
Abstract
A standard salvage therapy of relapsed/refractory aggressive non-Hodgkin lymphoma (NHL) comprises autologous stem cell transplantation (ASCT) after chemotherapy conditioning with carmustine, etoposide, cytarabine, and melphalan (BEAM) regimen. However, the achievement of long-term disease-free survival remains challenging. We have introduced concomitant 131I-rituximab radioimmunotherapy (RIT) in an attempt to effect the elimination of lymphoma cells. Our phase II physician-sponsored study of 16 consecutive patients with relapsed, refractory, aggressive B-cell NHL reports a median 44 month follow-up after 131I-rituximab-BEAM conditioning therapy and ASCT. Prospective personalized dosimetry performed in each patient limited the whole body radiation absorbed dose to 0.75 Gy. RIT 131I-rituximab was administered on an outpatient basis on day −15 before ASCT. The BEAM conditioning regimen was commenced on day −6. Evaluable engraftment data are available for 15 patients who had 16 ASCTs. Engraftment was achieved in all patients, 15 out of 16 ASCTs achieved a complete response, and 1 out of 15 ASCTs achieved a partial response. Twelve out of sixteen patients remained alive and disease free at a median of 44 months (range 4–108 months) post-ASCT. This study suggests that the addition of 131I-rituximab RIT to BEAM conditioning, before ASCT, for relapsed or primary refractory B-cell NHL improves disease eradication, compared with BEAM conditioning alone, without significant additional toxicity. In particular, there is an impression of improved disease control in the subset of patients with transformed follicular and mantle cell lymphomas.
Introduction
B-cell non-Hodgkin lymphoma (NHL) is the most common hematologic malignancy, and its incidence is increasing. 1,2 Relapsed and primary refractory B-cell NHL has a poor prognosis with simple salvage chemotherapy. 3,4 Autologous stem cell transplantation (ASCT) has become the standard of care, as the superiority of this modality was first documented in 1991. 5 The addition of rituximab, 6 an anti-CD20 monoclonal antibody, which selectively binds to CD20 antigen on the surface of B lymphocytes, has further improved survival, with minimal additional toxicity. 7 –10 However, patients who relapse within 1 year after rituximab-containing primary therapy have a worse prognosis. 11 Rescuing relapsed aggressive NHL presents a major challenge with a need for new approaches, as adding more conventional therapy to patients for whom current standard treatments have failed will not provide clinical benefit. 12
Radioimmunotherapy (RIT) incorporated into the transplant conditioning regimen has the potential for more effective tumor eradication, before stem cell transplantation. Systemic administration of radioisotope-labeled monoclonal antibodies delivers cytotoxic radiation to tumor cells expressing the targeted CD20 antigen. Moreover, the neighboring tumor cells with lower or absent antigen expression are also irradiated by the 131I beta emission, which has a range of 200 cell diameters. 13 The inherently high sensitivity of lymphoma cells to radiation and the abundance of cell surface CD20 expressed in tumor cells make RIT an attractive adjuvant treatment. 14 –18
Preliminary studies incorporating anti-CD20 RIT with commercially available Yttrium-90–ibritumomab tiuxetan (Zevalin®) 19 –24 and 131I tositumomab (Bexxar®) 25 –27 with ASCT have been recently reported. No significant increase in transplant-related mortality was evident.
We have chosen to use the chimeric anti-CD20 monoclonal antibody rituximab for RIT of NHL and have a 12 year experience using this modality in other cases of B-cell NHL, including relapsed/refractory disease and first-line therapy in follicular lymphoma, and consolidation and conditioning regimens incorporating 131I-rituximab. 15,17,28 This article details the response and toxicity of our 131I-rituximab/carmustine, etoposide, cytarabine, and melphalan (BEAM) conditioning regimen in ASCT for NHL with a median follow-up of 44 months.
Methods
Patient selection
Sixteen patients with B-cell NHL (Table 1) were treated at Fremantle Hospital between January 2003 and January 2012. Patients were eligible if they had relapsed or primary refractory NHL that expressed surface CD20, and were scheduled for ASCT.
ASCT, autologous stem cell transplantation; MALT, mucosal associated lymphoid tissue lymphoma; 18F-FDG-PET-CT, 18F fluorodeoxyglucose positron emission tomography scan combined with computerized tomography scan; DLBCL, diffuse large B-cell lymphoma; MCL, mantle cell lymphoma.
