
Abstract
Background:
Cytokine-induced killer (CIK) cells have demonstrated antitumor effects in vitro and in vivo. The purpose of this study was to evaluate the effect of CIK cell treatment as an adjuvant immunotherapy on the prognosis of gastric carcinoma in patients after surgery.
Methods:
The patients with stage II–III gastric carcinoma after gastrectomy, including 53 patients receiving autologous CIK cell treatment combined with chemotherapy (CIK group) and 112 patients in the corresponding period receiving chemotherapy alone (control group), were retrospectively studied. The patients in the CIK group were matched to those in the control group regarding the sex and age of patients, tumor site, histological type, pathological grade, tumor size, clinical stage, and chemotherapy plan. Progression-free survival (PFS) and overall survival (OS) were evaluated.
Results:
The 5-year OS rate in the CIK group was significantly improved compared to that in the control group (56.6% vs. 26.8%, p=0.014). The 5-year PFS rate in the CIK group was also significantly improved compared to that in the control group (49.1% vs. 24.1%, p=0.026). The median PFS (36.0 months) and OS (96.0 months) in the CIK group were significantly prolonged than those in the control group (23.0 months for median PFS and 32.0 months for median OS, p=0.028 and p=0.003). No serious side effect was observed in the CIK group.
Conclusions:
This study suggests that immunotherapy with CIK cells may serve as an adjuvant treatment to prolong the survival of patients with stage II–III gastric carcinoma.
Introduction
Gastric carcinoma is the second leading cause of cancer-related death and the fourth most common cancer in the world. 1 It is estimated that nearly one million new cases were diagnosed each year. The incidence of gastric cancer is different throughout the world. In the United States, new diagnoses have declined steadily, whereas the incidence in Asian countries such as China and Japan remains high. Gastrectomy has been applied as the first choice of therapy for gastric cancer. Chemotherapy and radiotherapy alone or in combination with surgery showed some beneficial effects on gastric cancer. However, the current 5-year survival rate is as low as 20%–30%. 2,3 One of the major issues that cause this low 5-year survival rate is the relapse of cancer that occurs in 50%–90% patients after curative resection of the stomach. 4 Therefore, development of an effective therapy for preventing cancer relapse after surgery is needed for prolonging the survival of patients with gastric carcinoma.
Immunotherapy has currently become a standard treatment for a variety of cancers. The action of immunotherapy is to eliminate cancer cells through the transfer of ex vivo expanded and activated immune cells. Studies have shown that these immune cells, such as cytokine-induced killer (CIK) cells, lymphokine-activated killer cells, natural killer (NK) cells, and dendritic cells, exert immunoregulatory effects on various human cancer cells. 5,6 CIK cells are a heterogeneous subset of ex vivo expanded T-lymphocytes that present a mixed T-NK phenotype and are endowed with an MHC-unrestricted antitumor activity. 7 The antitumor activity of CIK cells is through the high proliferation rate of CD3+CD56+ cells. 8 Increasing evidence suggests that CIK cells have significant cytotoxic effects against various tumor cells, including hepatoma, leukemia, lung, ovarian, and renal cancers in preclinical and clinical studies. 6,9 –13 Thus, the aim of this study was to evaluate the clinical outcomes of CIK cell immunotherapy in patients with gastric carcinoma.
Materials and Methods
Patients
We performed a retrospective study to evaluate the clinical outcomes of autologous CIK cell immunotherapy for patients with stage II–III gastric carcinoma after surgery. The patients were recruited to our study from July 1, 1997, to December 31, 2007, including 53 patients who received chemotherapy and autologous CIK cell immunotherapy in the CIK treatment group, and 112 patients of the corresponding period who received chemotherapy alone were in the control group (Table 1). The criteria for patient selection included patients' age between 18 and 80 years old, an expected survival duration of longer than 4 months, a Karnofsky performance status score higher than 60%, and no cardiac arrhythmias, congestive heart failure, or severe coronary artery disease. Pregnant and lactating women were excluded. This study was approved by the State Food and Drug Administration, China (2006L01023), and by the Ethics Committee of Cancer Hospital of the Tianjin Medical University according to the guidelines of the Declaration of Helsinki.
