
Abstract
Rational and Objective:
Radioembolization with yttrium-90 microspheres is a therapy that is used for hepatic tumors. 20–30 μm microspheres loaded with Y90 are supposedly occluding tumor vessels at the capillary level. Then, these spheres deliver high-dose radiation to the tumor. However, this theoretical embolic effect has never been appreciated in imaging. Dual-Phase cone-beam computed tomography (DPCBCT) is a multi-phasic intra-procedural scan that uses only one contrast media injection to visualize early (feeding vessel) and delayed (capillary level) tumor enhancement. The purpose of this study was to determine whether there is a micro-embolic effect induced by TheraSpheres® (MDS Nordion, Ottawa, Ontario, Canada) at the capillary level by using DPCBCT imaging.
Materials and Methods:
14 patients with 72 carcinoid or neuroendocrine tumors were treated with radioembolization, and all underwent DPCBCT (Allura Xper, Philips Healthcare) imaging before and immediately after radioembolization with TheraSpheres®. Tumor enhancement was measured in each phase by drawing a region of interest within the tumors.
Results:
72 tumors were evaluated: average tumor density in the early arterial phase was 241 and 230 Hounsfield units (HU) (p<0.001) before and after radioembolization, respectively; the average density in the delayed arterial phase was 226 and 161 HU (p<0.001) before and after radioembolization, respectively. Average difference in tumor attenuation before and after radioembolization in early arterial and delayed phase was 11 HU and 64 HU (p<0.001), respectively.
Conclusion:
The significant decrease in tumor enhancement in the DPCBCT delayed phase after TheraSpheres® injection indicates that there is an appreciable microembolic effect at the tumor capillary bed level.
Introduction
Radioembolization is an image-guided interventional oncology therapy that is used to treat liver tumors. There are two radioembolization products that are currently commercially available: TheraSpheres® (MDS Nordion, Ottawa, Ontario, Canada) and SIR spheres® (SIRtex, Woburn, MA). As compared with SIR spheres®, TheraSpheres® utilize smaller and fewer beads (20 to 30 μm diameter, average of 1.2 million beads) but can deliver higher amounts of radioactivity for the same bead amount. 1 These radioactive spheres are supposed to lodge themselves within the tumor and produce microscopic embolization in the tumor capillary bed (Fig. 1) while not affecting blood flow in the larger intra-hepatic arterial branches. 2

Radioembolization and micro-embolization concept. This representative illustration presents a schematic view of the connection between tumor neo-vessel network and native hepatic arterial network. Neo-vessels are immature, tortuous and have small diameters. Theraspheres® should be deposited only in the tumor capillary bed, therefore delivering radiation close to the tumor.
However, the spatial resolution of modern x-ray digital subtraction angiography (DSA) systems (pixel sampling interval 154 μm; Nyquist frequency 3.25 lp/mm) is insufficient to resolve any density modification at the tumor capillary level, because the TheraSpheres® are very small. 3,4 Furthermore, DSA is a planar imaging technique that suffers from image superposition which further limits spatial resolution. More recently, C-arm cone-beam computed tomographic (CBCT) technology has emerged as a useful tool in conjunction with standard DSA for the treatment of liver tumors. In addition to having a higher contrast resolution as compared with DSA (contrast resolution 1 to 10 HU), CBCT generates a 3D image that does not suffer from superposition. 5,6 CBCT can also provide additional information about tumor and tissue perfusion. For example, CBCT is equally as sensitive as multiphasic MRI in detecting tumors. 7 –10 A recent improvement of the CBCT is Dual-Phase CBCT (DPCBCT). DPCBCT (Philips Healthcare, Best, The Netherlands) can acquire multi-phasic scans using only one injection of contrast media. When used for transcatheter arterial chemoembolization (TACE) or radioembolization, DPCBCT captures two enhancement phases of the same hepatic-tumor structure. The early arterial phase shows the normal arterial network and the tumor feeding arteries, while the delayed phase shows tumor enhancement at the capillary level. 11
The purpose of our study was (1) to evaluate the micro-embolic effect induced by TheraSpheres® at the capillary level by comparing delayed phase tumor image enhancement before and after radioembolization, and (2) to determine whether TheraSpheres® induce macrovascular flow reduction or occlusion (at the level of the hepatic arteries) by comparing early arterial DPCBCT images before and after radioembolization. The study was conducted in patients with neuroendocrine or carcinoid liver metastasis.