Stem cell collection was carried out using granulocyte colony stimulating factor (G-CSF) mobilization at 5 μg/kg twice daily after chemotherapy, in most cases (Cyclophosphamide or salvage chemotherapy), and apheresis with CD34 flow cytometry counts, with collection of at least 2×106 CD34+ cells/kg.
Institutional Ethics Committee approval in accordance with Australian National Health and Medical Research Council guidelines and the Declaration of Helsinki, and written informed consent from each patient were obtained.
Treatment protocol
Six weeks before transplantation, patients were assessed with regard to the histological diagnosis, date of diagnosis, and initial staging (Ann Arbor) based on computerized tomography (CT) scanning of chest and abdomen or 18 F-fluorodeoxyglucose positron emission tomography combined with computerized tomography ( 18 F-FDG-PET-CT) staging and follow up as recommended for NHL clinical trials. 29 Presence or absence of B symptoms, age, gender, and response to previous treatments were also documented. Other investigations included blood group and type, antibody screening, full blood picture, urea and electrolytes, liver function, lactate dehydrogenase, standard coagulation parameters (international normalized ratio, activated partial thromboplastin time, and fibrinogen), viral serologies (human immunodeficiency virus, hepatitis A, B, C, and cytomegalovirus [CMV]), urinalysis, gated heart scan, pulmonary function tests, chest x-ray, and CT scans of chest and abdomen.
RIT with 131I-rituximab on an outpatient basis was given according to the standard personalized dosimetry protocol predicated on a whole body radiation absorption dose of 0.75 Gy. 17 After RIT treatment at Fremantle Hospital, patients returned to their primary carer at one of the three tertiary teaching hospitals in Western Australia for completion of the conditioning and ASCT.
Standard BEAM chemotherapy consisted of carmustine 300 mg/m2 on day −6, etoposide 200 mg/m2 daily from days −5 to −2, cytarabine 200 mg/m2 twice daily from days −5 to −2, and melphalan 140 mg/m2 on day −1. The antiemetic regimen comprised ondansetron (8 mg intravenous once on days −6 and −1, 8 mg orally thrice daily from day −5 to day −2), dexamethasone (8 mg intravenous before chemotherapy on days −6 and −1), with breakthrough lorazepam (1–2 mg orally) and promethazine (25–50 mg intravenously or orally) if required. G-CSF 300 mcg daily was administered subcutaneously from day +1 until peripheral blood neutrophils were established. Antimicrobial prophylaxis comprised valaciclovir 500 mg and fluconazole 200 mg orally daily starting on day +1 and ending as clinically indicated (usually 28 days post-transplant), along with sulfamethoxazole/trimethoprim 800 mg/160 mg twice daily on 2 days per week. Other supportive therapies, including treatment of febrile neutropenia, blood transfusion support, and supplementation of oral intake, were managed as per the local hospital protocol. Post-transplant clinical monitoring consisted of daily clinical assessment, routine blood tests, and monitoring and treatment of complications as clinically indicated. After discharge from the hospital, patients were seen regularly in the outpatient clinics for ongoing care.
The primary objective of this study was to assess response to treatment by progression-free survival (PFS). The secondary objectives were to assess engraftment, toxicity, and overall survival (OS).
Monitoring response to treatment and unusual toxicity
Engraftment data for neutrophils and platelets were recorded. Response to therapy was monitored by PFS and treatment-related mortality (death within 28 days of transplantation) and relapse rates. Disease activity was assessed at day +100, and at regular 3–6 monthly intervals after ASCT. Assessment consisted of regular history and a physical examination with a blood test measuring the full blood picture, urea and electrolytes, liver function, lactate dehydrogenase, and with objective 18 F-FDG-PET-CT imaging at day +100. Bone marrow aspirates were repeated in those patients with previously documented disease in the bone marrow, or to investigate otherwise unexplained cytopenias. Toxic effects were assessed by using the National Cancer Institute Common Terminology Criteria for Adverse Events. 30
Statistical analysis
Kaplan–Meier methodology was used to estimate median PFS and the PFS of each subgroup using the log-rank test to compute p-values. Curves for PFS and OS are illustrated in Figure 1.