CIK, cytokine-induced killer.
Treatment plan
The treatment plan conformed to the 2010 NCCN Clinical Practice Guidelines in Oncology. 14 As shown in Figure 1, all patients in the CIK group and the control group received four cycles of chemotherapy within 1 month after surgery. The chemotherapy plan was practiced one cycle per month, which included FUP (DDP at 75–100 mg/m2 body area/day at day 1 and 5-Fu at 1000 mg/m2 body area/day at day 1–5, one time per cycle) or FOLFOX4 (OXA 85 mg/m2 body area/day at day 1, 5-Fu 400 mg/m2 body area/day [iv] and 600 mg/m2 body area/day [civ] at day 1–2, and CF 200 mg/m2 body area/day at day 1–2, two times per cycle).
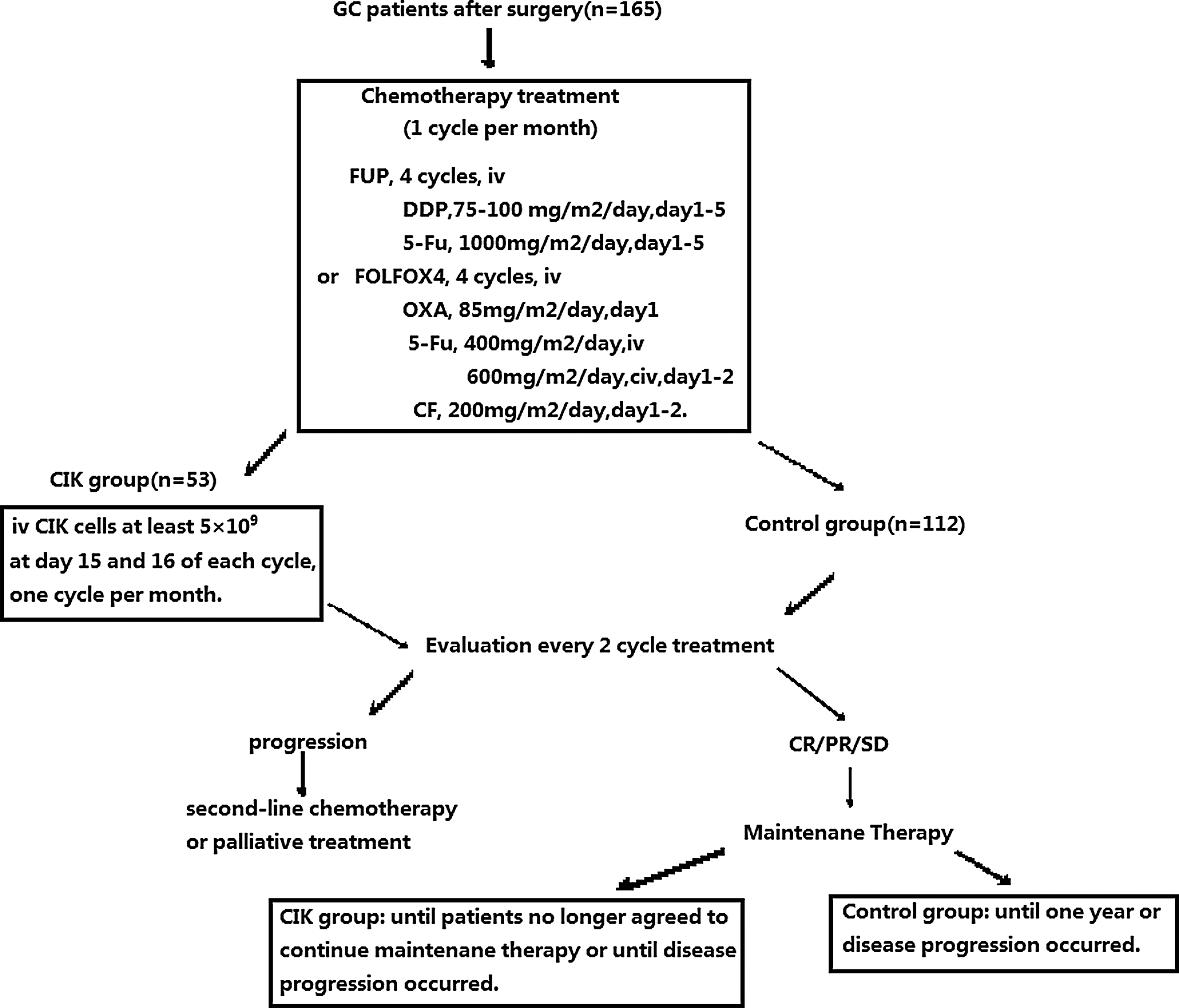
The flow sheets of the clinical study.