Materials and Methods
This was a single-institution prospective clinical trial of radioembolization for patients with liver dominant metastases (neuroendocrine or carcinoid) in which all imaging was analyzed retrospectively. It was compliant with the Health Insurance Portability and Accountability Act and was approved by the Institutional Review Board. All patients provided informed consent before inclusion in the study. Diagnosis of liver metastases was confirmed by biopsy, or past history of known primary malignancy. All patients for radioembolization were evaluated and treated for unresectable carcinoid or neuroendocrine liver metastases after discussion at our institution's multidisciplinary liver conference. Eligibility criteria for radioembolization were as follows: Eastern Cooperative Oncology Group performance status 2 or better; Child-Pugh classification A or B; focal or multifocal hepatic malignancy; and no contraindications to iodinated contrast media injection.
Radioembolization was performed with TheraSpheres® after a first angiography. This was done for nontarget arteries coil embolization and Y90 irradiation dose calculation with albumin macroaggregate injection. Both were performed as recommended by Kennedy et al. 2 Regardless of the tumor burden, all patients had single lobar treatments. For bilobar presentation, treatment was split into two separate sessions, ∼30 days apart. No whole-liver administration was performed. Lobar treatment was targeted to deliver an absorbed dose of 120 Gy according to previously published dosimetry techniques. 12
All patients underwent C-arm DPCBCT imaging before and immediately after radioembolization. Imaging was performed using a commercially available angiographic system (Allura Xper FD20, Philips Healthcare, Best, The Netherlands). This system was equipped with the XperCT option, enabling C-arm CBCT acquisition and volumetric image reconstruction (Feldkamp back projection). 13 For each CBCT scan, the region of interest (ROI) was positioned in the system iso-center. Over ∼10 seconds, 312 projection images (30 frames per second) were acquired with the motorized C-arm covering a 220° clockwise arc. As the images were acquired, the projections were reconstructed to produce volumetric data. The two-dimensional projection images were reconstructed using Feldkamp back projection into 3D volumetric images with 0.98 mm isotropic resolution for a 250×250×194 mm field of view (matrix size 256×256×198). 13 The DPCBCT feature allows for the acquisition of two sequential, back-to-back CBCT scans; so, both early and delayed arterial phases are captured using only one contrast injection. 11 In this study, the two scans were triggered at 3 and 28 seconds after a selective single injection of undiluted contrast medium through a 3-French co-axial microcatheter (Renegade® HI-FLO™; Boston Scientific, Natick, MA) placed in the proper hepatic artery. The same contrast injection protocol was applied to all cases (amount, 20 mL; rate, 2 mL/sec; Oxilan 300 mg I/mL, Guerbet, Roissy France). The patients were instructed to be at end-expiration apnea during each of the CBCT scans with free breathing between the early and delayed scans. Oxygen was administered to patients during the procedure to minimize the discomfort of breath holding. One-millimeter-thick CT-like axial images were obtained for analysis. Figure 2 summarizes the dual-phase CBCT concept.
