
Abstract
Aim:
To investigate the expression status of periostin in colorectal cancer (CRC) to lay a foundation for managing this disease.
Methods:
Periostin expression status was detected by immunohistochemistry staining in 720 CRC specimens. The relationship between the periostin protein and clinicopathological factors and prognosis was subsequently determined.
Result:
The periostin protein was expressed significantly higher in CD133+ tumor cells compared to CD133− tumor cells. Positively expressed periostin was observed in 218 (30.28%) of the 720 cases. Spearman correlation analysis showed that periostin expression has a linear correlation to the tumor size, histological type, lymph node metastasis, TNM stage, and postoperative liver metastasis (p=0.02, 0.035, 0.001, 0.001, and 0.001, respectively). Multivariate analysis showed that histological type, lymph node metastasis, TNM stage, and periostin were found to be related to liver metastasis (p=0.01, 0.035, 0.01, and 0.001, respectively). In the Cox regression test, the histological grade, Lymph node metastasis, TNM stage, and periostin were detected as independent prognostic factors (p=0.01, 0.001, 0.001, and 0.001, respectively).
Conclusion:
Periostin was found to be related to the liver metastasis of CRC and may be a potential target for CRC.
Introduction
Colorectal cancer (CRC) is a common malignancy and remains a formidable health burden worldwide. Almost 70% of CRC patients develop liver metastasis during the course of the disease. 1 Without treatment, the median survival of patients with colorectal liver metastases is (CRLM) 6 to 12 months, and the 5-year survival is less than 10%. 2 Palliative therapy remains the only option for patients with CRLM to improve patient survival, decrease tumor-related symptoms, and improve the quality of life. Developing predictive markers that will lead to early discovery of the distant metastasis and treatment decision are needed urgently for this disease.
Periostin is a kind of bone adhesion molecule that regulates osteoblast adhesion and differentiation and is classified in the extracellular matrix (ECM) proteins. 3 It presents as part of the ECM in natural conditions and plays an important role in fetal development. In adults, the periostin activity occurs only in certain specific organs, such as the breast, bone, skin, and colorectal bowel. 4,5 Periostin has been reported to be involved in tumor Epithelial–Mesenchymal Transition (EMT), ECM degradation, tumor invasion, and distant metastasis. 6 –8
Currently, studies addressing the function and specific mechanism of periostin in the biological behavior of CRC are rare. 4 Moreover, the relationship between periostin expression and the clinic-pathological features and prognosis of CRC is still unclear. In the present study, we investigate the expression status and clinical implications of the periostin protein in CRC and evaluate the possibility of the periostin protein as a biological maker in CRC.
Materials and Methods
Patients and tissue specimens
A total of 720 patients who had histologically confirmed CRC and who underwent radical operations in the General Hospital of ShenYang Military Area Command and the China Medical University between January 2002 and January 2006 were enrolled for immunohistochemical testing and prognostic analysis. The mean age was 49.35±7.68 years (range from 31–82 years). All of the enrolled patients received curative operations and more than 10 lymph nodes were pathologically examined after the operation. The study protocol was approved by the Ethics Committee of the General Hospital of ShenYang Military Area Command and the China Medical University, and written informed consent was obtained from all participants involved in the study.
Tumorigenicity experiment and mammosphere generation test
Human colon cancer tissue (1×1×1 cm per specimen) was minced to 1×1×1 mm with scalpels, washed three times with phosphate-buffered saline (PBS), and then digested by Collagenase III. At the end of the incubation, cells were filtered through a 45-μm nylon mesh and washed twice with PBS. Cells to be injected were then suspended in 1,640/Matrigel mix (1:1 volume) and were then injected into the appropriate area.
For the experiment, we prepared the Complete MammoCult™ Medium (human) by adding 50 mL of thawed MammoCult Proliferation Supplements (human) to 450 mL of MammoCult Basal Medium (human). Single cells were plated on ultralow attachment plates (Corning) at a density of 20,000 viable cells/mL in the Complete MammoCult Medium. The number of spheres for each well was evaluated after 7 days of culture.
