best sequence of treatment in mRCC, revaluating a potential role of immunotherapy (in particular INF-α) in first line; in fact, the best results in term of OS were obtained for patients treated with immunotherapy (especially INF-α) in first line and with target therapies in second or subsequent lines compared with patients treated only with immunotherapy and patients treated with target therapies in first line. These results were probably related to the best rationalization of the sequential use of all possible drugs. High-dose IL-2 and IFN-α were the most commonly administered therapies before the recent introduction of targeted agents, but since the introduction of targeted therapies, the use of immunotherapy, and in particular single-agent IFN, has decreased significantly, and it remains in the frontline setting in combination with bevacizumab. 20 This study can introduce a possible idea of best therapy sequence in mRCC, consequent with the revaluation of a possible the role of bevacizumab in first line, to overwork all available drugs. We know from the randomized phase III trial of sunitinib versus INF-α that the median OS was greater in the sunitinib group than in the INF-α group, 5 and we do not dispute these much larger data, but we shift the attention on the problem of the correct sequence of therapy in patients with mRCC, to take advantage of the increasing number of treatment options that actually excluded for example the use of INF-α and bevacizumab at the outside of the first line. 9 We also know both the limit of a retrospective study, the small size of the cohorts, and the fact that data coming from a single institution could reflect only the habits of that particular set of physicians; on the contrary, studies like the above, though the analysis of not selected casistics, are able to evaluate treatment patterns in a real-world clinical practice, reflecting changes in therapy prescription (patients received cytokines in the pre-TKI era). Other retrospective studies have also emphasized the potential significance of utilizing immunotherapy in the initial treatment of mRCC in order to optimize treatment options and in particular considering IL-2 as the initial therapy in any patients with mRCC who are medically fit for such therapy, based on the fact that if other therapies are used first, patients who were potential candidates for IL-2 may deteriorate because of progressive disease or complications of these other therapies and may no longer be suitable for IL-2; moreover, it is unclear whether treatment with target therapies is associated with long-term survival benefit. 21 Our conclusions partially agree with this results, but there were some differences between these two different retrospective experiences and in particular that the study we mentioned considered only patients treated with high-dose IL-2 to determine the long-term survival of patients who were treated with IL-2; instead, our study counted a general casuistic composed by all consecutive patients with mRCC treated at our Clinical Oncology Unit to identify a possible best sequence of therapy. Our data and consequently our proposal are heavily provocative to point out the attention to this actually partially unsolved question; obviously other larger experiences, pre-eminent opinion, and clinical trials are needed.