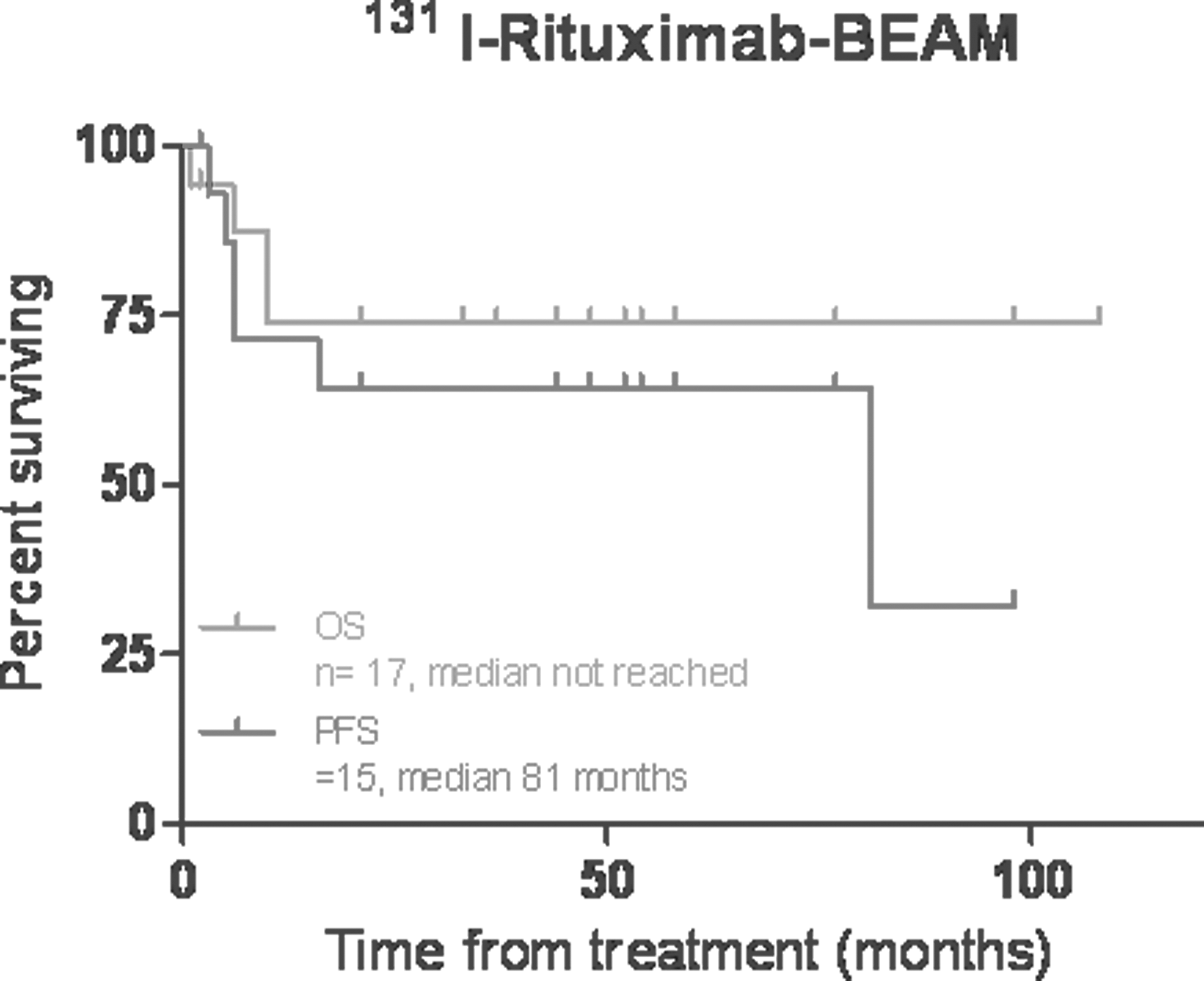
Kaplan–Meier plot of progression-free (PFS) and overall survival (OS) following 131I-rituximab BEAM conditioning and ASCT in 16 patients with aggressive non-Hodgkin lymphoma. PFS n=15 median 81 months. OS n=17 median not reached.