Western blot analysis
For Western blot analysis, cells were lysed with a buffer (0.1% sodium dodecyl sulfate (SDS), 50 mM Tris-HCl.(pH 7.6), 1% NP-40, 150 mM NaCl, 2 mg/mL aprotinin, 2 mg/mL leupeptin, and 7 mg/mL PMSF). The protein concentrations were determined using a BCA Protein Assay Kit (Pierce Biotechnology). Thirty micrograms of protein were separated on 10% SDS-polyacrylamide gel electrophoresis gels and transferred to a PVDF membrane. After blocking, the membrane was incubated with the anti-periostin antibody (1:500; Biorbyt Ltd.) at 4°C overnight. After washing, the membrane was incubated with a secondary antibody at a 1:2,000 dilution at room temperature for 1 h. Proteins were detected with an ECL Kit (Varsal Instruments), and the anti-β-actin antibody (Sigma-Aldrich) was used as a loading control. Densitometry was performed by Gel-pro Analyzer software (Media Cybernetics).
Immunohistochemistry experimental procedures
Thin slices of tumor tissue for all cases received in our histopathology unit were fixed in a 4% formaldehyde solution (pH 7.0) for periods not exceeding 24 hours. The tissues were processed routinely for paraffin embedding, and 4 μm-thick sections were cut and placed on glass slides coated with 3-aminopropyl triethoxysilane for immunohistochemistry. Tissue samples were stained with hematoxylin and eosin to determine the histological type and tumor grade.
Briefly, CRC tissues were cut at a thickness of 4 μm using a cryostat. The sections were mounted on microscope slides, air-dried, and then fixed in a mixture of 50% acetone and 50% methanol. The sections were then de-waxed with xylene, gradually hydrated with gradient alcohol, and washed with PBS. Sections were then incubated for 60 minutes with the primary antibody. Following washings with PBS, sections were incubated for 30 minutes in the secondary biotinylated antibody (Multilink Swine anti-goat/mouse/rabbit immunoglobulin; Dako, Inc.). Following washings, the Avidin–Biotin Complex (1:1,000 dilution, Vector Laboratories, Ltd.) was applied to the sections for 30 to 60 minutes at room temperature. The immunoreactive products were visualized by catalysis of 3,3′-diaminobenzidine by horseradish peroxidase in the presence of H2O2 after extensive washings. Sections were then counterstained in Gill's hematoxylin and dehydrated in ascending grades of methanol before clearing in xylene, and then mounting under a coverslip.
To score periostin as immunopositive staining, the positive cells appeared as a yellow to brown color in the nucleus and/or cytoplasm. Periostin expression was classified semiquantitatively according to the following criteria: 0 if <1% of neoplastic cells discretely expressed periostin; 1+ if ≥1 and <10% of morphologically unequivocal neoplastic cells discretely expressed periostin; and 2+ if ≥10% of morphologically unequivocal neoplastic cells discretely expressed periostin. Samples scored as 1+ or 2+ were considered positive.
Statistical analysis
All data were analyzed with SPSS Statistics software (Version 13.0). Relationships between periostin and other parameters were studied using the chi-square test, Fisher's extract test, or independent t tests. Disease-specific survival was analyzed using the Kaplan–Meier method. The log-rank test was used to analyze survival differences. Multivariate analysis was performed using the Cox proportional hazards model selected in forward stepwise. A p-value of less than 0.05 was considered statistically significant.
Results
Periostin expression status in cancer stem cells of CRC
After 7 days of culture, single-cell suspensions of cancer stem cells (CSCs) that were separated from the solid tumors produced viable mammospheres (20–100 μm), which could be passaged further. No mammosphere was produced by the non-CSCs in the same culture condition.
A quantity of 103, 104, 105, and 106 CSCs that were separated from the solid tumors was injected subcutaneously into the right upper back of SCID mice. Meanwhile, the same number of non-CSCs was injected into the left mammary fat pad as a control. Eight weeks postinjection, 103 CSCs successfully formed a tumor (2/4), while non-CD133+ tumor cells failed to form tumors until attaining 106 cells (1/4) (Table 1).