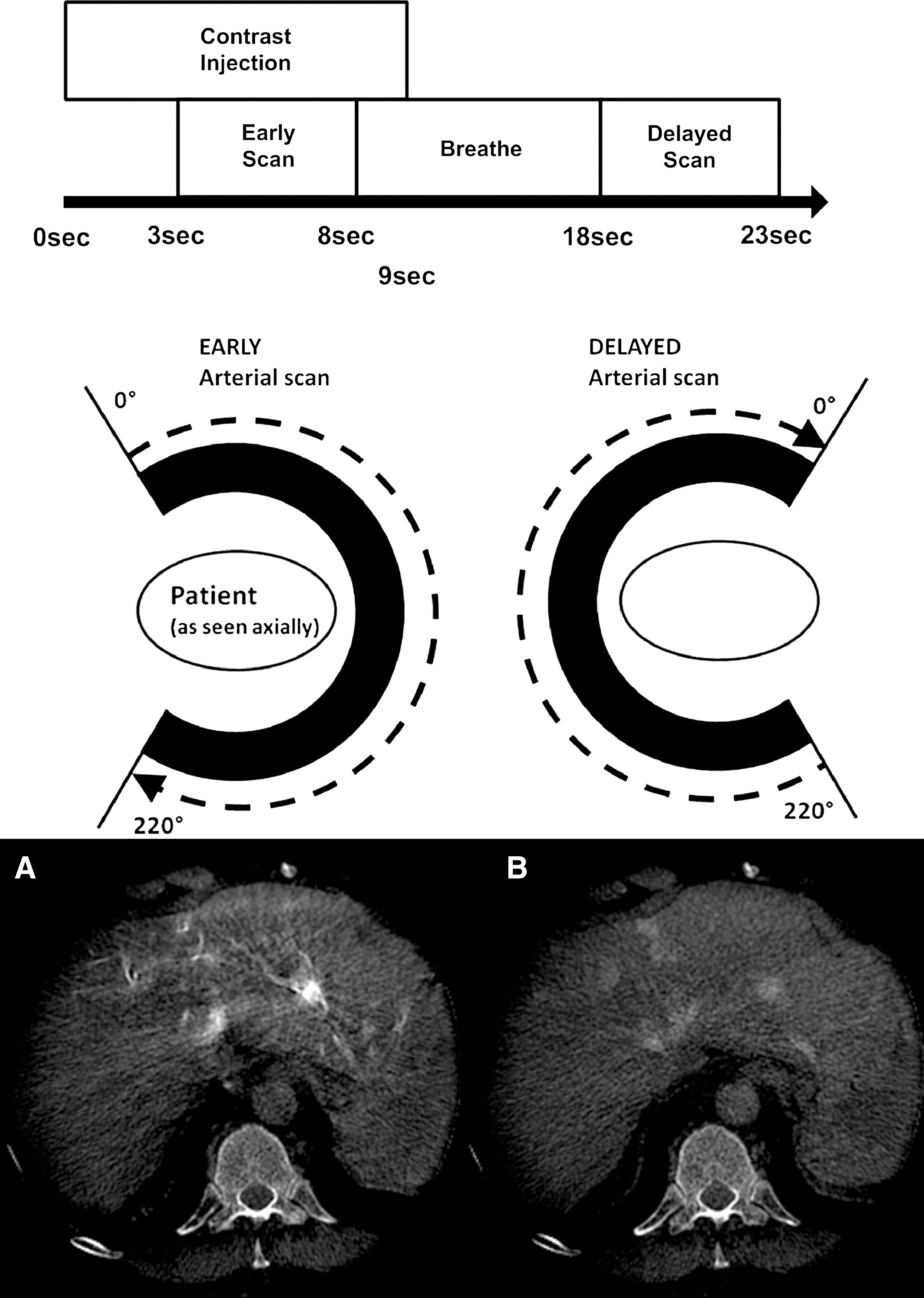
Representative view of the Dual-Phase cone-beam computed tomography (DPCBCT) concept. Imaging is performed using a commercially available angiographic system (Allura Xper FD20, Philips Healthcare, Best, The Netherlands) equipped with the XperCT option, enabling C-arm CBCT acquisition and volumetric image reconstruction (Feldkamp back projection).13 For each CBCT scan, the region of interest (ROI) is covered by 312 projection images (30 frames per second) covering a 220° clockwise arc. As the images are acquired, the projections are reconstructed to produce volumetric data with 0.98 mm isotropic resolution for a 250×250×194 mm field of view (matrix size 256×256×198).13 The DPCBCT feature allows the acquisition of two sequential, back-to-back CBCT scans; so, both early
One experienced Interventional Radiologist with 9 years of experience, who did not participate in the radioembolization procedures, evaluated all DPCBCT images retrospectively using ImageJ software (National Institutes of Health, Bethesda, MD). This software was used to evaluate the enhancement change by measuring the density of a target structure in Hounsfield Unit (HU). 14 ROIs were drawn on one axial slice for each phase of DPCBCT before and after radioembolization where the tumor presented with the largest axial diameter as commonly done in RECIST. 15 For each DPCBCT, the density (mean, standard deviation, and range value) of liver tumor, right lumbar muscle, and right retro-peritoneal fat were measured by ROIs. The density measurements in muscle and fat were performed five times in the pre-/post-radioembolization and at both DPCBCT phases. These measurements were considered a signal base reference. The density of the tumor was then measured using the same axial slice pre-/post radioembolization and same-sized ROI (Fig. 3). To mitigate any density modification, the same window level and width were applied to all four data groups (early and delayed scans for pre-/post-radioembolization). Image artifacts were defined as the presence of streak artifacts and/or motion artifacts and/or artifacts caused by the catheter placed in the hepatic artery.

Representative DPCBCT images (in 3 mm thick maximum intensity projection [MIP*] post processing), of the early and delayed arterial phase before radioembolization procedure
Paired t-tests were used to compare the average pre- and post-radioembolization ROIs density at early and delayed DPCBCT phases for muscle and fat. The difference in density pre-/post-radioembolization between arterial and delayed phases for muscle and fat were also compared using a paired t-test. Mixed effects models were used to compare the average pre- and post-radioembolization density and the difference in density level pre-/post-radioembolization for tumor to account for the correlations among measures taken from the same tumor or the same patient. Statistical significance in this study was reported as p-values. To adjust for multiple comparisons using Bonferroni approach, a p-value <0.004 was considered statistically significant. Data analysis was performed using STATA version 11.0 (Stata Statistical Software; College Station, TX 2010).