Results
Patient details
Sixteen patients were enrolled in the study; there are evaluable data for 15 patients who had 16 ASCTs. The characteristics of the patients and the diseases are listed in Table 1, and details of treatment before ASCT are provided in Table 2. The median age was 61 years (range 34–71 years). Disease histology was diffuse large B-cell lymphoma (DLBCL) (n=7), transformed or clinically aggressive follicular lymphoma (n=3), mantle cell lymphoma (MCL) (n=6), and mucosal associated lymphoid tissue lymphoma (n=1). Four ASCTs were performed for primary refractory disease, 11 for relapsed disease, and 2 for histological transformation in first remission. Before ASCT, 11 patients had a negative 18 F-FDG-PET-CT scan, 2 patients had a negative CT scan, 2 patients had a positive 18 F-FDG-PET-CT scan, and 2 patients did not have a scan repeated, as ASCT was deemed urgent due to severe disease. The median number of lines of treatment before ASCT was 2 (range 1–11). Disease characteristics and engraftment times and PFS are shown in Table 3. One patient (female) had a second 131I-rituximab BEAM ASCT 7 years after her first procedure, due to late relapse of MCL. One patient aged 59 died on day +6 after ASCT. She had a background of bulky DLBCL with blastic features and t(3;14), which had been diagnosed 19 months earlier. She had relapsed within 4 months of her initial therapy, and received multiple lines of salvage chemotherapy as well as radiotherapy to a refractory site in the skin and soft tissue of the left lower limb, with an associated slowly healing area of ulceration. Persistent disease was documented on 18F-FDG-PET-CT before transplantation, and the significantly increased risks of treatment-related mortality in this patient were discussed and documented. At day +1, she developed fever with respiratory failure and septic shock requiring admission to the intensive care unit for treatment with inotropes and multiple broadspectrum anti-infective agents. Enterobacter aerogenes was identified in multiple blood cultures, as well as Escherichia coli and Staphylococcus species (coagulase negative).
BEAM, carmustine, etoposide, cytarabine, melphalan.
Time (days) until neutrophils >0.5×109/L.
Time (days) until platelets >20×109/L unsupported.
N/A, data not available; FL, follicular lymphoma; IPI, international prognostic index 41 ; MIPI, mantle cell lymphoma international prognostic index 42 ; FLIPI, follicular lymphoma international prognostic index 43 ; CR, complete response; PD, progressive disease; Neut, neutrophils; Plat, platelets; OS, overall survival, PFS, progression-free survival; NHL, non-Hodgkin lymphoma.
Engraftment and toxicity
The engraftment rate was 100% of the 15 evaluable patients, one of whom received a second ASCT. The median time to absolute neutrophil count >0.5×109/L was 12 days (range 9–25 days). The median time to unsupported platelet count of >20×109/L was 17.5 days (range 10–65 days). Grade 3 or 4 toxicity comprised mucositis in 4 patients, with no cases of hepatic, renal, or cardiovascular toxicity. There were no acute infusion reactions associated with 131I-rituximab administration. Transient febrile neutropenia occurred in all patients. Clinically significant infections included the patient who died from respiratory and gram-negative neutropenic sepsis; Pneumocystis jiroveci pneumonia was suspected in 1 patient, and systemic CMV infection was suspected in another—both of whom made a full recovery. The latter was treated with prolonged gancyclovir and received a repeat stem cell infusion at day +52 for significant cytopenias, at which time the quantitative polymerase chain reaction testing was negative for CMV.
Treatment-related morbidity included thyroid gland dysfunction in 3 patients, all of whom were treated satisfactorily with thyroxine and returned to a biochemically euthyroid state.
Response to treatment
Patients were evaluated after RIT and ASCT clinically and with 18F-FDG-PET-CT. At 3 months, the complete response rate (CR) was 15/16 (94%). At a median follow up of 44 months (range 4–108 months), 12 patients are alive, nine remain in remission after RIT and ASCT, 4 patients have relapsed needing subsequent treatment, and four have died. PFS according to prognostic factors was analyzed. Patients with DLBCL had longer PFS compared with other histological subtypes, which was statistically significant (median PFS for DLBCL not reached [range 6–77 months] vs. 4 months [3–5] for aggressive/transformed follicular lymphoma and 81 months [2–81] for MCL, p=0.0011]. Patients with DLBCL had longer PFS compared with patients with aggressive/transformed follicular lymphoma, which was statistically significant (median not reached vs. 4 months, p=0.0039). PFS according to age (<55 years median not reached vs. ≥55 years 81 months [2–81], p=0.2122), gender (male median not reached vs. female 81 [2–81], p=0.9272), and status at ASCT (relapsed median not reached [2–98] vs. refractory 81 [6–81] p=0.8279) was not statistically significant.
