
Abstract
Purpose:
The association between Toll-like receptor 2 (TLR2) −196 to −174del polymorphism and Toll-like receptor 4 (TLR4) polymorphisms (Asp299Gly, Thr399Ile, and 3725G>C) and gastric cancer risk are still conflicting. For better understanding of the effects of these four polymorphisms on gastric cancer risk, a meta-analysis was performed.
Methods:
An extensive search was performed to identify all case–control studies investigating such associations. Odds ratios (ORs) with 95% confidence intervals (CIs) were estimated to assess the relationship.
Results:
A total of 21 studies (3,436 cases and 4,239 controls) were found to be eligible for meta-analysis. In the overall analysis, a significantly increased risk was observed in TLR4 Asp299Gly polymorphism (G allele vs. A allele: OR=1.84, 95%CI: 1.41, 2.39; GA vs. AA: OR=1.89, 95%CI: 1.43, 2.48; Recessive model: OR=1.90, 95%CI: 1.44, 2.49) and TLR4 Thr399Ile polymorphism (T allele vs. C allele: OR=1.97, 95%CI: 1.22, 3.18; TC vs. CC: OR=1.94, 95%CI: 1.19, 3.15; Recessive model: OR=1.98, 95%CI: 1.21, 3.21), whereas no associations were found in any genetic models of TLR2 −196 to −174del and TLR4 3725G>C polymorphisms. Similar results were found in the subgroup analyses by ethnicity. However, we detected that A allele carriers of the TLR4 Asp299Gly polymorphism might have an increase risk of gastric cancer in the Helicobacter pylori-positive population (G allele vs. A allele: OR=2.01, 95%CI: 1.22, 3.31).
Conclusion:
The results of this meta-analysis indicate that the TLR4 Asp299Gly and Thr399Ile polymorphisms are risk factors for gastric cancer development.
Background
While gastric cancer incidence and mortality have both shown decreasing trends in recent decades, gastric cancer is still one of the most devastating human cancers worldwide, ranking fourth in incidence and second in mortality universally. 1 In 2008, an estimated 989,600 new cases and 738,000 deaths occurred, accounting for 8% of the total cases and 10% of total deaths, respectively. 2 Over two-thirds of the cases and deaths occurred in developing countries and 42% in Eastern Asia. 2 Although the precise etiology of gastric cancer is unknown, unhealthy diet, infectious agents (e.g., Helicobacter pylori), genetic factors, and pre-existing conditions (e.g., pernicious anemia, atrophic gastritis, and intestinal polyps) are thought to be risk factors for the development of gastric cancer. 3 On the other hand, a diet that is high in raw fruits and vegetables, citrus fruits, and fiber may lower the risk. 4 However, they do not provide a complete explanation. Recently, close attention has been paid to the association between genetic factors, such as single-nucleotide polymorphisms (SNPs) of genes, and the development of gastric cancer. 5
Toll-like receptors (TLRs) belong to a group of pattern recognition receptors that play an important role in the regulation of inflammatory reactions and activation of the adaptive immune response to eliminate infectious pathogens and cancer debris. 6 –8 In humans, 10 different TLRs have been identified. 9 TLRs are important pattern recognition receptors of microorganisms. Their dysregulations owing to SNPs may alter the ligand binding and balance between pro- and anti-inflammatory cytokines and may thereby modulate the risk of developing chronic inflammatory diseases and cancers. 10 –12
In the past decade, there were many epidemiological studies, which have studied the association between TLR gene variants and risk of gastric cancer; however, the results of these studies were conflicting. For example, a case–control study conducted in Brazil by de Oliveira 13 indicated that TLR2 −196 to −174del and TLR4+896G may increase the risk of gastric cancer. However, other studies reported that there were no associations between TLR polymorphisms (e.g., TLR4 3725G>C and TLR2 −196 to −174del) and the risk of gastric cancer. 14,15 Similarly, inconclusive results were also reported for other polymorphisms.
To further evaluate the association between TLR2 polymorphisms (−196 to −174del) and TLR4 polymorphisms (Asp299Gly, Thr399Ile, and 3725G>C) and the risk of gastric cancer, a meta-analysis was conducted on all eligible published studies in the current study.