For patients in the CIK group, patients were given autologous CIK cell treatment after four cycles of chemotherapy. CIK cell treatment was given at a 1-month interval. The patients were eligible for maintenance treatment until they no longer agreed to continue maintenance treatment or until disease progression occurred. For each treatment, patients were given an infusion of at least 5×109 CIK cells at day 15 and 16 of each cycle. The median courses of CIK treatment were three cycles (range: 2–20 cycles).
Clinical assessment and follow-up
All patients were followed up at the outpatient clinic from the date of initial treatment to December 31, 2010, or to the time of death. Clinical examinations were performed by oncology specialists after every two cycles of treatment, including a complete blood count, abdomen computed tomography scan, and pelvis ultrasonography. Patients were also assessed by a gastroscope once half a year. The response was determined by the National Cancer Institute's Response Evaluation Criteria in Solid Tumors (RECIST). 15 Overall survival (OS) was calculated from the time of surgery until death, and patients alive were censored at the time of last contact. Progression-free survival (PFS) was calculated from the date of surgery until first progression, and patients alive in a stable state were censored at the time of last contact.
CIK cell preparation
CIK cells were prepared as described in our previous studies. 11,16 Briefly, PBMC were collected from the patients after surgery and chemotherapy using a Cobe Spectra Apheresis System (CaridianBCT, Lakewood, CO). For culture of CIK cells, PBMC were cultured in an X-VIVO 20 serum-free medium (Cambrex, East Rutherford, NJ), containing 50 ng/mL anti-CD3 antibody to stimulate CIK cell growth, 100 U/mL recombinant human interleukin (IL)-1α (e-Bioscience, Scan Diego, CA), and 1000 U/mL recombinant human interferon (IFN)-γ (Peprotech, Rocky Hill, NJ), at 37°C with 5% CO2 for 24 hours. Then, 300 U/mL recombinant human IL-2 (Peprotech) was added to the medium. IL-2 and IFN-γ were added to the culture system every 5 days. The CIK cells were cultured for 14 days before analyzed for phenotype and cytotoxicity and used for treating patients. Safety testing was performed during the course of cell culture. All products were free of bacterial and fungal contamination, negative for mycoplasma, and contained <5 Eu endotoxin. The viability of CIK cells was usually 90%–95%.
Detecting the phenotype of CIK cells
Phenotypes of untreated PBMCs and autologous CIK cells from 25 patients selected randomly from the 53 patients in the CIK group were detected by two-color fluorescence as described in our previous studies. 11,16 Briefly, 5×105 CIK cells were resuspended in 20 μL 2% newborn calf serum and 1% sodium azide in phosphate-buffered saline (PBS) and incubated with 10 μL Ab against CD3-FITC/CD56-PE (Dako, Glostrup, Denmark), CD3-FITC/CD4-RPE, and CD8-RPE (BD Bioscience, San Jose, CA) for 30 minutes at 4°C. After incubation, the cells were washed twice with PBS and resuspended in 1.0 mL staining buffer (BD Pharmingen, Franklin Lake, NJ). The cell population was analyzed using flow cytometry (BD Aria, San Jose, CA).