One patient received her entire treatment as an outpatient on our Domiciliary Home Transplant program, 44,45 including RIT and intravenous antibiotics. Five patients developed severe isolated neutropenia on routine testing at day +85 post-ASCT. None had significant infections. Two of these patients received G-CSF (Neupogen® [Filgrastim; Amgen, Inc.] 300 μg daily for 5 days). All cases resolved fairly promptly without complication.
One patient, a male who was 71 years old at ASCT, developed myelodysplasia 2.5 years post–ASCT, which was 4 years after his initial diagnosis and CHOP-Rituximab 31 chemotherapy. It was noted that his cytogenetic changes were −7 and add (5) (q22), which are consistent with treatment-related myelodysplastic syndrome 46 although the prognostic significance is not yet fully elucidated. 47
Salvage therapies for patients relapsing after autograft included local radiotherapy, second RIT and BEAM ASCT, and palliative vinorelbine/gemcitabine.
MCL was treated in 5 patients, 2 patients continue in ongoing remission, 2 are in subsequent remission following further therapies (1 received localized radiotherapy to an 18 F-FDG-PET-CT-positive inguinal area, and the other had a repeat ASCT for late relapse) at a median of 35.5 months (range 4–64 months), and 1 died.
Discussion
The addition of rituximab to standard chemotherapy has dramatically improved the response for indolent and aggressive B-cell NHL, 10,48,49 and rituximab maintenance has increased PFS. 49 –52 In contrast to the 90Y-ibritumomab-BEAM 23 and 131I-tositumomab-BEAM 26 protocols, our 131I-rituximab/BEAM protocol employs standard dose rituximab, which may confer an additional therapeutic benefit.
Patients who were recruited nonselectively to our study included many advanced and challenging cases—5 patients with MCL, 1 case of relapsed DLBCL involving the central nervous system, 2 cases with very many previous lines of treatment (6 and 11), and 9 patients over the age of 60. Such patients appear to have a significant risk of relapse after autograft, and it is postulated that the RIT may have assisted in disease eradication and control.
With any additional therapy, there are concerns of potential associated increased toxicity. In our single-agent study of 131I-rituximab therapy, in a more indolent NHL disease group, treatment-related morbidities were generally mild and manageable, and included self-limited cytopenias and delayed hypothyroidism. 17 Neither was mucositis encountered in that group, nor was an excessive problem in this current study of more aggressive NHL reported. Hypothyroidism occurred in 3 patients (19%), and was found on routine screening after 131I therapy. There were no cases of thyroid cancer or other malignancies.
The results in our patients with MCL are especially gratifying, with 4 out of 5 patients still alive and in remission at a median of 35.5 months (range 4–64 months). One patient received her second autograft with the combined 131I-rituximab RIT and BEAM without excessive toxicities or problems, and remains in remission at 2 years (9 years after her initial autograft with this same conditioning), highlighting the possibility of re-treatment with this modality. Similar studies have added RIT to chemotherapy for this disease, including a high-dose regimen followed by ASCT. 53 Reported and ongoing studies utilizing RIT with chemotherapy for MCL without autograft continue at various centers, including impressive early reports of improved CR and PFS rates. 54
RIT has an established role in the management of follicular lymphoma, 20,55 –58 including transformed disease. 55,59 A similar study using 90Y-ibritumomab-BEAM autograft in relapsed or refractory low-grade B-cell NHL demonstrated that 2 year event-free survival and OS were 63% and 97%, respectively. 60
In our small series, the results in DLBCL patients appear promising, though the early reports from a similar study using 131I-tositumomab-BEAM appear to question the value of RIT in this group. 27
Other treatments in relapsed and refractory B-cell lymphoma have included tandem transplantation incorporating RIT 61 and high-dose RIT alone, 62 including 131I-rituximab. 63
Our approach to RIT involves using a standard rituximab dose of 375 mg/m2 in conjunction with the radiolabeled chimeric anti-CD20 monoclonal antibody 131I-rituximab. This permits repeated therapies and does not have the potential for human anti-mouse antibody formation on repeat presentation, which may be seen in 131I-tositumomab RIT. 52 While it is not possible to make accurate comparison across different studies, the similar patient numbers and demographics between the reported 90Y-ibritumomab–BEAM 23 and 131I-tositumomab-BEAM 26 studies, and our 131I-rituximab BEAM, provides an opportunity to explore some similarities with regard to efficacy and toxicity. Table 4 illustrates the differences between the three modalities of RIT. There have been no studies directly comparing these agents, but the response rates to 131I-rituximab in other B-cell lymphomas have been very encouraging. 17,64131I-rituximab may have advantages compared with 131I-tositumomab, with some different characteristics, including the established role of rituximab immunotherapy in the treatment of B-cell lymphomas.