Methods
Selection of published studies
A systematic search was performed using the PubMed, Embase databases (last search: July 13, 2011) with the following MeSH terms and keywords: TLR2, TLR4, Toll-like receptor 2, Toll-like receptor 4, polymorphism, gastric cancer, gastric carcinoma, and stomach neoplasms. The scope of article search was expanded according to the reference list of retrieved studies. Studies included in our meta-analysis have to meet the following criteria: (i) articles investigating the association between TLR2 polymorphism (−196 to −174del) and TLR4 polymorphisms (Asp299Gly, Thr399Ile, and 3725G>C) and gastric cancer risk; (ii) case–control studies; (iii) providing available genotype frequency for computing odds ratios (ORs) with 95% confidence intervals (CIs); (iv) studies with full-text article. Major reasons for exclusion of studies were (i) only case population; (ii) the study did not have the outcomes of comparison reported or it was not possible to determine them; (iii) duplicate of previous publication; (iv) benign tumors, precancerous lesions.
Data extraction
Two investigators (Jian Chen and Sheng Hu) screened titles, abstracts, and full texts independently using a standardized extraction form. For conflicting evaluation, an agreement was reached following consensus and discussion. For each study, the following characteristics were collected: the first author's name, year of publication, country of origin, ethnicity, genotyping method, total number of cases and controls, H. pylori infection status, and genotype distributions in cases and controls. We did not define any minimum number of patients to include in our meta-analysis.
Statistical analysis
All analyses were performed using STATA software (version 11.0; Stata Corporation, College Station, TX), and all tests were two sided with a significance level of 0.05, unless stated otherwise. The Hardy–Weinberg equilibrium (HWE) in controls was assessed by the chi-squared test and a p<0.05 was considered as significant disequilibrium. If HWE disequilibrium existed (p<0.05), or it was impossible to evaluate this equilibrium, sensitivity analysis was performed. The strength of the association between the TLR polymorphisms and gastric cancer risk was measured by ORs with 95% CIs. The Q statistic was used to test for heterogeneity among the studies included in the meta-analysis. 16 When the Q-test p-value was no less than 0.1, the fixed effect model with the Mantel–Haenszel method was used to calculate the pooled ORs. 17 Otherwise, a random effect model with the inverse variance method was used. To take TLR4 Asp299Gly as an example, pooled ORs were obtained from a combination of single studies by heterozygote comparison (GA vs. AA), homozygote comparison (GG vs. AA), dominant and recessive models (GG+GA vs. AA and GG vs. GA+AA), and allelic comparison (G vs. A). Similarly, the comparisons of the results of other polymorphisms were also obtained. In addition, we also performed stratification analyses on ethnicity. The Begg and Mazumdar 18 adjusted rank correlation test and the Egger regression asymmetry test 19 were plotted to provide a diagnosis of publication bias.
Results
Characteristics of the studies
According to the search strategy of using different combinations of key terms on PubMed, a total of 90 articles were included in this meta-analysis (Fig. 1). Of the 90 studies, we reviewed the articles, abstracts, and the full texts. A total of 21 case–control studies in11 articles met our inclusion criteria, 12 –15,20 –26 including 3436 cases and 4550 controls. Table 1 lists the characteristics of each study. Among these studies, four case–control studies, including 1294 cases and 1566 controls were investigated in the TLR2 polymorphism (−196 to −174del); nine studies were included in the TLR4 Asp299Gly polymorphism analysis, with 1286 cases and 1215 controls; the TLR4 Thr399Ile polymorphism employed 5 studies, including 554 cases and 821 controls, whereas two studies were included in the TLR4 3725G>C polymorphism analysis, with 696 cases and 637 controls. The distribution of genotypes in the controls of all studies was consistent with the HWE.

Studies identified with criteria for inclusion and exclusion.
Study data of the status of Helicobacter pylori of gastric cancer were accessible.
HWE, Hardy–Weinberg equilibrium; PCR-RFLP, polymerase chain reaction-restriction fragment length polymorphism; PCR-CTPP, PCR with confronting two-pair primers; PB, population-based case–control study; HB, hospital-based case control.