Detecting cytotoxicity of CIK cells
The cytotoxicity of CIK cells was detected as described in our previous studies. 11,16 Briefly, the target cells used for this assay included the lung cancer cell lines A549 and Calu-6, breast cancer cell line MCF-7, gastric cancer cell line 823, and erythroleukemic cell line K562. Target cells (1×105 cells/mL) were incubated for 4 hours in triplicate sets with effector cells (CIK cells) at a ratio of effector to target cells of 40:1. At the end of incubation, 50 μL culture supernatant was transferred to a new, flat 96-well plate and incubated with 50 μL LDH substrate mixture (for detection of LDH released upon cell lysis) at room temperature for 30 minutes in dark. Then, 50 μL stop solution was added to each well. The absorbance was measured at 490 nm using a 96-well plate reader. Specific cytotoxicity was calculated as follows: % specific cytotoxicity=[(experimental counts − effector spontaneous counts − target spontaneous counts)/(target maximal counts − target spontaneous counts)]×100.
Statistical methods
Data were analyzed using the SPSS Version 16.0 for Windows. The OS rate, PFS rate, survival curves, and PFS curves were calculated by the Kaplan–Meier method. Statistical significance was assessed using the log-rank test. A p-value<0.05 was considered as statistically significant.
Results
Patient characteristics
Of the 53 paired patients in the CIK group, 22 had stage II disease, and 31 had stage III disease. The distributions of patient characteristics are shown in Table 1. No statistical difference was found in sex and age of patients, tumor site, histological type, pathological grade, tumor size, clinical stage, and surgical approach between the CIK group and the control group
Phenotypic analysis of CIK cells
Phenotypic analysis of CIK cells in the 25 patients before culture and after 14 days of culture demonstrated that the percentages of the CD3+, CD3+CD4+, CD3+CD8+, CD3+CD56+, and CD25+ cell subsets increased from 48.95%±6.89%, 29.23%±4.87%, 19.25%±5.64%, 3.70%±1.22%, and 15.01%±4.74% to 80.70%±9.21%, 42.75%±7.72%, 36.01%±9.27%, 20.05%±8.14%, and 30.21%±7.53%, respectively, with a p-value<0.05. However, the percentages of the CD3−/16+56+, CD14+, and CD20+ cell subsets decreased from 13.79%±4.97%, 15.84%±7.63%, and 13.02%±5.21% to 7.66%±2.89%, 6.48%±3.02%, and 7.82%±3.96%, respectively, with a p-value<0.05.
Cytotoxicity assays of CIK cells ex vivo
The cytotoxicity of cultured CIK cells against the human erythroleukemic cell line K562, lung cancer cell lines A549 and Calu-6, and breast cancer cell line MCF-7 was 45.21%±5.02%, 31.45%±4.22%, 30.28%±3.45%, and 30.56%±3.92%, respectively. Additionally, the cytotoxicity of CIK cells against the gastric cancer cell line 823 was 35.35%±8.02%.
Prognosis of gastric carcinoma in patients in the two groups
In this study, we evaluated the effects of CIK cell treatment as an adjuvant therapy on the prognosis of gastric carcinoma in patients undergoing chemotherapy after surgery. The 5-year PFS rate in the CIK group was 49.1% (95% CI: 35.4%–62.8%), which was significantly improved compared to that in the control group (24.1%, 95% CI: 16.1%–32.1%, p=0.026). Further, the 5-year OS rate in the CIK group was 56.6% (95% CI: 42.7%–70.5%), which was also significantly improved compared with that in the control group (26.8%, 95% CI: 18.4%–35.2%, p=0.014) (Table 2).
PFS, progression-free survival; OS, overall survival.
Compared to the 3-year PFS rate of 33.0% (95% CI: 24.2%–41.8%) and the 3-year OS rate of 46.4% (95%CI: 37.2%–55.6%) in the control group, the 3-year PFS rate and the 3-year OS rate in the CIK group [54.7% (95% CI: 41.2%–68.2%) and 62.3% (95% CI: 49.0%–75.6%), respectively] were improved; however, there was no significant difference of the 3-year PFS rate and the 3-year OS rate between these two groups (p>0.05) (Table 2).
The median PFS of patients in the CIK group was improved by 13 months compared with that in the control group (36 months vs. 23 months, p=0.028, Table 2 and Fig. 2). The median OS of patients in the CIK group was improved by 64 months compared with that in the control group (96 months vs. 32 months, p=0.003, Table 2 and Fig. 3). These results suggest that CIK cell treatment enhances the clinical efficacy of chemotherapy for patients with gastric carcinoma after surgery.