Not including mucositis.
Excluding uncomplicated febrile neutropenia.
Response in 16 treatments in 15 patients.
Five cases of severe isolated neutropenia at around day +80 provided some initial concerns, but were resolved quickly. It appears highly likely that this was a post-rituximab effect, as has been published. 65 –68 The underlying mechanism of this recognized clinical complication has been obscure, and felt to be complex and multifactorial, 66,67 though recently, the increased incidence associated with an FCγ RIIIa polymorphism has been noted, 65,69 as well as late-onset neutropenia has been related to a lack of granulopoiesis in the marrow coinciding with a very high level of B-cell activating factor. 68 Awareness of this phenomenon is important, with the need for prompt presentation with symptoms of infection as well as the monitoring of blood counts post-ASCT is recommended.
One patient developed systemic CMV infection, with marked reduction in graft function in the setting of valganciclovir therapy, necessitating a second infusion of autologous hematopoietic stem cells. Before ASCT, this patient was refractory to RCHOP 31 and received four cycles of RHyperCVAD, 32 which is likely to have contributed to his immunosuppression and associated infection, which was successfully managed. With regard to the patient who died on day +6, sepsis and its associated respiratory failure is a well-recognized complication of ASCT, including BEAM conditioning. Patients receiving single-agent 131I-rituximab at our institution have not developed this complication, and it did not appear likely that this agent had contributed substantially to the patient's demise, though this could not be fully excluded.
One patient in our study developed myelodysplasia at 2.5 years postautograft, with typical chromosome changes related to previous chemotherapy. 46 There have been early concerns that RIT may damage stem cells and the bone marrow microenvironment, with potential for cytopenias, myelodysplasia, and leukemias. Various reports have mitigated these concerns. 28,70,71 The possibility of any additional risk from the 131I-rituximab is uncertain, but probably quite low.
The limitations of our single-center nonrandomized study are acknowledged, though the open consecutive recruitment mitigated any selection bias. All patients who were offered 131I-rituximab-BEAM conditioning consented to this treatment and proceeded with the study. RIT remains an enticing targeted therapy and with further experience, the potential synergy with chemotherapy and the role of this modality will become clearer, particularly with consideration to the potential escalation of treatment intensity and also the utilization of other monoclonal antibodies. RIT with 131I-rituximab in combination with chemotherapy may become favored in certain disease subtypes, including MCL and transformed follicular lymphoma, and ongoing studies concentrating on the role of RIT and ASCT in these groups are planned.
Conclusions
RIT is affordable, practical, and able to be administered in the domiciliary setting. It can also be reutilized in late relapse. Additional toxicity appears limited, and engraftment is satisfactory. Our encouraging results suggest that the addition of 131I-rituximab to BEAM conditioning before ASCT may provide enhanced tumor eradication with improved disease control in aggressive B-cell NHL.
Footnotes
Acknowledgments
The authors wish to thank Jenny Lavin for preparation of the manuscript, Anna Chiam for clinical data management, and Suet Mei Yu for statistical analysis. The support of the WA Cancer and Palliative Care Network is gratefully acknowledged. The authors also thank their fellow Hematologists who referred patients. No grant funding or Pharma industry support was sought or received.
Disclosure Statement
No conflict of interest is declared.