Meta-analysis
The association strength between TLR polymorphisms and the susceptibility for GC are presented in Table 2. Overall, no associations were found in any genetic models of TLR2 (−196 to −174del) polymorphism (del vs. ins: OR=1.27, 95%CI: 0.83, 1.95; insdel vs. deldel: OR=1.12, 95%CI: 0.74, 1.69; deldel vs. insins: OR=1.61, 95%CI: 0.64, 4.03; Dominant model: OR=1.58, 95%CI: 0.70, 3.57; Recessive model: OR=1.21, 95%CI: 0.75, 1.94) (Fig. 2) and TLR4 3725G>C (C allele vs. G allele: OR=0.90, 95%CI: 0.75, 1.08; CG vs. GG: OR=0.92, 95%CI: 0.72, 1.17; CC vs. GG: OR=0.79, 95%CI: 0.51, 1.22; Dominant model: OR=0.83, 95%CI: 0.54, 1.27; Recessive model: OR=0.89, 95%CI: 0.71, 1.13), whereas a significant increased risk was observed in the TLR4 Asp299Gly polymorphism (G allele vs. A allele: OR=1.84, 95%CI: 1.41, 2.39; GA vs. AA: OR=1.89, 95%CI: 1.43, 2.48; Recessive model: OR=1.90, 95%CI: 1.44, 2.49) (Fig. 3) and TLR4 Thr399Ile polymorphism (T allele vs. C allele: OR=1.97, 95%CI: 1.22, 3.18; TC vs. CC: OR=1.94, 95%CI: 1.19, 3.15; Recessive model: OR=1.98, 95%CI: 1.21, 3.21) (Fig. 4). When stratified according to ethnicity, we found that the TLR4 Asp299Gly polymorphism (G allele vs. A allele: OR=1.90, 95%CI: 1.43, 2.51; GA vs. AA: OR=1.96, 95%CI: 1.46, 2.63; Recessive model: OR=1.97, 95%CI: 1.47, 2.63) and the TLR4 Thr399Ile polymorphism (T allele vs. C allele: OR=2.84, 95%CI: 1.56, 5.15; TC vs. CC: OR=2.81, 95%CI: 1.53, 5.17; Recessive model: OR=2.88, 95%CI: 1.57, 5.29) increased the cancer risk in Caucasians, however, no association was found in any subgroup of the TLR2 polymorphism. When stratified by the source of control, significant associations between the TLR2 (−196 to −174del) polymorphism (del vs. ins: OR=1.93, 95%CI: 1.18, 3.15), TLR4 Asp299Gly polymorphism (G allele vs. A allele: OR=1.90, 95%CI: 1.43, 2.51), TLR4 Thr399Ile polymorphism (T allele vs. C allele: OR=2.84, 95%CI: 1.56, 5.15), and gastric cancer were found in the population-based case–control subgroup (Table 2). When stratifying for H. pylori infection status (H. pylori-positive cancer patients compared with H. pylori-positive controls, or H. pylori-negative cancer patients compared with H. pylori-negative controls), no statistically findings were observed in the TLR2 (−196 to −174del) polymorphism and TLR4 Thr399Ile polymorphism, whereas we detected that A allele carriers of the TLR4 Asp299Gly polymorphism might have an increase risk of gastric cancer in the H. pylori-positive population (G allele vs. A allele: OR=2.01, 95%CI: 1.22, 3.31).