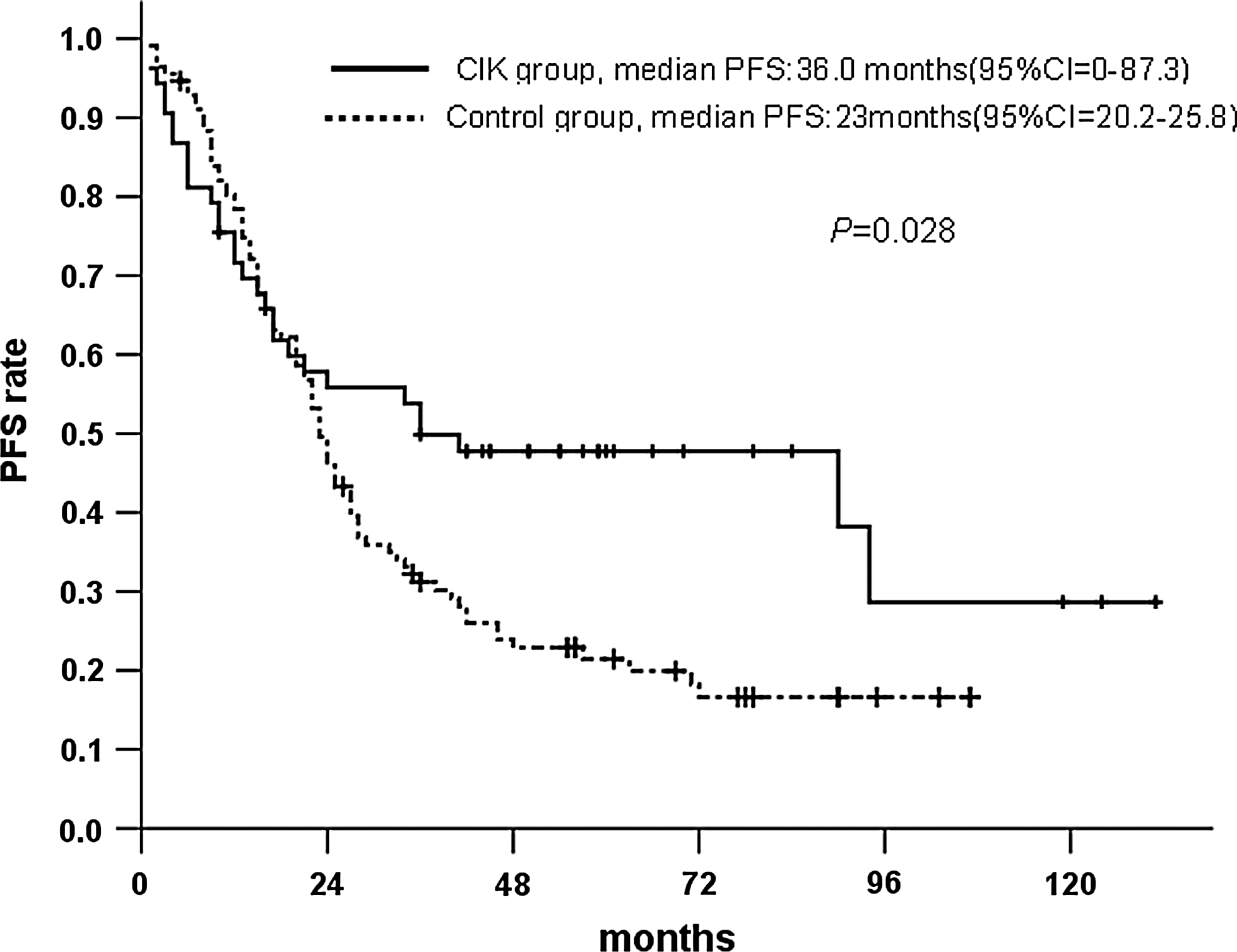
Progression-free survival (PFS) of patients in the two groups.