Results
Between January 2011 and July 2011, 14 consecutive patients (28 hepatic lobes, 11 men, 3 women; mean age, 66 years;±7.1 [range 53–78]) who had radioembolization performed for liver dominant carcinoid and neuroendocrine malignancies were successfully treated with radioembolization and included in this study. All patients underwent DPCBCT scans before and after radioembolization (28 total scans). Five DPCBCT scans had minimal image artifacts: two of these were from motion, and three were from the 3 Fr catheters in the hepatic artery. There were no major image artifacts (including streak artifacts). Table 1 summarizes all patient characteristics at baseline. The mean radiation absorbed dose to the target hepatic volume was 114 Gy±7 [range 96–124]. The mean activity administered was 2.3 GBq±0.5 [range 1.25–3.20].
All 72 tumors were studied (average tumor per patient: 5.14 tumors±3.3 [Range 1–13]). The mean tumor diameter was 44 mm±19.36 [Range 12–88]. A total of 848 density measurements were performed for the 72 tumors, including 70 right lumbar muscle ROIs, and 70 right retro-peritoneal fat ROIs. This included all pre- and post-radioembolization for both early and delayed arterial phases of DPCBCT.
The mean tumor densities observed in the early and delayed arterial phases before and after radioembolization were 241 HU±89 [104–537] and 226 HU±59 [127–420]; 230 HU±86 [127–420] and 161 HU±60 [10–326], (p<0.001), respectively (Table 2). A large density difference (64 HU) between the pre- and post-radioembolization, with strong statistical significance (p-value<0.001), was observed in the tumor for the delayed arterial phase. Though a statistical difference (p-value <0.001) was also observed in the tumor for the early arterial phase between pre- and post-radioembolization, the magnitude of density difference was much lower than that in the delayed phase (11 HU vs. 64 HU, Table 3). The density difference observed in the background tissue reference was not significant. Five DPCBCT scans had minimal image artifacts (motion artifact n=2, catheters n=3). There were no major image artifacts (including streak artifacts) that hindered measurements. Tables 2 and 3 summarize the density findings. A representative patient case is presented in Figure 3. Note the similar level of tumor enhancement between the pre-/post-Y90 early arterial phase (Fig. 3A, C) and the significant level of enhancement difference for the delayed phase (Fig. 3B, D).