CSCs generated new tumors in mice and cell microspheres that were deficient in NOD/SCID compared to the control group. Furthermore, the periostin protein was expressed higher in the CSCs compared to the control cells (Fig. 1).
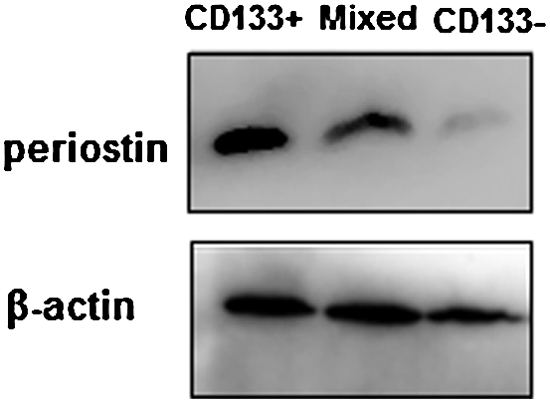
Western blots show that the periostin protein was expressed higher in cancer stem cells (CD133+) compared to the CD133− tumor cells.
Periostin expression in CRC and its relationship with clinicopathological factors
Immunohistochemical examination showed that periostin was located in the cytoplasm and membrane of the CRCs (Fig. 2B). In total, 218 (30.28%) of the 720 CRC cases showed high periostin expression. It was also observed that the periostin protein was expressed significantly higher in CRC tissues compared to paracancerous tissue (30.28% vs. 9.03%) (Fig. 2A).
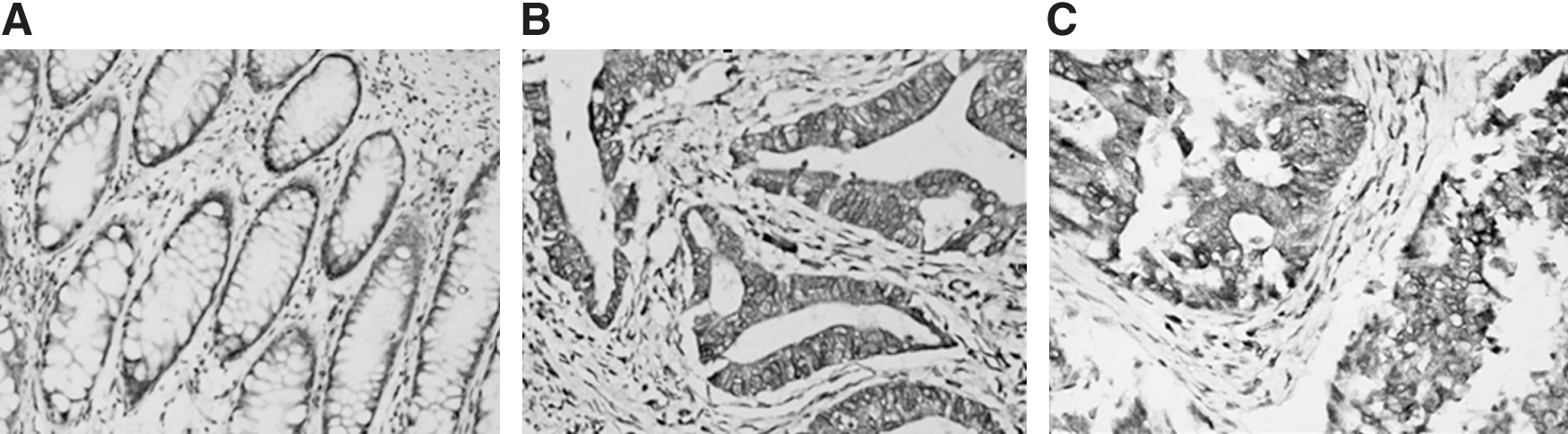
Representative immunohistochemical staining of the tissue samples for periostin. Increased expression of periostin was observed in colorectal cancer
Data from the present study showed that periostin expression was significantly associated with tumor size, histological grade, TNM stage, lymph node, and postoperative distant metastasis (p=0.001, 0.001, 0.001, 0.001, and 0.001, respectively). Periostin expression was not related, however, to patients' age or sex (p=0.864 and 0.074, respectively) (Table 2).