Forest plot of odd ratios (ORs) of TLR2 −196 to −174del polymorphism (del allele vs. ins allele) associated with cancer stratified by ethnicity.

Forest plot of ORs of TLR4 Asp299Gly polymorphism (G allele vs. A allele) associated with cancer stratified by ethnicity.
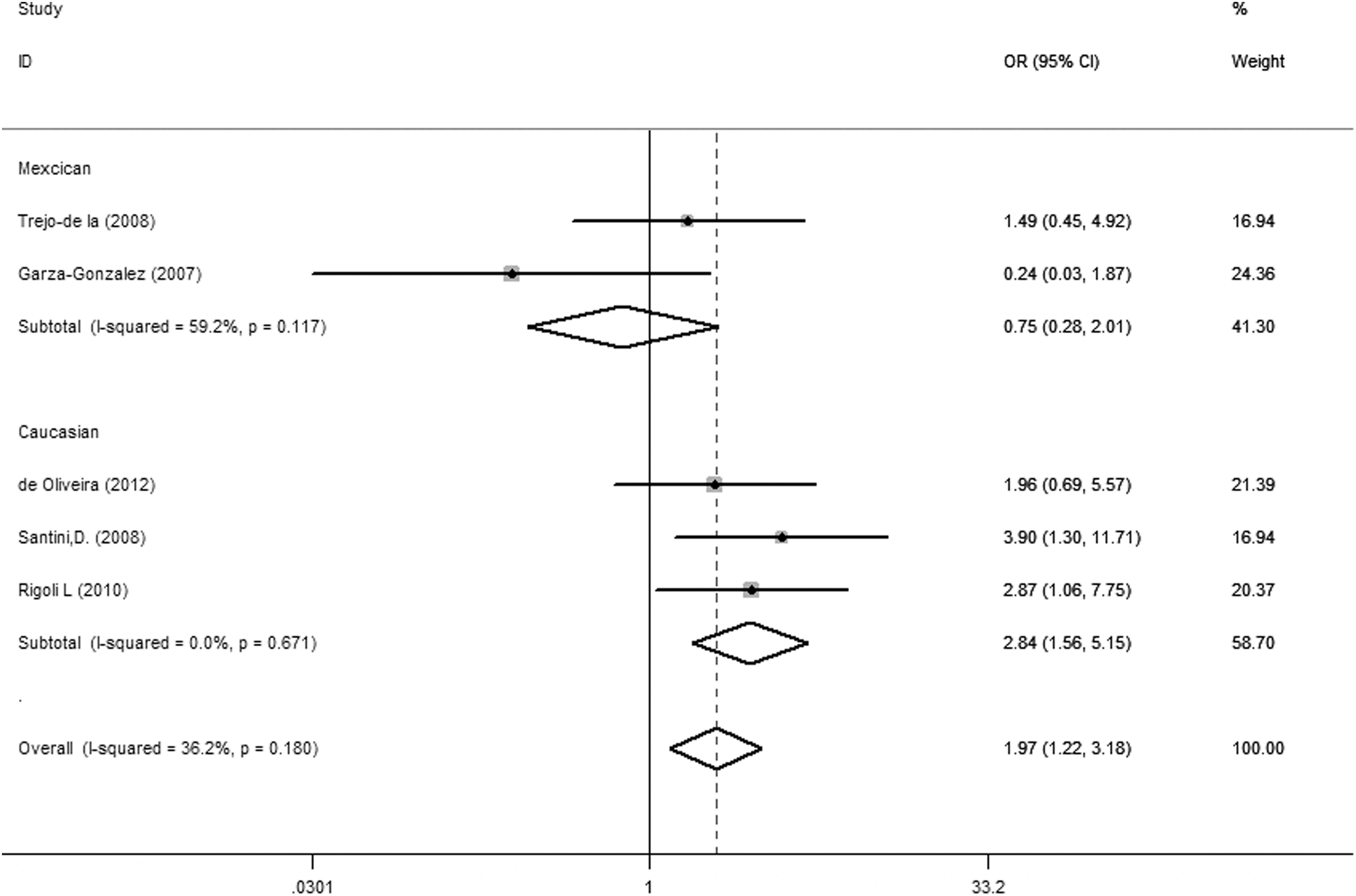
Forest plot of ORs of TLR4 Thr399Ile (T allele vs. C allele) associated with cancer stratified by ethnicity.
Random model was chosen for data pooling when p-value<0.10 and/or I 2>50%; otherwise fixed model was used. The numbers in bold indicated statistically significant values.
N, involved studies' number; OR, odds ratio; CI, confidence intervals; VR, variant; WT, wild-type; Ht, heterozygote; VR Ho, variant homozygote; WT Ho, wide-type homozygote; NA, not applicable.
Sensitivity analyses and publication bias
When examining the genotype frequencies in the controls, no significant deviation from HWE was detected, indicating that the final results of this meta-analysis were relatively stable and reliable. Both the Begg's and Egger's test were conducted to assess the publication bias of literature. For the Begg's test, no evidence of publication bias was observed in all comparison models in this meta-analysis, whereas the Egger's test revealed statistical significance for publication bias in all comparison models except one study 12 (Table 3). When this study was deleted, I 2 decreased from 34.3% (P=0.192) to 0% (P=0.663). While the summary OR for allele contrast (T vs. C) remained significant (OR=2.45, 95%CI: 1.46, 4.12), this result was similar to pooled OR without deletion of any study (OR=1.97, 95%CI: 1.22, 3.18).
The numbers in bold indicated no statistically significant values.
Discussion
TLRs are a central part of the innate immune defense against microorganisms. TLRs are evolutionarily conserved receptors first described in Drosophila 27 and contain three domains: (i) leucine-rich repeat motif in the ectodomain; (ii) the single transmembrane domain; and (iii) cytoplasmic signaling domains known as Toll IL-receptor domains. 28 The protein function of TLRs may be impaired by SNPs within TLR genes, causing an altered susceptibility to cancer. The importance of TLR polymorphisms' influence on gastric cancer has been recognized in recent years, however, the existing data are contradictory. Therefore, we provided a comprehensive analysis on the association of the TLR polymorphisms with gastric cancer risk. To the best of our knowledge, this is the first meta-analysis associating TLR polymorphisms with gastric cancer risk.