Difference of image density level between pre- and post-radioembolization at early and delayed arterial phases, grouped by ROI. Values: mean±standard deviation [range], HU, Hounsfield units; ROI, region of interest.
Values: mean±standard deviation [range], HU, Hounsfield units; ROI, region of interest.
Discussion
We report two main findings: (1) The statistically significant difference in tumor density on the delayed DPCBCT phase before and after radioembolization assesses the tumor enhancement change. This reflects tumor perfusion change, and suggests that the administration of TheraSpheres® modifies the tumor capillary bed flow. Furthermore, the level of this difference is especially high at 1050 HU, p<0.001, Table 3). This finding supports the theory that radioembolization with TheraSpheres® primarily affects the tumor capillary bed, confirming that the radiospheres lodge themselves deeply within the tumor. This difference, which was only observed in the tumors, is real because there was no significant difference in density in the tissue background measurement (used as reference). Since this difference is concentrated in the tumor, this could be called a “micro-embolic effect.” (2) The second main finding is the presence of a limited density difference between before and after radioembolization at the early arterial phase (11 HU at the early phase vs. 64 HU at the delayed phase p<0.001). (Table 3) supports the theory that radioembolization causes minimal changes in the macrovasculature. This change could be due to macrovascular upstream effects secondary to the hemodynamic changes mentioned earlier at the tumor capillary level and confirm the notion of an “inside-out” radiation delivery process.
The radioembolization concept is based on selective high-dose radiation delivery through the hepatic arterial network to the tumor. 2 The mechanism of treatment, at least until now, appeared to be due to internal radiation effects and microscopic embolization. As such, the main goal is not to occlude the macro-vessels but to deliver the radiospheres to the tumor bed via its arteriolar network. This is the intended effect, because adequate oxygenation of the tumor tissue acts synergistically with radiation and increases the lethal effect. 16,17 Furthermore, ischemia due to macro-vessel embolization could limit the efficacy of the treatment and induce post-embolization syndrome. 2,16 Radioembolization therapy success relies on the particles being able to reach the peri-tumoral and intra-tumoral vessels to deliver the Y90 as close as possible to the tumor cells while reducing more proximal arterial occlusion and consequent extra-tumoral irradiation.
Since the start of radioembolization, there has been controversy about the potential macro-embolic effect produced by the radiospheres, and its effect on the efficacy of therapy. Radiospheres have a potential of aggregating when injected in large quantities. Animal and clinical studies have shown that a macro-embolic effect could occur when more than 8 million beads are injected. 18 The embolization of the macro circulation is a possible complication of radioembolization and can be avoided by the use of very small spheres (<30 μm diameter) loaded with a high dose of Y90 (e.g., 2500 Bq per sphere) and delivered close to the tumor capillary bed by arterial flow. 18
Sato et al. 19 demonstrated no significant macroscopic evidence of embolization in the hepatic arterial vasculature—no diminished inflow or inflow contrast attenuation as a consequence of Therasphere® embolization. However, this was a subjective inter-observer analysis performed on pre- and post-Therasphere® DSA arteriograms. In a large retrospective study, Stribley et al. 20 showed that there was no change in the tumor blush after radioembolization procedure. However, due to the planar nature of DSA and its limitations with superposition, the true micro-embolic effect cannot be adequately observed. DPCBCT with its 3D capabilities, better soft-tissue image contrast, and multi-phasic acquisition has helped answer the question of C-arm CBCT being able to detect a micro-embolic effect after radioembolization of neuroendocrine and carcinoid liver metastasis.