Postoperative recurrence pattern
In the present study, patients with positive periostin expression attained a significantly higher rate of postoperative liver metastasis. Of the 218 cases with high periostin expression, 57 (26.15%) developed 5-year, postoperative liver metastasis, whereas only 5.47% of patients without periostin expression developed 5-year postoperative distant metastasis (p=0.001).
Multivariate Cox regression analysis showed that the histological type, lymph node metastasis, TNM stage, and periostin expression were independent prognostic factors for postoperative liver metastasis (p=0.01, 0.035, 0.01, and 0.001, respectively) (Table 3).
CI, confidence interval.
Prognostic analysis
Of all 720 cases studied, 682 were successfully followed up, for a rate of 94.72%. Survival analysis revealed that periostin was associated with CRC-specific survival in 682 cases (48.51% vs. 76.25%, p=0.001, log rank test, Figure 3A). Furthermore, it was observed that the histological type, lymph node metastasis, and TNM stage were also associated with poorer prognosis (p=0.01, 0.001, and 0.001, respectively; log rank test, Fig. 3B, C). After performing a Cox regression, the histological type, lymph node metastasis, TNM stage, and periostin were shown to be the independent prognostic factors of CRC (Table 4).
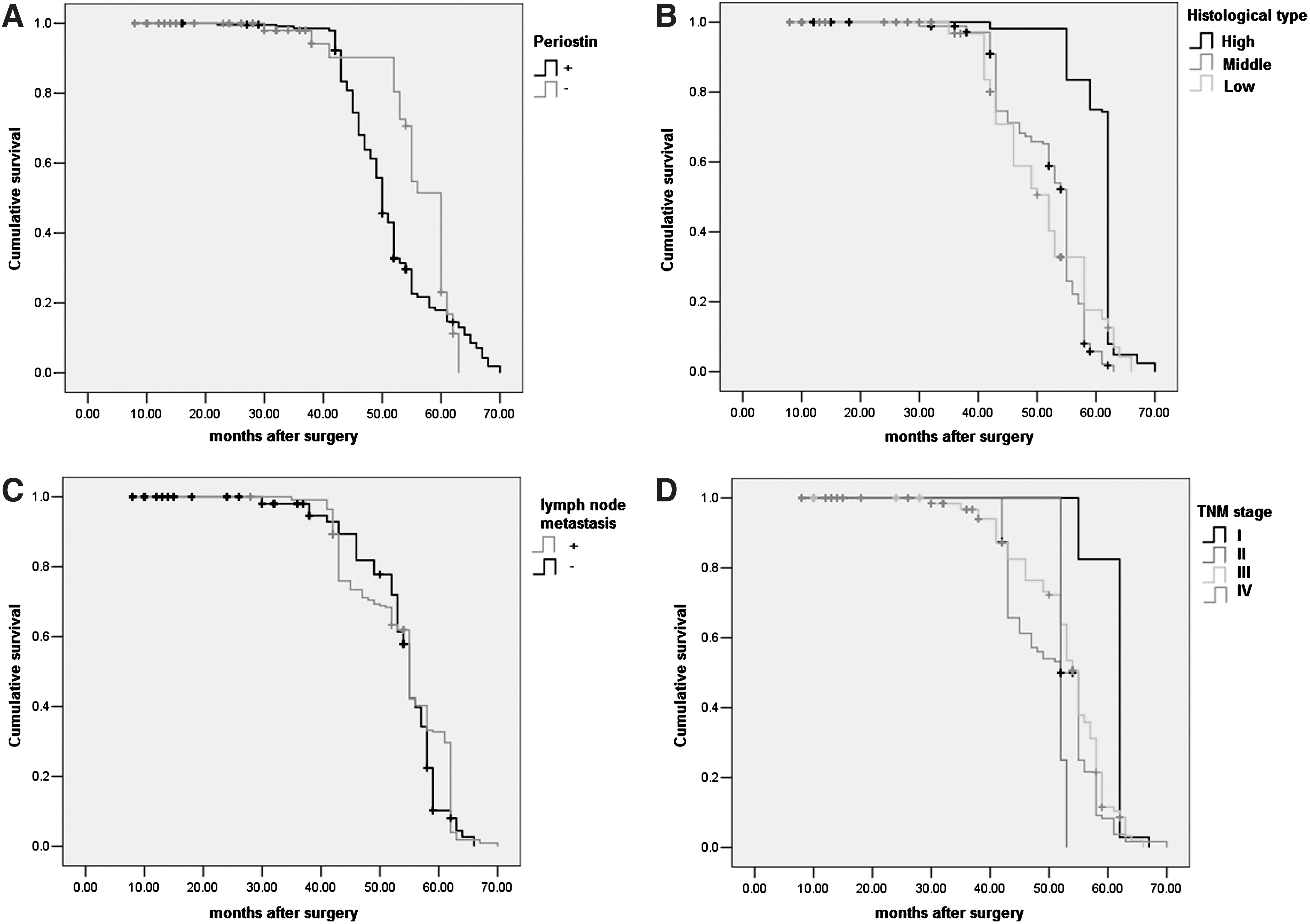
Kaplan–Meier curves for colorectal cancer-specific survival according to periostin expression
Discussion
The concept of CSC has been accepted gradually by most cancer researchers in recent years. The CSC model is also a current focus of CRC research. It has been reported that CD133 is a marker of CSCs in colon cancer. 9,10 The CD133+ tumor cells have the ability to self-renew and to recapitulate the bulk tumor population. Tumor stem cells have been found to be the source of most cancers, as well as the culprit of tumor recurrence, metastasis, and drug resistance. 11 –13 Therefore, selecting the potential targets for treating CRC based on the CSC concept is very important.