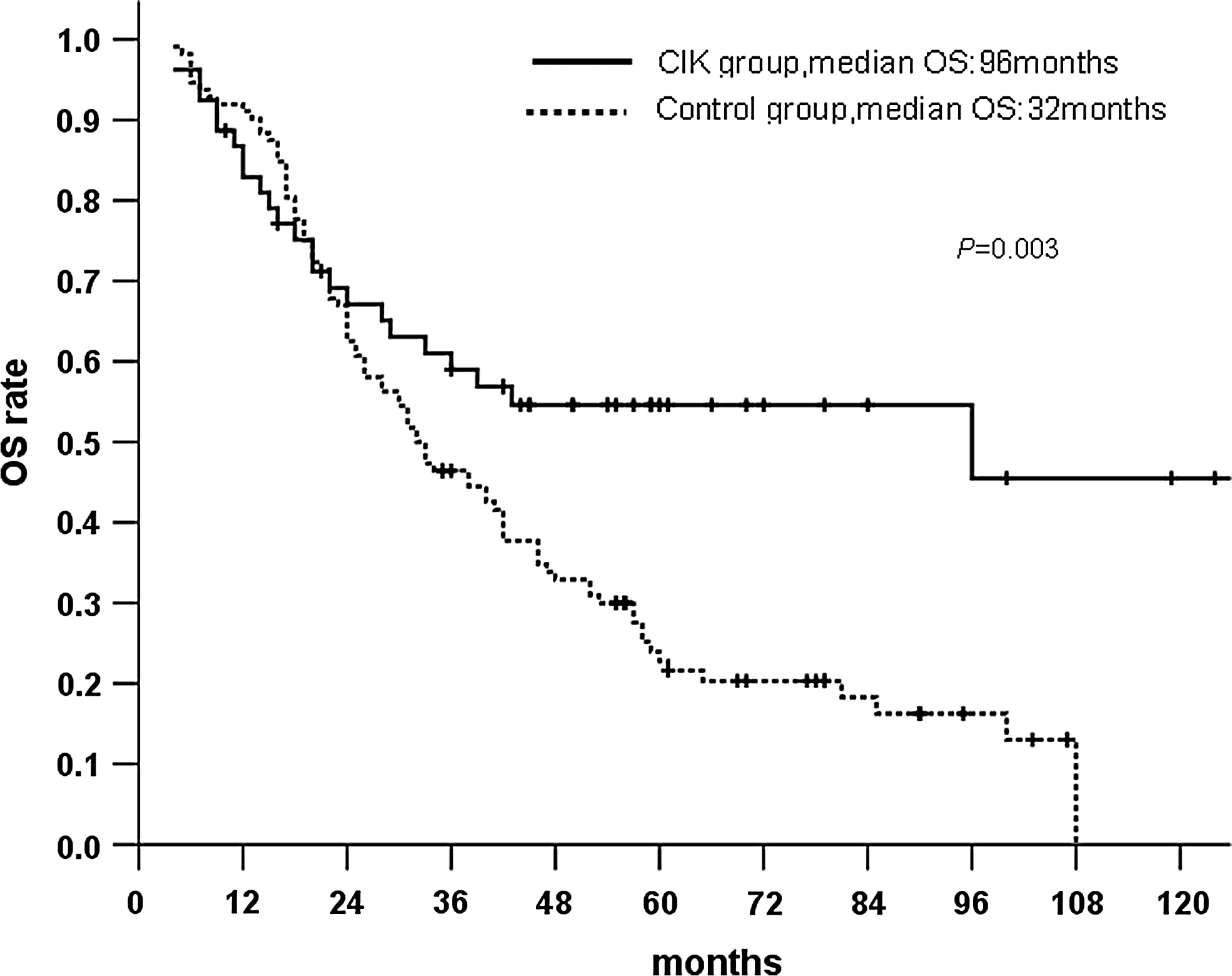
Overall survival (OS) of patients in the two groups.