The strength of our measurement method is that the density measurements of the reference ROIs were not subject to statistically significant variations for all phases, pre- and post-radioembolization. The mean denstity in muscle and fat was subject to minimal variation (Tables 2 & 3), whereas the tumor density at the early and delayed phases was significantly higher than the references for the pre- and post-radioembolization. This establishes that the density measured is due to contrast media injection, and is not related to image artifacts or noise.
The observed results were obtained using CBCT technology, specifically the Dual-Phase technique. Currently, CBCT is used to identify the arterial tumor network and extra hepatic feeding arteries in order to facilitate TACE and radioembolization procedures. 21 Acquisition of two sequential enhancement times of the same hepatic level exclusively by an arterial injection provide more accurate information on tumor perfusion. 22,23 Perfusion studies performed within conventional helical-CT units and direct injection of contrast media into the hepatic arteries have showed that early arterial imaging revealed all macro-arterial networks, including the tumor feeding arteries, while the delayed imaging contained only the tumor enhancement at the capillary level. 24 DPCBCT technology works in a similar manner. The hyper-acute nature of the arterial contrast medium bolus in enhancing hepatic tumors allows for increased tumor enhancement, and avoids portal enhancement of healthy liver. The novelty of DPCBCT is the possibility for tumor imaging at both early (hepatic arterial network and tumor feeding vessel enhancement) and delayed arterial (tumor at capillary level enhancement) phases using only one intra-arterial injection of contrast medium. The delayed phase is crucial in the study of tumor viability; especially in trans-arterial embolization and biotherapies, 17,25 because any perfusion changes observed at the capillary level is a major predictive factor of treatment success. 25 Decrease of tumor signal enhancement observed in the DPCBCT delayed phase after radioembolization is due to the micro-embolic effect of the 30 μm spheres. Theraspheres® should be considered a disruptive agent to capillary level enhancement, and is, therefore, responsible for the micro-embolic effect as observed with DPCBCT.
Our study has some limitations. The small patient number, although partially compensated by the number of tumors per patient, is a limitation. Moreover, variations in Therasphere® deposition into the tumor bed depends on tumor vascularity, blood flow direction, and velocity within the arterial tree and capillary bed. Finally, pathologic and histological correlations would be extremely useful to prove that the spheres lodged in the tumor capillaries. However, given the fact that these patients were not surgical candidates, this was not possible. TheraSphere® consists of insoluble glass microspheres, where yttrium-90 is an integral constituent of the glass. 26 The glass microsphere is not loaded or mixed with x-ray contrast agent and so, the microsphere's x-ray mass attenuation coefficient is similar to that of soft tissue. Furthermore, the line-integral of x-ray attenuation through even a completely filled tumor feeding micro-vessel is in the order of 1–2 mm. With the small amount of microspheres and minimal x-ray attenuation, the microspheres can be generally considered radio-lucent and, thus, minimally impacts the measurements in this work. 27 Even with these limitations, we believe that there is strong indirect evidence showing that the Theraspheres® cause significant micro-embolic effects.
Conclusion
Tumor imaging at both early (tumor feeding vessel enhancement) and delayed arterial (tumor parenchymal enhancement) phases using only one intra-arterial injection of contrast medium is possible using DPCBCT. DPCBCT's ability to assess image enhancement changes related to transarterial embolization demonstrates that radioembolization causes (1) a micro-embolic effect at the tumor capillary level, and a (2) minimal macro-embolic effect on tumor feeding arteries. This intra-procedural imaging concept appears as a promising technical development with numerous clinical ramifications, and can help elucidate the physiological mechanisms involved in embolization.
Footnotes
Acknowledgments
This study was funded by NIH/NCI R01 CA160771, P30 CA006973, Philips Research North America, Briarcliff Manor, New York, and the French Society of Radiology (SFR).
Disclosure Statement
MingDe Lin is a Philips employee. Jean-François Geschwind is a consultant to Biocompatibles, Bayer Healthcare, Guerbet, Nordion, Merit, Abbott and Jennerex. For other authors, no relevant disclosures.