In two recent studies, periostin was reported as a bridge between CSCs and metastasis. 14,15 Periostin plays an important role in tumor EMT, tumor angiogenesis, and tumor development. It is also considered as required to maintain CSCs, and that blocking its function prevents metastasis. 6,16 It is upregulated in a wide variety of cancers, including colon, pancreatic, ovarian, head, and gastric cancer. 4,7,8,17 Until now, the expression status and clinical implications of the periostin protein in CRC, however, were still unclear. Furthermore, studies that have addressed the relationship between periostin and chemotherapy sensitivity and prognosis of CRC remain sparse. 18
In the present study, we sorted the CSCs from clinical specimens and observed that periostin was expressed high in CRC CSCs compared to the control group. Moreover, drug sensitivity tests showed that periostin protein expression was significantly related to chemotherapy resistance. We also investigated the relationship between periostin expression and the biological behavior of CRC. We observed that the periostin protein was expressed significantly higher in CRC tissues compared to paracancerous tissues. Periostin protein expression was also found to be related to the tumor size, histological grade, TNM stage, lymph node and postoperative distant metastasis. Moreover, we found that periostin expression has a linear correlation to the tumor size, histological type, lymph node metastasis, TNM stage, and postoperative liver metastasis.
In the present study, patients with positive periostin expression suffered a significantly higher postoperative liver metastasis rate. Furthermore, survival analysis revealed that periostin was associated with CRC-specific survival. After performing a Cox regression, periostin was shown to be an independent prognostic factor of breast cancer. The present study found that periostin was highly expressed in CSCs and could be a potential biomarker for the liver metastasis and chemotherapy resistance of CRC tumors. The underlying genetic mechanism by which periostin regulates CRC CSCs is still unclear, however, and needs further investigation.
Footnotes
Disclosure Statement
No financial conflict of interest exists.