Prognostic factors of patients in the CIK group
The frequency of CIK cell treatment, clinical stage, and follow-up therapy significantly improved the OS of patients in the CIK group in the univariate analysis (p<0.05). However, only the frequency of CIK cell treatment significantly improved the PFS of patients in the CIK group [(p<0.05), Table 3]. We further analyzed the multiparameters that affected the prognosis of gastric carcinoma in patients in this study through the Cox regression model. Clinical stage (HR: 3.474, 95% CI: 1.157 to 10.433, p=0.026) and cycle count of CIK cell treatment (HR: 0.286, 95% CI: 0.104 to 0.786, p=0.015) significantly improved the OS of patients in the CIK group in the multivariate analysis after adjustment for sex, age, tumor site and tumor size, histological type, surgery method, follow-up therapy, CIK cycle (defined with <3 cycles or ≥3 cycles), and clinical stage. However, the statistical data showed that only the CIK cycle significantly improved the PFS of patients in the CIK group in the multivariate analysis after adjustment for sex, age, tumor site and tumor size, histological type, surgery method, CIK cycle, and clinical stage [HR: 0.335, 95% CI: 0.147 to 0.764, p=0.009 (Fig. 4)].
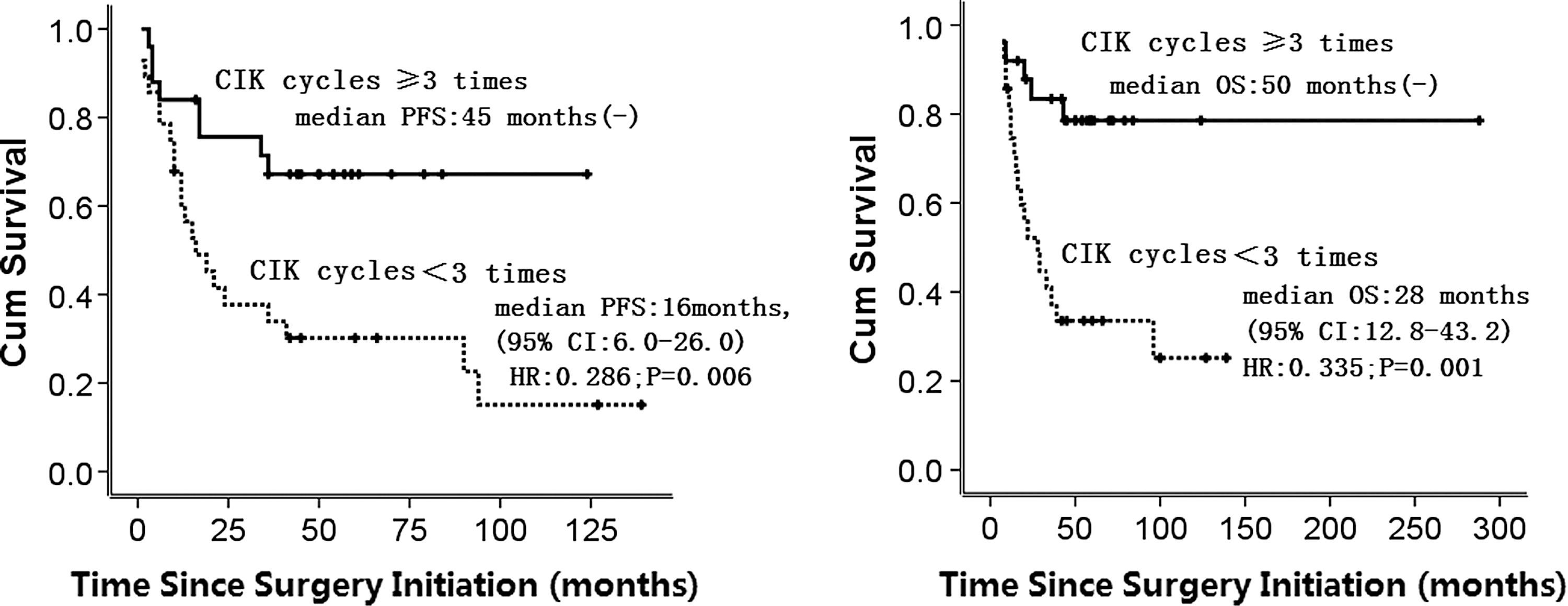
Prognostic impact of the frequency of cytokine-induced killer (CIK) cell therapy on patients in the CIK group.