For the past decades, the causal link between H. pylori and GC has been confirmed. 29 TLR2 mediates immune response against HP infection 30 and Noguchi 31 found that the del allele of the Delta22 SNP decreased the transcriptional activity of the TLR2 gene and may therefore increase the risk of H. pylori infection and lead to severe H. pylori-related disease, such as gastric cancer. 30 However, our meta-analysis indicated that the TLR2 gene polymorphism (−196 to −174del, Delta22) may not be associated with gastric cancer. In the stratified analysis by ethnicity, no significant associations were found. Possible explanations may include the following: (i) lack of case–control studies limited our evaluation on the association between Delta22 and gastric cancer risk; (ii) Mbulaiteye 32 and Cavaleiro-Pinto 33 showed a stronger association between noncardia gastric cancer and H. pylori infection than cardia gastric cancers, so no evidence of Delta22 on gastric cancer was found because of the different cases they recruited; and (iii) ethnic differences in the genetic background and the environment the population lived in may contribute to different cancer susceptibility. For example, Zeng 21 and de Oliveira 13 found that individuals with TLR2 del allele could reduce cancer susceptibility in Chinese (del vs. ins: OR=0.71, 95%CI: 0.56, 0.89), but increase cancer susceptibility in Caucasians (del vs. ins: OR=2.54, 95%CI: 1.66, 3.89), for the reason that the former subjects were from the northern Chinese and the latter Caucasian population were from Brazil (a country of high incidence of gastric cancer), suggesting that gastric cancer is a complex disease with many associated factors, such as the dietary habits and life-style factors. However, detailed large-sample studies should be employed.
In the overall Asp299Gly and Thr399Ile analysis, we showed that the presence of minor alleles significantly increased the risk of gastric cancer when compared to major alleles, indicating that the two genetic variants in TLR4 may crucially modify the susceptibility of GC. In the subgroup of ethnicity, we found significant associations between the two polymorphisms and increased risks of GC in Caucasians, but not in Mexicans. The inconsistency between the two ethnicities may be explained by the different life styles and environment factors of the different ethnic groups. A former meta-analysis reported insignificant associations between Asp299Gly and GC because of fewer included studies. 34 When stratified by H. pylori infection status for Asp299Gly polymorphism, we only found that patients with H. pylori infection (compared with H. pylori-positive controls) had a significantly higher frequency of A allele carriers, however, these results should be considered with care because of the limited studies. TLR4 is one of the best-studied TLRs. 9 Genetic variants of the two polymorphisms may disrupt the normal structure of the extracellular region of the TLR4 and are therefore thought to disturb TLR signaling and affect the production of inflammatory cytokines and the maturation and apoptosis of immune cells, which play a critical role in the development of carcinogenesis. 35 In conclusion, the two polymorphisms should be paid more attention as the most significant TLR4 polymorphisms.
In the overall TLR4 3725G>C analysis, our results did not show any statistical significance. However, new and large-scale case–control studies are required to ascertain the accurate effect of the polymorphism on gastric cancer risk.
In interpreting the present results, some limitations should be addressed. First, lack of the original data of the reviewed studies limited our evaluation on the potential both gene–gene and gene–environment interactions. Second, the controls were not uniformly defined. Some studies employed a healthy population as the reference group, whereas others used hospital patients without gastric cancer as the reference group. Thus, the controls may not always truly represent the underlying source populations. Third, all case–control studies were from Asia, Europe, the United States, and Mexico. Therefore, these results may be applicable only to these ethnicities.
In summary, this meta-analysis indicated that Delta22, Asp299Gly, and Thr399Ile may increase the susceptibility of gastric cancer in Caucasians, whereas Delta22 may decrease the susceptibility of gastric cancer in Chinese. However, it is necessary to employ detailed large-sample studies, containing detailed individual data, standardized unbiased genotyping methods, homogeneous gastric cancer patients, and well-matched controls, to lead to a better, in-depth understanding of the association between these polymorphisms and gastric cancer risk.
Footnotes
Acknowledgments
We thank all the people who helped in this study. This research was supported by the Guangdong Foundation for Leading Talented Scientists (C1030925).
Disclosure Statement
All authors have declared that no competing interests exist.