NA, not available.
Side effects
We did not observe significant side effects in patients by CIK cell treatment. Fever was the only side effect observed in patients receiving CIK cell treatment. Three patients in the CIK group had fever, which was lower than 38.5°C and resolved spontaneously without any medical treatment. No serious adverse events, such as high fever, chills, or anemia, occurred in the patients receiving the CIK cell treatment.
Discussion
Malignant tumor cells could survive after traditional treatments such as radiation and chemotherapy, and these two treatments may cause many side effects that suppress the patient's immune function. 17 Thus, metastatic tumor cells are able to remain and lead to the recurrence of the disease. Adoptive immunotherapy exerts promises as potential approaches for the treatment of various solid tumors, especially that refractory to conventional therapies. Immunotherapy has the advantage of stimulating and restoring the body's natural immune abilities that can recognize and induce tumor cell death. 18 –20 CIK cells, as NK T-lymphocytes, are a heterogeneous population that is generated by induction of peripheral blood lymphocytes using multiple cytokines, including IL-1α, IL-2, IFN-γ, and anti-hCD3 antibody. The major population (90%) of CIK cells is CD3+ T-cells. The other 10% of the CIK cell population consists of CD8+ T cells and CD4+ T cells. CD3+CD56+ cells, which coexpress CD8, but not CD4, are the greatest cytotoxic population in CIK cells. 16 It has been demonstrated that CIK cells can proliferate in vitro and show direct cytotoxicity on malignant tumor cells. 18,21,22 Moreover, CIK cells can secret a variety of cytokines that further enhance the cytotoxicity of immune effector cells and increase the host cellular immune function in vivo. 23,24
An increasing amount of studies showed that CIK cell-based immunotherapy is a promising new treatment modality with the potential to induce a wide spectrum of tumor cell death. In a registry collecting 11 CIK immunotherapy trials with a variety of cancers, although there was no given information on the OS rate, the investigators concluded that adjuvant immunotherapy with cytokine killer cells may prevent recurrence, improve PFS rates, and improve the quality of patient' life. 25 The CIK cells could also induce the death of the chemotherapeutic drug-resistant malignant cells in vivo and in vitro. 26
Our study evaluated the potential effects of autologous CIK cells on patients with stage II–III gastric cancer. We did not analyze the stage I patients because surgical treatments was enough for this part of patients. In our paired study, we showed that autologous CIK cells in combination with chemotherapy could prolong the survival time of patients with stage II–III gastric carcinoma after surgery. The results suggest that the combination of chemotherapy with autologous CIK cells exerts beneficial effects compared to chemotherapy alone.
It should be noted that there are several limitations in this study. First, current results were generated from a retrospective observational study to evaluate the clinical outcomes of autologous CIK cell immunotherapy in patients with gastric carcinoma after surgery. A prospective paired study is needed for confirming the effects of CIK cell treatment. Second, there are only patients with stage II–III gastric cancer in this study. More cases are needed for further analyzing the clinic benefit of CIK cytotherapy for patients with metastatic gastric cancer. Third, the number of the cases limits the further analyzing the influence of the frequency of CIK cell treatment.
In summary, our study suggested that CIK cell immunotherapy in combination with chemotherapy was associated with improvement of prognosis of stage II–III gastric carcinoma after surgery. The side effect of this treatment is limited. Thus, CIK cell immunotherapy may serve as a potential adjuvant treatment for stage II–III gastric carcinoma.
Footnotes
Acknowledgments
This work was partially supported by the National Natural Science Funds (No. 30901376), Tianjin Natural Science Funds (No. 09JCZDCZ0400 and No. 11jcybjc13200), and Tianjin Health Bureau Science and Technology Funds (No. 09KZ80).
Authors' Contributions
H.Z., Y.F., H.L., J.Y., L.L., S.C., B.R., F.Y., and X.R. participated in the design of the study and data analysis. H.Z., F.Y., and X.R. drafted and reviewed the manuscript. All authors read and approved the final manuscript.
Disclosure Statement
The authors declare that they have no competing interests.